1. Introduction
Forensic dentistry plays a crucial role in human identification, especially in situations where other methods fail, such as victims of natural disasters, fires or bodies in a high state of decomposition. Teeth are highly durable and resistant in extreme situations, such as heat or dehydration, and are often the only viable element for human identification in these contexts [
1,
2]. The uniqueness of dental structures such as restorations, cavities, fractures, and dental anatomy allows for precise identification based on a comparison of ante-mortem and post-mortem dental records [
3]. Clinical records are fundamental to the effectiveness of cadaveric identification, as they provide an indispensable basis for comparison when identifying victims. The absence of complete, illegible, or outdated medical records can make identification impossible, even when teeth are preserved [
4]. These records should include detailed data on the initial condition of the tooth, treatments carried out that are included in the medical record, radiographs, photographs, and any other type of clinical documentation that the dentist may find revealing [
5]. Photographs and panoramic radiographs are powerful tools in the forensic context, allowing morphological details, treatments, and dental materials used to be compared [
6,
7].
Dental materials used in restorations and prostheses, such as amalgam (AM), composite resin (CR), glass ionomer (GI), and ceramic or metal-ceramic crowns (CC/MCC), are also important in Forensic Dentistry due to their unique characteristics. AM is widely used in posterior tooth restorations due to its resistance to wear and ability to withstand high masticatory loads [
8]. Resins, on the other hand, are widely used due to their esthetic qualities and versatility but are more sensitive to extreme temperatures and less durable than AM [
9]. Another relevant material in Forensic Dentistry is GI, which, in addition to being used in provisional restorations, stands out for its ability to release fluoride, which makes it useful in preventing dental caries [
10]. However, their mechanical properties are inferior to those of composite resins, with lower compressive strength and greater susceptibility to degradation [
11]. CC/MCC are recognized for their esthetics and similarity to natural teeth. In particular, MCC offers greater mechanical resistance due to the presence of an internal metal structure and is widely used in areas with a higher masticatory load [
12].
In situations of exposure to high temperatures, teeth and restorative materials undergo predictable changes, which can be analyzed to provide important information about the condition of the body at the time of death [
13]. For example, enamel, which is highly mineralized, can fracture due to contraction of the underlying dentin, while dehydration of the soft tissues of the oral cavity exposes the front teeth, making them more vulnerable [
14]. These changes can be used as indicators of heat and exposure time, making it easier to reconstruct the circumstances of death [
15].
Therefore, the combination of analyzing dental characteristics and restorative materials with rigorous scientific methods allows for the identification of victims in very challenging scenarios. But the effectiveness of the methods depends heavily on the quality and completeness of the clinical records and the detailed documentation of the interventions carried out throughout the patient’s life. Therefore, the aim of this study is to assess the current state of dentists’ knowledge about changes in dental materials exposed to heat and the importance of clinical records from a forensic perspective.
2. Materials and Methods
From January to June 2024, information was collected through an online questionnaire (
Supplementary Materials Supplement S1—Questionnaire S1) using a snowball sampling method, as some dentists invited other dentists to participate by sharing the link from the Google Forms platform. Since, in this method, the sample is not randomly selected, findings cannot be easily generalized to the broader population. In this way, snowball sampling can lead to a non-representative sample by overrepresenting certain groups while excluding others, limiting the generalizability of the findings.
The questionnaire underwent a pre-test by a group of dentists. The goal is to improve the questionnaire in accordance with the found limitations. A full validation is planned as part of the authors’ ongoing research. The questionnaire targeted dentists from Portugal and Brazil.
It included sociodemographic information—such as sex, age, years of professional experience, and the country where they practice—perceptions about the importance of clinical records (the significance of the topic and what they prioritize in their daily practice), and questions about the influence of high temperatures (ranging from 200 °C to 1100 °C), heat exposure duration, resistance, and changes in colour and shape of materials and dental structures. The dental materials assessed were resin composite (CR), amalgam (AM), glass ionomer cement (GI), and metal-ceramic crowns (MCCs), while the dental structures analyzed included enamel and dentin.
Additionally, the questionnaire included questions regarding experience with Forensic Dentistry, whether during undergraduate education, postgraduate education, or both. Thus, it was assumed that the responses from participants who had contact with the field during undergraduate education were based on theoretical knowledge, whereas those who had exposure in postgraduate education or both levels of education had acquired knowledge through both theoretical learning and clinical experience.
A Likert scale from 1 to 5 was used to rate the importance and influence of the variables investigated. The sample was analyzed using descriptive and inferential statistics using the SPSS statistics programme, v. 30. Statistical significance was set at 0.05. The Kolmogorov–Smirnov test with Lilliefors correction verified the normality of the variables ‘age’ and ‘time working in the profession’. The Mann–Whitney test assessed the difference in importance attributed to clinical records in relation to variables such as gender, age and country of practice. McNemar’s test was used to compare what participants considered to be included and valued in clinical records. Chi-squared tests assessed the association between time in practice and items included in clinical records, while Friedman, followed by multiple comparisons using Bonferroni correction and Wilcoxon tests, compared the influence of heat exposure time on dental materials and dental pieces, respectively. The Kruskal–Wallis test compared the participants’ perceptions of the influence of Forensic Dentistry at different stages of their academic training.
3. Results
The study included 272 dentists, of whom 176 (64.7%) practised in Portugal and 96 (35.3%) in Brazil.
The respondents’ ages ranged from 22 to 66, with a median age of 39.0 years. The “time working in the profession” ranged from less than a year to forty-two years, with a median of 11.0 years of professional experience. As the results of the Kolmogorov–Smirnov test with Lilliefors correction indicated that the age variable (p < 0.001) and the length of professional activity (p < 0.001) did not follow a normal distribution, it was decided, for further analyses, to divide each into two groups based on the medians. For age, the groups were defined as ‘age < 39 years’ and ‘age ≥ 39 years’. For the length of professional experience, the groups were defined as ‘length of experience 11 years’ and ‘length of experience ≥ 11 years’. Concerning gender, most respondents were female (67.3%) and the rest male (32.7%). In addition, 210 dentists (77.2%) said they had encountered Forensic Dentistry in undergraduate education, 44 (16.2%) in postgraduate education and 18 (6.6%) in both.
The results of this study show that dentists clearly value complete clinical records, with 91.9% of them considering them to be very important.
There was no statistically significant difference in the degree of importance attributed to clinical records in relation to the gender (p = 0.696) and age (p = 0.676) of the respondents, nor in relation to the length of time they had worked in the profession (p = 0.377) and the country in which they practised (p = 0.393).
Medical records and radiographs were recognized as essential components, valued by 97.8% of respondents, and included by nearly the same percentage (
Table 1). Although 83.1% of dentists consider photographs to be important, only 50.4% use them regularly. As for models, 63.2% of dentists appreciate their importance, but only 30.1% consistently include them in their clinical records, as can be seen in
Table 1 below. Furthermore, the McNemar test showed a significant discrepancy when it came to the inclusion of photographs (
p < 0.001) and models (
p < 0.001) in the diary entries. The chi-squared test also showed that dentists with more professional experience were more likely to include models in their clinical records (
p = 0.001).
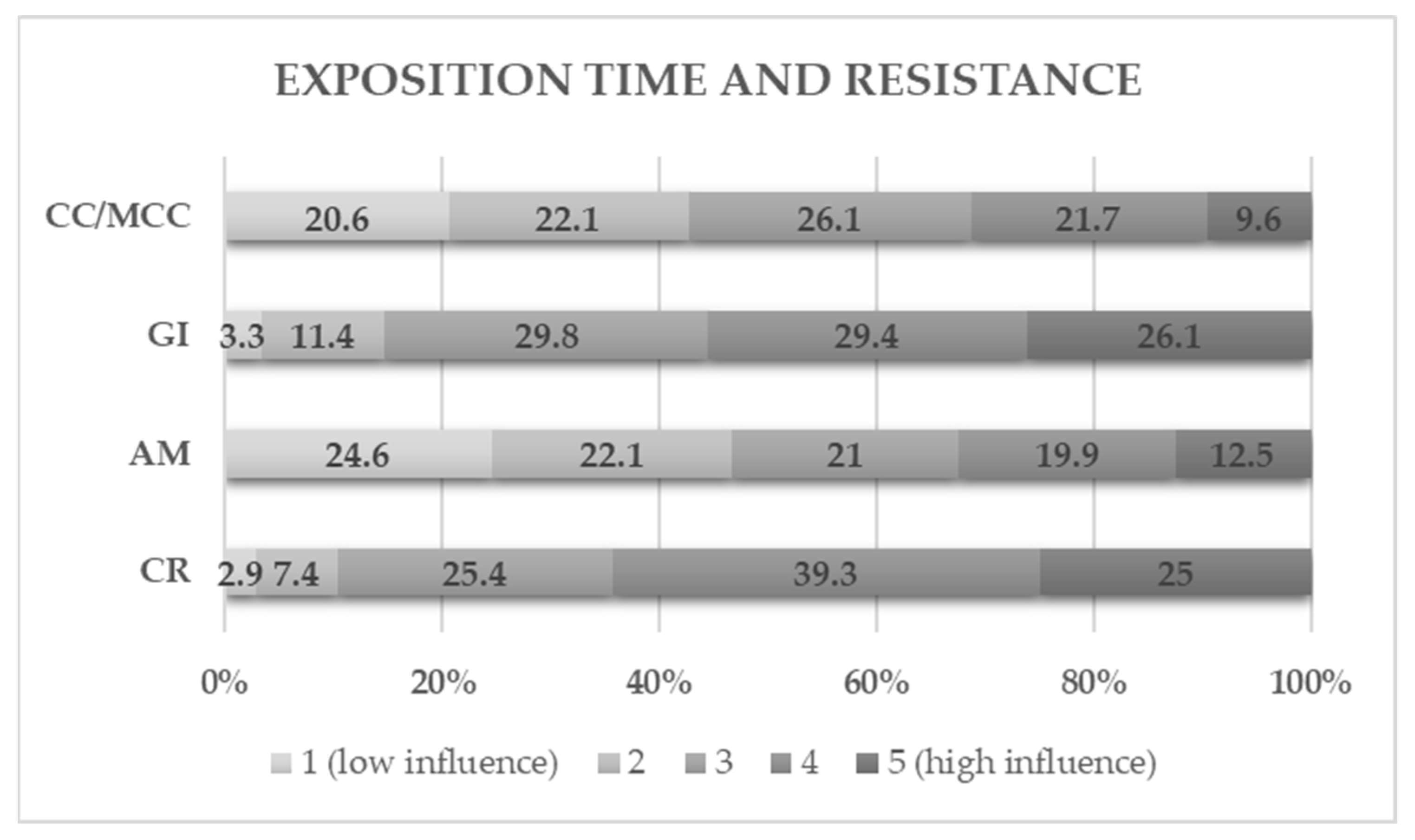
Regarding dental materials, CR and GI are seen as the most vulnerable, with 25% and 26.1% of dentists believing that time highly affects their resistance, respectively (
Figure 1). On the other hand, AM and CC/MCC are perceived as the most stable, with 24.6% and 20.6% of respondents, respectively, believing that exposure time has a low influence on its durability. The Friedman test, followed by multiple comparisons, revealed that, according to the dentists, only the CC/MCC-AM (
p = 1.000) and GI-CR (
p = 0.810) groups did not show statistically significant differences in resistance to high temperatures, with GI and CR being the most affected.
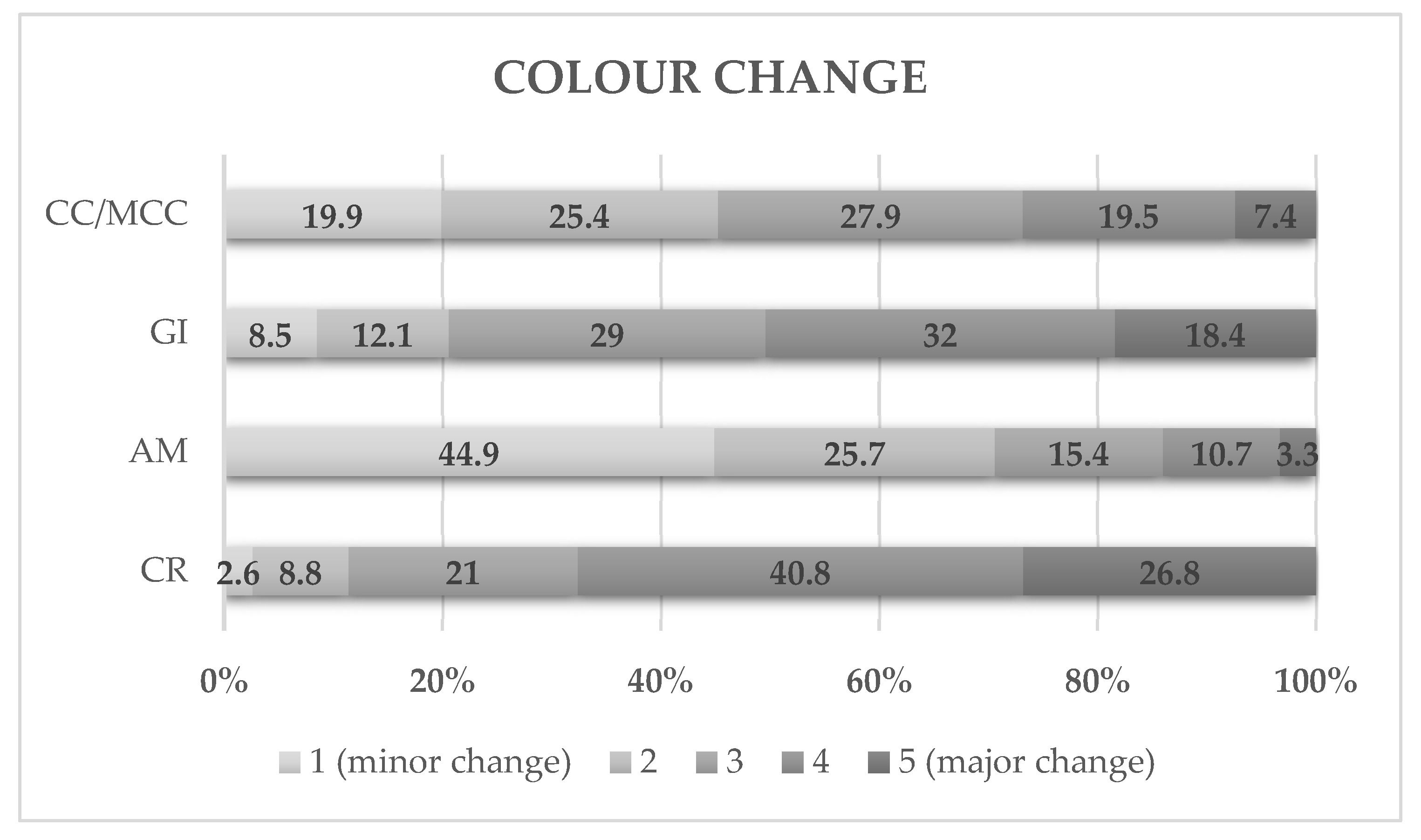
For the group of questions regarding colour changes, resin was perceived as the most susceptible to changes, with 67.6% of the answers pointing to considerable or major changes. AM is seen as the most stable, undergoing minor changes, with 44.9% of responses (
Figure 2). The perception of GI and CC/MCC is more varied but converges on the idea that both undergo moderate colour changes. Regarding colour, the Friedman test and multiple comparisons of order means revealed statistically significant differences (
p < 0.001) between all the dental materials considered. From the perspective of the dentists surveyed, from the most susceptible to colour changes to the least susceptible, the dental materials are like this: CR, GI, CC/MCC, and AM.
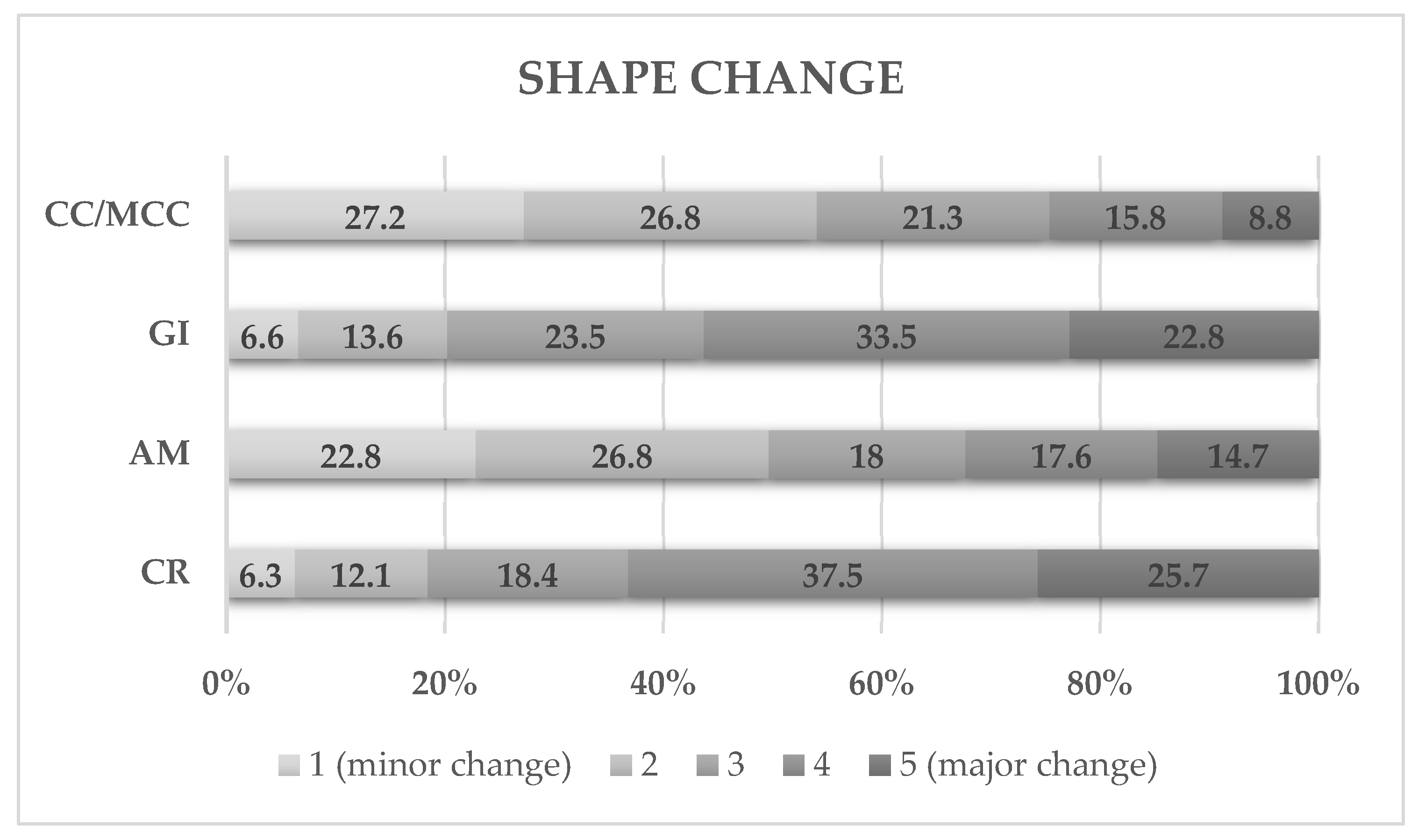
Regarding changes in shape (
Figure 3), CR (63.2%) and GI (56.3%) are presented as the most susceptible (considerable and major change), when compared to AM (32.3%) and CC/MCC (24.6%). After using the Friedman test and multiple comparisons it was possible to see that the respondents consider that GI-CR (
p = 0.711) and CC/MCC-AM (
p = 0.257) show similar behaviour regarding changes in shape.
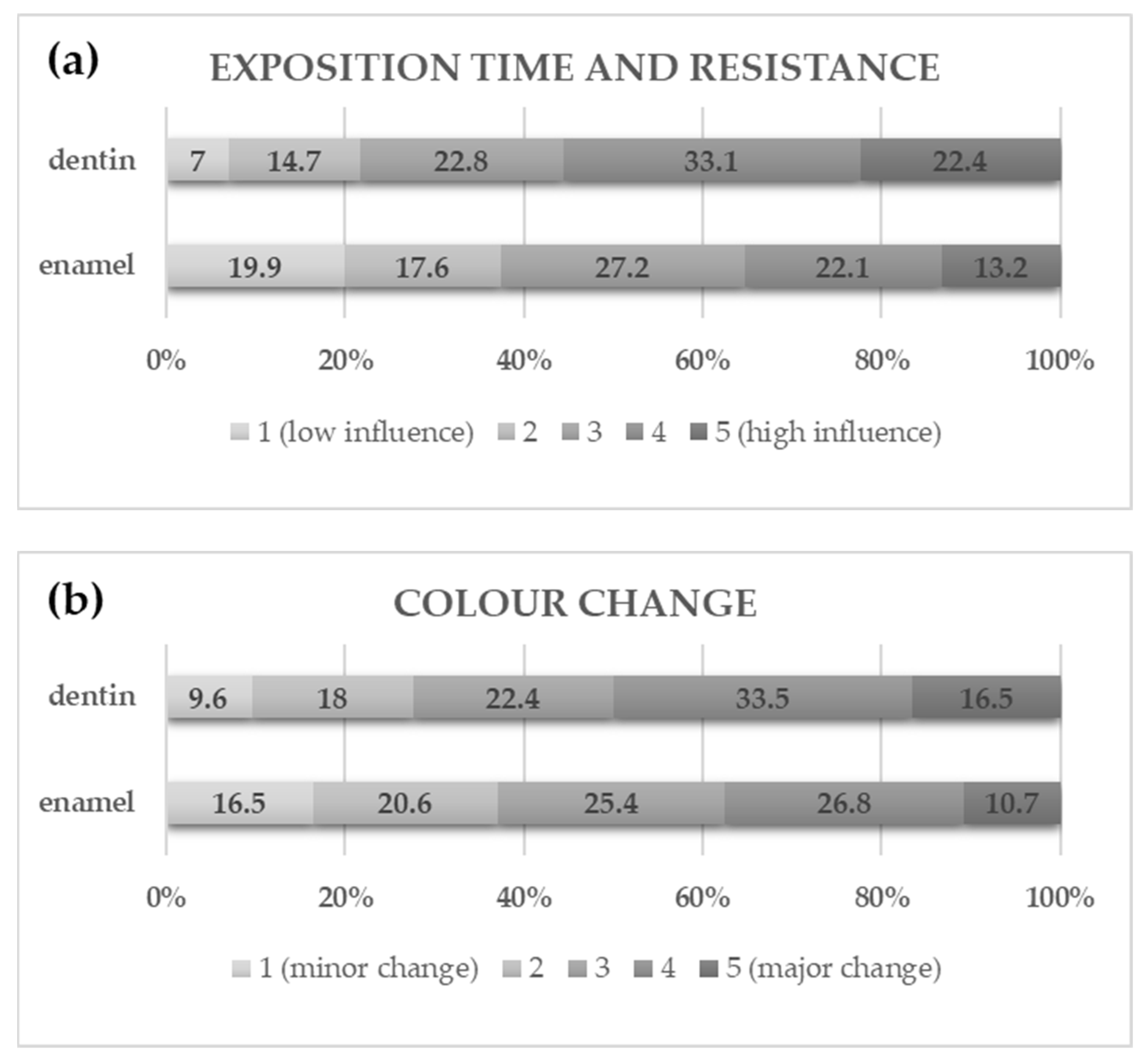
Regarding exposure time and the influence on the resistance of dental pieces to heat, respondents mentioned less influence on enamel (35.3%) compared to 55.5% on dentin (
Figure 4a). The Wilcoxon test (signed ranks) showed that the perception of the influence of exposure time on the resistance of enamel and dentin to heat is significantly different (
p < 0.001), with dentin being more affected than enamel. In addition, approximately 37.5% of the participants classified the colour changes in enamel as considerable and major, while 50.0% of the respondents gave this classification to dentin (
Figure 4b). The Wilcoxon test (signed ranks) revealed that the perception of colour changes after exposure to high temperatures in enamel and dentin is significantly different (
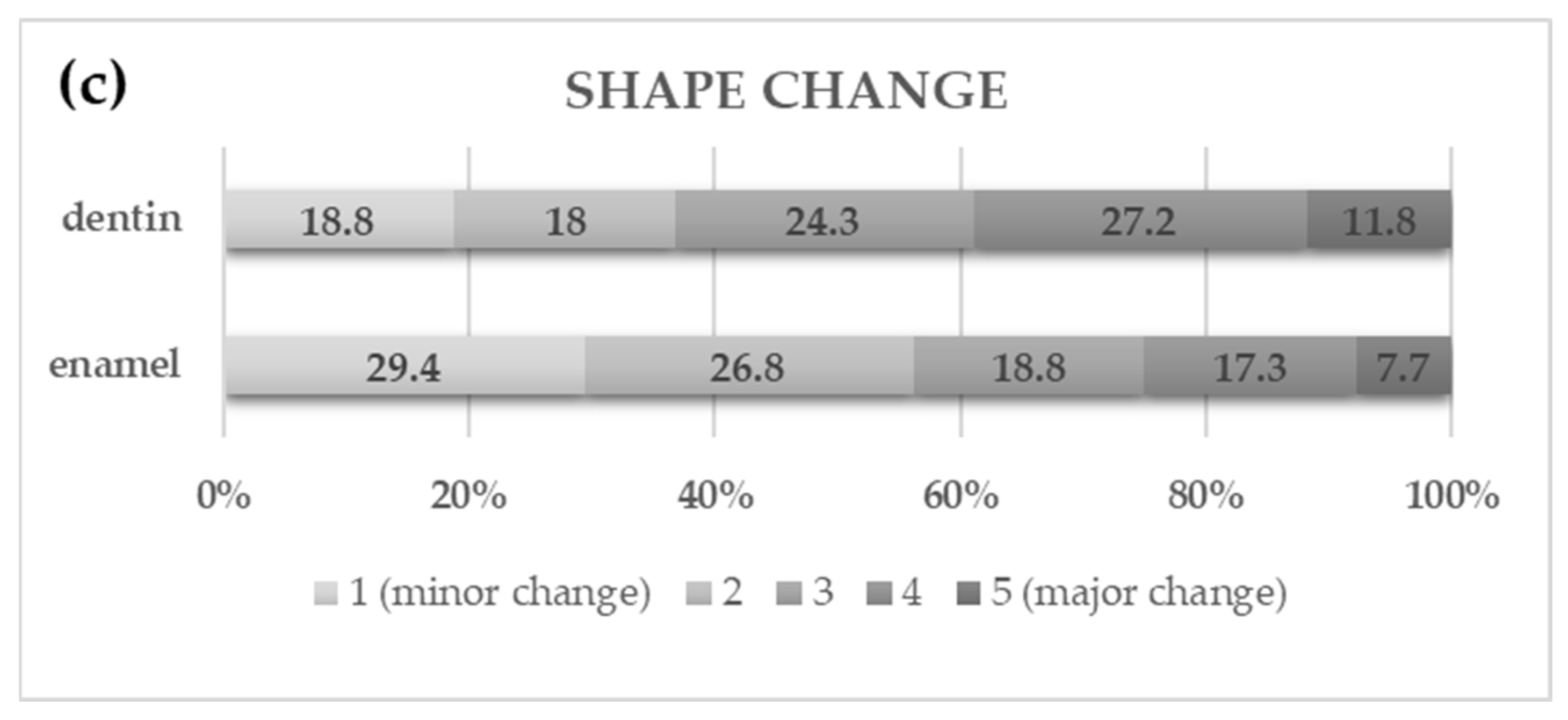
p < 0.001), with dentin being more susceptible to colour changes. Also, 29.4% of respondents indicated that enamel undergoes minor change in shape at high temperatures, while 7.7% indicated major changes. Dentin showed more balanced responses, with 18.8% and 11.8% of dentists saying that it suffers minor change and major change, respectively (
Figure 4c). Therefore, there is a greater consensus on the stability of enamel in terms of shape preservation during exposure to high temperatures. The Wilcoxon test (signed ranks) revealed that the perception of shape changes after exposure to high temperatures of enamel and dentin is significantly different (
p < 0.001), with dentin being also considered more susceptible to shape changes.
The Kruskal–Wallis test did not identified significant differences in the perception of changes in the resistance, colour and shape of dental materials between dentists, based on their contact with Forensic Dentistry. The only exception was the perception of changes in the resistance of AM, where a significant difference was found between the “undergraduate group” and the “both group” (p = 0.038), with dentists in the “both group” considering AM more susceptible.
4. Discussion
The importance of clinical records in dentistry is widely recognized and is essential for the quality and continuity of patient care. In 1994, Clark [
16] analyzed the crucial role of identification through dental records in ten disasters in the United Kingdom, and highlighted the difficulties faced in applying these methods, especially due to inconsistencies in clinical records. Therefore, it was suggested that the World Dental Federation should promote clear guidelines on how to fill in these registers correctly and that each country should publicize this information, considering that anyone, regardless of nationality, can be affected by disasters anywhere in the world.
This study found that, despite the unanimity of respondents’ opinions regarding the importance of complete clinical records, actual practice diverges from what is described in Article 30, paragraph 4 of the ethics code of the Portuguese Dental Association, which states that the patient’s clinical file should include the medical record and all diagnostic aids including photographs, models, imaging tests and all types of information collected during the diagnosis and treatment period, only 25% of dentists fully follow these guidelines. In addition, less experienced dentists value photographs more, while more experienced dentists prefer models, reflecting a generational difference in the use of technology. This discrepancy is worrying because it shows a gap between theoretical knowledge and actual practice and may be associated with various factors such as the type of training, available technology, clinical approach, and investment to be made in the latest machinery. However, out of a total of 272 surveyed dentists, 265 consider and value the medical record in their daily practice. So, it is possible to consider that this parameter is universal in clinical practice. Perhaps this phenomenon is related to the fact that the medical record is a comprehensive document for all specialties, as it covers a vast network of information, from the patient’s personal details to therapeutic interventions. However, the different types of clinical records can vary depending on the specialty in question, as each area values different tools. But the truth is that, although it is a highly valued document among dentists, it is important to recognize that, since it is based on written notes, it may be susceptible to human error. Variability in how it is filled out, accidental omissions, or subjective interpretations can compromise the accuracy of the clinical record.
Furthermore, different dental specialties use various tools for patient planning and documentation. Orthodontists and prosthodontists rely heavily on photographs and radiographs. In surgical and endodontic fields, radiographs are the most valued resource. General dentists, on the other hand, combine different tools as needed.
The restorative materials used in Dentistry are highly resistant to extremes of heat and react in a predictable way when subjected to different temperatures. In 2004, Merlati et al. [
17] found that from 200 °C onwards, AM showed microscopic bubbles on the surface due to the evaporation of mercury, and that at 1100 °C, this material remained in its original place, with its shape unchanged. On the other hand, at 400 °C, the CR already showed cracks and a black colour, and at 1100 °C, it remained in place, but with a completely altered shape. Later, Savio et al. [
18] found that the AM maintained its shape and location until 1000 °C. When considering temperatures in a fire event, it should be kept in mind that in a real-life incident a fire will not retain a consistent temperature, showing fluctuations with peaks and troughs depending upon fuel and oxygen availability and changes in surrounding temperatures [
19].
Miguel [
20] concluded that at 150 °C the AM was shiny, at 400 °C it became opaque and at 850 °C it began to turn red, with this colour becoming successively more intense up to 1000 °C and, from this temperature onwards, it took on a whitish red colour. Pol and Gosavi [
21] concluded that there was a clear superiority of ceramic materials in contrast to CR and GI, since at 1000 °C the CCs showed numerous bubbles on their surface, while the CR and GI were removed from the cavities and still showed rosy and black colours, respectively.
In the study, carried out by Pol et al. [
22], the authors observed cracks for GI from 200 °C, for CR from 400 °C and for AM from 800 °C. Fragmentation of GI was observed from 800 °C and of CR and AM from 1000 °C, while at this temperature, CC was the most resistant to heat, showing neither cracks nor fragmentation. In addition, Sharma’s [
23] in vitro study showed that AM and MCC restorations were identifiable up to 1200 °C, despite the disintegration of the tooth crown, while CR disappeared at 800 °C and GI from 600 °C.
In summary, it is possible to conclude that all the studies described almost unanimously propose that CC/MCC and AM are considered the most heat-resistant restorative materials and are therefore considered the most relevant for the dental identification of charred cadavers, a result that is in agreement with our study. This ideology is in line with dentists’ perceptions, since the majority believe that AM is the most stable for exposure time, and is therefore considered the most resistant, and that CC undergoes the least changes in shape when exposed to high temperatures. In the described studies, the materials most susceptible to colour and shape changes at high temperatures are GI and CR, results that are consistent with the conclusions of our study, since the respondents assume that these materials suffer the most shape changes and that CR is the most vulnerable and susceptible to colour changes, followed by GI, when compared to the other materials studied. CR was also perceived as the most vulnerable to exposure time, so in the opinion of dentists, its resistance is strongly affected when subjected to heat, corroborating what is concluded in the mentioned studies. The constant evolution of dental technologies not only provides new options for treatment but also requires dentists to update themselves regularly in order to optimize clinical results and patient satisfaction.
Teeth, per se, have the ability to withstand higher temperatures, both due to the histological topography of their mineralized tissues and their anatomical layout [
24]. Structural alterations to the enamel are therefore relevant, as this mineral tissue has a good capacity to resist heat. However, due to its prismatic nature, it becomes friable, i.e., brittle, at temperatures of around 400 °C [
25]. Dentin, which generally takes on a yellowish-white colour, is the mineralized tissue that occupies the largest volume of the tooth and, as a rule, this tissue is protected by enamel or bone. However, according to studies by Melani [
26] and Pereira [
25], at a temperature of 400 °C, multidirectional fractures can develop, taking on a brownish-black colour when it is charred. Carbonized teeth tend to suffer a change in volume of between 20 and 25%. This volume contraction is the most prevalent in the tissues that make up the crown and is mainly due to changes in dentin since it has a higher organic and water content compared to enamel. As enamel is essentially made up of inorganic material, it does not show any measurable changes. The remaining inorganic crystals of the structures tend to collapse into the gaps formed by the evaporation of the organic material, and when temperatures are above 800 °C, the fusion of these materials occurs, preventing volumetric changes and future fractures [
27]. Reesu et al. [
15] indicated that in many of the studies they evaluated, the change in colour is the most obvious as the temperature rises. At 500 °C, the dentin takes on a dark greyish-black colour, and there is a progressively greater tendency for the tissues to become lighter as the temperature rises, since at 900 °C they were all described as being almost white, progressing to porcelain white above 1000 °C, this whitening being associated with the progressive loss of water and dehydration of the tissues.
What can be concluded from the above-mentioned studies is that dentin is the first to undergo changes in colour, and it also suffers from the greatest number of variations. On the other hand, enamel is the first to undergo changes in shape and resistance since it is exposed, protecting dentin. Compared to the opinion of the dentists surveyed in this study, there is a discrepancy in the answers regarding the resistance of enamel, since they assume that enamel is more resistant and dentin is more vulnerable, which is not the case considering the studies, since enamel fragments first compared to dentin, despite being recognized at high temperatures.
Understanding and deepening the different responses concerning the constituents of the dental piece to environmental changes allows for a more precise and reliable analysis of human identification. Increasingly, especially in minimally invasive dentistry, the preservation of enamel during dental procedures is precious and tends to contribute to better forensic analysis, keeping more data available for evaluation, and emphasizing the importance of conservative and precise techniques.
The results of this study highlight the importance of dental materials in human identification under extreme conditions, demonstrating how the thermal stability of restorations can impact the preservation of unique dental characteristics. Furthermore, the inconsistency and incompleteness of clinical records emerge as critical challenges in forensic dentistry, potentially compromising the accuracy of the identification process. Therefore, the need for standardized documentation practises is reinforced to optimize its forensic applicability.
There are multiple situations where there is a need for human identification of carbonized bodies. An example of success is the study by Bush and Miller [
28]. The authors describe the identification of three victims from Colgan Air Flight 3407, which crashed in 2009 in the USA. The prolonged fire following the crash caused severe destruction of the victims’ bones and teeth. Another example described by Bux et al. [
29] occurred in Nepal in 2002, after a plane crash. The dental status of 14 European victims was examined during autopsy and after additional soft tissue removal. Antemortem records were available for 11 cases, allowing comparison. A re-examination of the jaws revealed that several dental restorations, including composite fillings, root fillings, and a parapulpal pin, had gone undetected during the initial autopsy. Since tooth-coloured restorations can be overlooked even by experienced forensic experts, full jaw resection and soft tissue removal are essential for accurate identification.
The study of Valenzuela et al. [
30], examines the role of dental identification in identifying 28 burn victims from a bus accident in Spain. Various postmortem forensic procedures were conducted, including external examination, routine photography, radiography, and complementary biological methods. The paper details the dental identification process, which successfully identified 57% of the victims. Among those under 20 years old, the identification rate increased to 76%. Additionally, dental age estimation contributed to identifying four victims. The findings highlight the importance of incorporating dental methods in post-disaster victim identification, as radiographic and odontological techniques are particularly effective for burn victims.
This study had some limitations that should be considered to improve future research, namely the lack of distinction between dental materials such as ceramic crowns and metal-ceramic crowns in the questions, which prevented a more detailed comparative analysis of the behaviour of these materials at high temperatures. Likewise, the questionnaire did not include an option for respondents to indicate that they had no experience with Forensic Dentistry, highlighting a limitation of the study. It was assumed that all respondents had some contact with the field during their academic journey, which may not be entirely accurate. Another point that could have been improved is the inclusion of questions about the place of training and area of specialization, which could generate professional and regional differences relevant to the study. Factors such as cultural influences, access to technology, and variations in clinical experience may contribute to these differences. While our study did not specifically focus on this aspect, future research could explore these elements through qualitative methods or comparative analyses across different regions and professional backgrounds.



 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}