Knowledge, Perspectives, and Priorities Regarding Self-Care Activities: A Population-Based Qualitative Study among Iranian Adolescents

 , ,
, , 
Abstract
1. Introduction
- What Iranian adolescents know about self-care and self-care activities and where they mostly get the information?
- Considering their gender, what Iranian adolescents DO as self-care?
- Considering their gender, what are the adolescents first choices of self-care activities (or what they called as self-care activities) if they have no limitation?
2. Material and Methods
2.1. Study Design
2.2. Population and Sampling Method
2.3. Development of the Study Instrument
2.4. Data Collection
2.5. Data Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Knowledge Regards Self-Care
3.3. Definition
3.4. Suitable Self-Care Activities
3.5. Self-Care Activities Regularly Performed
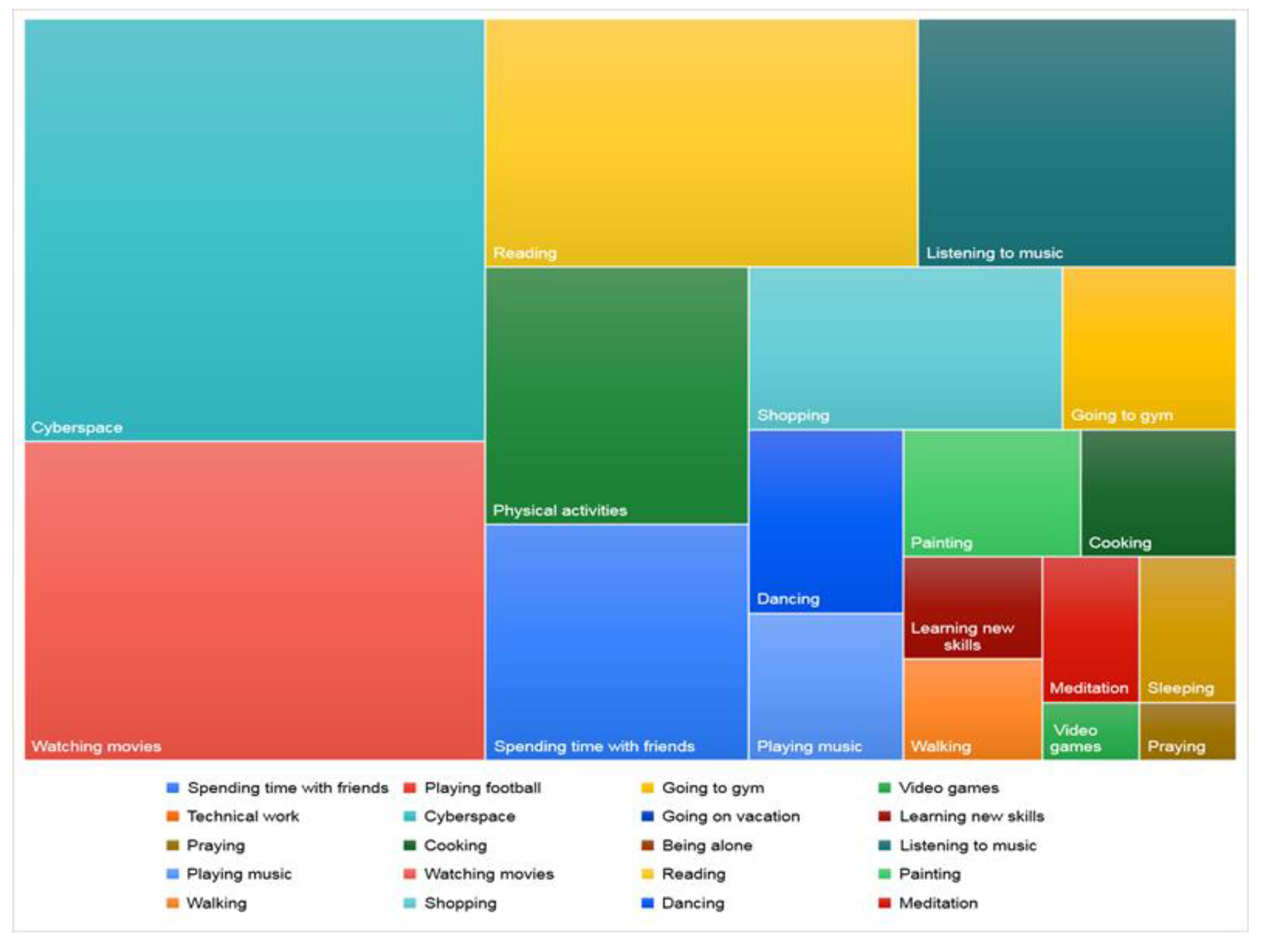
3.6. Desired Free Time Activities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Ethical Approval
Appendix A


References
- WHO Consolidated Guideline on Self-Care Interventions for Health: Sexual and Reproductive Health and Rights; World Health Organization: Geneva, Switzerland, 2019.
- Riegel, B.; Dunbar, S.B.; Fitzsimons, D.; Freedland, K.E.; Lee, C.S.; Middleton, S.; Stromberg, A.; Vellone, E.; Webber, D.E.; Jaarsma, T. Self-care research: Where are we now? Where are we going? Int. J. Nurs. Stud. 2019, 103402. [Google Scholar] [CrossRef] [PubMed]
- Jaarsma, T.; Strömberg, A.; Ben Gal, T.; Cameron, J.; Driscoll, A.; Duengen, H.-D.; Inkrot, S.; Huang, T.-Y.; Huyen, N.N.; Kato, N.; et al. Comparison of self-care behaviors of heart failure patients in 15 countries worldwide. Patient Educ. Couns. 2013, 92, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Uzuncakmak, T.; Beser, N.G. The effects of self-care education of adolescents on the power of self-care. Int. J. Caring Sci. 2017, 10, 1368. [Google Scholar]
- Köberich, S.; Lohrmann, C.; Mittag, O.; Dassen, T. Effects of a hospital-based education programme on self-care behaviour, care dependency and quality of life in patients with heart failure—A randomised controlled trial. J. Clin. Nurs. 2015, 24, 1643–1655. [Google Scholar] [CrossRef]
- Dickson, V.V.; McCarthy, M.M.; Howe, A.; Schipper, J.; Katz, S.M. Sociocultural Influences on Heart Failure Self-care Among an Ethnic Minority Black Population. J. Cardiovasc. Nurs. 2013, 28, 111–118. [Google Scholar] [CrossRef]
- Siabani, S.; Leeder, S.R.; Davidson, P.M. Barriers and facilitators to self-care in chronic heart failure: A meta-synthesis of qualitative studies. SpringerPlus 2013, 2, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Eftekhar, H.; Mirkamali, S.K.; Tavafian, S.S.; Mohammad, K.; Shahnazi, H.; Sharifirad, G. Exploring self care in Tehran, Iran: A population based study. J. Res. Med. Sci. 2012, 17, 1144–1149. [Google Scholar]
- Granger, B.B.; Sandelowski, M.; Tahshjain, H.; Swedberg, K.; Ekman, I. A qualitative descriptive study of the work of adherence to a chronic heart failure regimen: Patient and physician perspectives. J. Cardiovasc. Nurs. 2009, 24, 308–315. [Google Scholar] [CrossRef]
- Mohammadzadeh, M.; Awang, H.; Ismail, S.; Shahar, H.K. Improving emotional health and self-esteem of Malaysian adolescents living in orphanages through Life Skills Education program: A multi-centre randomized control trial. PLoS ONE 2019, 14, e0226333. [Google Scholar] [CrossRef] [PubMed]
- Tajik, E.; Latiff, L.A.; Mohammadzadeh, M. Stress, Depression and Obesity among Adolescents: A Narrative Review. Pyrex J. Nutr. Metab. 2015, 1, 1–6. [Google Scholar]
- Mohammadzadeh, M.; Tajik, E.; Awang, H.; Latiff, L.A. Emotional health and coping mechanisms among adolescents in Malaysian residential foster care homes: A comparative study with adolescents living with families. Asian J. Psychiatry 2018, 32, 156–158. [Google Scholar] [CrossRef]
- Stewart, J.G.; Shields, G.S.; Esposito, E.C.; Cosby, E.A.; Allen, N.B.; Slavich, G.M.; Auerbach, R.P. Life Stress and Suicide in Adolescents. J. Abnorm. Child Psychol. 2019, 47, 1707–1722. [Google Scholar] [CrossRef] [PubMed]
- DuPont-Reyes, M.J.; Villatoro, A.P.; Phelan, J.C.; Painter, K.; Link, B.G. Adolescent views of mental illness stigma: An intersectional lens. Am. J. Orthopsychiatry 2019, 90, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Foo, S.; Majid, S.; Chang, Y.-K.; Dumaual, H.T.J.; Suri, V.R. Self-Care and Health-Information-Seeking Behaviours of Diabetic Patients in Singapore. Health Commun. 2019, 35, 994–1003. [Google Scholar] [CrossRef] [PubMed]
- Mohammadzadeh, M.; Awang, H.; Mirzaei, F. Mental Health Stigma among Middle Eastern Adolescents: A Protocol for a Systematic Review. J. Psychiatr. Ment. Health Nurs. 2020, 27. [Google Scholar] [CrossRef] [PubMed]
- Mohammadzadeh, M.; Awang, H.; Ismail, S.; Shahar, H.K. Influence of coping mechanisms on emotional problems among adolescents in Malaysian orphanages. Asia-Pac. Psychiatry 2017, 9, e12288. [Google Scholar] [CrossRef]
- Zarei, E.; Simbar, M.; Shahhoseini, Z. Explaining the concept of self-care in adolescents. J. Qual. Res. Health Sci. 2016, 4, 395–405. [Google Scholar]
- Teh, C.H.; Teh, M.W.; Lim, K.H.; Kee, C.C.; Sumarni, M.G.; Heng, P.P.; Zahari, T.H.M.; Chan, Y.Y.; Hafiza, I.N.; Tee, E.O.; et al. Clustering of lifestyle risk behaviours and its determinants among school-going adolescents in a middle-income country: A cross-sectional study. BMC Public Health 2019, 19, 1177. [Google Scholar] [CrossRef]
- Al-Sheyab, N.A.; Alomari, M.A.; Hayajneh, A.A.; Shah, S. Attitudes and perceived barriers toward healthy lifestyle behaviors in Jordanian adolescents: A developing country perspective. Adolesc. Health Med. Ther. 2019, 10, 39–47. [Google Scholar] [CrossRef]
- Mohammadzadeh, M.; Awang, H.; Shahar, H.K.; Ismail, S. Life Skills Education for Malaysian Institutionalised Adolescents: Knowledge, Needs and Priorities: A Qualitative Pilot Study. Iran. J. Public Health 2017, 46, 1739–1741. [Google Scholar]
- Gheibizadeh, M.; Bazpour, M.; Malehi, A.S.; Keikhaei, B. Health-Promoting Lifestyle of Adolescents with β-Thalassemia Based on Precede Model in Ahvaz, Iran, 2016. Jundishapur J. Chronic Dis. Care 2016, 6. [Google Scholar] [CrossRef]
- Solhi, M.; Mehri, A.; Garmaroudi, G.; Nadrian, H.; Sighaldeh, S.S. Health promoting lifestyle and its determinants among University students in Sabzevar, Iran. Int. J. Prev. Med. 2016, 7, 65. [Google Scholar] [CrossRef] [PubMed]
- Doshmangir, L.; Moshiri, E.; Mostafavi, H.; Sakha, M.A.; Assan, A. Policy analysis of the Iranian Health Transformation Plan in primary healthcare. BMC Health Serv. Res. 2019, 19, 670. [Google Scholar] [CrossRef]
- Emami, H.; Ghazinour, M.; Rezaeishiraz, H.; Richter, J. Mental Health of Adolescents in Tehran, Iran. J. Adolesc. Health 2007, 41, 571–576. [Google Scholar] [CrossRef]
- Panjalipour, S.; Khalesi, Z.B.; Mirhaghjoo, S.N. Iranian Female Adolescents’ Reproductive Health Needs: A Systematic Review. Int. J. Women’s Health Reprod. Sci. 2017, 6, 226–232. [Google Scholar] [CrossRef]
- Goudarzian, A.H.; Boyle, C.; Beik, S.; Jafari, A.; Nesami, M.B.; Taebi, M.; Zamani, F. Self-Care in Iranian Cancer Patients: The Role of Religious Coping. J. Relig. Health 2019, 58, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Stearns, S.C.; Bernard, S.L.; Fasick, S.B.; Schwartz, R.; Konrad, T.R.; Ory, M.G.; DeFriese, G.H. The economic implications of self-care: The effect of lifestyle, functional adaptations, and medical self-care among a national sample of Medicare beneficiaries. Am. J. Public Health 2000, 90, 1608–1612. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Dashiff, C.J.; McCaleb, A.; Cull, V. Self-Care of Young Adolescents with Type 1 Diabetes. J. Pediatr. Nurs. 2006, 21, 222–232. [Google Scholar] [CrossRef]
- Masoumi, M.; Shahhosseini, Z. Self-care challenges in adolescents: A comprehensive literature review. Int. J. Adolesc. Med. Health 2017, 31. [Google Scholar] [CrossRef]
- Mohammadzadeh, M.; Awang, H.; Tajik, E. Life Skills Needs Assessment among Iranian Immigrant Students in Malaysia. Iran. J. Public Health 2017, 46, 143–145. [Google Scholar]
- Fink, E.; Patalay, P.; Sharpe, H.; Holley, S.; Deighton, J.; Wolpert, M. Mental Health Difficulties in Early Adolescence: A Comparison of Two Cross-Sectional Studies in England From 2009 to 2014. J. Adolesc. Health 2015, 56, 502–507. [Google Scholar] [CrossRef]
- De Silva, M.J.; Breuer, E.; Lee, L.; Asher, L.; Chowdhary, N.; Lund, C.; Patel, V. Theory of change: A theory-driven approach to enhance the Medical Research Council’s framework for complex interventions. Trials 2014, 15, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. Int. J. Nurs. Stud. 2013, 50, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.; Fitzpatrick, R.; Haines, A.; Kinmonth, A.L.; Sandercock, P.; Spiegelhalter, D.; Tyrer, P. Framework for design and evaluation of complex interventions to improve health. BMJ 2000, 321, 694–696. [Google Scholar] [CrossRef]
- Morrow, R.; Rodriguez, A.; King, N. Colaizzi’s descriptive phenomenological method. Psychologist 2015, 28, 643–644. [Google Scholar]
- Daher, M.; Carré, D.; Jaramillo, A.; Olivares, H.; Tomicic, A. Experience and meaning in qualitative research: A conceptual review and a methodological device proposal. FQS 2017, 3. [Google Scholar] [CrossRef]
- Qutoshi, S.B. Phenomenology: A Philosophy and Method of Inquiry. J. Educ. Educ. Dev. 2018, 5, 215–222. [Google Scholar] [CrossRef]
- Schmidt, C. Phenomenology: An Experience of Letting go and Letting be. Waikato J. Educ. 2016, 11, 121–133. [Google Scholar] [CrossRef]
- Korstjens, I.; Moser, A. Series: Practical guidance to qualitative research. Part 2: Context, research questions and designs. Eur. J. Gen. Pract. 2017, 23, 274–279. [Google Scholar] [CrossRef]
- Malterud, K.; Siersma, V.D.; Guassora, A.D. Sample size in qualitative interview studies: Guided by information power. Qual. Health Res. 2016, 26, 1753–1760. [Google Scholar] [CrossRef]
- Thomas, D.R. A General Inductive Approach for Analyzing Qualitative Evaluation Data. Am. J. Eval. 2006, 27, 237–246. [Google Scholar] [CrossRef]
- Hubley, J.; Copeman, J. Practical Health Promotion; John Wiley & Sons: Hoboken, NJ, USA, 2018. [Google Scholar]
- Pakpour, A.H.; Griffiths, M.D.; Ohayon, M.M.; Broström, A.; Lin, C.-Y. A Good Sleep: The Role of Factors in Psychosocial Health. Front. Neurosci. 2020, 14, 520. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Frequency | Percentage |
|---|---|---|
| Age Mean ± SD | 17.49 ± 2.01 | |
| Gender | ||
| Male | 92 | 31.3 |
| Female | 202 | 68.7 |
| Current education status | ||
| University student | 68 | 23.1 |
| Bachelor | 81 | 27.5 |
| Secondary school/second | 74 | 25.2 |
| Secondary school/first | 52 | 17.6 |
| Other | 19 | 6.6 |
| Source | Males (n = 52) * | Females (n = 140) * |
|---|---|---|
| Television | 11.54% | 7.14% |
| Social media/Internet | 19.23% | 18.57% |
| Friends | 15.38% | 7.14% |
| Parents/Family | 23.08% | 21.43% |
| School | 23.08% | 41.43% |
| Health workers | 11.54% | 2.86% |
| Other sources (not specific) | 3.84% | 2.86% |
| Major Theme | Details | Subtheme |
|---|---|---|
| Taking care of my … | physical health mental health spiritual health | Thoughts Assets Body Motivations Positive performance Emotions/Feelings Nutrition Happiness General health Self-confidence |
| Protecting myself from…/Avoiding…. | Diseases Harming myself Bad friends Strangers Stress and anxiety Drugs and substance Social risks/sexual abuse Family/peer conflicts Harmful activities | |
| Understanding/Respecting | My calm and peace My spiritual needs My lifestyle My/others’ feelings Ideas |
| Activities | Male | Female | Total | |||
|---|---|---|---|---|---|---|
| N | (%) | N | (%) | N | (%) | |
| Spending time/going out with friends | 24 | 26.1% | 45 | 22.3% | 69 | 23.3% |
| Playing football | 36 | 38.3% | 0 | 0.0% | 36 | 12.2% |
| Going to gym | 52 | 55.3% | 20 | 9.9% | 72 | 24.3% |
| Video games | 44 | 46.8% | 18 | 8.9% | 62 | 20.9% |
| Technical work | 35 | 37.2% | 0 | 0.0% | 35 | 11.8% |
| Internet/social media | 92 | 100% | 78 | 38.6% | 176 | 59.5% |
| Going on vacation | 15 | 16.0% | 11 | 5.4% | 26 | 8.8% |
| Learning new skills | 20 | 21.3% | 35 | 17.3% | 55 | 18.6% |
| Praying | 8 | 8.5% | 21 | 10.4% | 29 | 9.8% |
| Cooking | 2 | 2.1% | 10 | 5.0% | 12 | 4.1% |
| Being alone | 15 | 16.0% | 0 | 0.0% | 15 | 5.1% |
| Listening to music | 44 | 46.8% | 80 | 39.6% | 124 | 41.9% |
| Playing music | 8 | 8.5% | 0 | 0.0% | 8 | 2.7% |
| Watching movies | 30 | 31.9% | 10 | 5.0% | 40 | 13.5% |
| Drinking tea and coffee | 5 | 5.3% | 15 | 7.4% | 20 | 6.8% |
| Healthy nutrition | 17 | 18.1% | 54 | 26.7% | 71 | 24.0% |
| Reading | 25 | 26.6% | 61 | 30.2% | 86 | 29.1% |
| Other sports | 20 | 21.3% | 25 | 12.4% | 45 | 15.2% |
| Art | 5 | 5.3% | 15 | 7.4% | 20 | 6.8% |
| Walking | 8 | 8.5% | 22 | 10.9% | 30 | 10.1% |
| Shopping | 10 | 10.6% | 58 | 28.7% | 68 | 23.0% |
| Dancing | 0 | 0.0% | 52 | 25.7% | 52 | 17.6% |
| Meditation | 8 | 8.5% | 14 | 6.9% | 22 | 7.4% |
| Sleeping | 20 | 21.3% | 20 | 9.9% | 40 | 13.5% |
| Fitness | 20 | 21.3% | 82 | 40.6% | 102 | 34.5% |
| Activities | Male | Female | Total | |||
|---|---|---|---|---|---|---|
| N | (%) | N | (%) | N | (%) | |
| Spending time/going out with friends | 12 | 12.8% | 22 | 10.9% | 34 | 11.5% |
| Playing football | 16 | 17.0% | 0 | 0.0% | 16 | 5.4% |
| Going to gym | 12 | 12.8% | 10 | 5.0% | 22 | 7.4% |
| Video games | 20 | 21.3% | 2 | 1.0% | 22 | 7.4% |
| Technical work | 4 | 4.3% | 0 | 0.0% | 4 | 1.4% |
| Cyberspace/social media | 20 | 21.3% | 69 | 34.2% | 89 | 30.1% |
| Going on vacation | 2 | 2.1% | 0 | 0.0% | 2 | 0.7% |
| Learning new skills | 2 | 2.1% | 5 | 2.5% | 7 | 2.4% |
| Praying | 2 | 2.1% | 2 | 1.0% | 4 | 1.4% |
| Cooking | 2 | 2.1% | 7 | 3.5% | 9 | 3.0% |
| Being alone | 4 | 4.3% | 0 | 0.0% | 4 | 1.4% |
| Listening to music | 8 | 8.5% | 28 | 13.9% | 36 | 12.2% |
| Playing music | 6 | 6.4% | 8 | 4.0% | 14 | 4.7% |
| Watching movies | 22 | 23.4% | 52 | 25.7% | 74 | 25.0% |
| Reading | 34 | 36.2% | 38 | 18.8% | 72 | 24.3% |
| Painting | 0 | 0.0% | 8 | 4.0% | 8 | 2.7% |
| Walking | 4 | 4.3% | 5 | 2.5% | 9 | 3.0% |
| Shopping | 2 | 2.1% | 18 | 8.9% | 20 | 6.8% |
| Dancing | 0 | 0.0% | 10 | 5.0% | 10 | 3.4% |
| Meditation | 4 | 4.3% | 5 | 2.5% | 9 | 3.0% |
| Sleeping | 2 | 2.1% | 5 | 2.5% | 7 | 2.4% |
| Physical activities | 20 | 21.3% | 24 | 11.9% | 44 | 14.9% |
| Female | Male | ||
|---|---|---|---|
| Terms | Keywords (%) | Terms | Keywords (%) |
| Recreationalactivities | Going to party with friends (21.8), Cyberspace (10.4), Going to concerts/theaters (2.5), Watching movies (6.4), Music (3), Going to bars/nightclubs (4.9), spending time outside home late at night (2.5), traveling (25.2), Adventure (20.3), even more shopping (2.5), More reading (10.9) | Recreational activities | Having fun with friends (19.6), Cyberspace (14.1), Going to concerts/theaters (8.7), Watching movies (10.9), Music (6.5), Going to bars/nightclubs (2.2), traveling (26.1), Adventure (8.7), even more shopping (8.7), camping in deserts/jungles (4.3), Watching football (1.1), More reading (10.9) |
| Sports activities | Outdoor physical activities (16.8), Swimming (5.9), Mountain climbing (4.5), Cycling (4.5), motorcycling (4), Football (4), Horse-riding (2.5), rallying (2), Shooting (0.5), Martial arts (3) | Sports activities | Fitness (2.2), Swimming (17.4), Mountain climbing (1.1), Football (1.1), Horse-riding (1.1), rallying (2.2), Professional/luxury gym (1.1), Water sports (4.3) |
| Scientific/Educational activities | Learning professional dancing (10.9), New language (4), Musical instruments (8.9) | Scientific/Educational activities | New language (4.3), Musical instruments (4.3), Professional technical work (1.1), Computer science (4.3) |
| Art activities | Painting (4.9), dancing (4), Handcrafts (1), Photography (1) | Art activities | Painting (1.1), general art (8.7) |
| Other activities | Charity (9.9), Riding/driving luxury cars (1), driving cars with high speed (1), Unusual dangerous things (1) | Other activities | Riding/driving luxury cars (2.2), Charity (4.3), Even more alone (1.1), Visiting successful people in the world (1.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohammadzadeh, M.; Alizadeh, T.; Awang, H.; Mohammadzadeh, Z.; Mirzaei, F.; Stock, C. Knowledge, Perspectives, and Priorities Regarding Self-Care Activities: A Population-Based Qualitative Study among Iranian Adolescents. Adolescents 2021, 1, 123-137. https://doi.org/10.3390/adolescents1020010
Mohammadzadeh M, Alizadeh T, Awang H, Mohammadzadeh Z, Mirzaei F, Stock C. Knowledge, Perspectives, and Priorities Regarding Self-Care Activities: A Population-Based Qualitative Study among Iranian Adolescents. Adolescents. 2021; 1(2):123-137. https://doi.org/10.3390/adolescents1020010
Chicago/Turabian StyleMohammadzadeh, Marjan, Tayebe Alizadeh, Hamidin Awang, Zahra Mohammadzadeh, Frahnaz Mirzaei, and Christiane Stock. 2021. "Knowledge, Perspectives, and Priorities Regarding Self-Care Activities: A Population-Based Qualitative Study among Iranian Adolescents" Adolescents 1, no. 2: 123-137. https://doi.org/10.3390/adolescents1020010
APA StyleMohammadzadeh, M., Alizadeh, T., Awang, H., Mohammadzadeh, Z., Mirzaei, F., & Stock, C. (2021). Knowledge, Perspectives, and Priorities Regarding Self-Care Activities: A Population-Based Qualitative Study among Iranian Adolescents. Adolescents, 1(2), 123-137. https://doi.org/10.3390/adolescents1020010