1. Introduction
Anthropometric measurement, known as perimetry, refers to the assessment of the circumference of a body segment, performed using an anthropometric tape measure and applying an appropriate technique to ensure the measurement is taken perpendicularly to the body segment in question [
1,
2]. Accuracy in obtaining these measurements is essential for data collection in various fields, such as health, ergonomics, and sports [
2,
3]. The flexed and tensed arm (FTA) circumference is one of the main anthropometric variables used, assisting in the monitoring of muscle development, body composition, and body shape. Previously, this anthropometric measurement was used along with leg circumference, through the ratio of flexed and tensed arm circumference to leg circumference, as a criterion for suspected muscle dysmorphia [
4]. More recently, a positive correlation between flexed and tensed arm circumference and lean body mass was observed [
5]. Additionally, this measurement is also one of the ten variables in a recognized model for the study of somatotype, specifically within the mesomorphic component [
6].
According to ISAK [
7], flexed and tensed arm circumference should be measured perpendicularly to the longitudinal axis, at the highest point of the contracted biceps brachii, with the subject positioning the right arm at 90° relative to the body, the elbow flexed at 90°, and the forearm in supination. The protocol establishes two possibilities for performing this measurement: with the left hand opposing the right arm, ensuring maximum voluntary contraction, or by performing maximum voluntary contraction without contralateral opposition. Opposition is recommended to help the subject achieve maximum contraction, based on the assumption that in individuals with low levels of physical activity, elbow flexion and voluntary contraction of the elbow flexors (mainly the biceps brachii and brachialis) alone may not be sufficient to reach the largest possible arm circumference. However, to our knowledge, no research has investigated the influence of contralateral opposition on both the measurement of the flexed and tensed arm circumference or muscle activation.
From a practical standpoint, variations in anthropometric protocols can represent a significant source of error, compromising the reliability of measurements and derived variables. For example, Cintra-Andrade et al. [
8] demonstrated that the size of the skinfold during measurement can substantially influence the obtained value, even affecting the estimation of body fat percentage. This variation constitutes a relevant factor contributing to the technical error of measurement (TEM). Regarding circumference measurements, Lennie et al. [
9] reported arm position during waist circumference assessment had a direct impact on the results, highlighting the need for caution when interpreting studies that do not clearly specify upper limb positioning. These findings reinforce the importance of strict standardization of anthropometric procedures to ensure the validity and comparability of data.
In most studies, it is unclear whether contralateral opposition was used, while a few, such as Oliveira and Araújo [
4], explicitly state opposition was applied to all participants. The main discussion regarding the use of opposition revolves around the criteria for its application, considering factors such as physical activity level, age, sex, and involvement in motor sports requiring elbow flexion. Additionally, it is still unclear whether the use of opposition affects variables dependent on this measure, such as the calculation of mesomorphy. Aiming to contribute to the standardization of this evaluation, this study investigated whether contralateral opposition influences both the arm circumference in flexion and tension as well as the activation of the biceps brachii in physically active young individuals.
2. Materials and Methods
2.1. Participants
Participants were recruited by convenience sampling, as in previous studies [
8,
9]. Individuals aged between eighteen and thirty-five years with no history of musculoskeletal injuries in the upper limbs in the six months prior to data collection were included in this study. Fifty individuals with a mean (± SD) age of 22.7 ± 2.9 years (men: 23.4 ± 3.6; women: 22.3 ± 2.4), body mass of 71.2 ± 13.8 kg (men: 79.5 ± 12.1; women: 63.4 ± 10.4), and height of 169.1 ± 9.5 cm (men: 176.9 ± 5.8; women: 161.8 ± 5.7) were evaluated and classified as physically active, as verified through the short version of the IPAQ (International Physical Activity Questionnaire) [
10]. For the characterization of the sample, the anthropometric techniques of the International Society for the Advancement of Kinanthropometry (ISAK) [
7] were used, performed by a Level 2 certified anthropometrist. All procedures were carried out at the School of Physical Education and Sports of the Federal Rural University of Rio de Janeiro (EEFD/UFRRJ). This study was approved by the Ethics Committee of the University, and all participants agreed to participate and signed the informed consent form.
Body mass was measured using a digital scale (Omron
® HBF-514, Kyoto, Japan) with a precision of 0.1 kg. To measure height, a portable stadiometer (Cescorf
®, Porto Alegre, RS, Brazil) was used, ensuring that the Frankfürt plane was properly positioned. Body mass Index was calculated as body mass (kg) divided by height squared (m
2). Four skinfolds (triceps, subscapular, supraspinale, and calf), two circumferences (flexed and tensed arm and calf), and two bone diameters (humerus and femur) were measured, all on the right side. For skinfold, circumference, and bone diameter measurements, the following instruments were used: a scientific digital skinfold caliper (Avanutri
®, Três Rios, RJ, Brazil), an anthropometric metal tape measure (Cescorf
®, Porto Alegre, RS, Brazil), and a bone caliper (Cescorf
®, Porto Alegre, RS, Brazil). Two measurements were taken for each variable. When the difference between them exceeded 5% for skinfolds or 1% for the other measurements, a third measurement was performed. The technical error of measurement (TEM) was then calculated. The somatotype was determined based on the Heath and Carter [
6] model.
2.2. Testing Procedures
2.2.1. Circumference
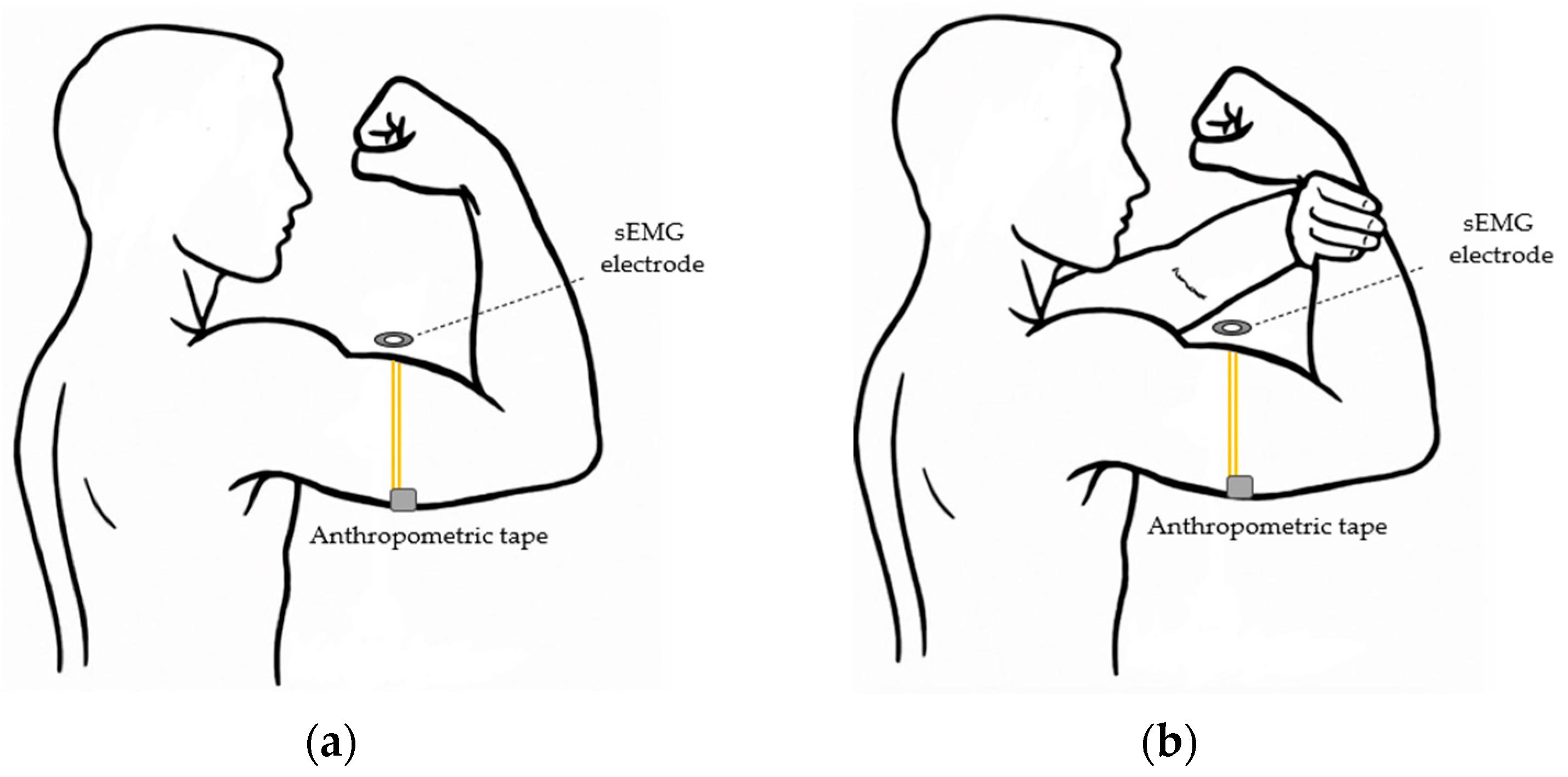
The anthropometric measurement of circumference was performed using two different methods (
Figure 1):
(1st) With the right shoulder flexed at 90°, elbow at 90°, and forearm in supination, performing a maximum contraction of the biceps brachii (FTA).
(2nd) With the right shoulder flexed at 90°, elbow at 90°, and forearm in supination, with the left hand opposing the right, performing a maximum contraction of the biceps brachii (FTA + OP).
In both methods, measurements were taken on the right arm, at the point of greatest circumference of the arm segment, with the tape measure positioned perpendicularly to the axis of the arm. For each protocol, the measurements were taken in duplicate. If the difference between the first two measurements exceeded 1%, a third measurement was taken. The experimental conditions were randomized by computer, and a rest interval of approximately 3 min was provided between measurements.
2.2.2. Surface Electromyography (sEMG)
Electromyographic activity of the biceps brachii was assessed under the two conditions previously mentioned for the measurement of flexed and tensed arm girth. A New Miotool USB/wireless (Miotec
®, Porto Alegre, RS, Brazil) was used for data acquisition, with 8 available channels and a sampling rate of 2000 samples per second per channel. The values used were 20 Hz for the high-pass filter and 500 Hz for the low-pass filter, while the responses obtained were automatically provided in root mean square (RMS) by the MiotecSuite 1.0 software [
11]. The contraction lasted three seconds, with electromyographic activity analyzed second-by-second. Additionally, the average value across the three seconds was calculated for further interpretation. The electromyographic activity of the biceps brachii muscle was assessed approximately 10 min after the anthropometric assessment, under the two previously mentioned conditions for measuring the flexed and tensed arm circumference.
The electrode placement site was determined following the guidelines by Barbero, Merletti, and Rainoldi [
12], which provide specific references to standardize electrode positioning regardless of the individual’s segment length. Surface adhesive electrodes (2223 BR, 3M
®, Campinas, Brazil) with a conductive gel and an AgCl detection surface of 1 cm in diameter, in the form of discs with a center-to-center distance of 2 cm, were positioned on the muscle belly at the point of greatest circumference of the right arm, with the shoulder and elbow flexed at 90°. To ensure the quality of the electromyographic signals, the skin surface was cleaned with 70% alcohol prior to electrode placement.
After preparation, a maximum voluntary contraction (MVC) was performed, both with and without contralateral opposition, following the same rest interval used during the anthropometric assessment. The order of conditions was randomly determined using a computerized randomization process, and the values were expressed in microvolts (µV). Root mean square (RMS) values were automatically provided by the MiotecSuite 1.0 software at the end of each test.
2.3. Statistical Analysis
To assess data distribution, the Shapiro–Wilk and Kolmogorov–Smirnov tests were applied. The statistical methods were based on data normality; for normally distributed data, a two-way repeated measures ANOVA (Type III) was performed, while for non-normal distributions, the Friedman test was applied. Post hoc multiple comparisons were conducted when necessary, and interactions were analyzed based on sex. The results obtained from the ANOVA included partial eta squared (η2p) as a measure of standardized effect size. The interpretation followed the conventional thresholds: small effect size (0.01 ≤ η2p < 0.06), medium effect size (0.06 ≤ η2p < 0.14), and large effect size (η2p ≥ 0.14).
The correlation analysis followed the same principle: the Pearson test was employed for data with a normal distribution, and the Spearman test for data with a non-normal distribution. Additionally, the intraclass correlation coefficient (3,1) (ICC) was calculated to assess the reliability of the measurements.
Descriptive results are presented as mean ± standard deviation. Statistical analysis was conducted using SPSS software, version 20 (IBM, Armonk, NY, USA) and GraphPad Prism, version 8.0 (San Diego, CA, USA). Statistically significant differences were considered when the p-value was less than 0.05.
3. Results
Table 1 presents the technical measurement errors and correlation coefficients. The measurements demonstrated good precision, with technical errors below 1% for circumferences and diameters and under 2% for skinfolds.
Table 2 presents the main anthropometric characteristics of the research volunteers, as well as the values of somatotype components.
Table 3 presents the comparison between measurement methods for the flexed and tensed arm, with and without contralateral opposition. No significant interaction between sex and condition was observed for any of the analyzed variables (circumference:
p = 0.101; mesomorphy:
p = 0.570; sEMG 1s:
p = 0.371; sEMG 2s:
p = 0.227; sEMG 3s:
p = 0.055; sEMG mean:
p = 0.089), indicating consistent results across sexes.
Due to the absence of significant interaction with sex, data were analyzed without stratification by sex. Arm circumference was significantly higher in the condition with opposition (p < 0.001), with an increase of over 1%. This difference significantly influenced the somatotype calculation (p < 0.001), increasing the mesomorphy component by approximately 0.1. sEMG values were also significantly higher in the condition with contralateral opposition across all time intervals, including the mean (p < 0.001). These results demonstrate a consistently higher in biceps brachii muscle activation, ranging from 24.57% to 47.46%, with a mean increase of 39.02%.
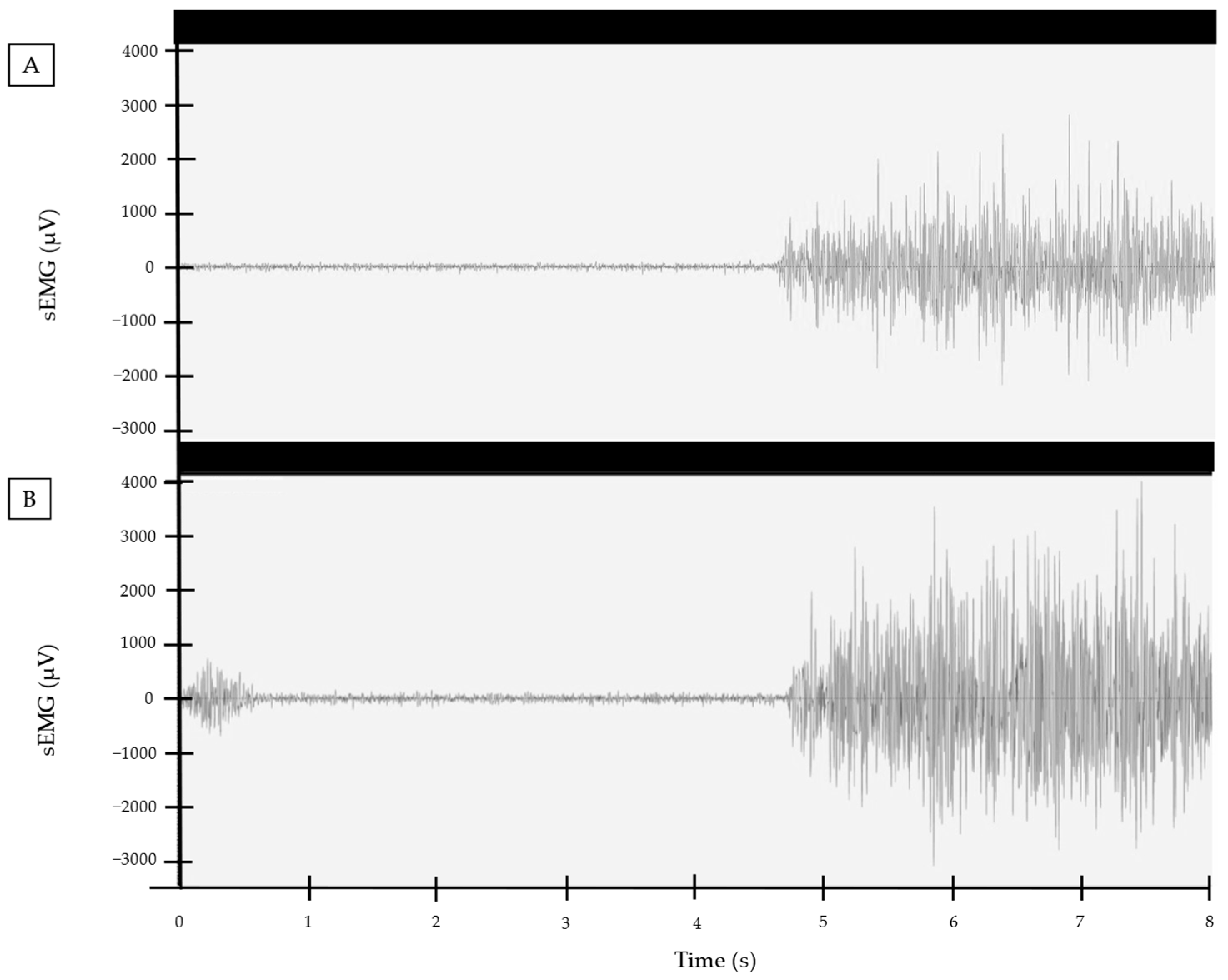
Figure 2 illustrates an example of the difference between the two conditions in a volunteer’s electromyographic signal. The observed variation is close to the average difference found among the volunteers.
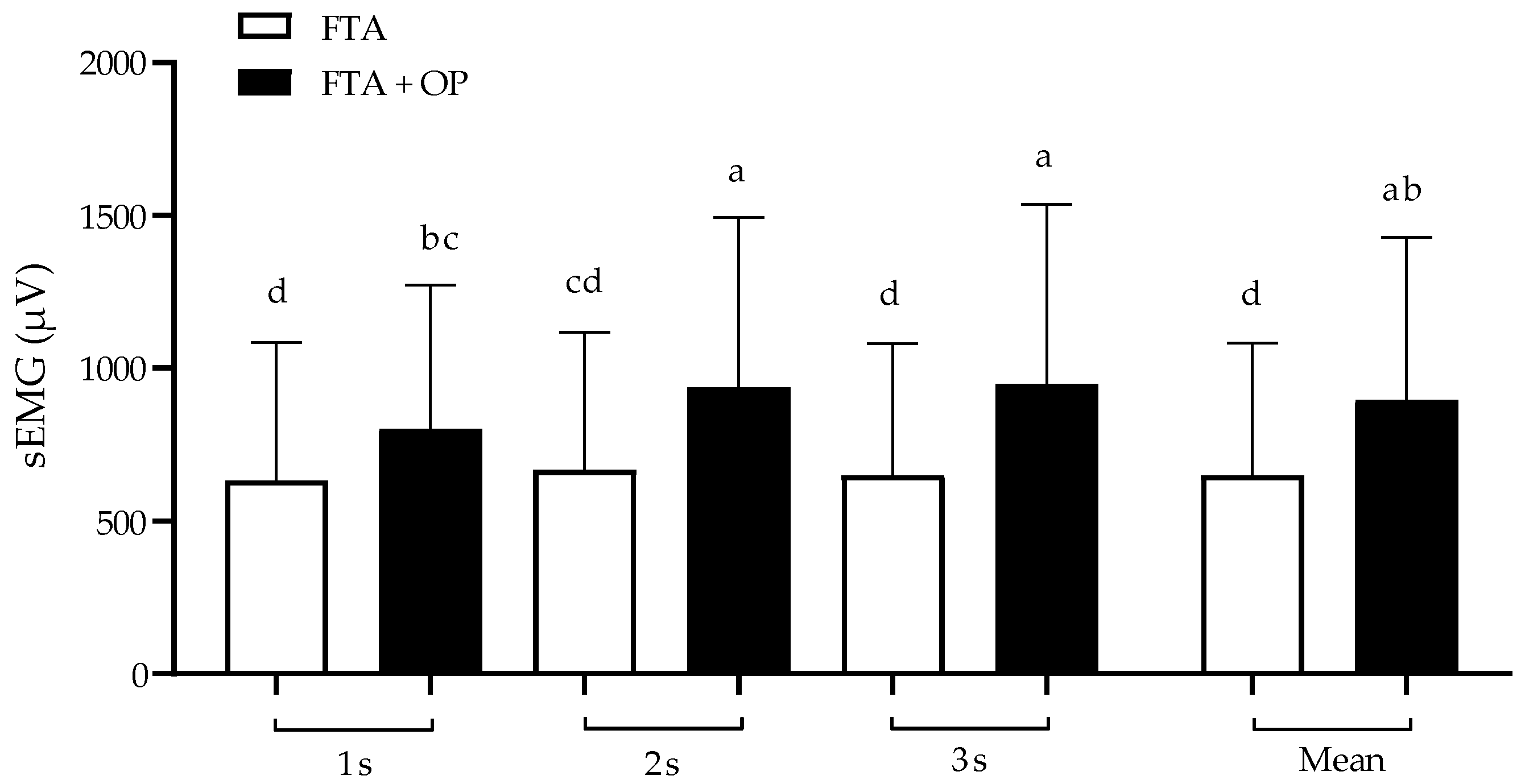
Figure 3 presents the comparison of electromyography values over the three seconds of contraction, along with the mean value. No significant differences were observed between time points in the FTA condition (
p > 0.999). However, in FTA + OP, the first second showed significant differences compared to the second (
p = 0.009) and third seconds (
p = 0.012). Additionally, significant differences between FTA and FTA + OP were observed at all contraction time intervals (
p < 0.02).
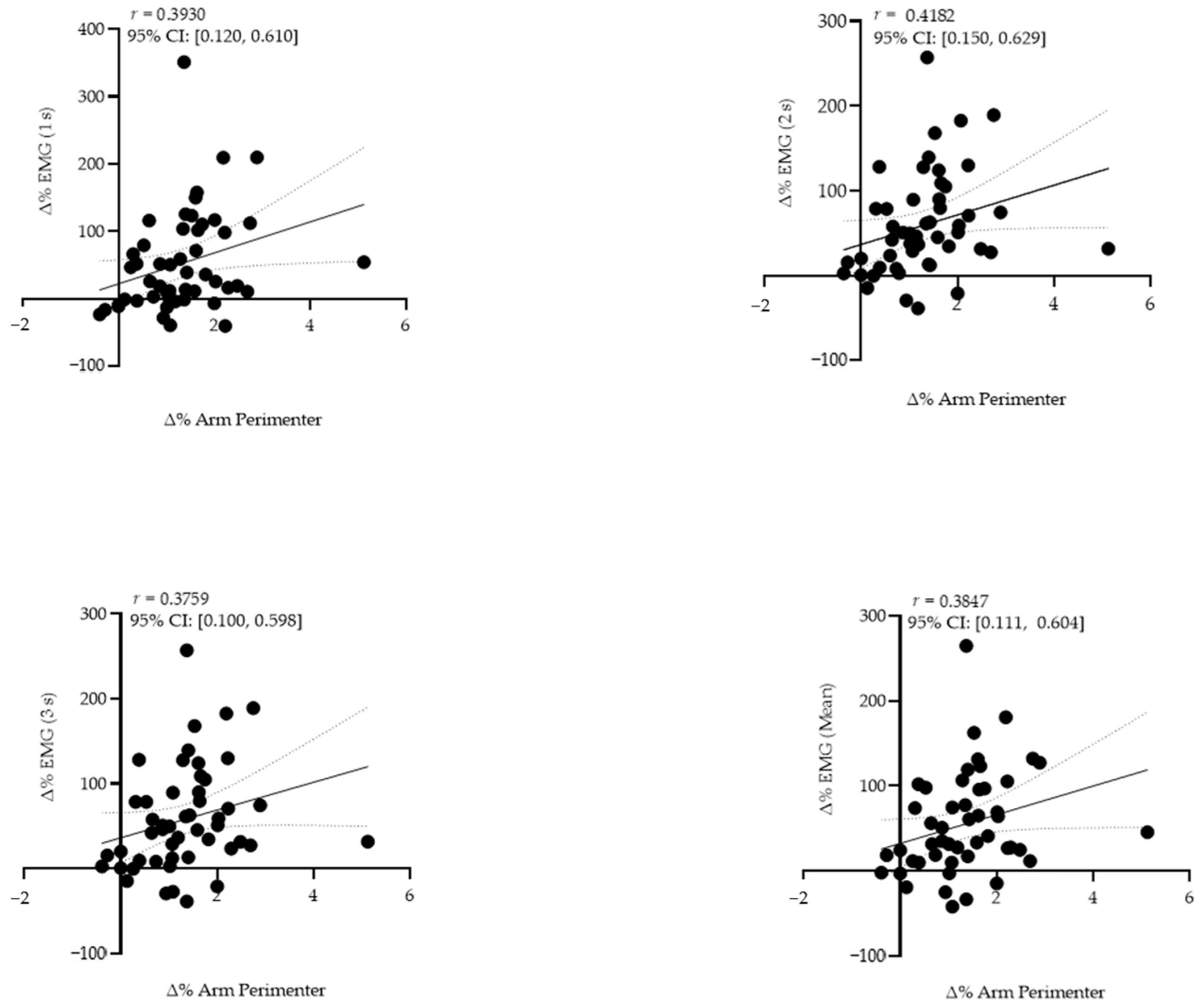
A moderate correlation was observed between the percentage difference in sEMG and circumference only in the middle second of contraction (r = 0.418). In contrast, the correlations were classified as weak in the first (r = 0.393), third (r = 0.376), and average contraction (r = 0.385) (
Figure 4).
4. Discussion
The present study aimed to investigate the influence of opposition on the measurement of flexed and tensed arm circumference, as well as on biceps brachii activation in physically active young adults. The results indicated contralateral opposition led to a significant increase in these variables and influenced the quantification of mesomorphy.
Among the circumference measurements, flexed and tensed arm circumference is the only variable in which the subject is instructed to perform an isometric contraction with maximum effort. According to ISAK guidelines, the difference between the first and second measurements should not exceed 5% for skinfolds and 1% for other measurements, including flexed and tensed arm circumference [
7]. In this context, we observed that counter-resistance increases flexed and tensed arm circumference measurement by more than 1% on average young, physically active individuals. This change in circumference has been shown to directly influence the mesomorphy component of the somatotype, as the calculation of this component uses the corrected flexed and tensed arm circumference [
13].
Conducting measurements with and without counter-resistance at different times may lead to misinterpretations of the somatotype and make it more susceptible to variations than those resulting from training and diet influences. For example, MMA athletes do not show changes in the mesomorphy component between the preparatory and competitive periods [
14], just as basketball players do not alter this component between pre-season and throughout the training period [
15], even though in both cases the groups showed significant modifications in the endomorphy and ectomorphy components during these periods.
This significant difference between the FTA (flexed and tensed arm) and FTA + OP (flexed and tensed arm with opposition) circumferences can be attributed, possibly at least in part, to greater activation of the biceps brachii muscle when individuals applied counter-resistance. Additionally, a moderate correlation was observed between the percentage difference in sEMG and arm circumference only in the middle second of contraction, while in the first and third seconds, this association was weak. A possible explanation for this finding is that the increase in arm circumference under counter-resistance may not be exclusively related to biceps brachii activation but also to the coactivation of antagonist muscles of the elbow flexors [
16], such as the triceps brachii, especially in the last second of contraction.
A major limitation of the present study was the lack of assessment of the coactivation of antagonistic muscles, which could provide a deeper understanding of this issue. Nevertheless, to the best of our knowledge, this is the first study to investigate the influence of contralateral opposition on the perimeter of the flexed and tensed arm, as well as on the muscle activation of the biceps brachii, contributing significantly to the advancement of knowledge and standardization in the field of kinanthropometry. In addition, there is a need for further investigations into the influence of anthropometric assessment protocols on more heterogeneous populations, considering different physical activity levels and age groups. Moreover, this study exclusively evaluated the ISAK protocol’s possibilities for the assessed circumference. However, it remains unclear whether shoulder position and elbow angle can impact these measurements. For example, Norton and Olds [
2] described a technique with the shoulder in abduction and the elbow flexed at 45°, which may influence results, as joint position variation can also affect muscle activation. For instance, studies have shown the innervation areas of the biceps brachii vary depending on the elbow angle [
17,
18].
From a practical standpoint, it is essential the evaluator records whether contralateral opposition was used during the measurement of flexed and tensed arm circumference, as this variable can be significantly influenced by this strategy, potentially leading to an overestimation or underestimation of changes over time. In a research context, we recommend the use or absence of opposition be clearly described in the methods section and applied consistently across all participants to ensure the comparability of results with future studies. It is important to emphasize that the current findings are based on a sample of young, healthy, and physically active individuals. Therefore, the differences observed may be underestimated in older populations, sedentary individuals, or those undergoing upper limb injury rehabilitation, where neuromuscular factors may have an even more pronounced impact on maximal voluntary contraction [
19,
20].
In view of this, we suggest adopting contralateral opposition whenever possible, as this strategy facilitates the maximal voluntary contraction of the biceps brachii. Additionally, hypothetically, contralateral opposition may attenuate the influence of transient neuromuscular factors, such as recent detraining, making the measurement more sensitive to morphological changes resulting from chronic training adaptations.
5. Conclusions
In an anthropometric assessment, the use of contralateral resistance during the measurement of flexed and tensed arm circumference resulted in a significant increase in both biceps brachii muscle activation and arm circumference. In addition, the application of counter-resistance led to a significant rise in the calculated mesomorphy component of the somatotype. Thus, if the goal is to obtain the highest possible value for flexed arm circumference, the use of contralateral resistance appears to be the most appropriate approach, particularly in physically active young adults. Nevertheless, these findings highlight the importance of standardizing measurement conditions, especially in longitudinal assessments where repeated comparisons are intended. In scientific research, it is essential to explicitly state whether opposition was employed or not, as its use can influence the results and compromise comparability between different studies.


 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}