
Mental Health Screening for Korean Ukrainian Refugee Minors in the Republic of Korea: A Cross Sectional Pilot Study

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
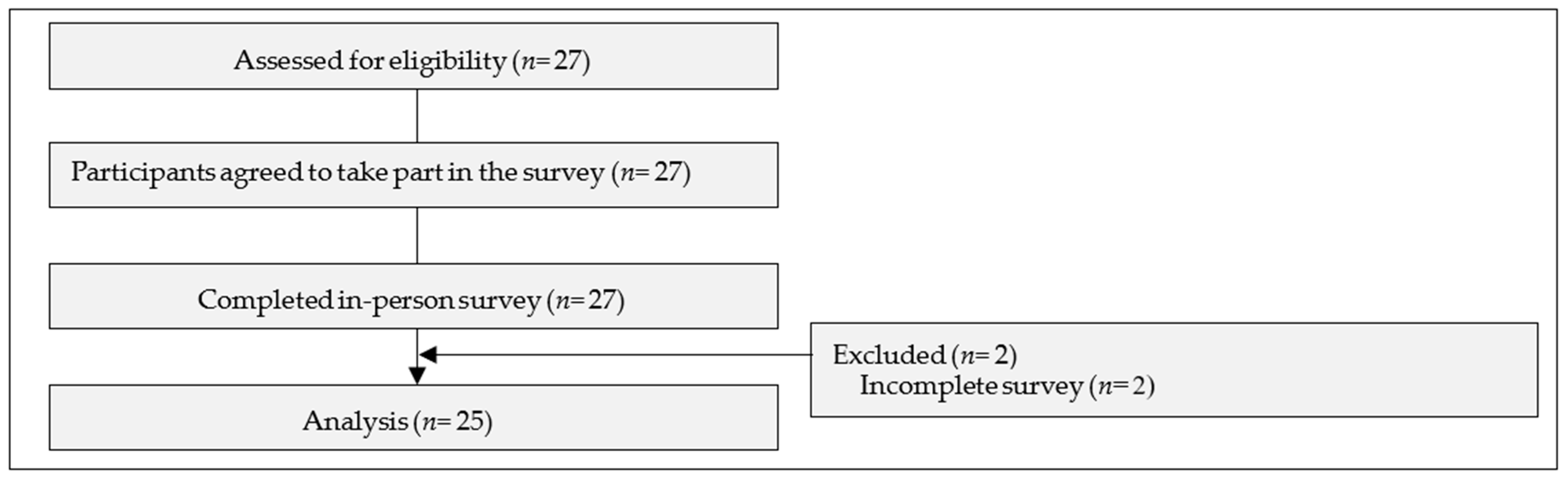
2.2. Sample Size
2.3. Setting
2.4. Particpants
2.5. Assessments
2.5.1. Child and Adolescent Trauma Screen 7–17 Year Self-Check (CATS)
2.5.2. General Anxiety Disorder-7 (GAD-7)
2.5.3. Subjective Unit of Distress Scale (SUDs)
2.6. Procedure
2.7. Statistical Analyses
2.8. Ethical Considerations
3. Results
3.1. Demographic Characteristics of Particpants
3.2. The Screening Results
3.3. The Result of CATS between Two Population Groups
3.4. The Result of GAD-7 and SUDs between Two Population Groups
4. Discussion
4.1. The Effect of Family Relationships
4.2. Stable Visa Status
4.3. Economic Development of the Host Country
4.4. Differences between Child and Teenage Refugees
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNHCR. Ukraine Refugee Situation. Available online: http://data.unhcr.org/en/situations/ukraine (accessed on 22 December 2022).
- Korea Times. Available online: https://www.koreatimes.co.kr/www/opinion/2022/12/197_333271.html?utm_source=CU (accessed on 22 December 2022).
- UNHCR. Republic of Korea. Available online: http://help.unhcr.org/southkorea (accessed on 22 December 2022).
- Bradby, H.; Humphris, R.; Newall, D.; Phillimore, J. Public Health Aspects of Migrant Health: A Review of the Evidence on Health Status for Refugees and Asylum Seekers in the European Region; WHO Regional Office for Europe: Copenhagen, Denmark, 2015; Volume 44. [Google Scholar]
- Mesa-Vieira, C.; Haas, A.D.; Buitrago-Garcia, D.; Roa-Diaz, Z.M.; Minder, B.; Gamba, M.; Salvador, D.; Gomez, D., Jr.; Lewis, M.; Gonzalez-Jaramillo, W.C.; et al. Mental Health of Migrants with Pre-migration Exposure to Armed Conflict: A Systematic Review and Meta-analysis. Lancet Public Health 2022, 7, 469–481. [Google Scholar] [CrossRef]
- Javanbakht, A. Addressing War Trauma in Ukrainian Refugees Before It Is Too Late. Eur. J. Psychotraumatol. 2022, 13, 2104009. [Google Scholar] [CrossRef]
- Rousseau, C. Addressing Mental Health Needs of Refugees. Can. J. Psychiatry 2018, 63, 287–289. [Google Scholar] [CrossRef] [PubMed]
- Dowling, A.; Enticott, J.; Kunin, M. An Investigation into The Association of Pre- and Post-Migration Experiences on The Self-rated Health Status among New Resettled Adult Humanitarian Refugees to Australia: A Protocol for a Mixed Methods Study. BMC Int. Health Hum. Rights 2019, 19, 15. [Google Scholar] [CrossRef] [PubMed]
- Blackmore, R.; Boyle, J.A.; Fazel, M.; Ranasinha, S.; Gray, K.M.; Fitzgerald, G.; Misso, M.; Gibson-Helm, M. The Prevalence of Mental Illness in Refugees and Asylum Seekers: A Systematic Review and Meta-Analysis. PLoS Med. 2020, 17, e1003337. [Google Scholar] [CrossRef] [PubMed]
- De Vito, E.; de Waure, C.; Specchia, M.L.; Ricciardi, W. Public Health Aspects of Migrant Health: A Review of the Evidence on Health Status for Undocumented Migrants in the European Region; WHO Regional Office for Europe: Copenhagen, Denmark, 2015; Volume 44. [Google Scholar]
- Newnham, E.A.; Pearman, A.; Olinga-Shannon, S.; Nickerson, A. The Mental Health Effects of Visa Insecurity for Refugees and People Seeking Asylum: A Latent Class Analysis. Int. J. Public Health 2019, 64, 763–772. [Google Scholar] [CrossRef]
- Nickerson, A.; Byrow, Y.; O’Donnell, M. The Association between Visa Insecurity and Mental Health, Disability and Social Engagement in Refugees Living in Australia. Eur. J. Psychotraumatol. 2019, 10, 1688129. [Google Scholar] [CrossRef]
- Slobodin, O.; Ghane, S.; De Jong, J.T. Developing Culturally Sensitive Mental Health Intervention for Asylum Seekers in the Netherlands: A Pilot Study. Intervention 2018, 16, 86–94. [Google Scholar] [CrossRef]
- Feyissa, I.F.; Noh, Y.; Yoon, M.S. Post-Migration Life Adversity and Mental Health of Refugees and Asylum Seekers: The Mediating Role of Resilience between Perceived Discrimination, Socio-Economic Strains, Structural Strains, and Mental Health. Behav. Sci. 2022, 12, 208. [Google Scholar] [CrossRef] [PubMed]
- Garcini, L.M.; Daly, R.; Chen, N.; Mehl, J.; Pham, T.; Phan, T.; Hansen, B.; Kothare, A. Undocumented Immigrants and Mental Health: A Systematic Review of Recent Methodology and Findings in the United States. J. Migr. Health 2022, 4, 100058. [Google Scholar] [CrossRef]
- Matthis, S.; Naser, M.; Panagiota, M.; Ulrich, S.; Richard, A.B.; Nickerson, A. Changes in Post-Migration Living Difficulties Predict Treatment Outcome in Traumatized Refugees. Front. Psychiatry 2018, 9, 476. [Google Scholar] [CrossRef]
- Bustamante, L.H.U.; Cerqueira, R.O.; Leclerc, E.; Brietzke, E. Stress, Trauma, and Posttraumatic Stress Disorder in Migrants: A Comprehensive Review. Rev. Bras. De Psiquiatr. 2018, 40, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Liddell, B.J.; O’Donnell, M.; Bryant, R.A.; Murphy, S.; Byrow, Y.; Mau, V.; McMahon, T.; Benson, G.; Nickerson, A. The Association between COVID-19 Related Stressors and Mental Health in Refugees Living in Australia. Eur. J. Psychotraumatol. 2021, 12, 1947564. [Google Scholar] [CrossRef] [PubMed]
- Mangrio, E.; Sjöström, K.; Grahn, M.; Zdravkovic, S. Risk for Mental Illness and Family Composition After Migration to Sweden. PLoS ONE 2021, 16, e0251254. [Google Scholar] [CrossRef] [PubMed]
- Rostami, R.; Wells, R.; Solaimani, J.; Berle, D.; Hadzi-Pavlovic, D.; Silove, D.; Nickerson, A.; O’Donnell, M.; Bryant, R.; McFarlane, A.; et al. The Mental Health of Farsi-Dari Speaking Asylum-Sseeking Children and Parents Facing Insecure Residency in Australia. Lancet Reg. Health-West. Pac. 2022, 27, 100548. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.M.; Brand, T.; Zeeb, H. Pre-Migration Socioeconomic Status and Post-Migration Health Satisfaction Among Syrian Refugees in Germany: A Cross-Sectional Analysis. PLoS Med. 2020, 17, e1003093. [Google Scholar] [CrossRef] [PubMed]
- Isaksen, J.V. The Impact of the Financial Crisis on European Attitudes Toward Immigration. Comp. Migr. Stud. 2019, 7, 24. [Google Scholar] [CrossRef]
- United Nations. Available online: http://unctadstat.unctad.org (accessed on 23 December 2022).
- Fajth, V.; Bilgili, Ö.; Loschmann, C. How Do Refugees Affect Social Life in Host Communities? The Case of Congolese Refugees in Rwanda. Comp. Migr. Stud. 2019, 7, 33. [Google Scholar] [CrossRef]
- Depetris-Chauvin, E.; Santoss, R. Unexpected Guests: The Impact of Internal Displacement Inflows on Rental Prices in Colombian Host Communities. J. Dev. Econ. 2018, 134, 289–309. [Google Scholar] [CrossRef]
- Straiton, M.L.; Reneflot, A.; Diaz, E. Mental Health of Refugees and Non-refugees from War-Conflict Countries: Data from Primary Healthcare Services and the Norwegian Prescription Database. J. Immigr. Minor. Health 2017, 19, 582–589. [Google Scholar] [CrossRef]
- Mels, C.; Derluyn, I.; Broekert, E. Screening for Traumatic Exposure and Post-Traumatic Stress Symptoms in Adolescents in War-Affected Eastern Democratic Republic of Congo. Arch. Pediatr. Adolesc. Med. 2009, 63, 525–530. [Google Scholar] [CrossRef] [PubMed]
- Ssenyonga, J.; Owens, V.; Kani, O.D. Traumatic Experiences and PTSD Among Adolescent Congolese Refugees in Uganda: A Preliminary Study. J. Psychol. Afr. 2012, 22, 629–632. [Google Scholar] [CrossRef]
- Lindgren, J.; Ekblad, S.; Asplund, M.; Irestig, R.; Burström, B. Mental Ill Health Among Asylum Seekers and Other Immigrants in Sweden. Int. J. Migr. 2012, 8, 167–179. [Google Scholar] [CrossRef]
- Spaas, C.; An, V.; Ines, D.; Sanni, A.; Arnfinn, A.; Natalie, D.; Per, H.; Reeta, K.; Nina, P.; Marianne, O.; et al. Mental health of refugees and non-refugee migrant young people in European secondary education: The role of family separation, daily material stress, and perceived discrimination in resettlement. J. Youth Adolesc. 2022, 51, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Song, J.J.; Bell, M. North Korean Secondary Asylum in the UK. Migr. Stud. 2019, 7, 160–179. [Google Scholar] [CrossRef]
- Frounfelker, L.R.; Miconi, D.; Farra, J.; Brooks, M.A.; Rousseau, C.; Betancourt, S.T. Mental Health of Refugee Children and Youth: Epidemiology, Interventions, and Future Directions. Annu. Rev. Public Health 2020, 41, 159–176. [Google Scholar] [CrossRef]
- Labott, S.M.; Johnson, T.P.; Fendrich, M.; Feeny, N.C. Emotional Risks to Respondents in Survey Research. J. Empir. Res. Hum. Res. Ethics 2013, 8, 53–66. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Uro. Today Int. J. 2007, 335, 806–808. [Google Scholar] [CrossRef]
- World Health Organization. Available online: http://apps.who.int (accessed on 23 December 2022).
- Sachser, C.; Berliner, L.; Holt, T.; Jensen, T.K.; Jungbluth, N.; Risch, E.; Goldbeck, L. International Development and Psychometric Properties of the Child and Adolescent Trauma Screen (CATS). J. Affect. Disord. 2017, 210, 189–195. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Ulmer Onlineklinik. CATS Questionnaire. Available online: http://ulmer-onlineklinik.de/course/view.php?id=1701 (accessed on 22 December 2022).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV; American Psychiatric Publishing: Washington, DC, USA, 1994. [Google Scholar]
- Zinchuk, M.; Kustov, G.; Pashnin, E.; Gersamia, A.; Rider, F.; Yakovlev, A.; Voinova, N.; Popova, S.; Avedisova, A.; Guekht, A. Validation of the Generalized Anxiety Disorder-7 (GAD-7) in Russian People with Epilepsy. Epilepsy Behav. 2021, 123, 108269. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, C.L.; O’Neil, K.A.; Crawley, S.A. Patterns and Predictors of Subjective Units of Distress in Anxious Youth. Behav. Cogn. Psychother. 2010, 38, 497–504. [Google Scholar] [CrossRef]
- The Path of Greatest Advantage. SUDS Scale. Available online: www.disordersofmood.com/pdf/SUDS.pdf (accessed on 22 December 2022).
- Hvidtfeldt, C.; Petersen, J.H.; Norredam, M. Waiting for Family Reunification and the Risk of Mental Disorders Among Refugee Fathers: A 24-Year Longitudinal Cohort Study from Denmark. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 57, 1061–1072. [Google Scholar] [CrossRef] [PubMed]
- Braun-Lewensohn, O.; Khaled, A. Syrian Adolescent Refugees: How Do They Cope During Their Stay in Refugee Camps? Front. Psychol. 2018, 9, 1258. [Google Scholar] [CrossRef] [PubMed]
- Braun-Lewensohn, O. Coping and Social Support in Children Exposed to Mass Trauma. Curr. Psychiatry Rep. 2015, 17, 46–56. [Google Scholar] [CrossRef] [PubMed]
- Weine, S.; Muzurovic, N.; Kulauzovic, Y.; Besic, S.; Lezic, A.; Mujagic, A.; Muzurovic, J.; Spahovic, D.; Feetham, S.; Ware, N.; et al. Family Consequences of Refugee Trauma. Fam. Process 2004, 43, 147–160. [Google Scholar] [CrossRef] [PubMed]
- Bernd, H.; Michael, K.; Werner, F.; Jörn, P.; Eric, H.; Tam, T.; Burkhard, B.; Bernd, G.; Christoph, M.; Markus, S. Different Patterns of Mental Health Problems in Unaccompanied Refugee Minors(URM): A Sequential Mixed Method Study. Front. Psychiatry 2020, 11, 324. [Google Scholar]
- Pollard, T.; Howard, N. Mental Healthcare for Asylum-Seekers and Refugees Residing in the United Kingdom: A Scoping Review of Policies, Barriers, and Enablers. Int. J. Ment. Health Syst. 2021, 15, 60. [Google Scholar] [CrossRef]
- Doma, H.; Tran, T.; Rioseco, P. Understanding the Relationship Between Social Support and Mental Health of Humanitarian Migrants Resettled in Australia. BMC Public Health 2022, 22, 1739. [Google Scholar] [CrossRef]
- United Nations. Available online: www.un.org/development/desa/dpad/wp-content/uploads/sites/45/WESP2022_ANNEX.pdf (accessed on 22 December 2022).
- United Nations. Available online: https://www.un.org/development/desa/publications/wesp-2020 (accessed on 22 December 2022).
- The Organization for Economic Cooperarion and Development. Available online: http://data.oecd.org (accessed on 22 December 2022).
- Kouni, M. Impact of Refugee Population on Development: A Comparative Analysis for the Case of Host Economies. Rev. Econ. Perspect. 2018, 18, 77–96. [Google Scholar] [CrossRef]
- Gomez, M.P.; Christensen, A.; Araya, Y.Y.; Harild, N. The Impacts of Refugees on Neighboring Countries: A Development Challenge; World Development Report Background Papers; World Bank: Washington, DC, USA, 2010. [Google Scholar]
- IDEA. Available online: http://www.idea.int/publications/catalogue/political-participation-refugees-bridging-gaps (accessed on 22 December 2022).
- Braun-Lewensohn, O.; Celestin-Westreich, S.; Celestin, L.P.; Verte, D.; Ponjaert-Kristoffersen, I. Adolescents’ Mental Health Outcomes as a Function of Different Types of Exposure to Ongoing Terror Attacks. J. Youth Adolesc. 2009, 38, 850–862. [Google Scholar] [CrossRef] [PubMed]
- Geltman, P.L.; Grant-Knight, W.; Mehta, S.D.; Lloyd-Travaglini, C.; Lustig, S.; Landgraf, J.M.; Wise, P.H. The “Lost boys of Sudan”. Functional and Behavioral Health of Unaccompanied Refugee Minors Resettled in the United States. Arch. Pediatr. Adolesc. Med. 2005, 159, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, E. Trauma and Resilience in Young Refugees: A 9 year Follow-Up Study. Dev. Psychopathol. 2010, 22, 477–489. [Google Scholar] [CrossRef] [PubMed]
- Fazel, M.; Reed, R.V.; Panter-Brick, C.; Stein, A. Mental Health of Displaced and Refugee Children Resettled in High-Income Countries: Risk and Protective Factors. Lancet 2012, 379, 266–282. [Google Scholar] [CrossRef]
- Reviriego-Reinaldo, N. Junior And Teen Refugee Mental Health: Sex Differences. In Observatory for Research and Innovation in Social Sciences, Proceedings of the International Conference of Psychology, Sociology, Education and Social Sciences (OPIICS 2019), Zaragoza, Spain, 26–28 September 2019; Salavera, C., Teruel, P., Antoñanzas, J.L., Eds.; European Publisher: Heraklion, Greece, 2015; Volume 84, pp. 265–275. [Google Scholar] [CrossRef]
- Derluyn, I.; Broekaert, E. Different Perspectives on Emotional and Behavioural Problems in Unaccompanied Refugee Children and Adolescents. Ethn. Health 2007, 12, 141–162. [Google Scholar] [CrossRef]
- Braun-Lewensohn, O.; Sagy, S.; Roth, G. Coping strategies among adolescents: Israeli Jews and Arabs facing missile attacks. Anxiety Stress Coping Int. J. 2010, 23, 35–51. [Google Scholar] [CrossRef]
- Júnior, B.J.P. Social Desirability Bias in Qualitative Health Research. Rev. De Saude Publica 2022, 56, 101. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Sub-Variables | n | % |
|---|---|---|---|
| Age | Children | 13 | 52 |
| Teenagers | 12 | 48 | |
| Gender | Male | 13 | 52 |
| Female | 12 | 48 | |
| Country of origin | Ukraine | 25 | 100 |
| Ethnicity | Korean | 25 | 100 |
| Length of stay since arrival | ≤ 1 month | 9 | 36 |
| Between 2–6 months | 15 | 60 | |
| More than 6 months | 1 | 4 | |
| Level of proficiency in Korean language | Low | 24 | 96 |
| Moderate | 1 | 4 | |
| High | 0 | 0 |
| Variables | Sub-Variables | M(SD) | ||
|---|---|---|---|---|
| Children (n = 13) | Teenage (n = 12) | Adolescences (n = 25) | ||
| CATS (PSS) | Total | 1.78 (1.61) | 3.41 (3.17) | 2.56 (2.57) |
| Re-experiencing | 0.49 (0.43) | 0.80 (0.65) | 0.64 (0.56) | |
| Avoidance | 0.57 (0.67) | 0.95 (1.03) | 0.76 (0.86) | |
| NACM | 0.37 (0.45) | 0.80 (0.79) | 0.58 (0.66) | |
| Hyperarousal | 0.34 (0.50) | 0.84 (0.82) | 0.58 (0.71) | |
| GAD-7 | 3.38 (3.64) | 5.25 (4.37) | 4.28 (4.03) | |
| SUDs | 20.91 (21.19) | 39.17 (23.91) | 30.43 (24.02) | |
| Variables | Sub-Variables | Count (%) |
|---|---|---|
| CATS (PTEs) | Serious natural disaster | 3 (12%) |
| Serious accident or injury | 4 (16%) | |
| Robbed by threat | 2 (8%) | |
| Abuse by family | 3 (12%) | |
| Abuse by someone | 6 (24%) | |
| Seeing someone in your family get abused | 3 (12%) | |
| Seeing someone in your community get abused | 11 (44%) | |
| Someone old touching your body | 1 (4%) | |
| Someone forcing sex | 0 (0%) | |
| Someone close to you dying suddenly or violently | 0 (0%) | |
| Attacked, stabbed, shot at or hurt badly | 0 (0%) | |
| Seeing someone attacked, stabbed, shot at, hurt badly or killed | 2 (8%) | |
| Stressful of medical procedure | 6 (24%) | |
| Being around war | 19 (76%) | |
| Other events | 4 (16%) | |
| CATS (psychosocial functionality) | Getting along with others | 5 (20%) |
| Hobbies/Fun | 6 (24%) | |
| School or work | 5 (20%) | |
| Family relationship | 2 (8%) | |
| General happiness | 8 (32%) |
| Variables | Sub-Variables | M(SD) | t | p | |
|---|---|---|---|---|---|
| Children (n= 13) | Teenagers (n= 12) | ||||
| CATS (PSS) | Total | 1.78 (1.61) | 3.41 (3.17) | −1.59 | 0.130 |
| Re-experiencing | 0.49 (0.43) | 0.80 (0.65) | −1.39 | 0.177 | |
| Avoidance | 0.57 (0.67) | 0.95 (1.03) | −1.10 | 0.281 | |
| NACM | 0.37 (0.45) | 0.80 (0.79) | −1.66 | 0.115 | |
| Hyperarousal | 0.34 (0.50) | 0.84 (0.82) | −1.84 | 0.078 | |
| CATS (PTEs) | Serious natural disaster | 1.77 (0.43) | 0.00 (0.00) | −1.89 | 0.082 |
| Serious accident or injury | 1.69 (0.48) | 0.00 (0.00) | −2.30 * | 0.040 | |
| Robbed by threat | 1.85 (0.37) | 0.00 (0.00) | −1.47 | 0.165 | |
| Abuse by family | 1.83 (0.38) | 1.92 (0.28) | −0.59 | 0.557 | |
| Abuse by someone | 1.77 (0.43) | 1.75 (0.45) | 0.10 | 0.915 | |
| Seeing someone in your family get abused | 1.92 (0.27) | 1.83 (0.38) | 0.66 | 0.511 | |
| Seeing someone in your community get abused | 1.77 (0.43) | 1.33 (0.49) | 2.34 * | 0.028 | |
| Someone old touching your body | 0.00 (0.00) | 1.92 (0.28) | 1.00 | 0.339 | |
| Someone forcing sex | 0.00 (0.00) | 0.00 (0.00) | - | - | |
| Someone close to you dying suddenly or violently | 0.00 (0.00) | 0.00 (0.00) | - | - | |
| Attacked, stabbed, shot at or hurt badly | 0.00 (0.00) | 0.00 (0.00) | - | - | |
| Seeing someone attacked, stabbed, shot at, hurt badly | 0.00 (0.00) | 1.83 (0.38) | 1.48 | 0.166 | |
| Stressful of medical procedure | 1.77 (0.43) | 1.75 (0.45) | 0.10 | 0.915 | |
| Being around war | 1.15 (0.37) | 1.33 (0.49) | −1.01 | 0.320 | |
| Other events | 1.69 (0.48) | 0.00 (0.00) | −2.30 * | 0.040 | |
| CATS (psychosocial functionality) | Getting along with others | 1.69 (0.48) | 1.91 (0.30) | −1.34 | 0.194 |
| Hobbies/Fun | 1.69 (0.48) | 1.82 (0.40) | −0.68 | 0.500 | |
| School or work | 1.69 (0.48) | 1.91 (0.30) | −1.34 | 0.194 | |
| Family relationship | 1.85 (0.37) | 0.00 (0.00) | −1.47 | 0.165 | |
| General happiness | 1.69 (0.48) | 1.64 (0.50) | 0.27 | 0.784 | |
| Variables | M(SD) | t | p | |
|---|---|---|---|---|
| Children (n= 13) | Teenagers (n= 12) | |||
| GAD-7 | 3.38 (3.64) | 5.25 (4.37) | −1.16 | 0.257 |
| SUDs | 20.91 (21.19) | 39.17 (23.91) | −1.93 | 0.067 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.; Lee, J.S.; Kim, H.-J.; Lee, H.; Lee, M.; Kim, S.-Y.; Choi, H. Mental Health Screening for Korean Ukrainian Refugee Minors in the Republic of Korea: A Cross Sectional Pilot Study. Adolescents 2023, 3, 141-152. https://doi.org/10.3390/adolescents3010011
Park S, Lee JS, Kim H-J, Lee H, Lee M, Kim S-Y, Choi H. Mental Health Screening for Korean Ukrainian Refugee Minors in the Republic of Korea: A Cross Sectional Pilot Study. Adolescents. 2023; 3(1):141-152. https://doi.org/10.3390/adolescents3010011
Chicago/Turabian StylePark, Sejeong, Jenny Seongryung Lee, Hye-Jung Kim, Hojung Lee, Myungjoo Lee, Soo-Yeon Kim, and Han Choi. 2023. "Mental Health Screening for Korean Ukrainian Refugee Minors in the Republic of Korea: A Cross Sectional Pilot Study" Adolescents 3, no. 1: 141-152. https://doi.org/10.3390/adolescents3010011
APA StylePark, S., Lee, J. S., Kim, H.-J., Lee, H., Lee, M., Kim, S.-Y., & Choi, H. (2023). Mental Health Screening for Korean Ukrainian Refugee Minors in the Republic of Korea: A Cross Sectional Pilot Study. Adolescents, 3(1), 141-152. https://doi.org/10.3390/adolescents3010011