

Age-at-Death Estimation by Dental Means as a Part of the Skeletal Analysis
Abstract
1. Introduction
2. Tooth Formation and Eruption
3. Dental Age Estimation Methods Based on Developmental Changes
4. Post-Formation Changes in the Dental Structures
5. Dental Age Estimation Methods Based on Post-Formation Changes
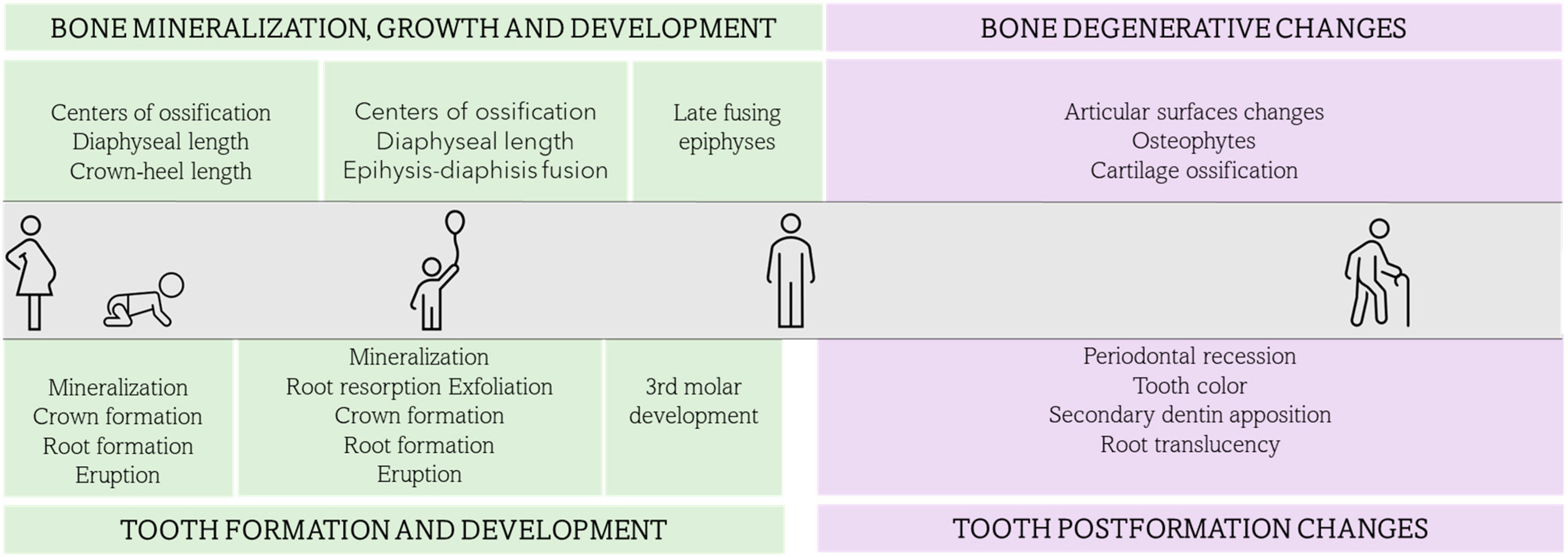
6. Integrating Dental Age Estimation in the Skeletal Analysis
7. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- ADA Technical Report No. 1077–2020. Available online: https://www.nist.gov/system/files/documents/2021/02/23/ADA%20Technical%20Report%20No.%201077_July_2020.pdf (accessed on 15 January 2023).
- Thesleff, I. The genetic basis of tooth development and dental defects. Am. J. Med. Genet. Part A 2006, 140, 2530–2535. [Google Scholar] [CrossRef]
- Thesleff, I. From understanding tooth development to bioengineering of teeth. Eur. J. Oral Sci. 2018, 126 (Suppl. 1), 67–71. [Google Scholar] [CrossRef]
- Yu, T.; Klein, O.D. Molecular and cellular mechanisms of tooth development, homeostasis and repair. Development 2020, 147, dev184754. [Google Scholar] [CrossRef]
- AlQahtani, S.J. Dental age estimation in fetal and children. In Age Estimation. A Multidisciplinary Approach; Adserias-Garriga, J., Ed.; Elsevier: London, UK, 2019; pp. 89–106. [Google Scholar]
- Nanci, A. Chapter 5: Development of the Tooth and Its Supporting Tissues. In Ten Cate’s Oral Histology: Development, Structure and Function, 9th ed.; Nanci, A., Ed.; Elsevier: St. Louis, MO, USA, 2018; pp. 68–90. [Google Scholar]
- Ono, W.; Sakagami, N.; Nishimori, S.; Ono, N.; Kronenberg, H.M. Parathyroid hormone receptor signalling in osterix-expressing mesenchymal progenitors is essential for tooth root formation. Nat. Commun. 2016, 7, 11277. [Google Scholar] [CrossRef]
- Takahashi, A.; Nagata, M.; Gupta, A.; Matsushita, Y.; Yamaguchi, T.; Mizuhashi, K.; Maki, K.; Ruellas, A.C.; Cevidanes, L.S.; Kronenberg, H.M.; et al. Autocrine regulation of mesenchymal progenitor cell fates orchestrates tooth eruption. Proc. Natl. Acad. Sci. USA 2019, 116, 575–580. [Google Scholar] [CrossRef]
- AlQahtani, S.J.; Hector, M.P.; Liversidge, H.M. Brief communication: The London atlas of human tooth development and eruption. Am. J. Phys. Anthropol. 2010, 142, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.M.; Senn, D.R. Dental age estimation. In Manual of forensic odontology, 5th ed.; Senn, D.R., Weems, R.A., Eds.; Taylor and Francis Group: Boca Raton, FL, USA, 2013; pp. 221–255. [Google Scholar]
- Adserias-Garriga, J.; Visnapuu, V. The neonatal line as evidence of live birth. Dental age estimation in fetal and children. In Age Estimation. A Multidisciplinary Approach; Adserias-Garriga, J., Ed.; Elsevier: London, UK, 2019; pp. 161–167. [Google Scholar]
- Nelson, S.J.; Ash, M.M. Development and eruption of the teeth. In Wheeler’s Dental Anatomy, Physiology, and Occlusion, 9th ed.; Saunders Elsevier: St. Louis, MO, USA, 2010; pp. 21–44. [Google Scholar]
- Scheid, R.C.; Weiss, G.; Woelfel, J.B. Primary (and Mixed) Dentition. In Woelfel’s Dental Anatomy, 8th ed.; Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012; pp. 164–193. [Google Scholar]
- Moorrees, C.; Fanning, E.; Hunt, E. Formation and resorption of three deciduous teeth in children. Am. J. Phys. Anthropol. 1963, 21, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Moorrees, C.; Fanning, E.; Hunt, E. Age variation of formation stages for ten permanent teeth. J. Dent. Res. 1963, 42, 1490–1502. [Google Scholar] [CrossRef] [PubMed]
- Demirjian, A.; Goldstein, H.; Tanner, J.M. A new system of dental age assessment. Hum. Biol. 1973, 45, 211–227. [Google Scholar] [PubMed]
- Demirjian, A.; Goldstein, H. New systems for dental maturity based on seven and four teeth. Ann. Hum. Biol. 1976, 3, 411–421. [Google Scholar] [CrossRef] [PubMed]
- AlQahtani, S.; Nuzzolese, E.; Adserias-Garriga, J. The accuracy of the London Atlas of Human Tooth Development and Eruption in dental age estimations of Saudi, Spanish, and Italian children. J. Forensic Odonto-Stomatol. 2017, 1, 62. [Google Scholar]
- Ishwarkumar, S.; Pillay, P.; Chetty, M.; Satyapal, K.S. Employing the London Atlas in the Age Estimation of a Select South African Population. Dent. J. 2022, 10, 171. [Google Scholar] [CrossRef]
- Namwong, W.; Mânica, S. Testing the London atlas for age estimation in Thai population. Acta Odontol. Scand. 2020, 78, 161–164. [Google Scholar] [CrossRef]
- McCloe, D.; Marion, I.; da Fonseca, M.A.; Colvard, M.; AlQahtani, S. Age estimation of Hispanic children using the London Atlas. Forensic Sci. Int. 2018, 288, 332.e1–332.e6. [Google Scholar] [CrossRef]
- Jayaraman, J.; Roberts, G.J.; Wong, H.M.; King, N.M. Dental age estimation in southern Chinese population using panoramic radiographs: Validation of three population specific reference datasets. BMC Med. Imaging 2018, 18, 5. [Google Scholar] [CrossRef] [PubMed]
- AlQahtani, S.J.; Hector, M.P.; Liversidge, H.M. Accuracy of dental age estimation charts: Schour and Massler, Ubelaker and the London Atlas. Am. J. Phys. Anthropol. 2014, 154, 70–78. [Google Scholar] [CrossRef]
- Harris, E.F. Mineralization of the mandibular third molar: A study of American blacks and whites. Am. J. Phys. Anthropol. 2007, 132, 98–109. [Google Scholar] [CrossRef] [PubMed]
- Mincer, H.H.; Harris, E.F.; Berryman, H.E. The ABFO study of the third molar development and it use as an estimator of chronological age. J. Forensic Sci. 1993, 38, 379–390. [Google Scholar] [CrossRef] [PubMed]
- Solari, A.C.; Abramovitch, K. The accuracy and precision of third molar development as an indicator of chronological age in Hispanics. J. Forensic Sci. 2002, 47, 531–535. [Google Scholar] [CrossRef]
- Blankenship, J.A.; Mincer, H.H.; Anderson, K.M.; Woods, M.A.; Burton, E.L. Third molar development in the estimation of chronologic age in American Blacks as compared with Whites. J. Forensic Sci. 2007, 52, 428–433. [Google Scholar] [CrossRef]
- UT-Age; Lewis, J.; Senn, D.; Silvaggi, J. Forensic Odontology at UT Health San Antonio School of Dentistry. Available online: www.utforensic.org (accessed on 15 January 2023).
- Graham, J.P.; O’Donnell, C.J.; Craig, P.J.; Walker, G.L.; Hill, A.J.; Cirillo, G.N.; Clark, R.M.; Gledhill, S.R.; Schneider-Kolsky, M.E. The application of computerized tomography (CT) to the dental ageing of children and adolescents. Forensic Sci. Int. 2010, 195, 58–62. [Google Scholar] [CrossRef]
- Marquez-Ruiz, A.B.; Treviño-Tijerina, M.C.; Gonzalez-Herrera, L.; Sanchez, B.; Gonzalez-Ramirez, A.R.; Valenzuela, A. Three-dimensional analysis of third molar development to estimate age of majority. Sci. Justice 2017, 57, 376–383. [Google Scholar] [CrossRef]
- De Tobel, J.; Phlypo, I.; Fieuws, S.; Politis, C.; Verstraete, K.L.; Thevissen, P.W. Forensic age estimation based on development of third molars: A staging technique for magnetic resonance imaging. J. Forensic Odontostomatol. 2017, 35, 117–140. [Google Scholar]
- Ten Cate, A.R.; Thompson, G.W.; Dickinson, J.B.; Hunter, H.A. The estimation of age of skeletal remains from the colour of roots of teeth. Dent. J. 1977, 43, 83–86. [Google Scholar]
- Solheim, T. Dental color as an indicator of age. Gerodontics 1988, 4, 114–118. [Google Scholar]
- Martin-de las Heras, S.; Valenzuela, A.; Bellini, R.; Salas, C.; Rubiño, M.; Garcia, J.A. Objective measurement of dental color for age estimation by spectroradiometry. Forensic Sci. Int. 2003, 132, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Martin de las Heras, E. Dental Age Estimation in Adults. Dental age estimation in fetal and children. In Age Estimation. A Multidisciplinary Approach; Adserias-Garriga, J., Ed.; Elsevier: London, UK, 2019; pp. 125–142. [Google Scholar]
- Kvaal, S.I.; Kolltveit, K.M.; Thomsen, I.O.; Solheim, T. Age estimation of adults from dental radiographs. Forensic Sci. Int. 1995, 74, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Solheim, T. Dental root translucency as an indicator of age. Eur. J. Oral Sci. 1989, 97, 189–197. [Google Scholar] [CrossRef]
- Lamendin, H.; Baccino, E.; Humbert, J.F.; Tavernier, J.C.; Nossintchouk, R.M.; Zerilli, A. A simple technique for age estimation in adult corpses the 2 criteria dental method. J. Forensic Sci. 1992, 37, 1373–1379. [Google Scholar] [CrossRef] [PubMed]
- Gustafson, G. Age determination on teeth. J. Am. Dent. Assoc. 1950, 41, 45–54. [Google Scholar] [CrossRef]
- Harris, E.F.; Mincer, H.H.; Anderson, K.M.; Senn, D.R. Age estimation from oral and dental structures. In Forensic Dentistry, 2nd ed.; Senn, D.R., Stimson, P.G., Eds.; Taylor & Frances Group: Boca Raton, FL, USA, 2010; pp. 263–303. [Google Scholar]
- Johanson, G. Age determinations from human teeth: A critical evaluation with special consideration of changes after fourteen years of age. Odontol. Rev. 1971, 22, 1–12. [Google Scholar]
- Prince, D.A.; DH Ubelaker. Application of Lamendin’s adult ageing technique to a diverse skeletal sample. J. Forensic Sci. 2002, 47, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Adserias-Garriga, J.; Nogué-Navarro, L.; Zapico, S.C.; Ubelaker, D.H. Setting the light conditions for measuring root transparency for age-at-death estimation methods. Int. J. Leg. Med. 2018, 132, 637–641. [Google Scholar] [CrossRef]
- Kvaal, S.I.; Solheim, T. A non-destructive dental method for age estimation. J. Forensic Odontostomatol. 1994, 12, 6–11. [Google Scholar]
- Cameriere, R.; Ferrante, L.; Belcastro, M.G.; Bonfiglioli, B.; Rastelli, E.; Cingolani, M. Age estimation by pulp/tooth ratio in canines by peri-apical X-rays. J. Forensic Sci. 2007, 52, 166–170. [Google Scholar] [CrossRef]
- Cameriere, R.; De Luca, S.; Aleman, I.; Ferrante, L.; Cingolani, M. Age estimation by pulp/tooth ratio in lower premolars by orthopantomography. Forensic Sci. Int. 2012, 214, 105–112. [Google Scholar] [CrossRef]
- Molina, A.; Bravo, M.; Fonseca, G.M.; Márquez-Grant, N.; Martín-de-Las-Heras, S. Dental age estimation based on pulp chamber/crown volume ratio measured on CBCT images in a Spanish population. Int. J. Leg. Med. 2021, 135, 359–364. [Google Scholar] [CrossRef]
- Merdietio Boedi, R.; Shepherd, S.; Oscandar, F.; Mânica, S.; Franco, A. 3D segmentation of dental crown for volumetric age estimation with CBCT imaging. Int. J. Leg. Med. 2023, 137, 123–130. [Google Scholar] [CrossRef]
- Fazekas, I.G.Y.; Kosa, F. Forensic Fetal Osteology; Akademiai Kaido: Budapest, Hungary, 1978. [Google Scholar]
- Scheuer, J.L.; Musgrave, J.H.; Evans, S.P. The estimation of late fetal and perinatal age from limb bone length by linear and logarithmic regression. Ann. Hum. Biol. 1980, 7, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Greulich, W.W.; Pyle, S.I. Radiographic Atlas of Skeletal Development of the Hand and Wrist; Stanford University Press: Redwood City, CA, USA, 1959. [Google Scholar]
- Warren, M.W. Radiographic determination of development age in fetuses and stillborns. J. For. Sci. 1999, 44, 708–712. [Google Scholar]
- Scheuer, L.; Black, S. Developmental Juvenile Osteology; Academic Press: San Diego, CA, USA, 2000. [Google Scholar]
- Gaskin, C.M.; Kahn, S.L.; Bertozzi, J.C.; Bunch, P.M. Skeletal Development of the Hand and Wrist: A Radiographic Atlas and Digital Bone Age Companion; Oxford University Press: New York, NY, USA, 2011. [Google Scholar]
- Langley-Shirley, N.; Jantz, R.L. A Bayesian approach to age estimation in modern Americans from the clavicle. J. Forensic Sci. 2010, 55, 571–583. [Google Scholar] [CrossRef] [PubMed]
- Shirley, N.R.; Jantz, R.L. Spheno-occipital synchondrosis fusion in modern Americans. J. Forensic Sci. 2011, 56, 580–585. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.; Suchey, J.M. Skeletal age determination based on the Os pubis: A comparison of the Acsdai-Nemeskeri and Suchey-Brooks methods. Hum. Evol. 1990, 5, 227–238. [Google Scholar] [CrossRef]
- Lovejoy, C.O.; Meindl, R.S.; Pryzbeck, T.R.; Mensforth, R.P. Chronological metamorphosis of the auricular surface of the ilium: A new method for the determination of adult skeletal age at death. Am. J. Phys. Anthropol. 1985, 68, 15–28. [Google Scholar] [CrossRef]
- Meindl, R.S.; Lovejoy, C.O. Ectocranial suture closure: A revised method for the determination of skeletal age at death based on the lateral-anterior sutures. Am. J. Phys. Anthropol. 1985, 68, 57–66. [Google Scholar] [CrossRef]
- Rouge-Maillart, C.; Jousset, N.; Vielle, B.; Gaudin, A.; Telmon, N. Contribution of the study of acetabulum for the estimation of adult subjects. Forensic Sci. Int. 2006, 171, 103–110. [Google Scholar] [CrossRef]
- Hartnett, K.M. Analysis of age-at-death estimation using data from a new, modern autopsy sample—Part II: Sternal end of the fourth rib. J. Forensic Sci. 2010, 55, 1152–1156. [Google Scholar] [CrossRef]
- Falys, C.G.; Prangle, D. Estimating age of mature adults from the degeneration of the sternal end of the clavicle. Am. J. Phys. Anthropol. 2015, 156, 203–214. [Google Scholar] [CrossRef]
- Shen, S.; Liu, Z.; Wang, J.; Fan, L.; Ji, F.; Tao, J. Machine learning assisted Cameriere method for dental age estimation. BMC Oral Health 2021, 21, 641. [Google Scholar] [CrossRef]
- Saric, R.; Kevric, J.; Hadziabdic, N.; Osmanovic, A.; Kadic, M.; Saracevic, M.; Jokic, D.; Rajs, V. Dental age assessment based on CBCT images using machine learning algorithms. Forensic Sci. Int. 2022, 334, 111245. [Google Scholar] [CrossRef]
- Zaborowicz, K.; Garbowski, T.; Biedziak, B.; Zaborowicz, M. Robust Estimation of the Chronological Age of Children and Adolescents Using Tooth Geometry Indicators and POD-GP. Int. J. Environ. Res. Public Health 2022, 19, 2952. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Mineralization | Crown Completion | Root Completion | Eruption | |||
|---|---|---|---|---|---|---|
| DECIDUOUS DENTITION | Central Incisor | Maxillary | 14th week iu | 1.5 months | 1.5 years | 7.5 months |
| Mandibular | 14th week iu | 2.5 months | 1.5 years | 6 months | ||
| Lateral incisor | Maxillary | 16th week iu | 3 months | 2 years | 9 months | |
| Mandibular | 16th week iu | 2.5 months | 1.5 years | 7 months | ||
| Canine | Maxillary | 17th week iu | 9 months | 3.5 years | 18 months | |
| Mandibular | 17th week iu | 9 months | 3.5 years | 16 months | ||
| 1st Molar | Maxillary | 15.5th week iu | 6 months | 2.5 years | 14 months | |
| Mandibular | 15.5th week iu | 5.5 months | 2.5 years | 12 months | ||
| 2nd Molar | Maxillary | 19th week iu | 11 months | 3 years | 24 months | |
| Mandibular | 18th week iu | 10 months | 3 years | 20 months | ||
| PERMANENT DENTITION | Central Incisor | |||||
| Mandibular | 3–4 months | 4–5 years | 9 years | 6–7 years | ||
| Lateral incisor | Maxillary | 10–12 months | 4–5 years | 11 years | 8–9 years | |
| Mandibular | 3–4 months | 4–5 years | 10 years | 7–8 years | ||
| Canine | Maxillary | 4–5 months | 6–7 years | 13–15 years | 11–12 years | |
| Mandibular | 4–5 months | 6–7 years | 12–14 years | 9–10 years | ||
| 1st Premolar | Maxillary | 1.5–1.75 years | 5–6 years | 12–13 years | 10–11 years | |
| Mandibular | 1.75–2 years | 5–6 years | 12–13 years | 10–12 years | ||
| 2nd Premolar | Maxillary | 2–2.5 years | 6–7 years | 12–14 years | 10–12 years | |
| Mandibular | 2.25–2.5 years | 6–7 years | 13–14 years | 11–12 years | ||
| 1st Molar | Maxillary | 0 month (birth) | 2.5–3 years | 9–10 years | 6–7 years | |
| Mandibular | 0 month (birth) | 2.5–3 years | 9–10 years | 6–7 years | ||
| 2nd Molar | Maxillary | 2.5–3 years | 7–8 years | 14–16 years | 17–21 years | |
| Mandibular | 2.5–3 years | 7–8 years | 14–16 years | 17–21 years |
| ¼ Resorption (SD) | ½ Resorption (SD) | ¾ Resorption (SD) | Exfoliation (SD) | |||
|---|---|---|---|---|---|---|
| Females | Canine | 4.9y (0.54) | 7.3y (0.78) | 8.7y (0.92) | 9.5y (1) | |
| 1st Molar | Mesial Root | 4.9y (0.54) | 7.2y (0.78) | 8.7y (0.93) | 9.5y (1.05) | |
| Distal Root | 5.1y (0.58) | 7.7y (0.82) | 9.3y (0.97) | 10.1y (1.05) | ||
| 2nd Molar | Mesial Root | 6.1y (0.67) | 8.3y (0.88) | 10y (1.005) | 11.1y (1.15) | |
| Distal Root | 6.9y (0.74) | 8.6y (0.91) | 9.9y (1.04) | 11.1y (1.16) | ||
| Males | Canine | 6.1y (0.67) | 8.4y (0.89) | 9.8y (1.02) | 10.6y (1.1) | |
| 1st Molar | Mesial Root | 5.4y (0.6) | 7.6y (0.82) | 9.4y (0.98) | 10.7y (1.12) | |
| Distal Root | 6.4y (0.69) | 8.3y (0.88) | 10y (1.04) | 10.7y (1.12) | ||
| 2nd Molar | Mesial Root | 6.6y (0.72) | 8.5y (0.99) | 10.04y (1.08) | 11.6y (1.2) | |
| Distal Root | 6.6y (0.79) | 8.5y (0.99) | 10.04y (1.14) | 11.6y (1.2) |
| Method | Dental Changes | Methodology | Sample Destruction | |
|---|---|---|---|---|
| Methods based on teeth formation and development | Ubelaker (1989) | Development and eruption | Radiographical assessment | No |
| AlQahtani (2010) | Development and eruption (deciduous and permanent) | No | ||
| Morrees, Faning and Hunt (1963) | Root resorption, exfoliation (deciduous) Development and eruption (permanent) | Radiographic assessment and scoring | No | |
| Demirjian (1973) | Development and eruption (permanent) | No | ||
| Mincer (1993) | Development and eruption (third molars) | No | ||
| Methods based on teeth postformation changes | Johanson (1971) | Dental wear, periodontal recession, secondary dentine formation, cementum apposition, root resorption, root translucency. | Macroscopic assessment | Yes |
| Lamendine (1992) | Root translucency, periodontal recession | Macroscopic measurements | No | |
| Prince and Ubelaker (2002) | Root translucency, periodontal recession | No | ||
| Kvaal (1995) | Secondary dentin apposition | Radiographic measurements | No | |
| Camariere (2004, 2007) | Secondary dentin apposition | No | ||
| Martin de las Heras (2003) | Dentin color | Spectroradiometric measurement | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adserias-Garriga, J. Age-at-Death Estimation by Dental Means as a Part of the Skeletal Analysis. Forensic Sci. 2023, 3, 357-367. https://doi.org/10.3390/forensicsci3020027
Adserias-Garriga J. Age-at-Death Estimation by Dental Means as a Part of the Skeletal Analysis. Forensic Sciences. 2023; 3(2):357-367. https://doi.org/10.3390/forensicsci3020027
Chicago/Turabian StyleAdserias-Garriga, Joe. 2023. "Age-at-Death Estimation by Dental Means as a Part of the Skeletal Analysis" Forensic Sciences 3, no. 2: 357-367. https://doi.org/10.3390/forensicsci3020027
APA StyleAdserias-Garriga, J. (2023). Age-at-Death Estimation by Dental Means as a Part of the Skeletal Analysis. Forensic Sciences, 3(2), 357-367. https://doi.org/10.3390/forensicsci3020027