Abstract
Pandemic restrictions and reduced social opportunities led to increased loneliness in affected countries. Considering that stressful situations activate the attachment system and engage various coping strategies, the present study explored the role of attachment dimensions and coping styles in perceived social isolation and the subsequent effect on emotional distress. Data were collected using an online survey between the third and fourth waves in Romania during the second year of the pandemic. Correlational analyses presented significant relationships between all variables measured. Regression analysis showed that attachment insecurity could predict up to half of the variance in loneliness and one-third of emotional distress. Coping styles that predicted both loneliness and emotional distress were problem-focused and socially supported coping, though the effect was minimal. Emotion-focused coping presented a protective role against loneliness. Finally, mediation analysis revealed how loneliness fully mediated the relationship between insecure attachment styles and emotional distress. Further implications for research on loneliness and pandemic resilience are discussed.
1. Introduction
The emergence in late 2019 and rapid spread throughout 2020 of the SARS-CoV-2 virus has led to an unprecedented public health crisis in the modern world [1]. Despite the general availability of vaccines beginning in 2021, political, legislative, and societal factors contributed to pandemic fatigue and vaccine hesitancy during the second year of the pandemic [2]. This led to a third wave in spring 2021 and a catastrophic fourth one beginning in October 2021 [3], with the period in between characterized by fluctuating restrictions, partial lockdown measures, and uncertainty. Psychological distress is largely defined as a state of emotional suffering, characterized by symptoms of depression and anxiety [4], which can be tied to somatic symptoms (e.g., insomnia, headache) [5]. Studies measuring the psychological burden of the pandemic found high rates of depressive, anxious, and post-traumatic symptoms in the general population [6], along with pandemic-specific symptoms like worry regarding COVID-19 contagion [7]. Multiple studies have outlined the important effect on emotional well-being during and after the pandemic, with two meta-analyses during the pandemic reporting the prevalence of depression and anxiety in the population of nearly one-third [6,8] and a more recent one reporting a prevalence of depression of 15.97% and a prevalence of anxiety of 15.15% [9]. Emotional distress during the pandemic has been associated with low perceived social support, low emotional stability [10], and loneliness [11].
A pandemic’s psychological footprint could be more extensive than its medical one [12]. Even after restrictions were lifted in China, most people continued to self-isolate to some degree [13], and an increase in loneliness compared to pre-pandemic times was described in a meta-analysis [14]. While social isolation describes the objective absence of social interactions [15], loneliness refers to the subjective experience arising from the discrepancy between one’s desires and received social interactions [16]. Though conceptually separate constructs, objective and perceived social isolation are interrelated, with the former a risk factor for the latter [15,17]. Even before the full brunt of the pandemic, loneliness has been described as an epidemic affecting developed countries [18,19]. It has been identified as a risk factor for somatic illness [15,20,21], neurodegenerative symptoms [22], and psychiatric disorders [15,17]. A comparative analysis of loneliness throughout Europe found that former Soviet countries had an even higher incidence of loneliness than the rest of Europe in all age brackets [23]. This is important because the pandemic came superimposed on prior risk factors [24]. Compared to pre-pandemic times, some risk groups for loneliness remained the same (e.g., women living alone), other groups experienced greater risk (e.g., younger people), and groups that were previously safe became at-risk (e.g., students) [25]. A study undertaken during the COVID-19 pandemic in Israel found that loneliness was the main risk factor for depression and anxiety and their comorbidities, even when accounting for demographics, health-related factors, exposure to COVID-19-related events, and behavioral change [26].
Ainsworth and Bowlby’s attachment theory emerges as a variant of object relations theory aimed at studying human development via the initial bonding between children and primary caregivers [27]. Using the behavioral patterns Ainsworth described, Hazan and Shaver (1987) described three types of adult attachment: secure, avoidant, and anxious [28]. Attachment styles have been linked to loneliness through social skills [29,30], with insecure attachment linked to worse social skills [26]. Thus, attachment appears to predicate loneliness [31,32], with greater loneliness associated with insecure attachment styles [28,31,33] and secure attachment predicting the lowest levels of perceived loneliness [28,34]. The attachment system reflects how individuals regulate their affect, especially in novel or threatening situations [35]. Bowlby’s theory also stipulated that novel or threatening conditions, like a pandemic, automatically trigger the attachment system [36]. Securely attached individuals seek close partners for comfort and support, helping them cope with distress. Avoidant individuals try to minimize distress and retreat, while anxiously attached individuals cope by persistently signaling distress and seeking reassurance [35]. During the COVID-19 pandemic, anxious attachment predicted more suicidal ideation and loneliness in a longitudinal study [37]. Meanwhile, avoidant attachment was associated with loneliness, perceived stress [38], and suicidal ideation [37]. During the pandemic, insecure attachment was found to predict greater depressive and anxious symptoms [39] in a relationship partially mediated by loneliness [38].
After primary and secondary appraisals of stressors, Lazarus described the coping process in 1966 [40]. This process is fluid, with both threat appraisal and employed strategies undergoing multiple reappraisals [41]. The efficiency of coping strategies can also depend on external factors: Park and colleagues pointed out that problem-focused coping substantially impacts positive mood in high-control situations, whereas emotion-focused strategies seem more suitable for uncontrollable stressors [42]. Problem-focused coping, alternative seeking, and social support were commonly used during the prior epidemics [43]. Studies measuring coping strategies employed during the COVID-19 pandemic have revealed mixed results, partially due to the different models employed. Thus, more distress has been associated with passive coping [44]; self-blame, venting, and disengagement [45]; wishful thinking [46]; and stronger problem-focused coping [47,48]. In line with Park’s suggestion, Fluharty and colleagues [49] found that problem-focused, avoidant, and emotion-focused coping strategies were not associated with faster mental health improvements during the pandemic, while socially supported coping was associated with a faster decrease in affective symptoms.
Taking this all together, our study focused on the general population of Romania between the third and fourth COVID-19 outbreaks and aimed to investigate attachment, coping, and their relationship to loneliness and emotional distress during the second years of the COVID-19 pandemic in Romania. As such, the primary objectives consisted of:
- (1)
- Measuring the impact of attachment and coping on loneliness;
- (2)
- Measuring the impact of attachment and coping on emotional distress;
- (3)
- Measuring loneliness as a mediator between attachment and emotional distress. The secondary goals included measuring the impact of gender and age.
The secondary goals included measuring the effect that age and gender had on loneliness and emotional distress.
2. Study Design
The general population of Romania during the second year of the COVID-19 pandemic represented the current study’s target. Using the web-based Google Forms platform, we collected data (April 2021–September 2021) across Romania using a snowball design, with the form disseminated via social media platforms. Participation in the study was preceded by an online consent form, during which participants were instructed on the goals and methods of the study as well as data storage. Participants had to finish the questionnaire in one sitting, though the design set no time limit for completion. The questionnaire was tested before publishing by the main author. No incentives were offered. The Institutional Review Board of the Cluj-Napoca Military Emergency Hospital reviewed and approved the study before release (reference number 1855/11.05.2020).
2.1. Sample Demographics
On the final day of data collection, our sample was composed of 141 responders who completed the online survey. Ages ranged from 19 to 71 (M = 35.18, SD = 10.64). Most participants were female (N = 111, 75.5%), had a university degree (N = 129, 87.7%), and described themselves as employed (N = 113, 76.9%).
2.2. Measurements
Emotional distress was assessed via Lovibond and Lovibond’s Depression, Anxiety, and Stress Scale (DASS-21) [50]. The DASS-21 contains 21 self-report items (7 items per subscale), including: “I couldn’t seem to experience any positive feelings at all” (depression), “I experienced trembling (e.g., in the hands)” (anxiety), and “I tended to overreact to situations” (stress). Higher scores suggest a greater frequency of depressive, anxiety, and stress symptoms, whereas low scores suggest a lower frequency. In our sample, the total calculated score presented excellent reliability results (α = 0.95, M = 17.9, SD = 12.9)
Loneliness was measured using the University of California, Los Angeles Loneliness Scale [51]. Modeled on the conceptualization of loneliness as, first and foremost, a subjective emotion, this self-reported scale uses 20 items representing Likert-type scales. The scale has repeatedly demonstrated good construct validity and reliability and has been extensively used on younger populations. Higher scores reflect higher perceived social isolation. Completion of the scale was mandatory for all participants. The reliability analysis of the scale in our sample revealed excellent results (α = 0.95, M = 22.43, SD = 13.38).
Attachment was measured using the Revised Adult Attachment Scale (RAAS) [52], a questionnaire in which the individual, through self-report, provides a graded assessment of his or her skills in forming relationships. The 18 items on this scale are rated on a 5-point Likert scale ranging from 1 (“not at all characteristic of me”) to 5 (“very characteristic of me”). The scale can be divided into an anxiety subscale composed of six items, measuring the extent to which a person is worried about being rejected or unloved, and an avoidance subscale composed of twelve items, measuring how uncomfortable the person is with closeness and dependence on others. The anxiety subscale in our sample presented excellent validity (α = 0.88, M = 14.02, SD = 6.33), with similar results for the avoidance subscale (α = 0.81, M = 33.17, SD = 8.44).
Coping strategies were measured using the self-administered Brief COPE Inventory (B-COPE) [53], an abbreviated version of the original 60-item COPE inventory [41]. The 28 items load onto 14 factors or coping styles: self-distraction; active coping; denial; substance use; use of emotional support; use of instrumental support; behavioral disengagement; venting; positive reframing; humor; acceptance; religion, and self-blame. The B-COPE has been used to evaluate coping strategies during previous infectious disease outbreaks [54], and its Romanian adaptation has presented good psychometric characteristics in prior studies [55]. In our sample, the scale showed good internal consistency, with α = 0.88. Prior studies regarding coping strategies have used all 14 coping strategies in the scale or several coping styles categorized following conceptual or theoretical models by authors. Congruent with prior studies on coping during the pandemic [49], we used the 4-factor model by Bose and colleagues [56] to diminish these limitations. This 4-factor model consists of the following dimensions: problem-focused coping (active coping, planning), emotion-focused coping (positive reframing, acceptance, humor, religion), avoidant coping (behavioral disengagement, denial, substance use), and socially supportive coping (emotional support, instrumental support, and venting).
2.3. Statistical Analysis
Gender differences were measured via multiple independent sample t-tests comparing dependent and independent variables by gender. Two-tailed Pearson correlational analyses were used to the relationships between age, loneliness, emotional distress, attachment, and coping styles. Our study plan was to reach a sample size that would allow us to detect the equivalent of a medium effect size (Cohen’s d 0.5 or Pearson r = 0.24), with a statistical power of 0.80 or greater, in a two-tailed test of a correlation or a multiple regression coefficient. Power calculations using G*Power [57] indicated that the required sample size was 131. This sample size also allowed us to detect, with a power equal to 0.80 or above, indirect effects for which at least one of the standardized paths composing the product coefficient of the indirect effect was in the large effect size range (r > 0.39) and the second one was at least in the medium effect size range (r > 0.26) [58]. The results for all the mediation models we tested indicated that the coefficients forming the indirect effects were all in the large effects size range, and thus, the achieved power was probably greater than the standard threshold.
Four different regression models were performed, testing how attachment and coping affect loneliness and emotional distress while considering age and gender as covariates. Multicollinearity analysis was also performed, with no Variance Inflation Factor (VIF) larger than five being discovered. We also checked the homoscedasticity and the normal distribution of the residuals for our multiple regression models using visual inspection and formal tests (i.e., Shapiro–Wilk and Breusch–Pagan tests). These checks indicated that the assumptions were not completely met for some of the models. Thus, when running those regression models, we compared the OSL results with those of additional statistical techniques that are more robust to deviations from the homoscedasticity and normal distribution assumptions. Specifically, we computed the same models using conservative heteroskedasticity-consistent (HC3) standard error estimators [59] and using robust regression with the Huber estimator [60]. The conclusions based on the results of each model were identical regardless of the statistical approach. Thus, we reported in the manuscript only the OLS regression results.
Finally, mediation analysis was performed using the PROCESS macro for SPSS [61]. The indirect effect was tested using a percentile bootstrap estimation approach using 10,000 samples. Two paths were tested: path 1 measured the mediating effect of loneliness between attachment anxiety and emotional distress, whereas path 2 measured the mediating effect of loneliness between attachment avoidance and emotional distress.
3. Results
3.1. Gender Differences
Independent sample t-tests were conducted to compare age, loneliness, emotional distress, avoidance, and coping styles between genders. Significant differences in the scores for problem-focused coping were found between male (M = 8.06, SD = 4.05) and female responders (M = 10.23, SD = 4.34), t(139) = −2.45, p = 0.014). Male participants also presented lower scores (M = 33, SD = 14.84) than female participants (M = 41.08, SD = 14.31) on emotion-focused coping, t(139) = −2.60, p = 0.010. Avoidant coping presented significant gender differences between male (M = 22.50, SD = 9.21) and female participants (M = 27.32, SD = 10.61), t(139) = −2.29, p = 0.023. Finally, gender differences were also found for socially supported coping between males (M = 15.50, SD = 7.47) and females (M = 19.43, SD = 9.94). Statistical analysis failed to reveal gender differences for age, loneliness, emotional distress, and attachment. The results are summarized in Table 1.

Table 1.
Gender differences.
3.2. Correlational Analyses
Pearson correlation coefficients were computed to assess the linear relationships between loneliness, emotional distress, attachment, and coping styles. Loneliness presented positive correlations with emotional distress (r(139) = 0.70, p < 0.001), attachment anxiety (r(139) = 0.63, p < 0.001), and avoidance (r(139) = 0.51, p < 0.001), along with problem-focused coping (r(139) = 0.21, p <.013) and socially supported coping (r(139) = 0.20, p < 0.016). Emotional distress presented positive correlations with attachment anxiety (r(139) = 0.53, p < 0.001) and attachment avoidance (r(139) = 0.41, p < 0.001), as well as problem-focused coping (r(139) = 0.24, p = 0.004) and socially supported coping (r(139) = 0.26, p = 0.002). The results are summarized in Table 2.
Table 2.
Correlation matrix.
3.3. Regression Analysis
3.3.1. Attachment as Predictor of Loneliness and Emotional Distress
Multiple linear regression analysis was used to test whether attachment styles significantly predicted loneliness, correcting for age and gender. The results of the regression indicated that the two predictors explained 42.3% of the variance (R2 = 0.42, F(4, 136) = 25.107, p < 0.001). Model coefficients (see Table 3) indicated that attachment anxiety (b = 1.06, SE = 0.17, β = 0.50, t(136) = p < 0.001) and attachment avoidance (b = 0.32, SE = 1.55, β = 0.20, t(136) = 2.49, p = 0.014) predicted loneliness. The results are summarized in Table 3.
Table 3.
Attachment dimensions as predictors of loneliness and emotional distress.
The model for emotional distress was also significant, explaining 30.9% of the variance (R2 = 0.30, F(4, 136) = 15.20, p < 0.001). Individual coefficients (see Table 3) indicated that only attachment anxiety (b = 0.87, SE = 0.18, β = 0.42, t(136) = 4.71, p < 0.001) predicted emotional distress. The results are summarized in Table 3.
3.3.2. Coping Styles as Predictors of Loneliness and Emotional Distress
We conducted a similar analysis using coping style as the predictor of interest, once more controlling for age and gender as covariates.
The overall model for loneliness was statistically significant, explaining 11.8% of the variance (R2 = 0.11, F(6, 134) = 2.99, p = 0.009). Individual coefficients revealed that problem-focused coping (b = 2.05, SE = 0.74, β = 0.33, t(134) = 2.75, p = 0.007), emotion-focused coping (b = −1.38, SE = 0.56, β = -.38, t(134) = −2.42, p = 0.015), and socially supported coping (b = 0.1.19, SE = 0.50, β = 0.28, t(134) = 2.37, p = 0.019) predicted loneliness. The results are summarized in Table 4.
Table 4.
Coping styles as predictors of loneliness and emotional distress.
Our emotional distress model achieved statistical significance, predicting 18.9% of the variance (R2 = 0.18, F(6, 134) = 5.20, p < 0.001). The model coefficients revealed that only problem-focused coping (b = 1.85, SE = 0.68, β = 0.31, t(134) = 2.69, p = 0.008), socially supported coping (b = 0.1.83, SE = 0.46, β = 0.45, t(134) = 3.93, p < 0.001), and age (b = −0.29, SE = 0.10, β = −0.24, t(134) = −2.96, p = 0.004) predicted emotional distress. The results are summarized in Table 4.
3.4. Mediation Analysis
3.4.1. Path 1
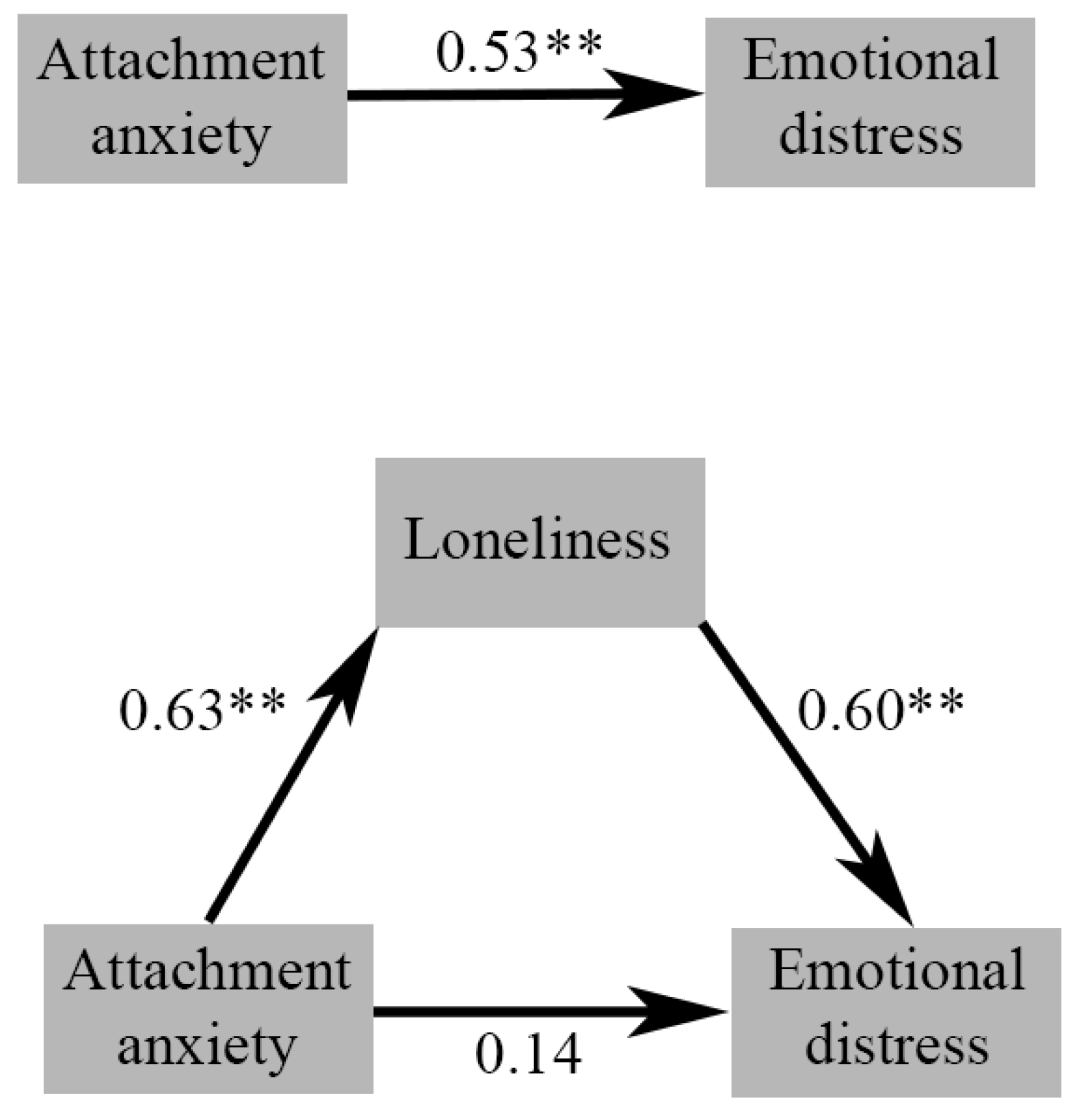
The results of our mediation analysis indicated that attachment anxiety was a significant predictor of loneliness (B = 1.33, SE = 0.13, 95% CI [1.05,1.60], β = 0.63, p < 0.001) and loneliness was a significant predictor of emotional distress (B = 0.58, SE = 0.07, 95% CI [0.44, 0.73], p < 0.001). With the inclusion of loneliness as a mediator, attachment anxiety no longer significantly predicted emotional distress (B = 0.30, SE = 0.15, 95% CI [−0.00, 0.61], p = 0.054), consistent with complete mediation. The predictors accounted for approximately 50.3% of the variance (R2 = 0.50).
The indirect effect was tested using a percentile bootstrap estimation approach with 10,000 samples, implemented via the PROCESS macro [61]. These results indicated that the indirect coefficient was significant (B = 0.73, SE = 0.15, 95% CI [0.49, 1.09], standardized β = 0.38). The standardized coefficients are presented in Figure 1.
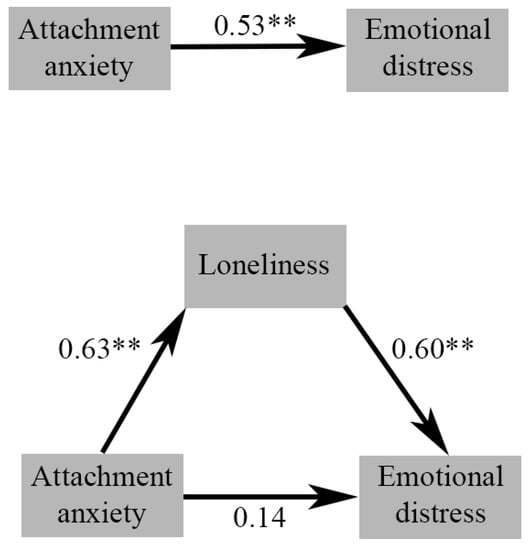
Figure 1.
Standardized regression coefficients for the relationship between attachment anxiety and emotional distress: total effect (above) and mediated by loneliness (below). ** represents p < 0.01.
3.4.2. Path 2
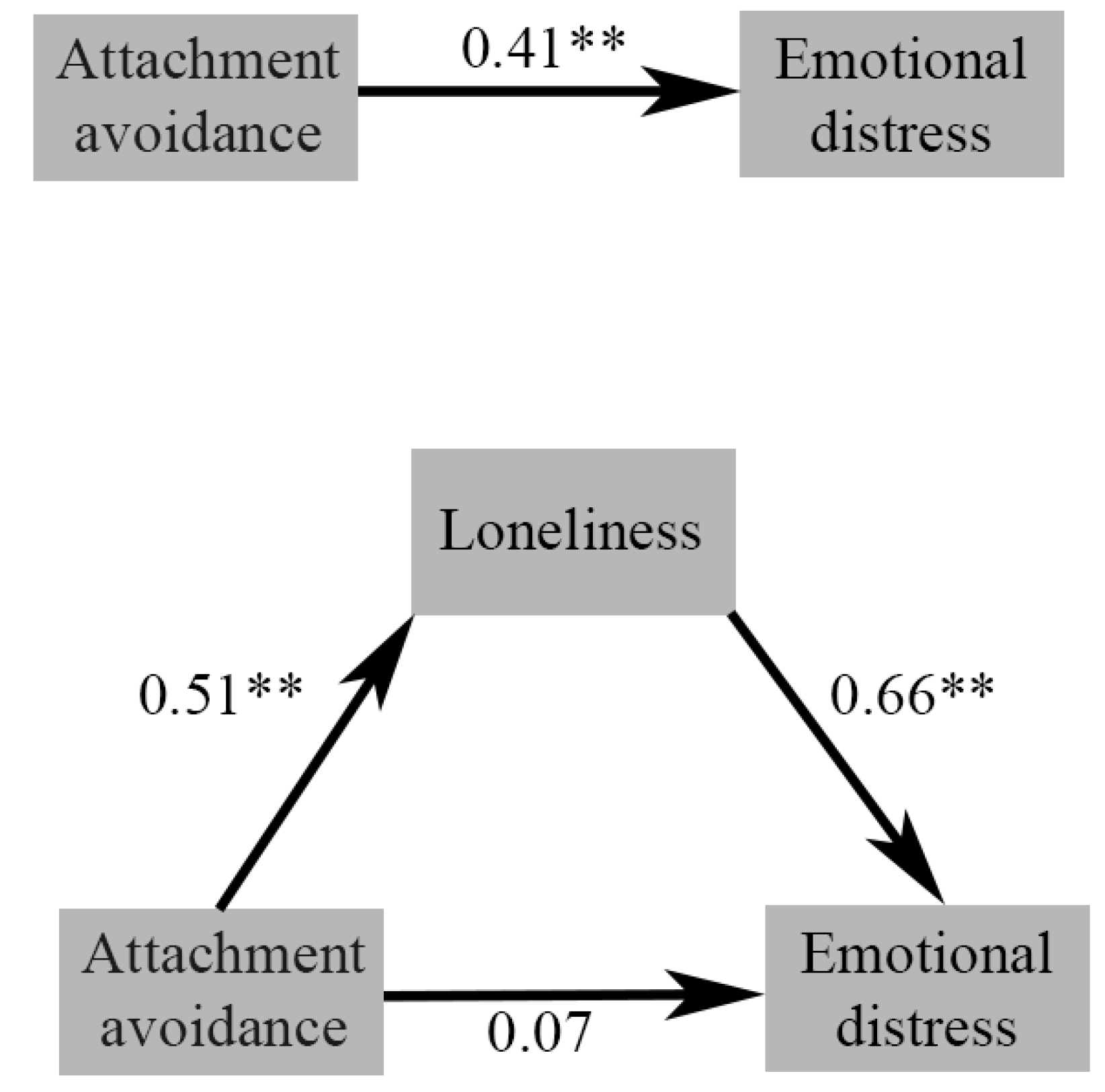
The results of our second mediation analysis revealed that attachment avoidance was a significant predictor of loneliness (B = 0.81, SE = 0.11, 95% CI [0.58, 1.03], β = 0.51), and loneliness was again a significant predictor for emotional distress (B = 0.64, SE = 0.06, 95% CI [0.50, 0.77], p < 0.001). Once loneliness was introduced as a mediator, attachment avoidance no longer significantly predicted emotional distress (B = 1.22, SE = 0.10, 95% CI [−0.08, 0.33], p = 0.25), consistent with complete mediation. Approximately 49.9% of the variance was accounted for by the two predictors (R2 = 0.49).
The bootstrapped results for the indirect effect indicated that it achieved statistical significance (B = 0.51, SE = 0.11, 95% CI [0.30, 75], standardized β = 0.33). The standardized coefficients are presented in Figure 2.
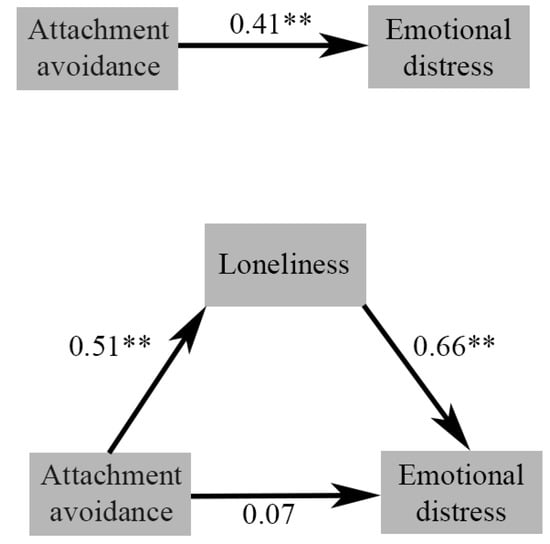
Figure 2.
Standardized regression coefficients for the relationship between attachment avoidance and emotional distress: total effect (above) and mediated by loneliness (below). ** represents p < 0.01.
4. Discussion
The COVID-19 pandemic and the public health measures that accompanied it were superimposed over what was already being described as a loneliness epidemic in developed countries [18,19]. The persistence of socially isolating behavior and perceived isolation after the implementation of pandemic measures could be explained by a wide variety of factors, from learned helplessness and global and economic stressors [62] to social withdrawal as a coping mechanism [63]. The pandemic’s widespread psychological footprint is still being discussed, though some have already argued for the emergence of a pandemic disengagement syndrome [64]. The present study, undertaken during the second year of the pandemic in Romania, set out to measure the general population’s emotional distress and loneliness while accounting for predisposing factors, like attachment and coping styles, and demographic variables, like age and gender.
The demographic factors in our study revealed weak to statistically insignificant results. Correlational analysis showed that age presented statistically significant albeit minimal- to low-strength negative correlations with emotional distress; attachment anxiety; and problem-focused, emotion-focused, and avoidant coping. Our results align with prior research reporting that young adults were at risk for more mental health symptoms during the pandemic [65,66,67]. Age, however, was a significant predictor of emotional distress when considered alongside coping, but not attachment, suggesting that the latter played a more salient role in the resilience of older age groups during the pandemic. This aligns with Okely and colleagues’ [68] suggestions that with age, more refined emotional and cognitive skills provide individuals with better ways of coping with the lockdown. One of the mechanisms Okely mentioned was emotional stability, which has been consistently linked to attachment theory [69,70], as our results indicate a small yet significant decrease in attachment anxiety with age. Adult attachment is not set in stone [71,72]: parent–child bonds can predict attachment stability for the first fifteen years, yet said stability diminishes past that point [73]. Our study found no significant differences between genders in our samples for emotional distress, loneliness, or attachment dimensions. Gender differences in attachment are still being debated [74] and are subject to important cross-cultural factors [75], and the similar scores for attachment dimensions reported by both men and women could account for the lack of group differences regarding loneliness or emotional distress, contrary to most reports on women being at greater risk than men for both loneliness [25] and mental health symptoms [76,77]. Our sample’s predominantly female, predominantly younger distribution could explain the minor effects and lack of statistical significance.
Consistent with previous studies, insecure attachment influenced emotional distress [38,78,79]. Attachment styles are closely tied to how an individual handles their affect, especially during novel and/or threatening conditions [35]; they are linked to both the sympathetic nervous system stress response [80] and the hypothalamic–pituitary–adrenergic stress response [80,81] and partially depend on the relationship context [82]. Considering the restrictions imposed by social distancing, partner presence and relationship quality might have become a critical support pillar for some individuals. Moreover, attachment styles predict potentially protective or damaging behaviors arising in response to stressors [82]. These secondary attachment strategies [83,84] vary according to attachment, with anxiously attached individuals displaying hyperactivating strategies and those avoidantly attached employing deactivating strategies. Predisposing, precipitating, and crisis-state factors can mediate the link between attachment insecurity and suicidality [85]. Loneliness has been found to mediate the effect between insecure attachment and the medical lethality of suicide attempts [86].
Individuals with high attachment anxiety perceive others to be emotionally unpredictable and unreliably responsive to their affective needs, and they closely monitor their significant others for cues of emotional unavailability [38,87]. This hyperactivation strategy leads to further activation of the attachment system and inhibition of exploratory behavior [38]. Our regression analysis showed that attachment anxiety and avoidance explained nearly half the variance in perceived social isolation, with the former displaying an effect twice as strong as the latter. Attachment anxiety also significantly predicted nearly one-third of emotional distress symptoms, though attachment avoidance failed to reach the significance threshold. Furthermore, our first mediation model revealed that attachment anxiety fully predicted emotional distress via loneliness, with the direct effect becoming insignificant once the mediator was introduced. Individuals who score high on attachment anxiety tend to use hyperactivating strategies that lead to increased perception and expression of threatening signals, making them more prone to developing anxiety disorders [88,89], post-traumatic stress symptoms [90,91], and post-natal depression [92].
Conversely, individuals high in attachment avoidance present a different attachment strategy: deactivation, inhibition of the attachment system, and minimization of perceived frustration and distress [87]. Attachment avoidance was a statistically significant predictor of loneliness in our regression analysis, although it was not as strong as attachment anxiety. Relationship quality is more related to avoidance rather than attachment anxiety [93], with avoidant individuals experiencing their partners as less supportive [94]. Considering the restrained social options during the pandemic, this would explain why those who were more avoidantly attached perceived themselves as lacking support and described themselves as lonely. Our regression analysis failed to find a significant effect for attachment avoidance of emotional distress once attachment anxiety was considered. However, our subsequent mediation model revealed a significant, fully mediated path from attachment avoidance to emotional distress via loneliness. Attachment avoidance has been linked with the risk of depression [91] and suicidal ideation [70,95]. Finally, since both attachment avoidance and anxiety presented essential effects on mental health, a synergistic effect cannot be disconfirmed. This is conceptually equivalent to Bartholomew’s ‘fearful’ type [96], which features individuals with high attachment anxiety (model of self) and high avoidance (model of other) and is conceptually similar to the disorganized attachment style observed, as further described by Main and Solomon [97]. Though disorganized attachment is rarely studied in adults [98], it has been shown to be associated with high levels of attachment avoidance and anxiety [99] and clinically associated with more severe personality traits [100].
By contrast, correlation and regression analyses revealed more mixed, weaker interactions between coping, loneliness, and emotional distress. Notably, problem-focused and socially supported coping was associated with more loneliness and perceived emotional distress. Our results align with those of Fluharty and colleagues [49], which found that participants with higher scores for problem-focused and socially supportive coping had higher mental health symptoms at the start of the pandemic lockdown in the UK. Socially supportive coping is known to be associated with better mental health and increased resilience [101], as are problem-focused strategies [102]. During the pandemic, coping strategies mediated the relationship between uncertainty and psychological distress [103]. As the period between the third and fourth waves was marked by uncertainty and mixed messaging from the media and authorities, it is possible that outward-focused, reactive strategies like active coping and planning might have proven insufficient and detrimental for individuals. Similarly, during a time marked by restrictions and reduced social opportunities, socially supported coping might have proven to be an inefficient strategy for dealing with stress. Meanwhile, emotion-focused coping seemed to have a negative predictive effect on loneliness alone but not on perceived emotional distress. Because loneliness is defined as a reduced perceived quality of social support, it is reasonable to assume those who focused on addressing the emotions of the situation would have a better perceived quality of social interactions with peers or partners. These results again reinforce Park’s [42] suggestion that context is essential in determining the efficacy of coping strategies.
Our study is not without strengths or limitations. The dimensional approach and utilizing an attachment scale focused on romantic attachment strategies can be considered a fundamental strength of our study. To the best of our knowledge, aside from an ongoing study by Edjolo and colleagues [104], this is the only pandemic-related study to measure attachment and coping styles in the same sample. Similarly, the exploration of loneliness in Romania, an at-risk country, is a developing field to which our research will hopefully contribute. Among the more important limitations, we mention our sample’s predominantly female and more educated distribution, which restricts its application to the general population. The cross-sectional design also severely restricts any causal inferences from being drawn. Aside from the qualitative limitations, our limited sample size and the convenience sampling method similarly reduce the applicability of our results to the general population.
Loneliness is not only a symptom of social isolation. Future research should consider the importance of dyadic relationships and the role of partners, or lack thereof, in emotion regulation, as well as how childhood attachment is pivotal in received and perceived support. Furthermore, coping strategies should not be automatically segregated into ‘adaptive’ or ‘dysfunctional,’ as the controllability of the context plays a crucial role in the efficacy of the strategies employed. Humankind and humans are essentially social, and both public health measures and individual psychotherapeutic approaches must not forget this ‘need to belong’.
5. Conclusions
Insecure attachment predicted a significant percentage of emotional distress during the pandemic, even when correcting for age and gender. Problem-focused and socially supported coping both predicted greater loneliness and emotional distress, whereas emotionally supported coping predicted less. Attachment anxiety and avoidance are essential predictors of emotional distress during the second year of the pandemic, with loneliness completely mediating the relationship for both. Coping strategies predicted a smaller percentage of emotional distress than attachment. Further research should, therefore, focus on attachment as a component of stress resilience and consider external contexts when measuring the efficiency of coping mechanisms.
Author Contributions
A.H.-P. worked on conceptualization, methodology, and formal analysis and wrote the original manuscript; M.F.-S. helped write the original manuscript (review and editing); M.M. oversaw conceptualization, review, and supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the “C. Papilian” Military Emergency Hospital, Cluj-Napoca.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Research data are available upon reasonable requests for future studies.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Dong, L.; Bouey, J. Public mental health crisis during COVID-19 pandemic, China. Emerg. Infect. Dis. 2020, 26, 1616. [Google Scholar] [CrossRef]
- Dascalu, S.; Geambasu, O.; Valentin Raiu, C.; Azoicai, D.; Damian Popovici, E.; Apetrei, C. COVID-19 in Romania: What went wrong? Front. Public Health 2021, 9, 813941. [Google Scholar] [CrossRef]
- Thorpe, N. COVID: Romania’s Health System Torn Apart by Pandemic. BBC. Available online: https://www.bbc.com/news/world-europe-58992090 (accessed on 23 October 2021).
- Horwitz, A.V. Selecting outcomes for the sociology of mental health: Issues of measurement and dimensionality. J. Health Soc. Behav. 2002, 43, 130. [Google Scholar]
- Drapeau, A.; Marchand, A.; Beaulieu-Prevost, D. Epidemiology of psychological distress. Ment. Illnesses-Underst. Predict. Control. 2012, 69, 105–106. [Google Scholar]
- Wang, Y.; Kala, M.P.; Jafar, T.H. Factors associated with psychological distress during the coronavirus disease 2019 (COVID-19) pandemic on the predominantly general population: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0244630. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Navarro, R.; Malonda, E.; Llorca-Mestre, A.; Cano-Vindel, A.; Fernández-Berrocal, P. Worry about COVID-19 contagion and general anxiety: Moderation and mediation effects of cognitive emotion regulation. J. Psychiatr. Res. 2021, 137, 311–318. [Google Scholar] [CrossRef]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 1. [Google Scholar] [CrossRef]
- Cénat, J.M.; Blais-Rochette, C.; Kokou-Kpolou, C.K.; Noorishad, P.G.; Mukunzi, J.N.; McIntee, S.E.; Dalexis, R.D.; Goulet, M.A.; Labelle, P.R. Prevalence of symptoms of depression, anxiety, insomnia, posttraumatic stress disorder, and psychological distress among populations affected by the COVID-19 pandemic: A systematic review and meta-analysis. Psychiatry Res. 2021, 295, 113599. [Google Scholar] [CrossRef] [PubMed]
- Margetić, B.; Peraica, T.; Stojanović, K.; Ivanec, D. Predictors of emotional distress during the COVID-19 pandemic; a Croatian study. Personal. Individ. Differ. 2021, 175, 110691. [Google Scholar] [CrossRef]
- Sitarz, R.; Forma, A.; Karakuła, K.; Juchnowicz, D.; Baj, J.; Bogucki, J.; Karakuła-Juchnowicz, H. How do polish students manage emotional distress during the COVID-19 lockdown? A web-based cross-sectional study. J. Clin. Med. 2021, 10, 4964. [Google Scholar] [CrossRef]
- Taylor, S. The psychology of pandemics. Annu. Rev. Clin. Psychol. 2022, 18, 581–609. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.; Nguyen, T.V.T.; Zhong, J.; Liu, J. A COVID-19 descriptive study of life after lockdown in Wuhan, China. R. Soc. Open Sci. 2020, 7, 200705. [Google Scholar] [CrossRef] [PubMed]
- Ernst, M.; Niederer, D.; Werner, A.M.; Czaja, S.J.; Mikton, C.; Ong, A.D.; Rosen, T.; Brähler, E.; Beutel, M.E. Loneliness before and during the COVID-19 pandemic: A systematic review with meta-analysis. Am. Psychol. 2022, 77, 660. [Google Scholar] [CrossRef]
- Leigh-Hunt, N.; Bagguley, D.; Bash, K.; Turner, V.; Turnbull, S.; Valtorta, N.; Caan, W. An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health 2017, 152, 157–171. [Google Scholar] [CrossRef]
- Perlman, D.; Peplau, L.A. Toward a social psychology of loneliness. Pers. Relatsh. 1981, 3, 31–56. [Google Scholar]
- Hawkley, L.C.; Cacioppo, J.T. Loneliness matters: A theoretical and empirical review of consequences and mechanisms. Ann. Behav. Med. 2010, 40, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.E.; Braun, B. Loneliness and social isolation-a private problem, a public issue. J. Fam. Consum. Sci. 2019, 111, 7–14. [Google Scholar] [CrossRef]
- Jeste, D.V.; Lee, E.E.; Cacioppo, S. Battling the modern behavioral epidemic of loneliness: Suggestions for research and interventions. JAMA Psychiatry 2020, 77, 553–554. [Google Scholar] [CrossRef]
- Foti, S.A.; Khambaty, T.; Birnbaum-Weitzman, O.; Arguelles, W.; Penedo, F.; Espinoza Giacinto, R.A.; Gutierrez, A.P.; Gallo, L.C.; Giachello, A.L.; Schneiderman, N.; et al. Loneliness, cardiovascular disease, and diabetes prevalence in the hispanic community health study/study of latinos sociocultural ancillary study. J. Immigr. Minor. Health 2020, 22, 345–352. [Google Scholar] [CrossRef]
- Abdellaoui, A.; Sanchez-Roige, S.; Sealock, J.; Treur, J.L.; Dennis, J.; Fontanillas, P.; Elson, S.; 23andMe Research Team; Nivard, M.G.; Ip, H.F. Phenome-wide investigation of health outcomes associated with genetic predisposition to loneliness. Hum. Mol. Genet. 2019, 28, 3853–3865. [Google Scholar] [CrossRef]
- Buchman, A.S.; Boyle, P.A.; Wilson, R.S.; James, B.D.; Leurgans, S.E.; Arnold, S.E.; Bennett, D.A. Loneliness and the rate of motor decline in old age: The rush memory and aging project, a community-based cohort study. BMC Geriatr. 2010, 10, 77. [Google Scholar] [CrossRef]
- Yang, K.; Victor, C. Age and loneliness in 25 European nations. Ageing Soc. 2011, 31, 1368–1388. [Google Scholar] [CrossRef]
- Baarck, J.; d’Hombres, B.; Tintori, G. Loneliness in Europe before and during the COVID-19 pandemic. Health Policy 2022, 126, 1124–1129. [Google Scholar] [CrossRef] [PubMed]
- Bu, F.; Steptoe, A.; Fancourt, D. Who is lonely in lockdown? Cross-cohort analyses of predictors of loneliness before and during the COVID-19 pandemic. Public Health 2020, 186, 31–34. [Google Scholar] [CrossRef]
- Palgi, Y.; Shrira, A.; Ring, L.; Bodner, E.; Avidor, S.; Bergman, Y.; Cohen-Fridel, S.; Keisari, S.; Hoffman, Y. The loneliness pandemic: Loneliness and other concomitants of depression, anxiety and their comorbidity during the COVID-19 outbreak. J. Affect. Disord. 2020, 275, 109–111. [Google Scholar] [CrossRef]
- Ainsworth, M.S.; Bowlby, J. An ethological approach to personality development. Am. Psychol. 1991, 46, 333. [Google Scholar] [CrossRef]
- Shaver, P.; Hazan, C. Being lonely, falling in love. J. Soc. Behav. Personal. 1987, 2, 105. [Google Scholar]
- Larose, S.; Guay, F.; Boivin, M. Attachment, social support, and loneliness in young adulthood: A test of two models. Personal. Soc. Psychol. Bull. 2002, 28, 684–693. [Google Scholar] [CrossRef]
- Mallinckrodt, B. Attachment, social competencies, social support, and interpersonal process in psychotherapy. Psychother. Res. 2000, 10, 239–266. [Google Scholar] [CrossRef]
- Deniz, M.; Hamarta, E.; Ari, R. An investigation of social skills and loneliness levels of university students with respect to their attachment styles in a sample of Turkish students. Soc. Behav. Personal. Int. J. 2005, 33, 19–32. [Google Scholar] [CrossRef]
- Russell, D.; Cutrona, C.E.; Rose, J.; Yurko, K. Social and emotional loneliness: An examination of Weiss’s typology of loneliness. J. Personal. Soc. Psychol. 1984, 46, 1313. [Google Scholar] [CrossRef]
- Margalit, M.; Margalit, M. Loneliness Conceptualization. Lonely Children and Adolescents: Self-Perceptions, Social Exclusion, and Hope; Springer: New York, NY, USA, 2010; pp. 1–28. [Google Scholar]
- Bernardon, S.; Babb, K.A.; Hakim-Larson, J.; Gragg, M. Loneliness, attachment, and the perception and use of social support in university students. Can. J. Behav. Sci. /Rev. Can. Des Sci. Du Comport. 2011, 43, 40. [Google Scholar] [CrossRef]
- Pietromonaco, P.R.; Beck, L.A. Attachment processes in adult romantic relationships. In APA Handbook of Personality and Social Psychology, Volume 3: Interpersonal Relations; American Psychological Association: Washington, DC, USA, 2015; pp. 33–64. [Google Scholar]
- Bowlby, J. Separation, anxiety and anger. In Attachment and Loss; Basic Books: New York, NY, USA, 1973; Volume II, p. 429. [Google Scholar]
- Lewis, K.C.; Roche, M.J.; Brown, F.; Tillman, J.G. Attachment, loneliness, and social connection as prospective predictors of suicidal ideation during the COVID-19 pandemic: A relational diathesis-stress experience sampling study. Suicide Life-Threat. Behav. 2023, 53, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Rollè, L.; Trombetta, T.; Calabrese, C.; Vismara, L.; Sechi, C. Adult attachment, loneliness, COVID-19 risk perception and perceived stress during COVID-19 pandemic. Mediterr. J. Clin. Psychol. 2022, 10. [Google Scholar] [CrossRef]
- Vowels, L.M.; Vowels, M.J.; Carnelley, K.B.; Millings, A.; Gibson-Miller, J. Toward a causal link between attachment styles and mental health during the COVID-19 pandemic. Br. J. Clin. Psychol. 2023, 62, 605–620. [Google Scholar] [CrossRef]
- Lazarus, R.S. Psychological Stress and the Coping Process; McGraw-Hill: New York, NY, USA, 1984. [Google Scholar]
- Carver, C.S.; Scheier, M.F.; Weintraub, J.K. Assessing coping strategies: A theoretically based approach. J. Personal. Soc. Psychol. 1989, 56, 267. [Google Scholar] [CrossRef] [PubMed]
- Park, C.L.; Armeli, S.; Tennen, H. Appraisal-coping goodness of fit: A daily internet study. Personal. Soc. Psychol. Bull. 2004, 30, 558–569. [Google Scholar] [CrossRef] [PubMed]
- Chew, Q.H.; Wei, K.C.; Vasoo, S.; Chua, H.C.; Sim, K. Narrative synthesis of psychological and coping responses towards emerging infectious disease outbreaks in the general population: Practical considerations for the COVID-19 pandemic. Singap. Med. J. 2020, 61, 350. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Havewala, M.; Zhu, Q. COVID-19 stressful life events and mental health: Personality and coping styles as moderators. J. Am. Coll. Health 2022, 1–10. [Google Scholar] [CrossRef]
- Gurvich, C.; Thomas, N.; Thomas, E.H.; Hudaib, A.R.; Sood, L.; Fabiatos, K.; Sutton, K.; Isaacs, A.; Arunogiri, S.; Sharp, G.; et al. Coping styles and mental health in response to societal changes during the COVID-19 pandemic. Int. J. Soc. Psychiatry 2021, 67, 540–549. [Google Scholar] [CrossRef] [PubMed]
- Garbóczy, S.; Szemán-Nagy, A.; Ahmad, M.S.; Harsányi, S.; Ocsenás, D.; Rekenyi, V.; Al-Tammemi, A.A.; Kolozsvári, L.R. Health anxiety, perceived stress, and coping styles in the shadow of the COVID-19. BMC Psychol. 2021, 9, 53. [Google Scholar] [CrossRef]
- Ciuhan, G.C.; Nicolau, R.G.; Iliescu, D. Perceived stress and wellbeing in Romanian teachers during the COVID-19 pandemic: The intervening effects of job crafting and problem-focused coping. Psychol. Sch. 2022, 59, 1844–1855. [Google Scholar] [CrossRef]
- Ding, Y.; Fu, X.; Liu, R.; Hwang, J.; Hong, W.; Wang, J. The impact of different coping styles on psychological distress during the COVID-19: The mediating role of perceived stress. Int. J. Environ. Res. Public Health 2021, 18, 10947. [Google Scholar] [CrossRef]
- Fluharty, M.; Bu, F.; Steptoe, A.; Fancourt, D. Coping strategies and mental health trajectories during the first 21 weeks of COVID-19 lockdown in the United Kingdom. Soc. Sci. Med. 2021, 279, 113958. [Google Scholar] [CrossRef]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Russell, D.W. UCLA Loneliness Scale (Version 3): Reliability, validity, and factor structure. J. Personal. Assess. 1996, 66, 20–40. [Google Scholar] [CrossRef]
- Collins, N.L. Revised adult attachment scale. In Behavior Therapy; American Psychological Association: Washington, DC, USA, 1996. [Google Scholar]
- Carver, C.S. You want to measure coping but your protocol’too long: Consider the brief cope. Int. J. Behav. Med. 1997, 4, 92–100. [Google Scholar] [CrossRef]
- Wong, T.W.; Yau, J.K.; Chan, C.L.; Kwong, R.S.; Ho, S.M.; Lau, C.C.; Lau, F.L.; Lit, C.H. The psychological impact of severe acute respiratory syndrome outbreak on healthcare workers in emergency departments and how they cope. Eur. J. Emerg. Med. 2005, 12, 13–18. [Google Scholar] [CrossRef]
- Crasovan, D.I.; Sava, F.A. Translation, adaptation, and validation on Romanian population of COPE questionnaire for coping mechanisms analysis. Cogn. Brain Behav. 2013, 17, 61. [Google Scholar]
- Bose, C.N.; Bjorling, G.; Elfstrom, M.L.; Persson, H.; Saboonchi, F. Assessment of coping strategies and their associations with health related quality of life in patients with chronic heart failure: The Brief COPE restructured. Cardiol. Res. 2015, 6, 239. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Fritz, M.S.; MacKinnon, D.P. Required sample size to detect the mediated effect. Psychol. Sci. 2007, 18, 233–239. [Google Scholar] [CrossRef]
- Hayes, A.F.; Cai, L. Using heteroskedasticity-consistent standard error estimators in OLS regression: An introduction and software implementation. Behav. Res. Methods 2007, 39, 709–722. [Google Scholar] [CrossRef]
- Andersen, R. Modern methods for robust regression. In Quantitative Applications in the Social Sciences; Sage: Thousand Oaks, CA, USA, 2008; Volume 12. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford publications: New York, NY, USA, 2017. [Google Scholar]
- Pieh, C.; O’ Rourke, T.; Budimir, S.; Probst, T. Relationship quality and mental health during COVID-19 lockdown. PLoS ONE 2020, 15, e0238906. [Google Scholar] [CrossRef]
- Zaidi, A.; Ali, A.Z. Living under the shadow of a pandemic: The psychological challenges underlying social distancing and awareness raising. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, 508. [Google Scholar] [CrossRef]
- Prati, G.; Mancini, A.D. Social and behavioral consequences of the COVID-19 pandemic: Validation of a Pandemic Disengagement Syndrome Scale (PDSS) in four national contexts. Psychol. Assess. 2023. [Google Scholar] [CrossRef]
- Kauhanen, L.; Wan Mohd Yunus, W.M.; Lempinen, L.; Peltonen, K.; Gyllenberg, D.; Mishina, K.; Gilbert, S.; Bastola, K.; Brown, J.S.; Sourander, A. A systematic review of the mental health changes of children and young people before and during the COVID-19 pandemic. Eur. Child Adolesc. Psychiatry 2023, 32, 995–1013. [Google Scholar] [CrossRef] [PubMed]
- Na, L.; Yang, L.; Mezo, P.G.; Liu, R. Age disparities in mental health during the COVID19 pandemic: The roles of resilience and coping. Soc. Sci. Med. 2022, 305, 115031. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, R.C.; Wetherall, K.; Cleare, S.; McClelland, H.; Melson, A.J.; Niedzwiedz, C.L.; O’Carroll, R.E.; O’Connor, D.B.; Platt, S.; Scowcroft, E.; et al. Mental health and well-being during the COVID-19 pandemic: Longitudinal analyses of adults in the UK COVID-19 Mental Health & Wellbeing study. Br. J. Psychiatry 2021, 218, 326–333. [Google Scholar]
- Okely, J.A.; Corley, J.; Welstead, M.; Taylor, A.M.; Page, D.; Skarabela, B.; Redmond, P.; Cox, S.R.; Russ, T.C. Change in physical activity, sleep quality, and psychosocial variables during COVID-19 lockdown: Evidence from the Lothian Birth Cohort 1936. Int. J. Environ. Res. Public Health 2021, 18, 210. [Google Scholar] [CrossRef] [PubMed]
- Shaver, P.R.; Mikulincer, M. An overview of adult attachment theory. In Attachment Theory and Research in Clinical Work with Adults; The Guilford Press: New York, NY, USA, 2009; pp. 17–45. [Google Scholar]
- Turton, H.; Berry, K.; Danquah, A.; Green, J.; Pratt, D. An investigation of whether emotion regulation mediates the relationship between attachment insecurity and suicidal ideation and behaviour. Clin. Psychol. Psychother. 2022, 29, 1587–1598. [Google Scholar] [CrossRef] [PubMed]
- Davila, J.; Burge, D.; Hammen, C. Why does attachment style change? J. Personal. Soc. Psychol. 1997, 73, 826. [Google Scholar] [CrossRef]
- Thompson, R.A.; Simpson, J.A.; Berlin, L.J. Taking perspective on attachment theory and research: Nine fundamental questions. Attach. Hum. Dev. 2022, 24, 543–560. [Google Scholar] [CrossRef]
- Pinquart, M.; Feußner, C.; Ahnert, L. Meta-analytic evidence for stability in attachments from infancy to early adulthood. Attach. Hum. Dev. 2013, 15, 189–218. [Google Scholar] [CrossRef] [PubMed]
- Bakermans-Kranenburg, M.J.; Van Ijzendoorn, M.H. No reliable gender differences in attachment across the lifespan. Behav. Brain Sci. 2009, 32, 22–23. [Google Scholar] [CrossRef]
- Hasson-Ohayon, I.; Goldzweig, G.; Sela-Oren, T.; Pizem, N.; Bar-Sela, G.; Wolf, I. Attachment style, social support and finding meaning among spouses of colorectal cancer patients: Gender differences. Palliat. Support. Care 2015, 13, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Beutel, M.E.; Hettich, N.; Ernst, M.; Schmutzer, G.; Tibubos, A.N.; Braehler, E. Mental health and loneliness in the German general population during the COVID-19 pandemic compared to a representative pre-pandemic assessment. Sci. Rep. 2021, 11, 14946. [Google Scholar] [CrossRef] [PubMed]
- Fernández, R.S.; Crivelli, L.; Guimet, N.M.; Allegri, R.F.; Pedreira, M.E. Psychological distress associated with COVID-19 quarantine: Latent profile analysis, outcome prediction and mediation analysis. J. Affect. Disord. 2020, 277, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Shaver, P.R.; Mikulincer, M.; Sahdra, B.; Gross, J. Attachment security as a foundation for kindness toward self and others. In The Oxford Handbook of Hypo-Egoic Phenomena; Oxford University Press: Oxford, UK, 2016; p. 10. [Google Scholar]
- Powers, S.I.; Pietromonaco, P.R.; Gunlicks, M.; Sayer, A. Dating couples’ attachment styles and patterns of cortisol reactivity and recovery in response to a relationship conflict. J. Personal. Soc. Psychol. 2006, 90, 613. [Google Scholar] [CrossRef]
- Diamond, L.M.; Fagundes, C.P. Psychobiological research on attachment. J. Soc. Pers. Relatsh. 2010, 27, 218–225. [Google Scholar] [CrossRef]
- Carter, C.S. Neuroendocrine perspectives on social attachment and love. Psychoneuroendocrinology 1998, 23, 779–818. [Google Scholar] [CrossRef] [PubMed]
- Pietromonaco, P.R.; Beck, L.A. Adult attachment and physical health. Curr. Opin. Psychol. 2019, 25, 115–120. [Google Scholar] [CrossRef]
- Mikulincer, M.; Shaver, P.R. The attachment behavioral system in adulthood: Activation, psychodynamics, and interpersonal processes. Adv. Exp. Soc. Psychol. 2003, 35, 56–152. [Google Scholar]
- Lopez, F.G.; Brennan, K.A. Dynamic processes underlying adult attachment organization: Toward an attachment theoretical perspective on the healthy and effective self. J. Couns. Psychol. 2000, 47, 283. [Google Scholar] [CrossRef]
- Green, J.; Berry, K.; Danquah, A.; Pratt, D. The role of psychological and social factors in the relationship between attachment and suicide: A systematic review. Clin. Psychol. Psychother. 2020, 27, 463–488. [Google Scholar] [CrossRef]
- Levi-Belz, Y.; Gvion, Y.; Horesh, N.; Apter, A. Attachment patterns in medically serious suicide attempts: The mediating role of self-disclosure and loneliness. Suicide Life-Threat. Behav. 2013, 43, 511–522. [Google Scholar] [CrossRef] [PubMed]
- Campbell, L.; Marshall, T. Anxious attachment and relationship processes: An interactionist perspective. J. Personal. 2011, 79, 1219–1250. [Google Scholar] [CrossRef] [PubMed]
- Marazziti, D.; Dell’Osso, B.; Dell’Osso, M.C.; Consoli, G.; Del Debbio, A.; Mungai, F.; Vivarelli, L.; Albanese, F.; Piccinni, A.; Rucci, P.; et al. Romantic attachment in patients with mood and anxiety disorders. CNS Spectr. 2007, 12, 751–756. [Google Scholar] [CrossRef]
- Eng, W.; Heimberg, R.G.; Hart, T.A.; Schneier, F.R.; Liebowitz, M.R. Attachment in individuals with social anxiety disorder: The relationship among adult attachment styles, social anxiety, and depression. Emotion 2001, 1, 365. [Google Scholar] [CrossRef]
- Woodhouse, S.; Ayers, S.; Field, A.P. The relationship between adult attachment style and post-traumatic stress symptoms: A meta-analysis. J. Anxiety Disord. 2015, 35, 103–117. [Google Scholar] [CrossRef]
- Ostacoli, L.; Cosma, S.; Bevilacqua, F.; Berchialla, P.; Bovetti, M.; Carosso, A.R.; Malandrone, F.; Carletto, S.; Benedetto, C. Psychosocial factors associated with postpartum psychological distress during the COVID-19 pandemic: A cross-sectional study. BMC Pregnancy Childbirth 2020, 20, 703. [Google Scholar] [CrossRef] [PubMed]
- Warfa, N.; Harper, M.; Nicolais, G.; Bhui, K. Adult attachment style as a risk factor for maternal postnatal depression: A systematic review. BMC Psychol. 2014, 2, 56. [Google Scholar] [CrossRef] [PubMed]
- Shaver, P.R.; Schachner, D.A.; Mikulincer, M. Attachment style, excessive reassurance seeking, relationship processes, and depression. Personal. Soc. Psychol. Bull. 2005, 31, 343–359. [Google Scholar] [CrossRef]
- Vowels, L.M.; Carnelley, K.B. Attachment styles, negotiation of goal conflict, and perceived partner support during COVID-19. Personal. Individ. Differ. 2021, 171, 110505. [Google Scholar] [CrossRef]
- Grunebaum, M.F.; Galfalvy, H.C.; Mortenson, L.Y.; Burke, A.K.; Oquendo, M.A.; Mann, J.J. Attachment and social adjustment: Relationships to suicide attempt and major depressive episode in a prospective study. J. Affect. Disord. 2020, 123, 123–130. [Google Scholar] [CrossRef]
- Bartholomew, K.; Horowitz, L.M. Attachment styles among young adults: A test of a four-category model. J. Personal. Soc. Psychol. 1991, 61, 226. [Google Scholar] [CrossRef]
- Main, M.; Solomon, J. Procedures for identifying infants as disorganized/disoriented during the Ainsworth Strange Situation. Attach. Presch. Years Theory Res. Interv. 1990, 1, 121–160. [Google Scholar]
- Briere, J.; Runtz, M.; Eadie, E.M.; Bigras, N.; Godbout, N. The Disorganized Response Scale: Construct validity of a potential self-report measure of disorganized attachment. Psychol. Trauma Theory Res. Pract. Policy 2019, 11, 486. [Google Scholar] [CrossRef] [PubMed]
- Paetzold, R.L.; Rholes, W.S.; Kohn, J.L. Disorganized attachment in adulthood: Theory, measurement, and implications for romantic relationships. Rev. Gen. Psychol. 2015, 19, 146–156. [Google Scholar] [CrossRef]
- Beeney, J.E.; Wright, A.G.; Stepp, S.D.; Hallquist, M.N.; Lazarus, S.A.; Beeney, J.R.; Scott, L.N.; Pilkonis, P.A. Disorganized attachment and personality functioning in adults: A latent class analysis. Personal. Disord. Theory Res. Treat. 2017, 8, 206. [Google Scholar] [CrossRef] [PubMed]
- Dumont, M.; Provost, M.A. Resilience in adolescents: Protective role of social support, coping strategies, self-esteem, and social activities on experience of stress and depression. J. Youth Adolesc. 1999, 28, 343–363. [Google Scholar] [CrossRef]
- Folkman, S.; Lazarus, R.S. Coping and emotion. In Stress and Coping: An Anthology; Columbia University Press: New York, NY, USA, 1991; pp. 207–227. [Google Scholar]
- Rettie, H.; Daniels, J. Coping and tolerance of uncertainty: Predictors and mediators of mental health during the COVID-19 pandemic. Am. Psychol. 2021, 76, 427. [Google Scholar] [CrossRef] [PubMed]
- Edjolo, A.; Dorey, J.M.; Herrmann, M.; Perrot, C.; Lebrun-Givois, C.; Buisson, A.; El Haouari, H.; Laurent, B.; Pongan, E.; Rouch, I. Stress, personality, attachment, and coping strategies during the COVID-19 pandemic: The STERACOVID prospective cohort study protocol. Front. Psychiatry 2022, 13, 918428. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).