1. Introduction
Fibromyalgia (FM) is a complex condition characterized by chronic pain, fatigue, sleep disorders, cognitive impairments, and other somatic symptoms [
1]. FM falls under the category of medically unexplained functional somatic syndromes and is considered a somatization disorder [
2]. The exact classification of FM remains imprecise [
2,
3]. Individuals with FM experience widespread chronic pain throughout the musculoskeletal system [
4] and often exhibit central physical sensitivity and persistent pain [
5,
6]. Chronic pain, which persists or recurs for over three months, is a primary feature of FM [
7]. It is recognized as “chronic primary pain” and is considered a separate condition [
8]. FM is associated with neurosensitivity and reduced conditioned pain modulation (CPM) [
9]. The concept of nociplastic pain arises from the understanding that nociception changes within the peripheral and central nervous system can lead to pain even without evidence of tissue damage or disease [
10,
11].
The prevalence of FM in the general population ranges from 0.2% to 6.6%, with higher rates among women (2.4–6.8%) [
12]. The prevalence of FM symptoms among female teachers in Israel was 11.4%, significantly higher than the rate among male teachers (1.5%) [
13]. While the exact etiology of FM remains unclear, trauma is recognized as a significant risk factor. FM patients commonly experience symptoms of post-traumatic stress disorder (PTSD) [
14]. Early adverse experiences or prolonged traumatic stress in adulthood can affect the central nervous system circuits involved in pain regulation and stress response, potentially contributing to increased pain sensitivity in FM [
15,
16].
1.1. The Effect of Exposure to a Security Threat on FM Patients
This paper focuses on the coping strategies of female FM patients (FFMPs) who live in the Gaza Envelope in southern Israel, which is exposed to security threats. The effects of the security threats on residents in this region range from mild stress reactions to severe stress reactions, such as mood changes, hyper-arousal, anxiety, depression, and psychological distress, and somatic symptoms, such as muscular pain and symptoms of joint inflammation [
17,
18]. Ablin et al. [
19] have found that there are more FM patients in the Gaza Strip than in other areas of the country and that the security threat has real physical consequences for FM patients. The diagnosis of FM is usually clinical, and doctors often treat the pain symptoms rather than the causes of the disease. FM patients’ main challenge is managing the disease, and coping resources and strategies are essential issues [
5,
20].
1.2. The Salutogenic Theory
Salutogenesis, a term coined by Aaron Antonovsky [
21], proposes that life experiences contribute to shaping one’s SoC. Antonovsky’s salutogenic theory suggests that developing a sense of coherence is a resilience factor in coping with stressful situations, reducing stress reactions, and maintaining physical and mental health against negative experiences. SoC is the central concept in the salutogenic model and is perceived as an internal coping resource that enables a person to cope positively with stress and maintain mental and physical health [
22,
23]. SoC provides the basis for mobilizing and activating coping resources, which is essential in promoting health and developing resistance and resilience [
24]. Salutogenesis is a conceptual framework for studies investigating internal coping resources that enable individuals such as FFMPs to cope optimally with their syndrome [
25].
1.3. Resilience
Resilience is a multifaceted construct that encompasses various psychological and social dimensions. It has been recognized as a pivotal concept in human development and developmental psychopathology [
26]. Resilience is characterized by positive adaptation patterns in the face of adversity and stressful life events [
27,
28]. Its conceptualization is grounded in the notion that individuals can withstand the impact of significant risk factors and adverse experiences without suffering from detrimental outcomes or deviating from their expected developmental trajectory [
29]. Furthermore, resilience implies that individuals can recover and return to their prior level of functioning, with or without external support, following a setback or developmental crisis.
1.4. Coping Strategies in Stressful Situations
Coping involves cognitive and behavioral efforts to manage or tolerate internal or external demands caused by a stressful event or situation. Coping strategies are influenced by an individual’s appraisal of a situation as a threat or challenge and the perception of internal and external resources [
30,
31]. The study focuses on three coping strategies: problem-oriented coping, emotion-oriented coping, and avoidant coping. Problem-oriented coping aims to solve or change the source of the stress and includes coping planning and actions to manage the situation. Emotion-oriented coping is maladaptive and can lead to mental health problems. In contrast, avoidant coping involves disengagement behavior and denial [
32]—internal resources such as a sense of coherence (SoC) and resilience influence coping strategies. Positive health outcomes were associated with problem-oriented coping, while negative health outcomes were linked with emotion-oriented and avoidant coping strategies [
33,
34].
We posit that an intervention program has the potential to enhance focused coping mechanisms in dealing with challenges in FFMPs. Following recent studies that have found the potential for promoting resilience [
35,
36,
37] and a sense of coherence [
38,
39] through intervention programs, we aimed to investigate whether a specialized intervention program tailored for FFMPs would impact their coping patterns, thereby enhancing resilience and SoC in the face of the challenges experienced by these patients. In the current study, we have chosen to concentrate on the fibrotherapy intervention program (FTI) which was developed at the Ezra Le’Marpe (Help for Healing) Rehabilitation Medical Center, headed by Rabbi Avraham Elimelech Firer. The program helps FFMPs through holistic body and mind treatment. It combines physical therapy, Pilates, hydrotherapy, emotional response in therapeutic groups, gardening, cooking therapy, and a ceramics workshop that summarizes the process that FFMPs go through.
From this, the following hypotheses have emerged:
The study hypotheses
H1: Following the FTI program, a positive relationship will be found between problem-focused coping and the SoC, so a high tendency to use a problem-focused coping strategy will be expressed in an increasing SoC.
H2: Following the FTI program, a negative relationship will be found between the SoC and the level of symptoms of the disease; the higher the SoC, the less the psychological distress, the physiological indices (increase in endurance), and the functional difficulty.
H3: Following the FTI program, a positive relationship will be found between problem-focused coping and resilience, so a high tendency to use a problem-focused coping strategy will increase resilience.
H4: Following the FTI program, a negative relationship will be found between resilience and the level of symptoms of the disease; the higher the resilience, the less the psychological distress, the physiological indices (increase in endurance), and the functional difficulty.
2. Materials and Methods
A total of 96 female FM patients aged 19–75 residing in the Gaza Envelope area who received fibrotherapy intervention at the Medical Rehabilitation Center Ezra Le’Marpe in 2020 were recruited to participate in the study. The socio-demographic characteristics of the sample are presented in
Table 1. To be eligible for the study, participants needed to meet the following criteria: (1) medical diagnosis by a physician of FM for at least one year; (2) age between 19 and 75; (3) Jewish women who speak Hebrew to minimize the potential for data bias resulting from language and cultural differences; and (4) due to confidentiality and accessibility issues, it was more realistic to approach patients who were treated at the Ezra Le’Marpe Rehabilitation Medical Center. The sample was selected based on convenience, and the data collection process was concluded after reaching 100 subjects.
All methods were performed in accordance with the relevant guidelines and regulations. We confirm that all experimental protocols have been approved by an institutional and/or licensing committee on behalf of the Ariel University Ethics Committee. Informed consent was obtained from all subjects.
2.1. Tools
The quantitative data collection process was carried out in two stages: at the beginning and end. At each stage, we distributed 96 questionnaires (a total of 192 questionnaires).
2.2. Socio-Demographic Data
The questionnaires included socio-demographic variables: age, socio-economic status, religious belief, and degree of proximity to the Gaza Strip. In addition, the questionnaires included the number of years since the diagnosis of FM.
2.3. Brief COPE
The Brief COPE [
40] questionnaire was designed to examine coping tendencies. The reliability measures in similar studies were as follows: problem-oriented α = 0.85; emotion-oriented α = 0.67; avoidance α = 0.65 [
41].
2.4. Sense of Coherence Scale
The SoC questionnaire [
22] was administered in its abbreviated version with 13 items with predictive validity [
26]. The reliability in similar studies was α = 0.85 [
42].
2.5. CD-RISC-10 Scale
The original Connor–Davidson [
28] resilience scale was shortened to 10 items by Campbell-Sills and Stein [
43]. The internal reliability of the original Connor–Davidson study was α = 0.89.
2.6. Health Survey (SF-36)
The SF-36 questionnaire was tested and validated by Lewin-Epstein et al. [
44], with the Cronbach’s alpha coefficient of its dimensions ranging from 0.76 to 0.93.
2.7. The Scale of Psychological Distress
The questionnaire was developed initially by Ben-Sira [
45], with a shortened version of the questionnaire adapted by Sagy and Dotan [
46]. The questionnaire contains five items from the Langer index [
47] to measure psychological balance. The reliability in similar studies was α = 0.75.
2.8. Exposure to Stressful Events
The five-item questionnaire was designed to build an index of the level of exposure by combining the items [
42].
2.9. Fibromyalgia Impact Questionnaire—Revised (FIQR)
The FIQR questionnaire examined FM symptoms. A previous study revealed a reliability of α = 0.95 [
48].
2.10. The 6MW Test
The primary variable measured is the total distance the FMP walked. The 6MW test provides information that may better measure a patient’s ability to perform daily activities as a correlate of standard quality of life [
49].
2.11. Intervention Program: The Fibrotherapy Model
Table 2 describes the FTI, which is carried out in three rounds of 10 weeks each, and at each stage, the patient receives a different set of 3 therapy sessions per week (for a total of 30 weeks).
2.12. Data Analysis
The data obtained from the questionnaires were coded in SPSS software. The testing of the hypotheses was first carried out through correlations by Pearson tests regarding the research variables among the entire sample. Later, regressions were conducted for each of the dependent variables. Subjects who did not respond to certain variables were not included in the analyses referring to these variables.
3. Results
Table 3 presents the change levels of coping patterns, problem-oriented patterns, psychological distress, functional ability, physiological scales, and SoC after the intervention program.
The distribution of change levels of coping patterns after the intervention program, which was published previously by the authors of this paper [
52,
53], shows that before and after the intervention, about two-thirds consistently used problem-oriented coping and one-third shifted from avoidant or emotion-oriented coping to problem-oriented coping after the program. Those who used problem-oriented coping showed reduced psychological distress post-intervention, and their health-related quality of life notably improved. Participants who did not employ problem-oriented coping did not significantly reduce psychological distress, and no notable improvement in health-related quality of life was found. All the participants showed an increase in a distance scale pre-exertion. Findings also showed mixed changes in physiological scales, with some decreases and increases post-intervention. Overall, problem-oriented coping was associated with positive changes in psychological distress, functional ability, and some physiological measures post-intervention. In contrast, non-problem-oriented coping showed mixed results in these areas.
The mean differences in SoC before and after FTI according to the level of change in coping patterns, which were published previously by the authors of this paper [
53], are presented in
Table 3. The findings supported our second hypothesis and showed a significant difference in the level of SoC resilience among problem-oriented FFMPs before and after participating in FTI (t (55) = 2.46,
p = 0.02), as this group reported a higher level of SoC following FTI. There was no significant difference in the level of SoC before and after participating in FTI among FFMPs who did not use problem-oriented coping [
53].
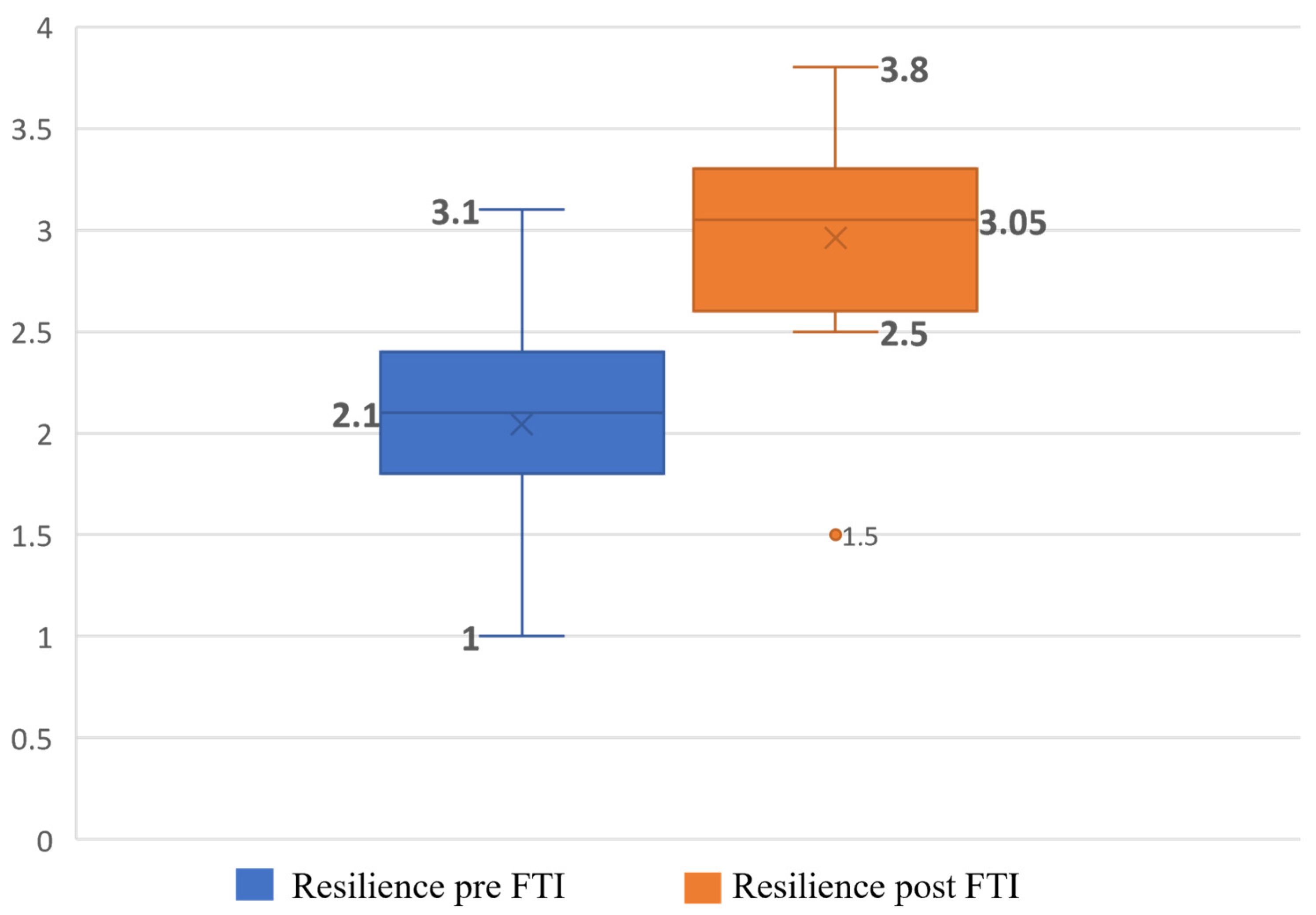
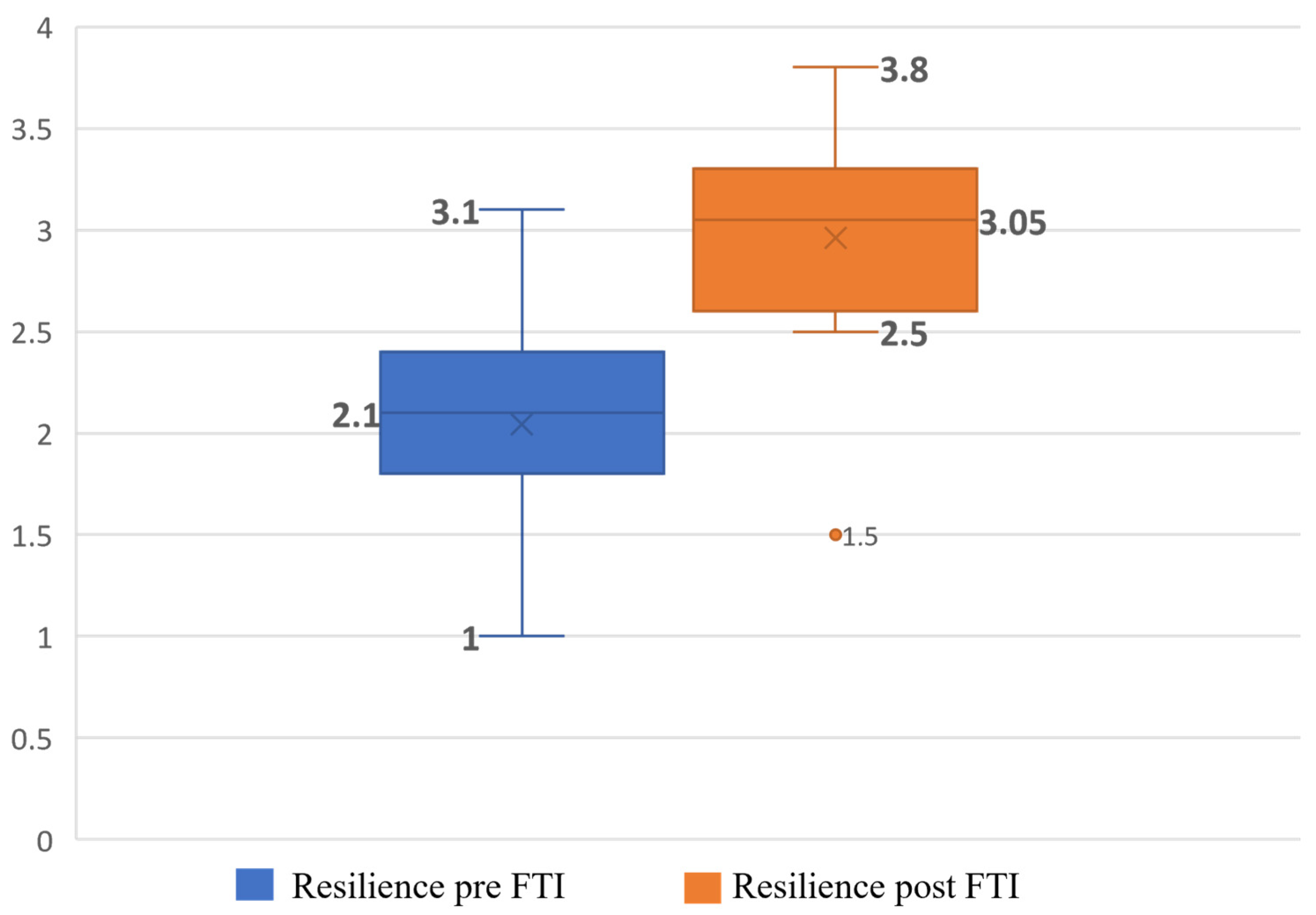
Analysis of the distribution of resilience data before and after participation in FTI among problem-oriented FFMPs showed a significant improvement in the level of resilience among problem-oriented FFMPs (t (55) = 9.38,
p < 0.001), as this group reported a higher level of resilience following FTI (M = 2.96, SD = 0.50) compared to the level of resilience before participating in FTI (M = 2.04, SD = 0.58). The extent of the effect between the two measurement dates was high (Cohen’s d = 1.68) [
54] (
Figure 1).
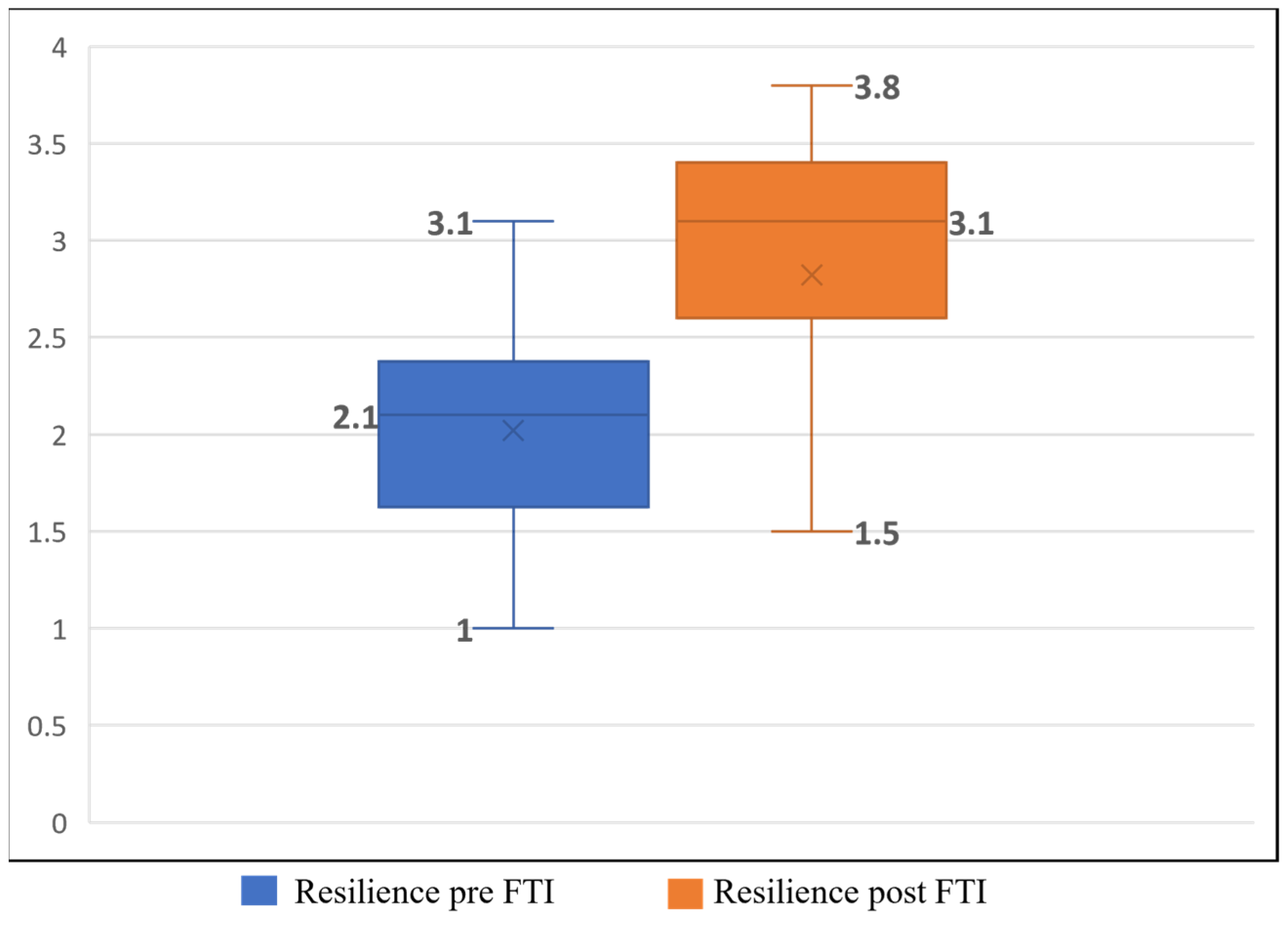
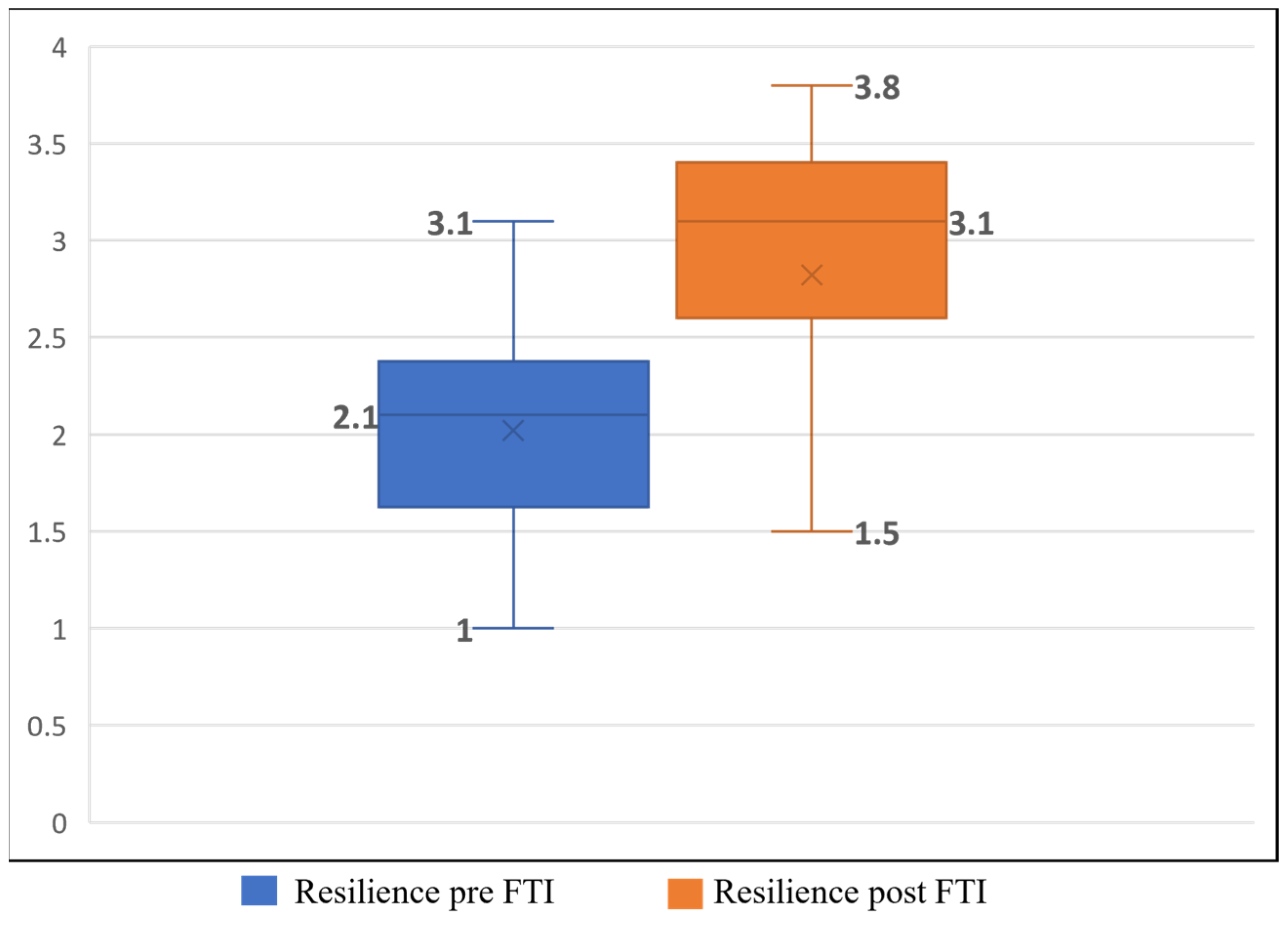
Analysis of the distribution of resilience data before and after participation in FTI among FFMPs who did not use problem-oriented coping showed a significant improvement in levels of resilience (t (39) = 5.05,
p < 0.001), as this group reported a higher level of resilience following FTI (M = 2.82, SD = 0.74) compared to the level of resilience before participating in FTI (M = 2.02, SD = 0.62). The extent of the effect between the two measurement dates was high (Cohen’s d = 1.16) [
54] (
Figure 2). We found that participation in FTI improved the level of resilience among the study subjects, problem-oriented and non-problem-oriented FFMPs. However, the effect size index significantly improved among problem-oriented FFMPs. Hence, our third hypothesis was confirmed.
4. Discussion
This paper examined how coping strategies affect the SoC and resilience levels among FFMPs under a prolonged security threat after participating in the FTI program. research [
52,
53] also established a link between stressful situations, such as security threats, and intensified FM symptoms. Qualitative findings from elaborate research by the authors of this paper [
54,
55,
56] revealed physical conditions among FFMPs under security threats that included pain and stiffness during sirens to the point of entering a state of physical paralysis for hours after the threat had passed. Findings from these studies suggest that FFMPs transitioning from emotion-oriented or avoidance coping to problem-oriented strategies during FTI demonstrated significant improvement.
The secondary outcomes of our study show that problem-oriented coping involves adapting to stressors by modifying difficulties due to chronic illness, leading to a better quality of life.
Previous analyses [
54,
55,
56] revealed that participation in FTI group therapy fostered attitude changes, transforming feelings of isolation into shared experiences and common goals among FFMPs. This shift from individual coping to collective participation led to increased optimism and a more assertive approach to managing the disease. In addition, problem-oriented coping post-FTI correlated with reduced psychological distress, improved physiological measures, and enhanced functional ability, indicating comprehensive health enhancement. According to Paterson [
57], the perception of reality provides the basis for the way people with chronic illness interpret and cope with their illness. Most treatments for FM patients address pain, imbalance, and sleep disorders. However, a few studies proposed to follow a program for resilience and sense of coherence among patients [
58,
59].
Patients who have developed or use problem-oriented coping patterns use what Antonovsky [
22,
25] called “generalized resistance resources” (GRRs), that is, the qualities or resources that provide support and assistance in coping with daily stressors. According to Shing et al. [
60], one major factor contributing to resilience is harnessing positive emotions, even during a difficult or stressful time. Positivity improves resilience in two main ways. First, positive emotions help construct social, psychological, and physical resources over time and develop coping skills for future times of stress. Second, according to Fredrickson’s broaden-and-build theory [
61], positive emotions can help people expand their thoughts, actions, and attention to the moments around them. Our data show that the level of mental resilience of the FFMPs increased following their participation in the FTI. This finding has great significance since “resilience” combines flexibility and the ability to return to life with elements related to accepting and adapting to change and coping with the consequences of FM. The more a person adapts, the higher their resilience level, allowing them to cope better with stressful situations [
62].
Our analysis revealed increased mental resilience among FFMPs following FTI participation, highlighting the significance of positivity and adaptability in coping with FM consequences. Problem-oriented coping led to higher levels of improvement, emphasizing the acquisition of coping resources and engagement in various proactive actions to manage FM. Contrary to Antonovsky’s [
21] claim that SoC develops between childhood and age 30 and is less likely to change after that, as can be established from previous studies [
63,
64], our data indicate that SoC increased following the FTI program.
The study’s primary focus was on how coping strategies, particularly problem-oriented coping, influenced SoC, resilience, and overall health outcomes among FFMPs in the context of prolonged security threats. The findings indicated substantial improvements across various health indicators post-FTI, particularly among those who adopted problem-oriented coping strategies.
5. Conclusions
The study highlighted the immense impact of FFMPs’ participation in FTI on transforming coping strategies. It notably shifted many women from disease preoccupation to active disease management. Through shared experiences in the program, FFMPs adopted problem-oriented coping, engaging in actions like physical exercises to enhance their quality of life despite the enigmatic nature of FM. Despite FM remaining a complex condition without definitive causes or diagnostic tests, our research demonstrated that FTI participation improved health. Emotional engagement during the program allowed participants to explore, discuss, and accept their condition, suggesting the scope for intervention programs to empower FFMPs and foster problem-oriented coping.
Moreover, participation in FTI enabled FFMPs to comprehend the disease’s significance, manage it effectively, and enhance their SoC. While empirical changes in SoC were lower than anticipated post-FTI, qualitative insights revealed substantial cognitive and behavioral shifts, emphasizing meaningfulness, understanding, and management of FM. This suggests the importance of comprehensively considering both emotional perceptions and empirical data in understanding chronic diseases.
Additionally, the study concluded that problem-oriented coping strategies facilitated the acquisition of resilience among participants. Facing and coping with challenges using this strategy reflected mental flexibility, aiding individuals in rebounding from setbacks and confronting life’s adversities. Furthermore, the research emphasized the pivotal role of physical activity in coping with FM symptoms, and engaging in purposeful physical activity, driven by the desire to manage the condition, notably improved health indicators despite the pervasive musculoskeletal pain experienced by FFMPs.
6. Limitations
The study included only female participants; thus, the results may not be generalized to male FM patients or patients from different cultural backgrounds. The study did not include a control group, making it difficult to determine whether the observed improvements were due to the intervention program or other factors.
Author Contributions
Conceptualization, L.C.-B. and R.N.-G.; methodology, L.C.-B.; software, L.C.-B.; validation, L.C.-B., R.N.-G. and D.B.; formal analysis, L.C.-B., D.B. and D.B.; investigation, L.C.-B.; resources, L.C.-B.; data curation, L.C.-B.; writing—original draft preparation, L.C.-B.; writing—review and editing, L.C.-B., D.B. and R.N.-G.; visualization, L.C.-B.; supervision, R.N.-G.; project administration, L.C.-B.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data supporting the findings of this study are available from the Ethics Committee of Ariel University. However, there are restrictions on the availability of these data, which were used under license for the current study and are therefore not publicly available. However, the data are available from the authors upon reasonable request and with the approval of the ethics committee. Also, some of the data form a basis for further research.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Bair, M.J.; Krebs, E.E. Fibromyalgia. Ann. Intern. Med. 2020, 172, ITC33–ITC48. [Google Scholar] [CrossRef]
- Häuser, W.; Fitzcharles, M.A. Facts and myths pertaining to fibromyalgia. Dialogues Clin. Neurosci. 2018, 20, 53–62. [Google Scholar] [CrossRef]
- Sumpton, J.E.; Moulin, D.E. Fibromyalgia. Handb. Clin. Neurol. 2014, 119, 513–527. [Google Scholar] [PubMed]
- Buskila, D.; Abramov, G.; Biton, A.; Neumann, L. The prevalence of pain complaints in a general population in Israel and its implications for utilization of health services. J. Rheumatol. 2000, 27, 1521–1525. [Google Scholar] [PubMed]
- Bellato, E.; Marini, E.; Castoldi, F.; Barbasetti, N.; Mattei, L.; Bonasia, D.E.; Blonna, D. Fibromyalgia syndrome: Etiology, pathogenesis, diagnosis, and treatment. Pain Res. Treat. 2012, 2012, 426130. [Google Scholar] [CrossRef] [PubMed]
- Adams, L.; Turk, D. Psychosocial factors and central sensitivity syndromes. Curr. Rheumatol. Rev. 2015, 11, 96–108. [Google Scholar] [CrossRef] [PubMed]
- Treede, R.D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. Chronic pain as a symptom or a disease: The IASP classification of chronic pain for the international classification of diseases (ICD-11). Pain 2019, 160, 19–27. [Google Scholar] [CrossRef]
- Alciati, A.; Nucera, V.; Masala, I.F.; Giallanza, M.; La Corte, L.; Giorgi, V.; Sarzi-Puttini, P.; Atzeni, F. One year in review 2021: Fibromyalgia. Clin. Exp. Rheumatol. 2021, 39, S-3–S-12. [Google Scholar] [CrossRef] [PubMed]
- Tzadok, R.; Ablin, J.N. Current and emerging pharmacotherapy for Fibromyalgia. Pain Res. Manag. 2020, 2020, 6541798. [Google Scholar] [CrossRef]
- Liptan, G.L. Fascia: A missing link in our understanding of the pathology of fibromyalgia. J. Bodyw. Mov. Ther. 2010, 14, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Trouvin, A.P.; Perrot, S. New concepts of pain. Best Pract. Res. Clin. Rheumatol. 2019, 33, 101415. [Google Scholar] [CrossRef]
- Marques, A.P.; De Sousa, A.; Santo, E.; Berssaneti, A.A.; Matsutani, L.A.; Lee, S. Prevalence of fibromyalgia: Literature review update. Rev. Bras. Reumatol. 2017, 57, 356–363. [Google Scholar] [CrossRef]
- Buskila, Y.; Buskila, D.; Jacob, G.; Ablin, J.N. High prevalence of fibromyalgia among Israeli school teachers. Clin. Exp. Rheumatol. 2019, 37, S21–S26. [Google Scholar]
- Whipple, M.; Toussaint, L.; Fleming, K.; Nanda, S.; Mohabbat, A.; Vincent, A. (221) Associations between post-traumatic stress disorder symptoms and mental health in fibromyalgia. J. Pain 2016, 17, S31. [Google Scholar] [CrossRef]
- Coppens, E.; Van Wambeke, P.; Morlion, B.; Weltens, N.; Giao Ly, H.; Tack, J.; Luyten, P.; Van Oudenhove, L. Prevalence and impact of childhood adversities and post-traumatic stress disorder in women with fibromyalgia and chronic widespread pain. Eur. J. Pain 2017, 21, 1582–1590. [Google Scholar] [CrossRef]
- Waller, E.; Scheidt, C.E.; Endorf, K.; Hartmann, A.; Zimmermann, P. Unresolved trauma in fibromyalgia: A cross-sectional study. J. Health Psychol. 2016, 21, 2457–2465. [Google Scholar] [CrossRef]
- Elran, M.; Israeli, T.; Padan, K.; Altchuler, A. Social resilience in the Jewish communities around the Gaza Strip Envelope during and after Operation Protective Edge. Mil. Strateg. Aff. 2015, 7, 5–26. [Google Scholar]
- Shpigelman, C.N.; Gelkopf, M. Psychological Impact of Exposure to War and Terrorism on Individuals with Physical or Sensory Disabilities; Haifa University: Haifa, Israel, 2016. [Google Scholar]
- Ablin, J.N.; Cohen, H.; Clauw, D.J.; Shalev, R.; Ablin, E.; Neumann, L.; Sarzi-Puttini, P.; Buskila, D. A Tale of Two Cities—The effect of low intensity conflict on prevalence and characteristics of musculoskeletal pain and somatic symptoms associated with chronic stress. Clin. Exp. Rheumatol. 2010, 28, S15–S21. [Google Scholar]
- Lerman, S.F.; Rudich, Z.; Shahar, G. Does war hurt? Effects of media exposure after missile attacks on chronic pain. J. Clin. Psychol. Med. Settings 2013, 20, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Antonovsky, A. Health, Stress, and Coping: New Perspectives on Mental and Physical Well-Being; The Jossey-Bass Social and Behavioral Science Series; Jossey-Bass: San Francisco, CA, USA, 1979. [Google Scholar]
- Antonovsky, A. Unraveling the Mystery of Health: How People Manage Stress and Stay Well; Jossey-Bass: San Francisco, CA, USA, 1987. [Google Scholar]
- Antonovsky, A. The salutogenic model as a theory to guide health promotion. Health Promot. Int. 1996, 11, 11–18. [Google Scholar] [CrossRef]
- Eriksson, M.; Lindström, B. Antonovsky’s sense of coherence scale and the relation with health: A systematic review. J. Epidemiol. Community Health 2006, 60, 376–381. [Google Scholar] [CrossRef]
- Antonovsky, A. The structure and properties of the sense of coherence scale. Soc. Sci. Med. 1993, 36, 725–733. [Google Scholar] [CrossRef]
- Greve, W.; Staudinger, U.M. Resilience in later adulthood and old age: Resources and potentials for successful aging. In Developmental Psychopathology: Risk, Disorder, and Adaptation, 2nd ed.; Cicchetti, D., Cohen, A., Eds.; Wiley & Sons, Inc.: Hoboken, NJ, USA, 2006; pp. 796–840. [Google Scholar]
- Patterson, J.M. Understanding family resilience. J. Clin. Psychol. 2002, 58, 233–246. [Google Scholar] [CrossRef]
- Connor, K.M.; Davidson, J.R.T. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Rutter, M. Psychosocial resilience and protective mechanisms. Am. J. Orthopsychiatry 1987, 57, 316–331. [Google Scholar] [CrossRef]
- Anshel, M.H.; Raviv, S.; Jamieson, J. Cognitive appraisals and coping strategies following acute stress among skilled competitive male and female athletes. J. Sport. Behav. 2001, 24, 128–134. [Google Scholar]
- Levy, A.R.; Nicholls, A.R.; Polman, R.C.J. Pre-competitive confidence, coping, and subjective performance in sport. Scand. J. Med. Sci. Sport. 2011, 21, 721–729. [Google Scholar] [CrossRef]
- Chen, Y.; Peng, Y.; Xu, H.; O’Brien, W.H. Age differences in stress and coping: Problem-focused strategies mediate the relationship between age and positive affect. Int. J. Aging Hum. Dev. 2018, 86, 347–363. [Google Scholar] [CrossRef]
- Penley, J.A.; Tomaka, J.; Wiebe, J.S. The association of coping to physical and psychological health outcomes: A meta-analytic review. J. Behav. Med. 2002, 25, 551–603. [Google Scholar] [CrossRef] [PubMed]
- Bennett, D.S.; Hersh, J.; Herres, J.; Foster, J. HIV-related stigma, shame, and avoidant coping: Risk factors for internalizing symptoms among youth living with HIV? Child. Psychiatry Hum. Dev. 2016, 47, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.J.W.; Ein, N.; Gervasio, J.; Battaion, M.; Reed, M.; Vickers, K. Comprehensive meta-analysis of resilience interventions. Clin. Psychol. Rev. 2020, 82, 101919. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Chi, I.; Zhan, Y.; Chen, W.; Li, T. Effectiveness of resilience interventions on psychosocial outcomes for persons with neurocognitive disorders: A systematic review and meta-analysis. Front. Psychiatry 2021, 12, 709860. [Google Scholar] [CrossRef] [PubMed]
- Chmitorz, A.; Kunzler, A.; Helmreich, I.; Tüscher, O.; Kalisch, R.; Kubiak, T.; Wessa, M.; Lieb, K. Intervention studies to foster resilience: A systematic review and proposal for a resilience framework in future intervention studies. Clin. Psychol. Rev. 2018, 59, 78–100. [Google Scholar] [CrossRef]
- Vastamäki, J.; Moser, K.; Paul, K.I. How stable is sense of coherence? Changes following an intervention for unemployed individuals. Scand. J. Psychol. 2009, 50, 161–171. [Google Scholar] [CrossRef]
- Langeland, E.; Vaandrager, L.; Nilsen, A.B.V.; Schraner, M.; Meier Magistretti, C. Effectiveness of interventions to enhance the sense of coherence in the life course. In The Handbook of Salutogenesis; Mittelmark, M.B., Bauer, G.F., Vaandrager, L., Pelikan, J.M., Sagy, S., Eriksson, M., Lindström, B., Magistretti, C.M., Eds.; Springer International Publishing: Berlin/Heidelberg, Germany, 2022; pp. 201–219. [Google Scholar]
- Carver, C.S. You want to measure coping but your protocol’s too long: Consider the brief COPE. Int. J. Behav. Med. 1997, 4, 92–100. [Google Scholar] [CrossRef]
- Sagi, S.; Braun-Lewensohn, A. Reactions to stressful situations and coping resources among adolescents under fire: A comparison between chronic and acute stressful situations. Megamot 2014, 49, 754–774. [Google Scholar]
- Braun-Lewensohn, O.; Celestin-Westreich, W.; Celestin, L.P.; Verté, D.; Ponjaert-Kristoffersen, I. Prevalence of post traumatic stress and emotional and behavioral problems among Israeli adolescents exposed to ongoing terrorism. Int. J. Psychol. Res. 2010, 5, 117–144. [Google Scholar]
- Campbell-Sills, L.; Stein, M.B. Psychometric analysis and refinement of the Connor-Davidson Resilience Scale (CD-RISC): Validation of a 10-item measure of resilience. J. Trauma Stress 2007, 20, 1019–1028. [Google Scholar] [CrossRef]
- Lewin-Epstein, N.; Sagiv-Schifter, T.; Shabtai, E.L.; Shmueli, A. Validation of the 36-Item Short-Form Health Survey (Hebrew Version) in the adult population of Israel. Med. Care 1998, 36, 1361–1370. [Google Scholar] [CrossRef]
- Ben-Sira, Z. A scale of psychological distress. Psychol. Res. Behav. Manag. 1979, 4, 337–356. [Google Scholar]
- Sagy, S.; Dotan, N. Coping resources of maltreated children in the family: A salutogenic approach. Child Abus. Negl. 2001, 25, 1463–1480. [Google Scholar] [CrossRef]
- Langer, P. Compulsivity and response set on the Structured Objective Rorschach Test. J. Clin. Psychol. 1962, 18, 299–302. [Google Scholar] [CrossRef]
- Bennett, R.M.; Friend, R.; Jones, K.D.; Ward, R.; Han, B.K.; Ross, R.L. The revised fibromyalgia impact questionnaire (FIQR): Validation and psychometric properties. Arthritis Res. Ther. 2009, 11, R120. [Google Scholar] [CrossRef]
- American Thoracic Society. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Jain, F.; Lenze, E.; Lavretsky, H. Advances in mind/body therapies: Concept, data and delivery. Am. J. Geriatr. Psychiatry 2023, 31, S13–S14. [Google Scholar] [CrossRef]
- Singh, S.; Rai, S.K.; Pndya, B.V.; Kumar, R. Yoga and Meditation, 1st ed.; AGPH Books: Bhopal, India, 2023. [Google Scholar]
- Compas, B.E.; Jaser, S.S.; Dunn, M.J.; Rodriguez, E.M. Coping with chronic illness in childhood and adolescence. Annu. Rev. Clin. Psychol. 2012, 8, 455–480. [Google Scholar] [CrossRef]
- Buskila, D.; Neumann, L.; Vaisberg, G.; Alkalay, D.; Wolfe, F. Increased rates of fibromyalgia following cervical spine injury: A controlled study of 161 cases of traumatic injury. Arthritis Rheum. 1997, 40, 446–452. [Google Scholar] [CrossRef]
- Cohen-Biton, L.; Buskila, D.; Nissanholtz-Gannot, R. Problem-oriented coping and resilience among Fibromyalgia patients who live under security threat and undergone Fibrotherapy intervention program. J. Psychosom. Res. 2023, in press. [CrossRef]
- Cohen-Biton, L.; Buskila, D.; Nissanholtz-Gannot, R. The correlation between problem-oriented coping and a sense of coherence among fibromyalgia patients who underwent the fibrotherapy model intervention program. Clin. Exp. Rheumatol. 2022, 40, 1143–1150. [Google Scholar] [CrossRef]
- Cohen-Biton, L.; Buskila, D.; Nissanholtz-Gannot, R. The effect of the Fibrotherapy intervention program on the coping patterns of fibromyalgia patients. J. Clin. Rheumatol. 2022, 28, 278–283. [Google Scholar] [CrossRef]
- Paterson, B.L. The shifting perspectives model of chronic illness. J. Nurs. Scholarsh. 2001, 33, 21–26. [Google Scholar] [CrossRef]
- Chiaramonte, R.; Bonfiglio, M.; Chisari, S. Multidisciplinary protocol for the management of fibromyalgia associated with imbalance. Our experience and literature review. Rev. Assoc. Med. Bras. 2019, 65, 1265–1274. [Google Scholar] [CrossRef]
- Turcotte, K.; Oelke, N.D.; Whitaker, G.; Holtzman, S.; O’Connor, B.; Pearson, N.; Teo, M. Multi-disciplinary community-based group intervention for fibromyalgia: A pilot randomized controlled trial. Rheumatol. Int. 2023, 43, 2201–2210. [Google Scholar] [CrossRef]
- Shing, E.Z.; Jayawickreme, E.; Waugh, C.E. Contextual positive coping as a factor contributing to resilience after disasters. J. Clin. Psychol. 2016, 72, 1287–1306. [Google Scholar] [CrossRef]
- Fredrickson, B.L. The broaden-and-build theory of positive emotions. Philos. Trans. R. Soc. B Biol. Sci. 2004, 359, 1367–1377. [Google Scholar] [CrossRef]
- Cabanyes Truffino, J. Resilience: An approach to the concept. Rev. Psiquiatr. Salud Ment. (Engl. Ed.) 2010, 3, 145–151. [Google Scholar] [CrossRef]
- Binder, H.P.; Mesenholl-Strehler, E.; Paß, P.; Christian Endler, P. Sense of Coherence (SOC) among psychotherapists in Austria, differentiated according to number of individually completed training therapy sessions. Sci. World 2006, 6, 2196–2199. [Google Scholar]
- Callahan, L.F.; Pincus, T. The sense of coherence scale in patients with rheumatoid arthritis. Arthritis Rheum. 1995, 8, 28–35. [Google Scholar] [CrossRef]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).




{kind=link}
{kind=link}