
Implementing A Flexible Sensor to Identify Forces during Instrument-Assisted Soft Tissue Mobilization



Abstract
1. Introduction
2. Materials and Methods
2.1. Methods
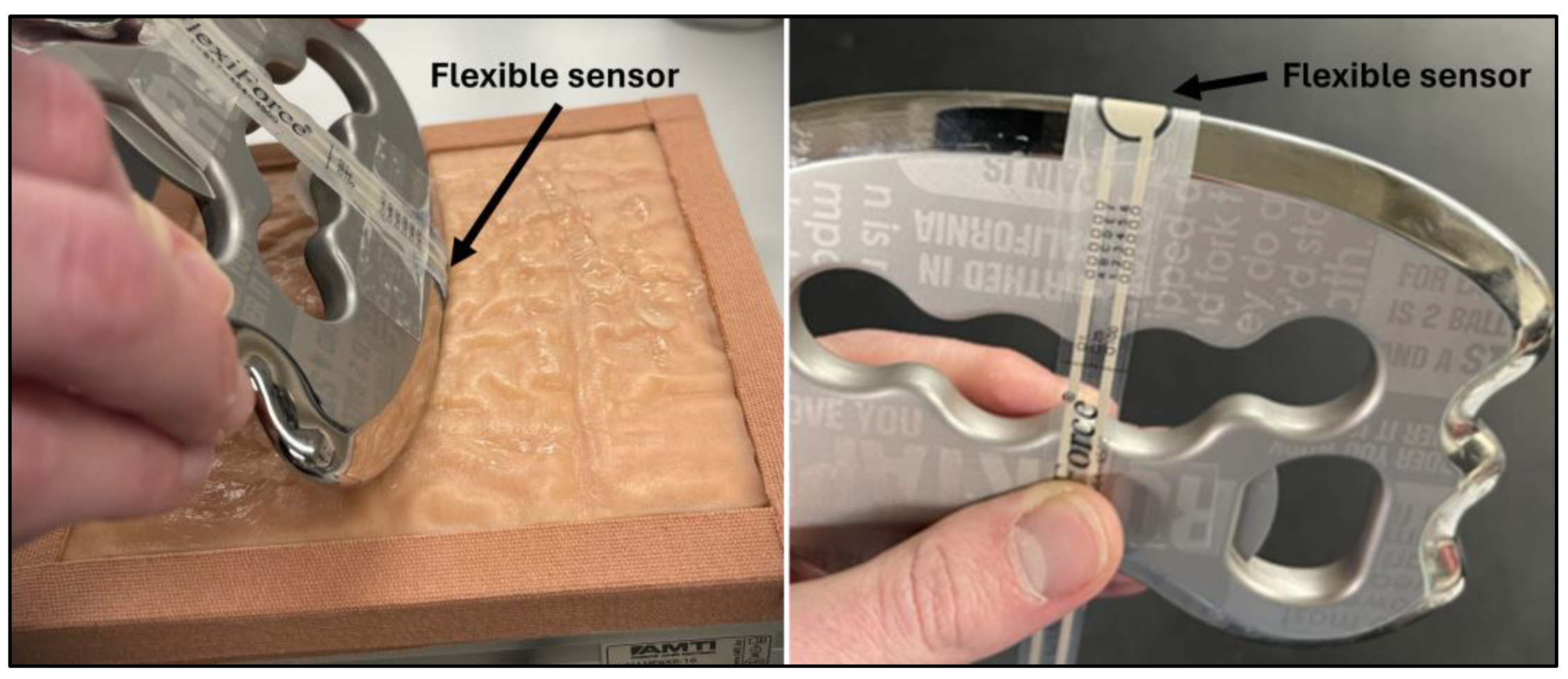
2.2. Instrumentation
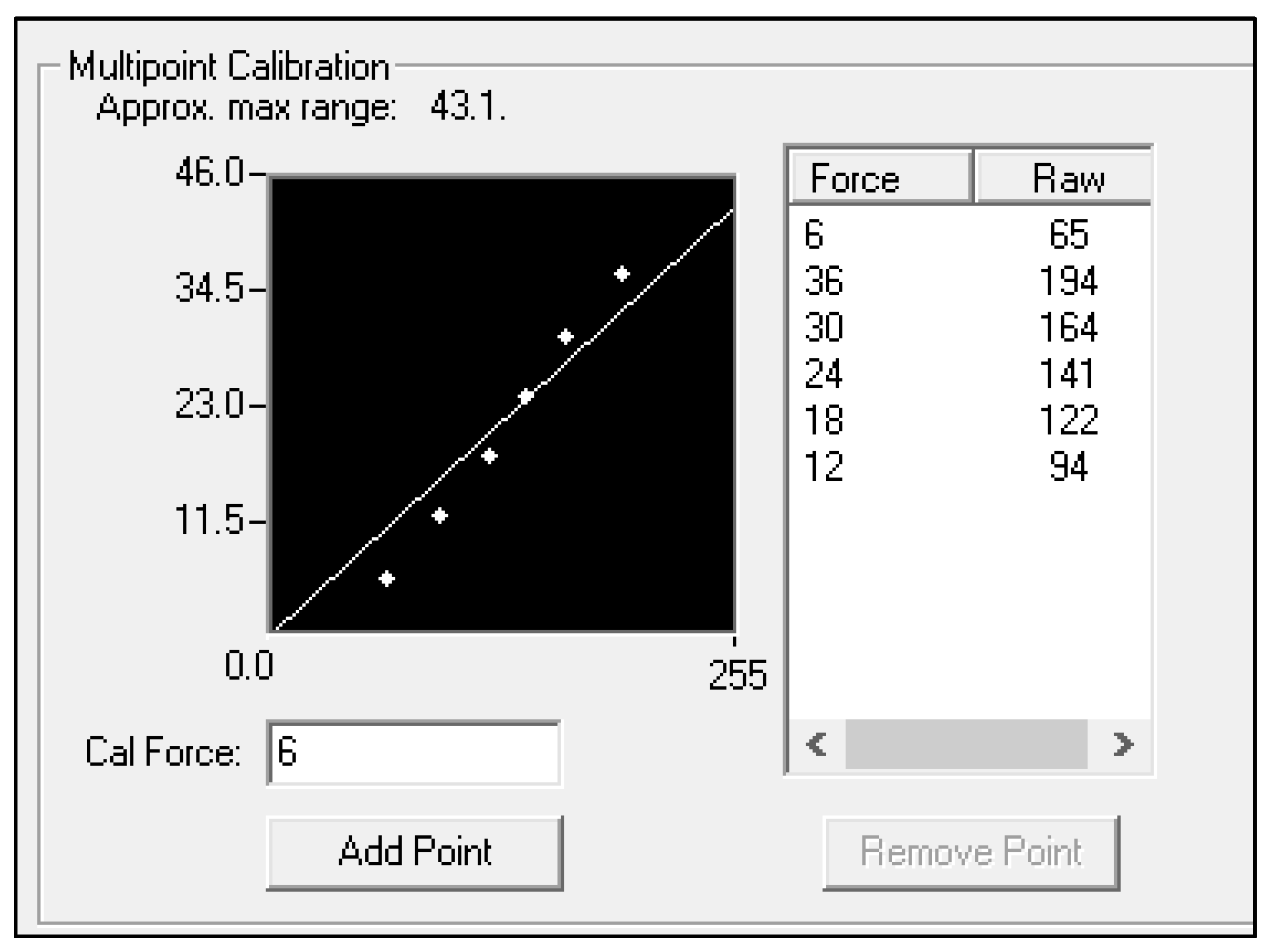
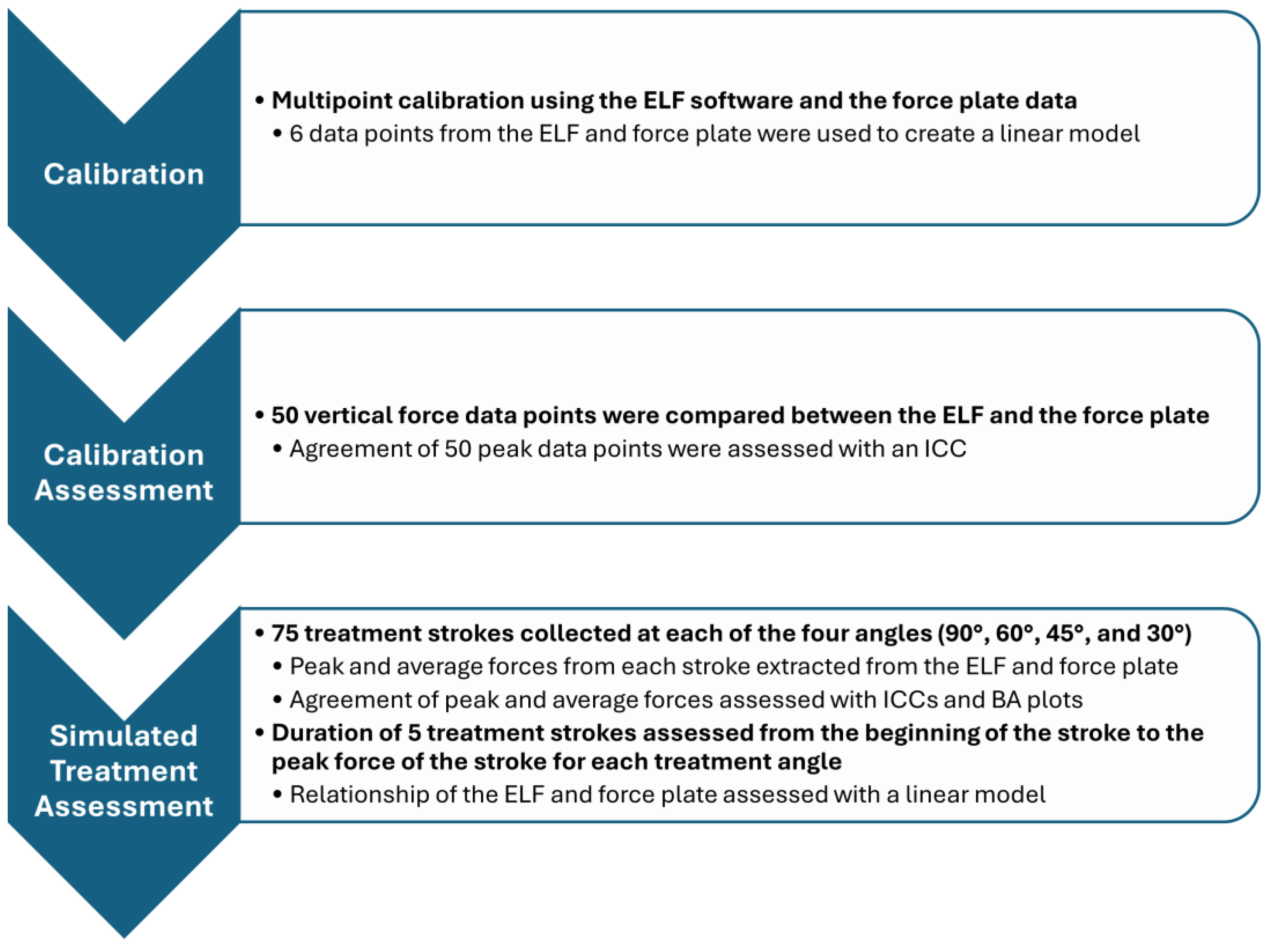
2.3. Calibration Assessment
2.4. Simulated Treatment Assessment
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Loghmani, T.; Whitted, M. Soft tissue manipulation: A powerful form of mechanotherapy. Physiother Rehabil. 2016, 1, 1000122. [Google Scholar] [CrossRef]
- Gulick, D.T. Instrument-assisted soft tissue mobilization increases myofascial trigger point pain threshold. J. Bodyw. Mov. Ther. 2018, 22, 341–345. [Google Scholar] [CrossRef]
- Fousekis, K.; Mylonas, K.; Charalampopoulou, V. Aggressive massage techniques can accelerate safe return after hamstrings strain: A case study of a professional soccer player. J. Sports Med. Doping Stud. 2013, 4, 2161-0673. [Google Scholar] [CrossRef]
- Bush, H.M.; Stanek, J.M.; Wooldridge, J.D.; Stephens, S.L.; Barrack, J.S. Comparison of the Graston Technique® with instrument-assisted soft tissue mobilization for increasing dorsiflexion range of motion. J. Sport Rehabil. 2021, 30, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Baker, R.T.; Start, A.; Larkins, L.; Burton, D.; May, J. Exploring the preparation, perceptions, and clinical profile of athletic trainers who use instrument-assisted soft tissue mobilization. Athl. Train. Sports Health Care 2018, 10, 169–180. [Google Scholar] [CrossRef]
- Koumantakis, G.A.; Roussou, E.; Angoules, G.A.; Angoules, N.A.; Alexandropoulos, T.; Mavrokosta, G.; Nikolaou, P.; Karathanassi, F.; Papadopoulou, M. The immediate effect of IASTM vs. Vibration vs. Light Hand Massage on knee angle repositioning accuracy and hamstrings flexibility: A pilot study. J. Bodyw. Mov. Ther. 2020, 24, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Cheatham, S.W.; Martonick, N.; Krumpl, L.; Baker, R.T. The effects of light pressure instrument-assisted soft tissue mobilization at different rates on grip strength and muscle stiffness in healthy individuals. J. Sport Rehabil. 2023, 32, 731–773. [Google Scholar] [CrossRef] [PubMed]
- Nazari, G.; Bobos, P.; MacDermid, J.C.; Birmingham, T. The effectiveness of instrument-assisted soft tissue mobilization in athletes, participants without extremity or spinal conditions, and individuals with upper extremity, lower extremity, and spinal conditions: A systematic review. Arch. Phys. Med. Rehabil. 2019, 100, 1726–1751. [Google Scholar] [CrossRef] [PubMed]
- Seffrin, C.B.; Cattano, N.M.; Reed, M.A.; Gardiner-Shires, A.M. Instrument-assisted soft tissue mobilization: A systematic review and effect-size analysis. J. Athl. Train. 2019, 54, 808–821. [Google Scholar] [CrossRef] [PubMed]
- Lambert, M.; Hitchcock, R.; Lavallee, K.; Hayford, E.; Morazzini, R.; Wallace, A.; Conroy, D.; Cleland, J. The effects of instrument-assisted soft tissue mobilization compared to other interventions on pain and function: A systematic review. Phys. Ther. Rev. 2017, 22, 76–85. [Google Scholar] [CrossRef]
- Cheatham, S.W.; Kreiswirth, E.; Baker, R.; Professor, A. Does a light pressure instrument assisted soft tissue mobilization technique modulate tactile discrimination and perceived pain in healthy individuals with DOMS? J. Can. Chiropr. Assoc. 2019, 63, 1. [Google Scholar]
- Vardiman, J.P.; Siedlik, J.; Herda, T.; Hawkins, W.; Cooper, M.; Graham, Z.A.; Deckert, J.; Gallagher, P. Instrument-assisted soft tissue mobilization: Effects on the properties of human plantar flexors. Int. J. Sports Med. 2015, 36, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Martonick, N.J.; Reeves, A.J.; Whitlock, J.A.; Stevenson, T.C.; Cheatham, S.W.; McGowan, C.P.; Baker, R.T. Instrument-Assisted Soft Tissue Mobilization Forces Applied by Trained Clinicians During a Simulated Treatment. J. Sport Rehabil. 2021, 31, 120–124. [Google Scholar] [CrossRef]
- Martonick, N.J.; North, K.; Reeves, A.; McGowan, C.; Baker, R.T. Effect of instrument type and one-handed versus two-handed grips on force application during simulated instrument-assisted soft tissue mobilisation. BMJ Open Sport Exerc. Med. 2023, 9, e001483. [Google Scholar] [CrossRef] [PubMed]
- Duffy, S.; Martonick, N.; Reeves, A.; Cheatham, S.W.; McGowan, C.; Baker, R.T. Clinician reliability of one-handed instrument-assisted soft tissue mobilization forces during a simulated treatment. J. Sport Rehabil. 2022, 31, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Everingham, J.B.; Martin, P.T.; Lujan, T.J. A hand-held device to apply instrument-assisted soft tissue mobilization at targeted compression forces and stroke frequencies. J. Med. Devices 2019, 13, 0145041. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjee, A.; Chien, S.Y.P.; Anwar, S.; Loghmani, M.T. Quantifiable Soft Tissue Manipulation (QSTMTM)—A novel modality to improve clinical manual therapy with objective metrics. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Virtual, 1–5 November 2021; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2021; pp. 4961–4964. [Google Scholar]
- Alotaibi, A.M.; Anwar, S.; Loghmani, M.T.; Chien, S. Force sensing for an instrument-assisted soft tissue manipulation device. J. Med. Devices 2017, 11, 031012. [Google Scholar] [CrossRef]
- Bhattacharjee, A.; Anwar, S.; Chien, S.; Loghmani, M.T. A handheld quantifiable soft tissue manipulation device for tracking real-time dispersive force-motion patterns to characterize manual therapy treatment. IEEE Trans. Biomed. Eng. 2023, 70, 1553–1564. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Zeng, H.; Best, T.M.; Haas, C.; Heffner, N.T.; Agarwal, S.; Zhao, Y. A mechatronic system for quantitative application and assessment of massage-like actions in small animals. Ann. Biomed. Eng. 2014, 42, 36–49. [Google Scholar] [CrossRef] [PubMed]
- Zeng, H.; Butterfield, T.A.; Agarwal, S.; Haq, F.; Best, T.M.; Zhao, Y. An engineering approach for quantitative analysis of the lengthwise strokes in massage therapies. J. Med. Devices 2008, 2, 041003. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Haghayegh, S.; Kang, H.-A.; Khoshnevis, S.; Smolensky, M.H.; Diller, K.R. A comprehensive guideline for Bland–Altman and intra class correlation calculations to properly compare two methods of measurement and interpret findings. Physiol. Meas. 2020, 41, 055012. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, S.; Nagi, S.S.; McGlone, F.; Mahns, D.A. Psychophysical investigations into the role of low-threshold c fibres in non-painful affective processing and pain modulation. PLoS ONE 2015, 10, e0138299. [Google Scholar] [CrossRef] [PubMed]
- Olson, W.; Dong, P.; Fleming, M.; Luo, W. The specification and wiring of mammalian cutaneous low-threshold mechanoreceptors. Wiley Interdiscip. Rev. Dev. Biol. 2016, 5, 389–404. [Google Scholar] [CrossRef] [PubMed]
- Speicher, T.E.; Selkow, N.M.; Warren, A.J. Manual Therapy Improves Immediate Blood Flow and Tissue Fiber Orientation of the Forearm Extensors. J. Phys. Med. Rehabil. 2022, 4, 28–36. [Google Scholar] [CrossRef]
- Coviello, J.P.; Kakar, R.S.; Reynolds, T.J. Short-term effects of instrument assisted soft tissue mobilization on pain free range of motion in a weightlifter with subacromial pain syndrome. Int. J. Sport Phys. Ther. 2017, 12, 144–154. [Google Scholar]
- Hammer, W.I. The effect of mechanical load on degenerated soft tissue. J. Bodyw. Mov. Ther. 2008, 12, 246–256. [Google Scholar] [CrossRef] [PubMed]
- Loghmani, M.T.; Warden, S.J. Instrument-assisted cross fiber massage increases tissue perfusion and alters microvascular morphology in the vicinity of healing knee ligaments. BMC Complement. Altern. Med. 2013, 13, 240. [Google Scholar] [CrossRef]
- Loghmani, M.T.; Warden, S.J. Instrument-assisted cross-fiber massage accelerates knee ligament healing. J. Orthop. Sports Phys. Ther. 2009, 39, 506–514. [Google Scholar] [CrossRef]
- Davidson, C.; Ganion, L.; Gehlsen, G.; Verhoestra, B.; Roepke, J.; Sevier, T. Rat tendon morphologic and functional changes resulting from soft tissue mobilization clinical sciences: Clinically relevant. Med. Sci. Sports Exerc. 1997, 29, 313–319. [Google Scholar] [CrossRef]
- Ikeda, N.; Otsuka, S.; Kawanishi, Y.; Kawakami, Y. Effects of instrument-assisted soft tissue mobilization on musculoskeletal properties. Med. Sci. Sports Exerc. 2019, 51, 2166–2172. [Google Scholar] [CrossRef] [PubMed]
- Melia, M.; Geissler, B.; König, J.; Ottersbach, H.J.; Umbreit, M.; Letzel, S.; Muttray, A. Pressure pain thresholds: Subject factors and the meaning of peak pressures. Eur. J. Pain 2019, 23, 167–182. [Google Scholar] [CrossRef] [PubMed]
- Persson, A.; Brogårdh, C.; Sjölund, B. Tender or not tender: Test-retest repeatability of pressure pain thresholds in the trapezius and deltoid muscles of healthy women. J. Rehabil. Med. 2004, 36, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Fousekis, K.; Varda, C.; Mandalidis, D.; Mylonas, K.; Angelopoulos, P.; Koumoundourou, D.; Tsepis, E. Effects of instrument-assisted soft-tissue mobilization at three different application angles on hamstring surface thermal responses. J. Phys. Ther. Sci. 2020, 32, 506–509. [Google Scholar] [CrossRef] [PubMed]
- Portillo-Soto, A.; Eberman, L.E.; Demchak, T.J.; Peebles, C. Comparison of blood flow changes with soft tissue mobilization and massage therapy. J. Altern. Complement. Med. 2014, 20, 932–936. [Google Scholar] [CrossRef] [PubMed]
- Laudner, K.; Compton, B.D.; A McLoda, T.; Walters, C.M. Acute effects of instrument assisted soft tissue mobilization for improving posterior shoulder range of motion in collegiate baseball players. Int. J. Sport Phys. Ther. 2014, 9, 1–7. [Google Scholar]
- Brimacombe, J.M.; Wilson, D.R.; Hodgson, A.J.; Ho, K.C.T.; Anglin, C. Effect of calibration method on tekscan sensor accuracy. J. Biomech. Eng. 2009, 131, 034503. [Google Scholar] [CrossRef] [PubMed]
- Parmar, S.; Khodasevych, I.; Troynikov, O. Evaluation of flexible force sensors for pressure monitoring in treatment of chronic venous disorders. Sensors 2017, 17, 1923. [Google Scholar] [CrossRef] [PubMed]
- Cordovani, D.; Russell, T.; Wee, W.; Suen, A.; Cooper, R.M. Measurement of forces applied using a Macintosh direct laryngoscope compared with a Glidescope video laryngoscope in patients with predictors of difficult laryngoscopy: A randomised controlled trial. Eur. J. Anaesthesiol. 2019, 36, 221–226. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Angle | Peak Forces | Average Forces | ||
|---|---|---|---|---|
| ICC (CIs) | Mean Diff. (LOA) (N) | ICC (CIs) | Mean Diff. (LOA) (N) | |
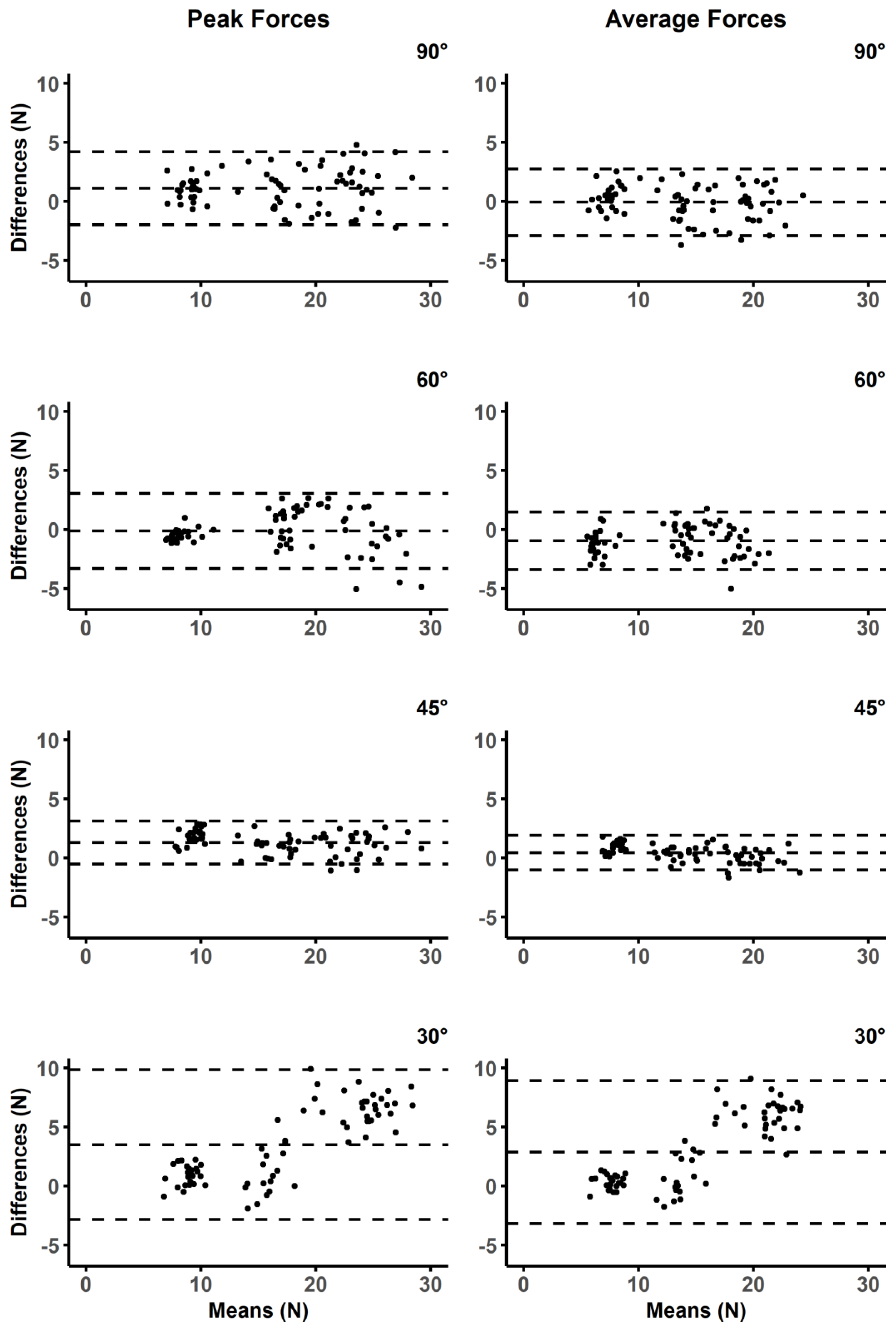
| 90 | 0.95 (0.86−0.98) | 1.10 (−1.89, 4.19) | 0.97 (0.94−0.98) | −0.06 (−2.89, 2.75) |
| 60 | 0.97 (0.95−0.98) | −0.12 (−3.30, 3.04) | 0.95 (0.82−0.98) | −0.95 (−3.40, 1.48) |
| 45 | 0.97 (0.49−0.99) | 1.29 (−0.53, 3.11) | 0.98 (0.96−0.99) | 0.44 (−1.03, 1.91) |
| 30 | 0.80 (0.18−0.92) | 3.49 (−2.84, 9.83) | 0.80 (0.31−0.92) | 2.87 (−3.16, 8.91) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martonick, N.J.P.; Baker, R.T.; McGowan, C.P. Implementing A Flexible Sensor to Identify Forces during Instrument-Assisted Soft Tissue Mobilization. BioMed 2024, 4, 100-111. https://doi.org/10.3390/biomed4020008
Martonick NJP, Baker RT, McGowan CP. Implementing A Flexible Sensor to Identify Forces during Instrument-Assisted Soft Tissue Mobilization. BioMed. 2024; 4(2):100-111. https://doi.org/10.3390/biomed4020008
Chicago/Turabian StyleMartonick, Nickolai J. P., Russell T. Baker, and Craig P. McGowan. 2024. "Implementing A Flexible Sensor to Identify Forces during Instrument-Assisted Soft Tissue Mobilization" BioMed 4, no. 2: 100-111. https://doi.org/10.3390/biomed4020008
APA StyleMartonick, N. J. P., Baker, R. T., & McGowan, C. P. (2024). Implementing A Flexible Sensor to Identify Forces during Instrument-Assisted Soft Tissue Mobilization. BioMed, 4(2), 100-111. https://doi.org/10.3390/biomed4020008