Abstract
Vaccination against infectious disease affords direct protection from vaccine-induced immunity and additional indirect protection for unvaccinated persons. A systematic review was conducted to estimate the indirect effect of COVID-19 vaccination. From PubMed and Embase, 31 studies were included describing the impact of original wild-type COVID-19 vaccines on disease transmission or viral load. Overall, study results showed the effectiveness of COVID-19 vaccination against SARS-CoV-2 transmission (range 16–95%), regardless of vaccine type or number of doses. The effect was apparent, but less pronounced against omicron (range 24–95% for pre-omicron variants versus 16–31% for omicron). Results from viral load studies were supportive, showing SARS-CoV-2 infections in vaccinated individuals had higher Ct values, suggesting lower viral load, compared to infections among the unvaccinated. Based on these findings, well-timed vaccination programs may help reduce SARS-CoV-2 transmission—even in the omicron era. Whether better-matched vaccines can improve effectiveness against transmission in the omicron era needs further study.
1. Introduction
The highly contagious coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), first emerged in December 2019 in China and spread across the world in a short period. The World Health Organization (WHO) declared the COVID-19 pandemic on 11 March 2020 [1]. As of September 2023 reported to the WHO, there were 771 million confirmed cases and 7 million deaths caused by COVID-19 worldwide [2].
Before the availability of antivirals and vaccines, primary preventive non-pharmaceutical public health measures were an essential component of the epidemic prevention and control of a new highly contagious disease [3]. Non-pharmaceutical interventions were implemented to reduce the person-to-person transmission of COVID-19 by altering contact rates and patterns, such as lockdowns, social distancing, quarantine, isolation, and wearing masks in public places [4]. Governments worldwide implemented various combinations of non-pharmaceutical interventions with different timing and duration [4]. These non-pharmaceutical interventions contributed to the reduction of the incidence, morbidity, and mortality of COVID-19, but also had other unintended negative health, social, and economic impacts [5,6].
Multiple COVID-19 vaccines were developed to further reduce the morbidity and mortality of COVID-19 [7,8]. The first COVID-19 vaccine was listed by the WHO for emergency use in December 2020, followed by other COVID-19 vaccines and approval for use in many countries [8]. The vaccine roll-out first targeted populations at high risk of infection, severe illness or death from COVID-19, such as frontline healthcare workers and the elderly, followed rapidly by administration of COVID-19 vaccines to the general population [1]. Persons have been vaccinated with various vaccine types and vaccination schedules [1]. After 3.5 years of the COVID-19 pandemic with emerging SARS-CoV-2 variants of concern, the number of cases and deaths have been decreasing steadily, since much of the population has some form of immunity through previous infection or the widespread use of COVID-19 vaccines [2]. This article focuses on the impact of COVID-19 vaccination on the epidemic prevention and control of COVID-19.
In general, vaccination against infectious diseases affords direct individual protection by preventing infection or reducing the development of disease after infection [9]. In addition, mass vaccination can afford indirect vaccine-induced protection benefits for other unvaccinated persons (i.e., herd immunity) [9]. There are two ways vaccination can provide indirect protection by reducing the onward transmission risk [10]. Firstly, a vaccine decreases the probability of a recipient becoming infected by protecting against both symptomatic and asymptomatic infection, resulting in a reduction in the number of infectious persons. Secondly, a vaccine decreases the probability of secondary transmission from persons who have become infected despite vaccination by reducing the degree of infectiousness (i.e., viral load) or duration of viral shedding. Real-time reverse transcriptase polymerase chain reaction (RT-PCR) tests are most frequently used to detect SARS-CoV-2 infection and the cycle threshold (Ct) results are inversely related to viral load [11].
The direct protection of COVID-19 vaccines as measured by their efficacy and effectiveness has been shown in numerous randomized controlled trials and observational studies and is reported in systematic reviews [12,13,14]. The indirect effect of COVID-19 vaccination has less often been studied. We performed a systematic review to describe the indirect effects of COVID-19 vaccination and provide an overview of the trend of these indirect effects. Two review objectives were formulated: (1) what is the indirect effect of COVID-19 vaccination on disease transmission?; and (2) what is the indirect effect of COVID-19 vaccination on viral load, as a proxy for infectiousness?
2. Materials and Methods
This systematic review was conducted following a review protocol and adhering to international methodological standards. The PECO (population–exposure–comparison–outcome) format (Table 1) was used to develop the search strategy. Search strings were compiled for the exposure to COVID-19 vaccination, the outcomes of disease transmission and viral load, and search limits (Supplement Table S1). The systematic literature search was conducted in PubMed and Embase on 16 November 2022. The retrieved records were screened against pre-specified eligibility criteria by a systematic approach; first based on the title and abstract, followed by a screening of the full-text article. The screening was conducted with Rayyan software (Rayyan Systems Inc., Cambridge, MA, USA) by one researcher (A.O.-S.) in close collaboration with a second researcher (M.K.). Disagreements during the screening process were discussed until a consensus was reached. In addition, backward citation searching was applied for references cited in the included studies and selected reviews. The review itself was excluded after the reference check.

Table 1.
PECO (population–exposure–comparison–outcome) for disease transmission and viral load.
Transmission and viral load studies were considered eligible if they reported a statistical comparison between the vaccinated and unvaccinated groups and had a matched study design or applied adjusted analyses. Exclusion criteria were the following: specific population (e.g., immunocompromised), small sample size (n ≤ 30), the vaccinated group is partially vaccinated or also includes partially vaccinated persons (>30% partially vaccinated persons or percentage partially vaccinated persons not reported), other comparators than unvaccinated (i.e., no unvaccinated group, unvaccinated group also includes partially vaccinated persons or placebo), and incomplete reporting of results for our objectives. If multiple articles reporting findings of the same study were retrieved, only the article with the most recent/complete data was included. Preprints were selected initially to search for the peer-reviewed versions of the articles. If at the end of the data extraction phase, this peer-reviewed article was not found, the preprint was excluded.
Data on the characteristics, PECO elements, and results of the included studies were extracted in a spreadsheet in Microsoft Excel. Separate spreadsheets were used for the transmission and viral load studies. To standardize the data extraction, a number of rules were applied. If studies reported results for different variants of concern, this data was preferred over the overall data. If studies reported only stratified data for COVID-19 vaccines, this data was extracted for each vaccine group. If studies reported data for multiple vaccine doses, the most complete vaccine data with the highest amount of vaccine doses was extracted. Most studies reported their data for the overall time since vaccination. If a study reported results only for different periods since vaccination, the data for the shortest period since the last vaccination was extracted (i.e., this concerned one transmission study [15] and five viral load studies [16,17,18,19,20]). If viral load studies reported cycle threshold (Ct) values for different genes, data on one gene were extracted.
The included studies were critically appraised with the 9-point Newcastle–Ottawa quality assessment scales for cohort studies and case–control studies [21]. Studies were classified as high (≤3 points), moderate (4–6 points), or low risk of bias (≥7 points). The data extraction and critical appraisal were done by one researcher (A.O.-S.), unclarities in data reporting in articles were discussed with the other researchers, and the files were reviewed by a second researcher (M.K.).
Based on our review aim and the clinical heterogeneity of the included studies (i.e., different countries and COVID-19 policies, study periods, SARS-CoV-2 variants of concern, vaccines, doses, populations, settings, testing, and outcome evaluated), the data was analyzed narratively and summarized in summary tables and figures. The data was stratified by COVID-19 vaccine (mRNA; mRNA or other vaccine; other vaccine) doses and SARS-CoV-2 variant of concern. When transmission studies reported only odds ratios (OR), relative risks (RR) or hazard ratios (HR), this was converted into vaccine effectiveness against transmission by the calculation VE = (1 − OR) × 100%, VE = (1 − RR) × 100%, or VE = (1 − HR) × 100%. When the odds ratio was reported with the vaccinated group as a reference, this was recalculated first for the unvaccinated reference as 1/OR. The original effect size and effect estimate in vaccine effectiveness against transmission are reported in the summary table.
3. Results
3.1. Study Characteristics
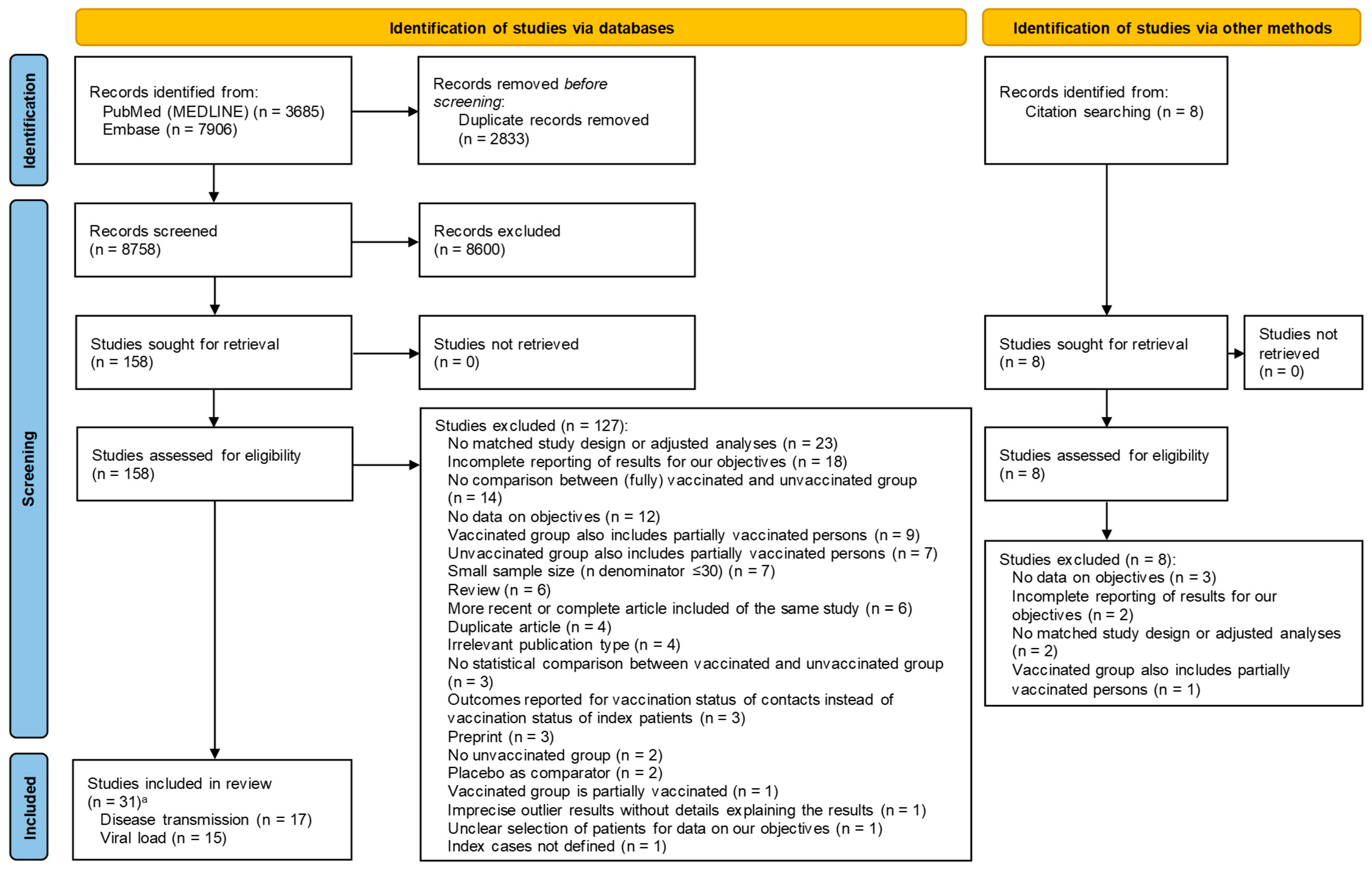
In total, 8758 unique records from PubMed and Embase were screened and 31 studies were selected in this systematic review. Of these, 17 studies [15,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37] reported data on disease transmission, and 15 studies [16,17,18,19,20,27,38,39,40,41,42,43,44,45,46] on viral load (i.e., one study [27] reported on both disease transmission and viral load). The reasons for exclusion at full-text review are enclosed in Figure 1 and Supplement Table S2.
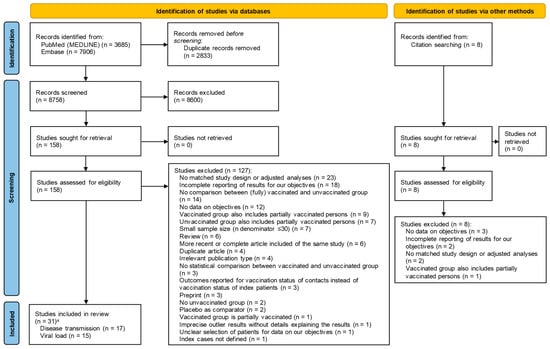
Figure 1.
PRISMA flow diagram. a One study reported on disease transmission and viral load.
Most studies had a retrospective cohort study design (68%) and were conducted in Europe (42%) or the Middle East (29%) (Table 2, Supplement Tables S3 and S4). Transmission studies were mostly conducted in households (82%). The population of the viral load studies was not specified in detail in 10/15 studies. The age and gender of vaccinated and unvaccinated SARS-CoV-2-infected persons were often not reported. Multiple SARS-CoV-2 variants of concern periods were covered in the studies, including alpha, beta, pre-delta, delta, and omicron. Study participants were most often vaccinated with an mRNA vaccine (45%) or a heterologous schedule that included an mRNA dose and another type of COVID-19 vaccine (42%). Transmission and viral load studies had a low (61%) or moderate (39%) risk of bias based on the Newcastle–Ottawa scale (Table 2, Supplement Tables S5 and S6).
Table 2.
Overview of study characteristics of the included studies.
3.2. Vaccine Effects on Transmission
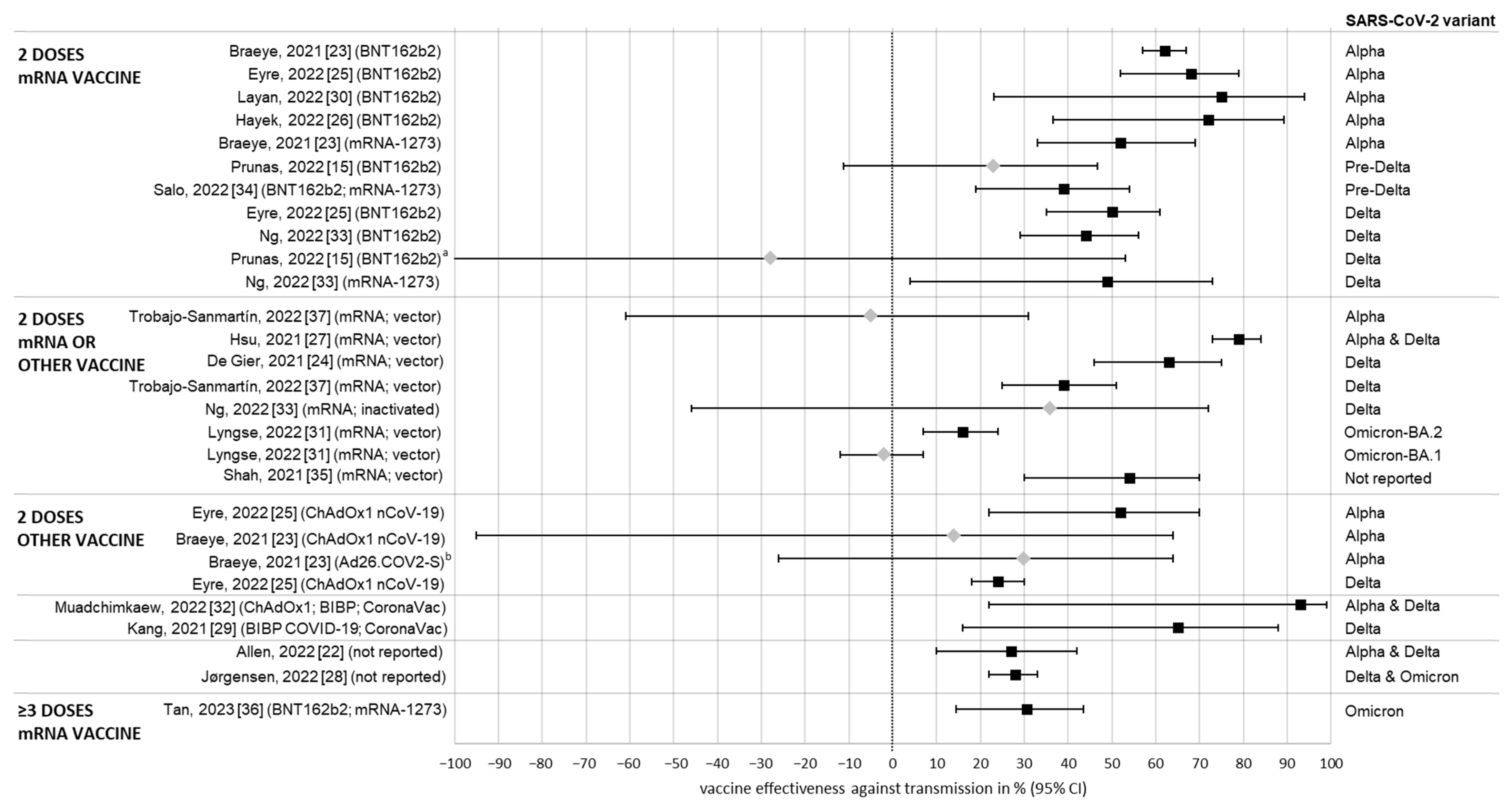
Figure 2 and Supplement Table S7 provide an overview of the effect estimate vaccine effectiveness against transmission. Secondary attack rates for the vaccinated and unvaccinated index cases are reported in Supplement Table S3.
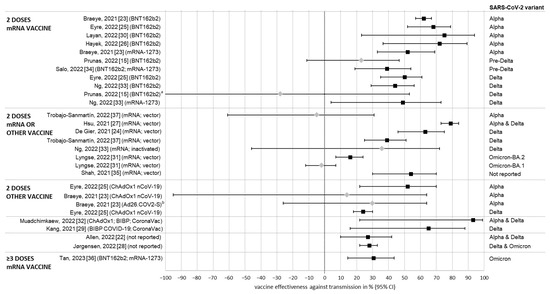
Figure 2.
Vaccine effectiveness against SARS-CoV-2 transmission in vaccinated versus unvaccinated index cases. a Lower confidence interval limit −249%; b 1 dose schedule of Ad26.COV2-S vaccine.  Significant effect.
Significant effect.  Non-significant effect.
Non-significant effect.
Significant effect. Non-significant effect.
Overall, a COVID-19 vaccination showed effectiveness against transmission, regardless of vaccine type, number of doses, or SARS-CoV-2 variant of concern. Of the study results, 75% (21/28) showed a significant effect of vaccinated versus unvaccinated index cases on the vaccine effectiveness against transmission ranging from 16% to 95%; the remaining 25% (7/28) of the study results did not show a significant effect of COVID-19 vaccination of index cases. In 81% (17/21) of these study results, effectiveness against transmission was >30% and 57% (12/21) of the study results were >50%. Effectiveness against transmission seems to be lower for the more recent variants of concern, ranging from 39% to 75% during the pre-delta period, 24% to 65% during delta, and from 16% to 31% during the omicron period.
3.3. Vaccine Effects on Viral Load
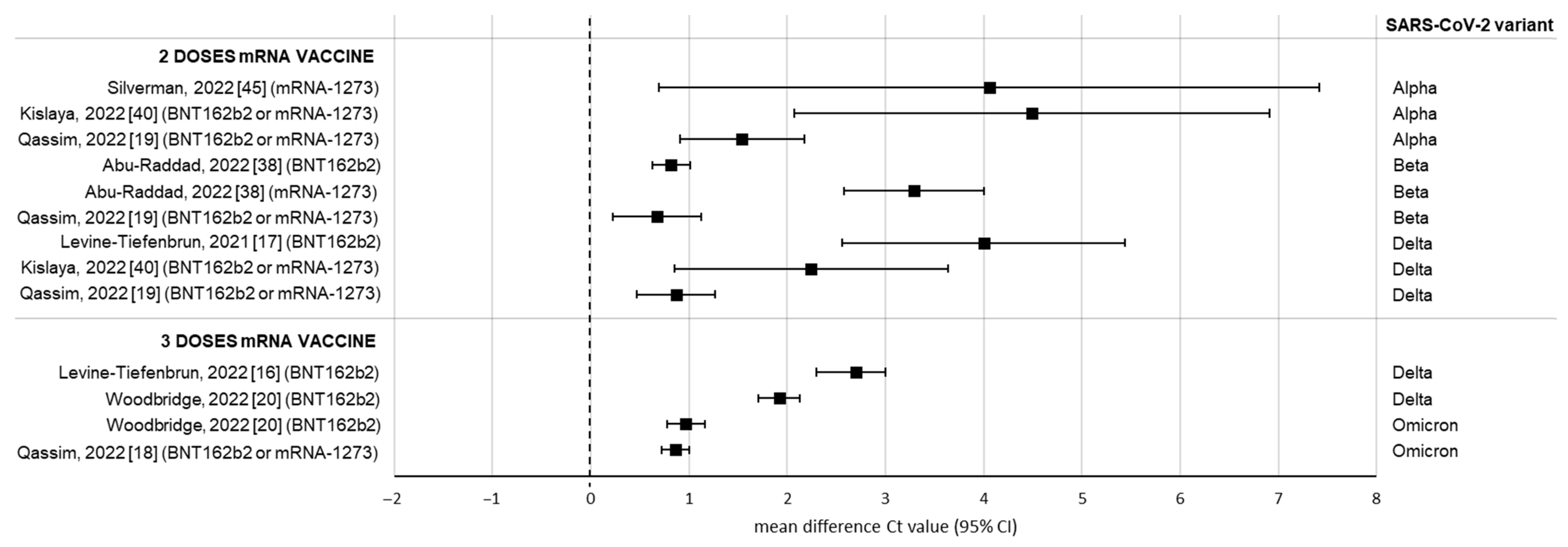
Effect estimates of the viral load studies expressed as the mean difference in Ct values between vaccinated and unvaccinated SARS-CoV-2-infected persons are summarized in Figure 3 and Supplement Table S8. Mean or median Ct values or viral load (i.e., if no Ct values were reported) for the vaccinated and unvaccinated groups are reported in Supplement Table S4.
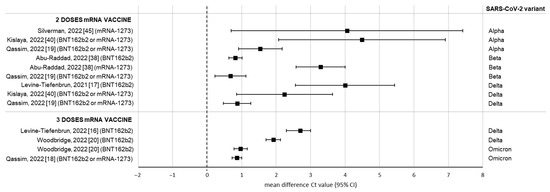
Figure 3.
Mean difference in Ct values between vaccinated versus unvaccinated SARS-CoV-2-infected persons (i.e., higher Ct values for the vaccinated group, suggesting lower viral load). Significant effect.
Significant effect.
All results in Figure 3 show a positive trend of COVID-19 vaccination on Ct values, with significant mean differences in Ct values for the vaccinated group versus the unvaccinated group ranging from 0.7 to 4.5 (i.e., higher Ct values for the vaccinated group, suggesting lower viral load). These mean differences in Ct values for the successive variants of concern during the pandemic became smaller, with smaller differences observed during the omicron period.
In addition, results from three studies with Ct data could not be included in the figure because of missing data. Two studies [27,41] reported significantly increased Ct values for vaccinated versus unvaccinated SARS-CoV-2-infected persons during the alpha and alpha/delta period and two studies [41,43] reported no significant effect of COVID-19 vaccination on Ct values during delta (Supplement Table S8). Four studies [39,42,44,46] reported results only on the outcome viral load for different variants of concern: three results showed a significantly decreased viral load for the vaccinated group for pre-delta and delta and three results showed a non-significant decreased viral load for delta and omicron (Supplement Table S8).
4. Discussion
Despite considerable clinical heterogeneity among the included transmission studies, published studies to date suggest the effectiveness of COVID-19 vaccines against transmission. COVID-19 vaccination reduced the transmission of SARS-CoV-2 regardless of vaccine type, number of doses, or SARS-CoV-2 variant of concern (range 16% to 95% versus unvaccinated). Statistically significant effectiveness against transmission was shown in 75% of the study results. This indicates that after a breakthrough infection, vaccinated persons have reduced infectiousness and a smaller chance of further transmission of SARS-CoV-2 to their contacts, although these findings were less pronounced in the omicron era.
The primary focus of vaccine development is to provide direct protection to help reduce clinical manifestations of infection, such as reducing disease severity or decreasing the rate of hospitalization or death. Direct protection is crucial to demonstrate the licensure of new vaccines [7,9], and COVID-19 vaccines have been shown to reduce COVID-19 incidence, hospitalization, and mortality [12,13,14]. However, vaccines often also contribute to infectious disease control by providing indirect protection by reducing the onward transmission risk [7,9]. Most notable examples were observed following the introduction of meningococcal and pneumococcal conjugate vaccines, with reductions of approximately 50% in disease incidence in unvaccinated populations [47]. Even for viral respiratory pathogens such as influenza, which is more similar to COVID-19 in terms of disease characteristics, there is evidence that childhood influenza vaccination may offer indirect protection to susceptible unvaccinated persons in settings such as household members, elderly, and other close contacts [48]. Based on our systematic review, COVID-19 vaccination showed effectiveness against SARS-CoV-2 transmission and led to lower viral loads compared to the unvaccinated. Although this effect was less pronounced against omicron, well-timed vaccination programs may help reduce SARS-CoV-2 transmission.
Over time, SARS-CoV-2 evolved in different variants of concern through genetic mutations. Compared to the previous variants of concern, omicron has many genetic mutations in the Spike protein that increase transmissibility and the ability to partial vaccine-induced immune escape, resulting in an increase in the number of infections [49]. The COVID-19 vaccines were developed based on the Spike protein of the ancestral SARS-CoV-2 strain and the mutations of the omicron variant of concern have decreased the vaccine effectiveness and led to re-infection [49]. Infections with omicron have been milder in comparison with the previous variants, with regard to the risk of hospitalization, need for mechanical ventilation, and death. However, these data must be interpreted in the context of continually evolving population immunity derived from previous infection and/or COVID-19 vaccination [49]. Whether better-matched vaccines can improve vaccine effectiveness against transmission in the omicron era needs further study. Regardless, the value of indirect benefits of COVID-19 vaccination should be taken into consideration when evaluating vaccination strategies or assessing the economic value of vaccination.
Considering the potential rapid surge in COVID-19 cases [50], the timing of COVID-19 vaccination programs to reduce SARS-CoV-2 transmission may be incorporated when COVID-19 displays a seasonal pattern. This is defined as the seasonality of a virus: variations in the virus prevalence across geographical regions at more or less regular intervals throughout the year [51,52]. Seasonality is more pronounced in regions with greater distance from the equator and has a different timing in the Northern and Southern hemispheres [51,52,53]. Outbreaks of respiratory viruses such as the human influenza virus, respiratory syncytial virus, and coronaviruses follow a seasonal pattern with higher prevalence during the winter period [52,53]. Whether COVID-19 displays a seasonal pattern is still under study. When a seasonal pattern of COVID-19 is shown, seasonal vaccination programs could be implemented instead of a year-round vaccination program to make the development and implementation of COVID-19 vaccines more effective and efficient. Furthermore, timing and preparedness are important aspects of pandemic control of highly contagious diseases such as COVID-19. When timed early during a pandemic, interventions are more effective and could substantially reduce transmission in household and community settings. Evidence from previous pandemics indicates that vaccination prior to the outbreak, before the peak of infections, is highly cost-effective [54]. Although vaccinating past the peak of infections may not be cost-effective, during the COVID-19 pandemic with multiple waves of infections, it seemed to be worth vaccinating past the peak, as there may be future waves of infections once the non-pharmaceutical interventions were eased [54].
It is challenging to assess the effect size of COVID-19 vaccination on transmission and to separate this from other factors that changed the SARS-CoV-2 circulation, for example, the shifting vaccine uptake which might vary over time as the perceived risk varies, the waning effect of vaccination, the prevalence of natural infections, elimination of preventive non-pharmaceutical interventions, and the emergence of novel variants with different levels of infectivity and transmissibility [55,56]. When mutant variants evolve with characteristics different from their ancestral strains this might affect the effectiveness of the COVID-19 vaccines, given the vaccines evaluated in the included studies (i.e., original wild-type vaccines) were designed based on the earlier variants of SARS-CoV-2 [55,56]. Furthermore, viral load studies are challenged by their use of Ct values as outcomes. RT-PCR tests are the gold standard for SARS-CoV-2 detection and based on the amount of viral RNA in the sample provide a qualitative result (i.e., detected/not detected) and quantitative result (i.e., Ct value; with lower Ct values indicative of higher viral load) [11]. Although viral load is a proxy for infectiousness, positive RT-PCR results do not necessarily imply a viable virus [11]. Precaution should be taken interpreting Ct data because currently there is no universal Ct value threshold to predict infectivity, Ct values can vary significantly across and within testing platforms, and Ct values vary during the course of a SARS-CoV-2 infection and with different virus variants [11].
This systematic review has several limitations. Firstly, the heterogeneity of the included studies such as different countries, study periods, SARS-CoV-2 variants, vaccines, populations, testing, and outcome measures. Though heterogeneity is inevitable, this was tackled partly by including only studies with a matched design or adjusted analyses. Most of the other factors that might change the SARS-CoV-2 circulation as described above, such as differences in non-pharmaceutical intervention policies, were not implemented in the analyses of the included studies. In mathematical modeling studies it is possible to take the effects and uncertainties of these factors into account in different scenarios and sensitivity analyses, and, for example, examine the effects of vaccine roll-out in combination with the relaxation of non-pharmaceutical interventions [4,57]. Secondly, some study results are outdated for the current SARS-CoV-2 situation. Early studies had low vaccination coverage and the vaccinated and unvaccinated populations are likely to be different in multiple aspects from the more recent studies, for example with regard to priority for vaccinating high-risk populations and willingness or unwillingness to vaccinate. However, we still saw an effect during the omicron period. Thirdly, incomplete reporting of data in the transmission and viral load studies, such as lacking patient characteristics or not reporting all data on the outcomes. Viral load was often not a primary outcome of interest.
There are several challenges with quantifying the indirect effects of COVID-19 vaccination accurately. Studies on transmission are less often conducted than studies on the direct protection of vaccines and heterogeneity will always be an element of these studies. For future studies, we would therefore recommend implementing standardization of variables where possible (e.g., testing platform and timing of test after infection and vaccination), applying matched designs or adjusted analyses, avoiding self-reported data, and more complete reporting of the data. Prospective designs will contribute to the completeness of data collection. We also observed that part of the studies did not have large sample sizes to evaluate the indirect effectiveness of the COVID-19 vaccine with clear certainty. Therefore, it is critical to design more robust and homogeneous studies across several geographical locations with adequate sample sizes to quantify the indirect effects of COVID-19 vaccination for different clinical outcomes and study populations so that the results can be confirmed and replicated. Studies with new methodological approaches to measuring accurate indirect effects are also needed to overcome these inherent limitations presented in modeling and real-world observational studies.
5. Conclusions
In conclusion, based on a systematic review, COVID-19 vaccination showed effectiveness against SARS-CoV-2 transmission and led to lower viral loads compared to the unvaccinated. Although this effect was less pronounced against omicron, well-timed vaccination programs may help reduce SARS-CoV-2 transmission. Future studies should evaluate the impact of updated omicron-adapted vaccines on transmission.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/covid3100103/s1, Supplement Table S1: search strategy; Supplement Table S2: primary reasons for exclusion by each excluded study at full-text review; Supplement Table S3: study characteristics of the transmission studies; Supplement Table S4: study characteristics of the viral load studies; Supplement Table S5: risk of bias assessment with the Newcastle–Ottawa Scale of the transmission studies; Supplement Table S6: risk of bias assessment with the Newcastle–Ottawa Scale of the viral load studies; Supplement Table S7: summary of effect estimates of the transmission studies; Supplement Table S8: summary of effect estimates of the viral load studies. References [15,16,17,18,19,20,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46] are cited in the Supplementary Materials.
Author Contributions
A.O.-S. and M.H.K. conceived and designed the study. A.O.-S. analyzed the data. A.O.-S. and M.H.K. wrote the first draft and are accountable for the accuracy and integrity of the contents of the manuscript. A.O.-S., M.H.K., J.S., C.M., J.Y., G.M. and J.M.M. interpreted the results. All authors provided critical revisions of the manuscript for the intellectual content. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Pfizer Inc.
Conflicts of Interest
A.O.-S. is a freelance systematic reviewer who was under contract with Pfizer Inc. for this systematic review. J.S., C.M., J.Y., G.M., J.M.M. and M.H.K. are employees of Pfizer Inc.
References
- World Health Organization. Timeline: WHO’s COVID-19 Response. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/interactive-timeline# (accessed on 31 March 2023).
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 18 September 2023).
- Zhou, F.; Hu, T.-J.; Zhang, X.-Y.; Lai, K.; Chen, J.-H.; Zhou, X.-H. The Association of Intensity and Duration of Non-Pharmacological Interventions and Implementation of Vaccination with COVID-19 Infection, Death, and Excess Mortality: Natural Experiment in 22 European Countries. J. Infect. Public Health 2022, 15, 499–507. [Google Scholar] [CrossRef]
- Lison, A.; Banholzer, N.; Sharma, M.; Mindermann, S.; Unwin, H.J.T.; Mishra, S.; Stadler, T.; Bhatt, S.; Ferguson, N.M.; Brauner, J. Effectiveness Assessment of Non-Pharmaceutical Interventions: Lessons Learned from the COVID-19 Pandemic. Lancet Public Health 2023, 8, e311–e317. [Google Scholar] [CrossRef]
- Iezadi, S.; Gholipour, K.; Azami-Aghdash, S.; Ghiasi, A.; Rezapour, A.; Pourasghari, H.; Pashazadeh, F. Effectiveness of Non-Pharmaceutical Public Health Interventions against COVID-19: A Systematic Review and Meta-Analysis. PLoS ONE 2021, 16, e0260371. [Google Scholar] [CrossRef]
- Talic, S.; Shah, S.; Wild, H.; Gasevic, D.; Maharaj, A.; Ademi, Z.; Li, X.; Xu, W.; Mesa-Eguiagaray, I.; Rostron, J. Effectiveness of Public Health Measures in Reducing the Incidence of COVID-19, SARS-CoV-2 Transmission, and COVID-19 Mortality: Systematic Review and Meta-Analysis. BMJ 2021, 375, e068302. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, S.H.; Mansatta, K.; Mallett, G.; Harris, V.; Emary, K.R.W.; Pollard, A.J. What Defines an Efficacious COVID-19 Vaccine? A Review of the Challenges Assessing the Clinical Efficacy of Vaccines against SARS-CoV-2. Lancet Infect. Dis. 2021, 21, e26–e35. [Google Scholar] [CrossRef]
- Young, M.; Crook, H.; Scott, J.; Edison, P. COVID-19: Virology, Variants, and Vaccines. BMJ Med. 2022, 1, e000040. [Google Scholar] [CrossRef] [PubMed]
- Pollard, A.J.; Bijker, E.M. A Guide to Vaccinology: From Basic Principles to New Developments. Nat. Rev. Immunol. 2021, 21, 83–100. [Google Scholar] [CrossRef]
- Richterman, A.; Meyerowitz, E.A.; Cevik, M. Indirect Protection by Reducing Transmission: Ending the Pandemic with Severe Acute Respiratory Syndrome Coronavirus 2 Vaccination. Open Forum Infect. Dis. 2022, 9, ofab259. [Google Scholar] [CrossRef] [PubMed]
- Binnicker, M.J. Can Testing Predict SARS-CoV-2 Infectivity? The Potential for Certain Methods to Be Surrogates for Replication-Competent Virus. J. Clin. Microbiol. 2021, 59, e00469-21. [Google Scholar] [CrossRef]
- Cochrane Emergency Critical Care Group. Efficacy and Safety of COVID-19 Vaccines. Cochrane Database Syst. Rev. 2023, 12, CD015477. [Google Scholar]
- Rahmani, K.; Shavaleh, R.; Forouhi, M.; Disfani, H.F.; Kamandi, M.; Oskooi, R.K.; Foogerdi, M.; Soltani, M.; Rahchamani, M.; Mohaddespour, M. The Effectiveness of COVID-19 Vaccines in Reducing the Incidence, Hospitalization, and Mortality from COVID-19: A Systematic Review and Meta-Analysis. Front. Public Health 2022, 10, 2738. [Google Scholar] [CrossRef]
- Zeng, B.; Gao, L.; Zhou, Q.; Yu, K.; Sun, F. Effectiveness of COVID-19 Vaccines against SARS-CoV-2 Variants of Concern: A Systematic Review and Meta-Analysis. BMC Med. 2022, 20, 200. [Google Scholar] [CrossRef] [PubMed]
- Prunas, O.; Warren, J.L.; Crawford, F.W.; Gazit, S.; Patalon, T.; Weinberger, D.M.; Pitzer, V.E. Vaccination with Bnt162b2 Reduces Transmission of SARS-CoV-2 to Household Contacts in Israel. Science 2022, 375, 1151–1154. [Google Scholar] [CrossRef] [PubMed]
- Levine-Tiefenbrun, M.; Yelin, I.; Alapi, H.; Herzel, E.; Kuint, J.; Chodick, G.; Gazit, S.; Patalon, T.; Kishony, R. Waning of SARS-CoV-2 Booster Viral-Load Reduction Effectiveness. Nat. Commun. 2022, 13, 1237. [Google Scholar] [CrossRef]
- Levine-Tiefenbrun, M.; Yelin, I.; Alapi, H.; Katz, R.; Herzel, E.; Kuint, J.; Chodick, G.; Gazit, S.; Patalon, T.; Kishony, R. Viral Loads of Delta-Variant SARS-CoV-2 Breakthrough Infections after Vaccination and Booster with Bnt162b2. Nat. Med. 2021, 27, 2108–2110. [Google Scholar] [CrossRef]
- Qassim, S.H.; Chemaitelly, H.; Ayoub, H.H.; AlMukdad, S.; Tang, P.; Hasan, M.R.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Abdul-Rahim, H.F.; et al. Effects of Ba.1/Ba.2 Subvariant, Vaccination and Prior Infection on Infectiousness of SARS-CoV-2 Omicron Infections. J. Travel Med. 2022, 29, taac068. [Google Scholar] [CrossRef]
- Qassim, S.H.; Hasan, M.R.; Tang, P.; Chemaitelly, H.; Ayoub, H.H.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Abdul-Rahim, H.F.; Nasrallah, G.K.; et al. Effects of SARS-CoV-2 Alpha, Beta, and Delta Variants, Age, Vaccination, and Prior Infection on Infectiousness of SARS-COV-2 Infections. Front. Immunol. 2022, 13, 984784. [Google Scholar] [CrossRef]
- Woodbridge, Y.; Amit, S.; Huppert, A.; Kopelman, N.M. Viral Load Dynamics of SARS-CoV-2 Delta and Omicron Variants Following Multiple Vaccine Doses and Previous Infection. Nat. Commun. 2022, 13, 6706. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 9 January 2023).
- Allen, H.; Vusirikala, A.; Flannagan, J.; Twohig, K.A.; Zaidi, A.; Chudasama, D.; Lamagni, T.; Groves, N.; Turner, C.; Rawlinson, C.; et al. Household Transmission of COVID-19 Cases Associated with SARS-CoV-2 Delta Variant (B.1.617.2): National Case-Control Study. Lancet Reg. Health Eur. 2022, 12, 100252. [Google Scholar] [CrossRef] [PubMed]
- Braeye, T.; Cornelissen, L.; Catteau, L.; Haarhuis, F.; Proesmans, K.; De Ridder, K.; Djiena, A.; Mahieu, R.; De Leeuw, F.; Dreuw, A.; et al. Vaccine Effectiveness against Infection and Onwards Transmission of COVID-19: Analysis of Belgian Contact Tracing Data, January-June 2021. Vaccine 2021, 39, 5456–5460. [Google Scholar] [CrossRef]
- De Gier, B.; Andeweg, S.; Backer, J.A.; Hahné, S.J.M.; van den Hof, S.; de Melker, H.E.; Knol, M.J. Vaccine Effectiveness against SARS-CoV-2 Transmission to Household Contacts During Dominance of Delta Variant (B.1.617.2), the Netherlands, August to September 2021. Eurosurveillance 2021, 26, 2100977. [Google Scholar] [CrossRef]
- Eyre, D.W.; Taylor, D.; Purver, M.; Chapman, D.; Fowler, T.; Pouwels, K.B.; Walker, A.S.; Peto, T.E.A. Effect of COVID-19 Vaccination on Transmission of Alpha and Delta Variants. N. Engl. J. Med. 2022, 386, 744–756. [Google Scholar] [CrossRef] [PubMed]
- Hayek, S.; Shaham, G.; Ben-Shlomo, Y.; Kepten, E.; Dagan, N.; Nevo, D.; Lipsitch, M.; Reis, B.Y.; Balicer, R.D.; Barda, N. Indirect Protection of Children from SARS-CoV-2 Infection through Parental Vaccination. Science 2022, 375, 1155–1159. [Google Scholar] [CrossRef]
- Hsu, L.; Grüne, B.; Buess, M.; Joisten, C.; Klobucnik, J.; Nießen, J.; Patten, D.; Wolff, A.; Wiesmüller, G.A.; Kossow, A.; et al. COVID-19 Breakthrough Infections and Transmission Risk: Real-World Data Analyses from Germany’s Largest Public Health Department (Cologne). Vaccines 2021, 9, 1267. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, S.B.; Nygård, K.; Kacelnik, O.; Telle, K. Secondary Attack Rates for Omicron and Delta Variants of SARS-CoV-2 in Norwegian Households. JAMA—J. Am. Med. Assoc. 2022, 327, 1610–1611. [Google Scholar] [CrossRef]
- Kang, M.; Xin, H.; Yuan, J.; Ali, S.T.; Liang, Z.; Zhang, J.; Hu, T.; Lau, E.H.; Zhang, Y.; Zhang, M.; et al. Transmission Dynamics and Epidemiological Characteristics of SARS-CoV-2 Delta Variant Infections in Guangdong, China, May to June 2021. Eurosurveillance 2022, 27, 2100815. [Google Scholar] [CrossRef] [PubMed]
- Layan, M.; Gilboa, M.; Gonen, T.; Goldenfeld, M.; Meltzer, L.; Andronico, A.; Hozé, N.; Cauchemez, S.; Regev-Yochay, G. Impact of Bnt162b2 Vaccination and Isolation on SARS-CoV-2 Transmission in Israeli Households: An Observational Study. Am. J. Epidemiol. 2022, 191, 1224–1234. [Google Scholar] [CrossRef]
- Lyngse, F.P.; Kirkeby, C.T.; Denwood, M.; Christiansen, L.E.; Mølbak, K.; Møller, C.H.; Skov, R.L.; Krause, T.G.; Rasmussen, M.; Sieber, R.N.; et al. Household Transmission of SARS-CoV-2 Omicron Variant of Concern Subvariants Ba.1 and Ba.2 in Denmark. Nat. Commun. 2022, 13, 5760. [Google Scholar] [CrossRef]
- Muadchimkaew, M.; Siripongboonsitti, T.; Wongpatcharawarakul, S.; Boonsankaew, C.; Tawinprai, K.; Soonklang, K.; Mahanonda, N. Effect of Inactivated SARS-CoV-2 Vaccines and Chadox1 Ncov-19 Vaccination to Prevent COVID-19 in Thai Households (Vacprevent Trial). Int. J. Infect. Dis. 2022, 124, 190–198. [Google Scholar] [CrossRef]
- Ng, O.T.; Koh, V.; Chiew, C.J.; Marimuthu, K.; Thevasagayam, N.M.; Mak, T.M.; Chua, J.K.; Ong, S.S.H.; Lim, Y.K.; Ferdous, Z.; et al. Impact of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Vaccination and Pediatric Age on Delta Variant Household Transmission. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2022, 75, e35–e43. [Google Scholar] [CrossRef]
- Salo, J.; Hägg, M.; Kortelainen, M.; Leino, T.; Saxell, T.; Siikanen, M.; Sääksvuori, L. The Indirect Effect of Mrna-Based COVID-19 Vaccination on Healthcare Workers’ Unvaccinated Household Members. Nat. Commun. 2022, 13, 1162. [Google Scholar] [CrossRef]
- Shah, A.S.V.; Gribben, C.; Bishop, J.; Hanlon, P.; Caldwell, D.; Wood, R.; Reid, M.; McMenamin, J.; Goldberg, D.; Stockton, D.; et al. Effect of Vaccination on Transmission of SARS-CoV-2. N. Engl. J. Med. 2021, 385, 1718–1720. [Google Scholar] [CrossRef]
- Tan, S.T.; Kwan, A.T.; Rodríguez-Barraquer, I.; Singer, B.J.; Park, H.J.; Lewnard, J.A.; Sears, D.; Lo, N.C. Infectiousness of SARS-CoV-2 Breakthrough Infections and Reinfections During the Omicron Wave. Nat. Med. 2023, 29, 358–365. [Google Scholar] [CrossRef]
- Trobajo-Sanmartín, C.; Martínez-Baz, I.; Miqueleiz, A.; Fernández-Huerta, M.; Burgui, C.; Casado, I.; Baigorría, F.; Navascués, A.; Castilla, J.; Ezpeleta, C. Differences in Transmission between SARS-CoV-2 Alpha (B.1.1.7) and Delta (B.1.617.2) Variants. Microbiol. Spectr. 2022, 10, e00008-22. [Google Scholar] [CrossRef]
- Abu-Raddad, L.J.; Chemaitelly, H.; Ayoub, H.H.; Tang, P.; Coyle, P.; Hasan, M.R.; Yassine, H.M.; Benslimane, F.M.; Al-Khatib, H.A.; Al-Kanaani, Z.; et al. Relative Infectiousness of SARS-CoV-2 Vaccine Breakthrough Infections, Reinfections, and Primary Infections. Nat. Commun. 2022, 13, 532. [Google Scholar] [CrossRef] [PubMed]
- Bramante, C.T.; Proper, J.L.; Boulware, D.R.; Karger, A.B.; Murray, T.; Rao, V.; Hagen, A.; Tignanelli, C.J.; Puskarich, M.; Cohen, K.; et al. Vaccination against SARS-CoV-2 Is Associated with a Lower Viral Load and Likelihood of Systemic Symptoms. Open Forum Infect. Dis. 2022, 9, ofac066. [Google Scholar] [CrossRef]
- Kislaya, I.; Rodrigues, E.F.; Borges, V.; Gomes, J.P.; Sousa, C.; Almeida, J.P.; Peralta-Santos, A.; Nunes, B. Comparative Effectiveness of Coronavirus Vaccine in Preventing Breakthrough Infections among Vaccinated Persons Infected with Delta and Alpha Variants. Emerg. Infect. Dis. 2022, 28, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Pouwels, K.B.; Pritchard, E.; Matthews, P.C.; Stoesser, N.; Eyre, D.W.; Vihta, K.D.; House, T.; Hay, J.; Bell, J.I.; Newton, J.N.; et al. Effect of Delta Variant on Viral Burden and Vaccine Effectiveness against New SARS-CoV-2 Infections in the Uk. Nat. Med. 2021, 27, 2127–2135. [Google Scholar] [CrossRef] [PubMed]
- Puhach, O.; Adea, K.; Hulo, N.; Sattonnet, P.; Genecand, C.; Iten, A.; Jacquérioz, F.; Kaiser, L.; Vetter, P.; Eckerle, I.; et al. Infectious Viral Load in Unvaccinated and Vaccinated Individuals Infected with Ancestral, Delta or Omicron SARS-CoV-2. Nat. Med. 2022, 28, 1491–1500. [Google Scholar] [CrossRef]
- Riemersma, K.K.; Haddock, L.A., III; Wilson, N.A.; Minor, N.; Eickhoff, J.; Grogan, B.E.; Kita-Yarbro, A.; Halfmann, P.J.; Segaloff, H.E.; Kocharian, A. Shedding of Infectious SARS-CoV-2 Despite Vaccination. PLoS Pathog. 2022, 18, e1010876. [Google Scholar] [CrossRef]
- Rife Magalis, B.; Rich, S.; Tagliamonte, M.S.; Mavian, C.; Cash, M.N.; Riva, A.; Marini, S.; Amador, D.M.; Zhang, Y.; Shapiro, J.; et al. Severe Acute Respiratory Syndrome Coronavirus 2 Delta Vaccine Breakthrough Transmissibility in Alachua County, Florida. Clin. Infect. Dis. 2022, 75, 1618–1627. [Google Scholar] [CrossRef]
- Silverman, R.A.; Ceci, A.; Cohen, A.; Helmick, M.; Short, E.; Bordwine, P.; Friedlander, M.J.; Finkielstein, C.V. Vaccine Effectiveness During Outbreak of COVID-19 Alpha (B.1.1.7) Variant in Men’s Correctional Facility, United States. Emerg. Infect. Dis. 2022, 28, 1321–1326. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.G.; Yoon, S.K.; Naleway, A.L.; Meece, J.; Fabrizio, T.P.; Caban-Martinez, A.J.; Burgess, J.L.; Gaglani, M.; Olsho, L.E.W.; Bateman, A.; et al. Association of Mrna Vaccination with Clinical and Virologic Features of COVID-19 among Us Essential and Frontline Workers. JAMA 2022, 328, 1523–1533. [Google Scholar] [PubMed]
- Stephens, D.S. Protecting the Herd: The Remarkable Effectiveness of the Bacterial Meningitis Polysaccharide-Protein Conjugate Vaccines in Altering Transmission Dynamics. Trans. Am. Clin. Climatol. Assoc. 2011, 122, 115. [Google Scholar]
- Yin, J.K.; Heywood, A.E.; Georgousakis, M.; King, C.; Chiu, C.; Isaacs, D.; Macartney, K.K. Systematic Review and Meta-Analysis of Indirect Protection Afforded by Vaccinating Children against Seasonal Influenza: Implications for Policy. Clin. Infect. Dis. 2017, 65, 719–728. [Google Scholar] [CrossRef]
- Pather, S.; Madhi, S.A.; Cowling, B.J.; Moss, P.; Kamil, J.P.; Ciesek, S.; Muik, A.; Türeci, Ö. SARS-CoV-2 Omicron Variants: Burden of Disease, Impact on Vaccine Effectiveness and Need for Variant-Adapted Vaccines. Front. Immunol. 2023, 14, 1130539. [Google Scholar] [CrossRef] [PubMed]
- Kinross, P.; Suetens, C.; Dias, J.G.; Alexakis, L.; Wijermans, A.; Colzani, E.; Monnet, D.L. Rapidly Increasing Cumulative Incidence of Coronavirus Disease (COVID-19) in the European Union/European Economic Area and the United Kingdom, 1 January to 15 March 2020. Eurosurveillance 2020, 25, 2000285. [Google Scholar] [CrossRef]
- Kronfeld-Schor, N.; Stevenson, T.J.; Nickbakhsh, S.; Schernhammer, E.S.; Dopico, X.C.; Dayan, T.; Martinez, M.; Helm, B. Drivers of Infectious Disease Seasonality: Potential Implications for COVID-19. J. Biol. Rhythm. 2021, 36, 35–54. [Google Scholar] [CrossRef]
- Neumann, G.; Kawaoka, Y. Seasonality of Influenza and Other Respiratory Viruses. EMBO Mol. Med. 2022, 14, e15352. [Google Scholar] [CrossRef]
- Li, Y.; Reeves, R.M.; Wang, X.; Bassat, Q.; Brooks, W.A.; Cohen, C.; Moore, D.P.; Nunes, M.; Rath, B.; Campbell, H. Global Patterns in Monthly Activity of Influenza Virus, Respiratory Syncytial Virus, Parainfluenza Virus, and Metapneumovirus: A Systematic Analysis. Lancet Glob. Health 2019, 7, e1031–e1045. [Google Scholar] [CrossRef]
- Juneau, C.-E.; Pueyo, T.; Bell, M.; Gee, G.; Collazzo, P.; Potvin, L. Lessons from Past Pandemics: A Systematic Review of Evidence-Based, Cost-Effective Interventions to Suppress COVID-19. Syst. Rev. 2022, 11, 90. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.M.; Masum, M.H.U.; Wajed, S.; Talukder, A. A Comprehensive Review on COVID-19 Vaccines: Development, Effectiveness, Adverse Effects, Distribution and Challenges. Virusdisease 2022, 33, 1–22. [Google Scholar] [CrossRef] [PubMed]
- She, J.; Hou, D.; Chen, C.; Bi, J.; Song, Y. Challenges of Vaccination and Herd Immunity in COVID-19 and Management Strategies. Clin. Respir. J. 2022, 16, 708–716. [Google Scholar] [CrossRef] [PubMed]
- Sonabend, R.; Whittles, L.K.; Imai, N.; Perez-Guzman, P.N.; Knock, E.S.; Rawson, T.; Gaythorpe, K.A.M.; Djaafara, B.A.; Hinsley, W.; FitzJohn, R.G. Non-Pharmaceutical Interventions, Vaccination, and the SARS-CoV-2 Delta Variant in England: A Mathematical Modelling Study. Lancet 2021, 398, 1825–1835. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).