Abstract
Objective: This study aimed to evaluate and compare the knowledge and attitudes of dentists and dental students regarding the early diagnosis of oral cancer. Study Design: Data were collected using a questionnaire administered to students on an integrated master’s degree in dentistry and to dentists. The data were then entered into SPSS, where they were statistically processed. Results: A total of 192 responses were considered (102 from dentists and 90 from dental students). Although both groups correctly recognized the gender most affected by the pathology, as well as the most common type of oral cancer, only 22.5% of dentists and 14.4% of students knew how to identify the sites with the greatest potential for malignancy. In both cases, the majority carried out a thorough intraoral assessment. Only less than half have ever performed a biopsy during their clinical practice. Only 4.9% of dentists and 3.3% of students consider their ability to diagnose pathology to be very good. Conclusions: Some gaps were observed and should be addressed, particularly in terms of knowledge about lesions with malignant potential. Therefore, it is crucial to invest in training in this area to halt the progression of this pathology.
1. Introduction
Oral cancer is a group of malignant neoplasms whose incidence has been increasing in recent years, making it the eighth most common cancer [1]. Recent global statistics reported 377,713 new cases and 177,757 deaths from oral cancer in 2020 worldwide [2]. The most common oral cancer is squamous cell carcinoma (SCC) since in the oral cavity, 90% of neoplasms have a histological origin in squamous cells [3]. Other tumors of the oral cavity include, for example, melanomas, lymphomas, and sarcomas [4].
The incidence of this pathology increases with age. It is most common in individuals aged between 50 and 60 years [4,5]. Males are the most affected, with a male-to-female ratio of 2:1. However, these figures have become less and less discrepant due to the adoption of smoking and alcohol habits by women and also by younger individuals [4]. It is clear that environmental influences, such as lifestyle, are factors that can potentiate the onset of most cancers, and oral cancer is no exception [6].
The incidence rates of oral cancer vary around the world due to the adoption of risk behaviors/factors associated with the disease [7]: (1) Tobacco: This has a dose-dependent relationship and remains the leading risk factor for oral cancer in any of its forms of consumption [6]; (2) Alcohol: An unequivocal causal relationship has been established between alcohol consumption and oral cavity cancer [8]. The concomitant consumption of alcohol and tobacco results in an increased risk of developing the condition [1]; (3) Human papillomavirus (HPV): HPV is consistently and more frequently detected in cancers of the oropharynx and tonsils than in other sites of the head and neck. HPV 16 and 18 tend to be the types most commonly found [9]; (4) UV radiation: This is more associated with cancer of the lower lip, often present in individuals who are professionally more exposed to sunlight and ultraviolet radiation [10]; (5) Oral health and diet: Poor oral health, although not an independent risk factor, is present in the majority of patients with cancer in this region [11]. A balanced diet reduces the risk of oral cancer and potentially malignant disorders [1]; (6) Potentially malignant disorders: Some cancers develop from potentially malignant disorders and/or conditions such as leukoplakia, erythroplakia, lichen planus, and discoid lupus erythematosus, among others. Not all of these need to turn into cancer; however, their presence significantly increases the risk, given that the malignant transformation of lesions is greater than that of healthy tissue [12].
At an early stage, oral cancer is mostly asymptomatic, and unfortunately, due to this factor, most patients are diagnosed at a much later stage of the disease [13]. In the absence of pain or overt clinical signs, early malignant or potentially malignant lesions may go unnoticed by patients and clinicians. Compounding this issue is the fact that the clinical presentation of early oral cancer often mimics that of common benign or traumatic lesions, such as frictional keratosis, aphthous ulcers, or areas of mucosal irritation caused by dental prostheses or occlusal trauma. These similarities can lead to a misinterpretation or underestimation of the lesion’s seriousness, especially during routine dental examinations, where such findings may be overlooked as transient or nonspecific. Consequently, valuable time may be lost before a definitive diagnosis is established, allowing the disease to progress to more advanced stages. This overlap underscores the crucial importance of heightened clinical vigilance, comprehensive soft tissue examination protocols, and timely referral or biopsy of persistent lesions, particularly those that do not resolve within two weeks or lack a clear traumatic etiology. Several characteristics can raise the suspicion of malignancy in a lesion (Table 1).

Table 1.
Characteristics of a lesion with suspected malignancy [14,15,16].
An effective way to reduce mortality, morbidity, and disease progression is to detect it at an early stage, when the lesions are still small and localized [17]. A correct oral cancer diagnosis should begin with an appropriate intraoral inspection and a detailed extraoral assessment. The importance of early screening and diagnosis is paramount because oral cancer detected at this stage is associated with significantly better prognosis, less invasive treatment, and higher survival rates. Conversely, late-stage diagnoses often result in poorer outcomes and more complex management. Therefore, any deficiencies in knowledge or attitudes, such as a lack of awareness of high-risk sites, limited clinical examination practices, or low confidence in diagnostic skills, can directly hinder early detection efforts. These gaps must be addressed to ensure that both students and professionals are adequately prepared to recognize early signs and contribute effectively to prevention strategies.
The dentist should pay attention to changes in the tissue’s color, elasticity, or even texture [18]. Screening can be more efficient by examining high-risk areas, such as the floor of the mouth, the posterior lateral edge of the tongue, and the soft palate [19]. In addition to detecting the disease, dentists also play a key role in rehabilitation, relieving the side effects of cancer therapy. It is common for these types of treatments to cause significant changes in the oral cavity, such as xerostomia, tooth decay, changes in taste, and mucositis. Regarding these aspects, the professional must act to improve the quality of life during cancer treatment [20].
Given the increasing prevalence of oral cancer, it is essential to expand knowledge about its characteristics. Only by knowing this reality will it be possible to draw data and conclusions for combating this pathology. Thus, this study aimed to understand the knowledge and attitudes of dentists and dental students regarding the prevention and early diagnosis of oral cancer.
2. Materials and Methods
All data collected were kept confidential, and anonymity was guaranteed throughout this study. The project was submitted and approved by the Portuguese Catholic University (UCP) Health Ethics Committee (protocol title “Knowledge and Attitudes of Dentists and Dental Medicine Students in the Prevention and Early Diagnosis of Oral Cancer”; no. 227/2022; date: 13 October 2022) and followed the Declaration of Helsinki (1964, revised 2024). All participants, prior to being included, signed an informed consent form.
2.1. Type of Study, Population, and Sample Selection
This is a cross-sectional, descriptive, observational study conducted by distributing an electronic questionnaire. It was administered electronically using Google Forms, allowing the participants to complete it remotely via computer or mobile devices. The survey link was distributed through email and messaging applications to facilitate broad and convenient access. Responses were collected anonymously, and data were stored securely within the platform to ensure participant confidentiality and compliance with data protection standards. The sample consisted of dentists and students in the 4th and 5th years of an integrated master’s degree in dental medicine in Portugal who responded anonymously and voluntarily to the data collection instrument.
2.2. Data Collection Instrument
The data collection instrument, adapted from the questionnaires by Horowitz (2000) [21], was initially pre-tested. It was administered to 20 participants (10 local dentists and 10 students) who were not included in this study. After completing it, all participants were asked to identify aspects that could be improved, relevant questions that should be included in the final questionnaire, and the clarity of the wording used in the questions. The results are presented in Table 2.
Table 2.
Pre-test comparing results between dentists and dental students.
After verifying the pre-test’s results, the final version was divided into four groups: (I) personal characterization of the oral health professional; (II) oral cancer and potentially malignant disorders; (III) clinical practice in diagnosing oral cancer; and (IV) personal opinion.
The data collected were socio-demographic data, such as nationality, gender, and age; years of clinical experience; information on attendance at training courses in the field of oral medicine; questions about potentially malignant disorders, including preferred site, appearance, and prevalence; questions about oral cancer: most affected gender and age group, subtype, location, and risk factors; clinical practice: intraoral and extraoral examination techniques; patient education for oral cancer self-screening; personal attitude toward a patient with lesions with malignant potential; questions about how to perform a biopsy and the technique/instrument used; personal opinion: the ability to make a clinical diagnosis of a lesion with malignant potential and ability to perform a biopsy; the importance of the dentist in the prevention and detection of oral cancer; and the level of training to work in the field of oral medicine, especially in the detection of oral cancer.
2.3. Data Analysis
After collecting the data, it was coded and entered into the Statistical Package for the Social Sciences (SPSS) software version 26.0, where the statistical treatment was carried out. Descriptive analysis used frequency distributions through tables, appropriate statistical measures, and graphical representations. The inferential analysis used the Mann–Whitney and Kruskal–Wallis non-parametric tests. The significance level was 5% (p < 0.05).
3. Results
3.1. Personal Characterization
A total of 102 responses were received from dentists and 90 from dental students. Table 3 shows the results regarding the personal characterization of the study participants. The majority of the sample was female (64.7% of dentists and 64.4% of students) and individuals aged between 21 and 30 (31.4% of dentists versus 92.2% of students). In terms of nationality, most respondents were Portuguese. Regarding clinical experience, 26.4% (n = 30) of the surveyed dentists had been practicing for less than 5 years, while the majority, 61.8% (n = 63), had been practicing for more than 10 years. Regarding the year of study, 53.3% (n = 48) of the respondents were in their fourth year, and 46.7% (n = 42) were in their fifth year.
Table 3.
Sample characterization.
3.2. Oral Cancer and Potentially Malignant Disorders
As Figure 1a,b show, when asked about the gender and age group most affected by the pathology, the vast majority of the students and dentists consider that males (69.6% dentists; 50.0% dental students) are the most affected, as well as individuals over the age of 40 (86.3% dentists; 88.9% dental students). Regarding the most common type of oral cancer, carcinoma was the answer most frequently selected by the participants in both groups, chosen by 73.5% of dentists and 83.3% of dental students (Figure 2a,b).
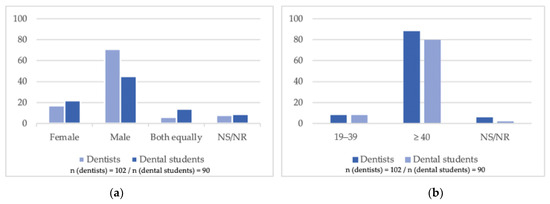
Figure 1.
(a) Gender and oral cancer: Which gender is most often affected by oral cancer? (b) Age and oral cancer: What is the most common age group for oral cancer? (NS/NR = not submitted/not reported).
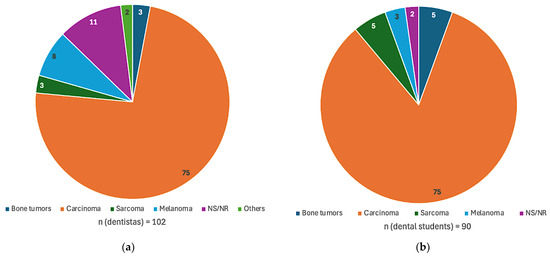
Figure 2.
(a) Dentists’ knowledge: characterization of knowledge about the most common type of oral cancer, according to dentists; (b) students’ knowledge: according to dental students (NS/NR = not submitted/not reported).
Figure 3 illustrates the results of the characteristics considered to have a greater malignancy potential for each group. It is worth noting that a significant number of dental students have mistakenly considered slow-growing lesions and soft, exophytic lesions to have a greater potential for malignancy. When asked about the sites with the most significant potential for malignancy, the most selected option was the tongue (71.6% dentists; 84.4% dental students), followed by the floor of the mouth (48.0% dentists; 65.6% dental students) and the jugal mucosa (30.4% dentists; 44.4% dental students). Both groups identified leukoplakia as the most common potentially malignant disorder (68.6% dentists; 67.8% dental students). However, a total of 20 respondents believed that traumatic fibroma is a potentially malignant lesion. Tobacco and alcohol were the risk factors most mentioned by both groups (Table 4).
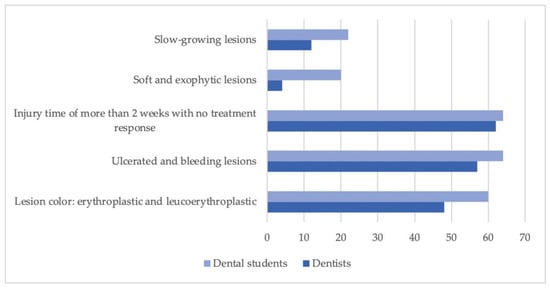
Figure 3.
Distribution of characteristics associated with higher malignancy potential. The figure presents a comparative analysis of key parameters identified as indicative of greater malignancy risk, stratified by group. Each bar represents the percentage of a specific characteristic within each group.
Table 4.
Answers about knowledge of oral cancer and potentially malignant disorders/conditions, and characterization of practice and attitudes.
3.3. Clinical Practice in Oral Cancer Diagnosis
According to Table 3, most individuals in both groups claim to perform a complete intraoral (95.1% dentists; 94.4% dental students) and extraoral (63.7% dentists; 81.1% dental students) examination of their patients. However, few dentists (30.4%)/students (37.8%) instill in all their patients the importance of self-examining for oral cancer. When asked about performing biopsies, the results are shown in Figure 4a,b.
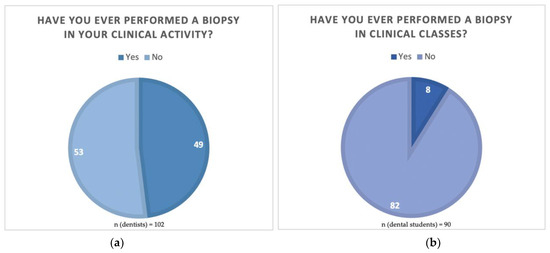
Figure 4.
(a) Biopsy in clinical activity: clinical practice of biopsies in the group of dentists and (b) biopsy in classes: in the group of dental students.
3.4. Personal Opinion
Table 5 shows the results of the respondents’ perceptions of their abilities to carry out a clinical diagnosis of oral cancer, as well as to perform a biopsy. Most dentists and students consider their ability to make a diagnosis only reasonable. Almost half of dentists (45.1%) feel uncomfortable performing biopsies, which contrasts with the more optimistic view of the student group, where around half (48.9%) consider themselves to have a reasonable capacity to do so. Both groups unanimously believe that healthcare professionals are essential in preventing and detecting oral cancer.
Table 5.
Perception of the capacity and importance of oral cancer prevention and detection.
4. Discussion
This study aimed to understand the knowledge and attitudes of dentists and dental students regarding the prevention and early diagnosis of oral cancer; it comprised a sample of 90 students from the integrated master’s degree in dental medicine and 102 professional dentists with consolidated clinical experience. With a total sample of 192 respondents, it was observed that most of the study participants were female, representing 64.7% of the dentists and 64.4% of the students. These results align with studies by Bhattacharjee et al. [22] and Gomes et al. [23], which also found that the majority of their participants were female. Otherwise, in the study by Kumar et al. [24], the sample consisted primarily of males.
When analyzing clinical experience, it was found that 26.4% of dentists had been practicing for less than 5 years, while the majority (61.8%) had been practicing for more than 10 years. In a similar study [25], the majority had more than 20 years of clinical experience. When assessing the outcomes in the present study, both dental students and dentists shared a similar view regarding the gender and age group most commonly affected by the pathology under study.
Concerning gender, most participants, both dentists (69.6%) and dental students (50.0%), believe that males are the most affected. Decuseara et al. [26] found the same results. Oral cancer exhibits a notable gender disparity, with a higher prevalence observed in males compared to females. This trend is supported by studies, indicating that the male-to-female ratio for oral cancer cases typically ranges from approximately 2:1 to 2.4:1 in various regions, reflecting a significant male predominance [27,28,29]. Factors contributing to this disparity include differential exposure to carcinogenic behaviors such as tobacco use and excessive alcohol consumption, which are more prevalent among males [30,31]. Specifically, evidence suggests that men are at a significantly elevated risk due to their higher rates of smoking and alcohol intake, which are well-documented risk factors for oral cancers, including squamous cell carcinoma [32,33]. This response consistency highlights the importance of considering gender as a relevant factor in the clinical approach and prevention of the pathology.
Regarding the age group, dentists (86.3%) and dental students (88.9%) consider individuals over 40 years old to be the most affected by the pathology. Silva et al. [34] found the same results. This perception may be related to the physiological changes and specific risk factors that are more prevalent in this age group.
The results of the presented study clearly show that dentists and dental students shared a similar view regarding the most common type of oral cancer. Both groups selected carcinoma, similar to the studies by Fotedar et al. [35] and Uti et al. [36]. This answer was chosen by 73.5% of dentists and 83.3% of dental students. These data indicate a high level of consensus and alignment in the participants’ perceptions regarding the predominant type of oral cancer.
According to Öien et al. [37], an ulcer that does not heal is the first warning sign for the diagnosis of the pathology, which is in line with the results of this research, where the vast majority of respondents said that a lesion that progressed for more than 2 weeks and did not respond to treatment is one of the characteristics with the most significant potential for malignization. Dentists and students also appear to be primarily aware of the potential for malignancy in red and/or white lesions, as well as those that are ulcerated or easily bleed when touched.
The distinctions between practicing dentists and dental students concerning their knowledge and attitudes toward oral cancer are critical for formulating effective educational strategies aimed at improving early diagnosis and prevention. Evidence suggests that dental students often exhibit a heightened awareness of oral cancer, stemming from more recent training curricula, compared to their practicing counterparts, who demonstrate variability in knowledge due to the practical experiences they have accrued over time. A study by Tunç et al. [38] highlights that while practicing dentists generally possess a foundational understanding of the risk factors associated with oral cancer, their engagement with new research findings or comprehensive screening procedures still lags. Similarly, Jafer et al. [39] found that dental students exhibited a more positive attitude toward oral cancer awareness compared to dentists, who were identified to engage less in screening practices and patient education regarding risk factors. This discrepancy underscores the importance of ongoing education, particularly for practicing dentists who may not have kept their knowledge up to date to align with the current oral cancer screening protocols.
In terms of clinical practice, professionals and students are expected to conduct thorough intraoral examinations, including the evaluation of critical areas such as mucous membranes, the tongue, palate, and floor of the mouth. However, Jafer et al. [40] elucidate that dentists often perform incomplete examinations, which can result in missed diagnoses of potentially malignant disorders. This finding corroborates Fanaras and Warnakulasuriya’s assertion [41] that early detection is vital in improving prognosis, particularly when dental practitioners consistently perform comprehensive examinations.
To cultivate robust preventive practices and improve the early detection of oral cancer, advancing education and awareness at earlier stages in dental training appears essential. This adjustment would ideally ensure that all dental healthcare providers are consistent in their evaluation methods and patient education concerning oral cancer risk factors, ultimately leading to improved patient outcomes.
When considering the data revealed, it can be seen that dentists and dental students share similar perceptions about the sites with the most significant potential for malignancy in the case of oral cancer. The tongue was the option most selected by both groups, with 71.6% of dentists and 84.4% of dental students naming it a site with a high potential for malignancy. Some authors agreed with these results [42]. Therefore, anatomically, oral cancer follows a “horseshoe” distribution pattern within the oral cavity, predominantly affecting high-risk sites such as the lateral borders of the tongue and the floor of the mouth. These areas are particularly vulnerable due to their thin, non-keratinized mucosa and greater exposure to carcinogenic substances, including tobacco and alcohol. However, in clinical evaluations, other critical regions such as the retromolar trigone may be underexamined or overlooked. This area, although less frequently involved, is of particular concern due to its proximity to vital structures and its potential for deep tissue invasion, often contributing to poorer prognoses when malignancy occurs.
Furthermore, it is essential to recognize that oral cancer also includes malignancies of the lips, especially the lower lip, which is more exposed to ultraviolet radiation and may present with distinctive etiological and clinical characteristics. Comprehensive oral cancer screening should therefore encompass all sites within the oral cavity, with careful attention to those that may be less visible or routinely neglected during examination. It is estimated that the accuracy of conventional oral examination for malignant-only lesions is 88% for sensitivity and 81% for specificity. The diagnostic accuracy of different types of dental professionals in identifying dysplastic or malignant lesions exhibits high variation, resulting in varying estimates of sensitivity and specificity [43].
Regarding the lesions with the most significant potential for malignancy, most participants (68.6% of dentists and 67.8% of dental students) identified leukoplakia as the primary lesion with the most significant potential for malignancy. In line with these data, the study by Kumar et al. [24] (Bangalore, India) also showed a high percentage of respondents who selected leukoplakia as one of the primary potentially malignant lesions (82%). Following leukoplakia in this study were erythroplakia (47.1% among dentists and 56.7% among dental students) and inverted smoker’s palate (33.3% among dentists and 72.2% among dental students). Hertrampf et al.’s study [25] also identified leukoplakia, erythroplakia, and erythroleukoplakia as the lesions with the greatest potential for malignancy.
In line with the literature, most of the participants identified tobacco and alcohol as the main risk factors for oral cancer. Indeed, excessive alcohol consumption and smoking not only increase the possibility of developing oral cancer but also reduce the chances of recovering from the disease. Making patients aware of this relationship is essential to promoting prevention and adopting a healthy lifestyle.
Almost all participants in this study (94.7%) reported being accustomed to inspecting the mucous membranes, tongue, palate, and retromolar region during intraoral examinations. A lower percentage (37%) was found by Kumar et al. [24]. With similar results, although with slightly lower percentages, 71.8% of the study participants reported palpating the nodules of the head and neck during the extraoral examination. However, regarding educating patients about oral self-examination, a similar number of participants said they did and did not do it (33.8%). A slightly lower percentage showed that they only do it for at-risk patients (32.4%). Given these discouraging results, this habit of educating patients to self-examine the oral cavity should still be implemented in university clinical practice.
Unfortunately, around 36.3% of dentists only consider their ability to make a clinical diagnosis of a potentially malignant lesion and/or oral cancer to be “reasonable”, and 29.4% are not at all comfortable carrying out this task. In contrast to this study, in the Italian study by Colella et al. [44], the majority of participants (64.8%) felt comfortable making a diagnosis of potentially malignant lesions and/or oral cancer. Regarding the group of students, the majority (55.6%) rated their ability as “reasonable”, consistent with the findings of Sheriff and Santhanam [45].
Regarding the limitations of this study, the demographic skew toward younger, female, and Portuguese participants limited the generalizability of the findings to other age groups, genders, and national contexts. Future studies are recommended to evaluate the effectiveness of changes or targeted training using longitudinal or interventional designs.
5. Conclusions
Given the increasing prevalence of oral cancer, the recognition of this pathology with the aim of early diagnosis is fundamental to reducing mortality and morbidity rates. High-risk oral HPV types are covered in the new nine-valent HPV vaccine; most are found in the oral cavity as well and are high-risk for oral cancer. The results of this study demonstrate that both dental students and practicing dentists possess a sound understanding of key epidemiological aspects, such as the gender and age group most commonly affected, and correctly identify carcinoma as the most prevalent form of oral cancer. The tongue and floor of the mouth were appropriately recognized as the sites with the highest malignant potential, and lesions persisting for more than two weeks without responding to treatment were identified as significant indicators of malignancy.
Author Contributions
Conceptualization, M.M.S., L.M.V., T.M., N.V. and P.C.; methodology, M.M.S., L.M.V., T.M., N.V., J.C.H.F., G.V.O.F. and P.C.; software, M.M.S., L.M.V. and T.M.; validation, T.M., N.V., J.C.H.F., G.V.O.F. and P.C.; formal analysis, M.M.S., L.M.V., T.M., N.V., J.C.H.F., G.V.O.F., and P.C.; investigation, M.M.S., L.M.V., T.M., N.V., J.C.H.F., G.V.O.F. and P.C.; resources, M.M.S., L.M.V., T.M., N.V., J.C.H.F., G.V.O.F. and P.C.; data curation, M.M.S., L.M.V., T.M., N.V., J.C.H.F., G.V.O.F. and P.C.; writing—original draft preparation, M.M.S., L.M.V., T.M., N.V., J.C.H.F., G.V.O.F. and P.C.; writing—review and editing, M.M.S., L.M.V., T.M., N.V., J.C.H.F., G.V.O.F. and P.C.; visualization, M.M.S., L.M.V., T.M., N.V., J.C.H.F., G.V.O.F. and P.C.; supervision, T.M., N.V. and P.C.; project administration, T.M., M.M.S. and P.C.; funding acquisition. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki. It was approved by the Institutional Ethics Committee of Universidade Católica Portuguesa (no. 227/2022) on 3 October 2022.
Informed Consent Statement
Informed consent was obtained from the subjects involved in this study.
Data Availability Statement
All data were included in the article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Kumar, M.; Nanavati, R.; Modi, T.G.; Dobariya, C. Oral cancer: Etiology and risk factors: A review. J. Cancer Res. Ther. 2016, 12, 458–463. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Rivera, C. Essentials of oral cancer. Int. J. Clin. Exp. Pathol. 2015, 8, 11884–11894. [Google Scholar] [PubMed]
- Neville, B.W.; Day, T.A. Oral cancer and precancerous lesions. CA Cancer J. Clin. 2002, 52, 195–215. [Google Scholar] [CrossRef] [PubMed]
- Sarode, S.C.; Sarode, G.S.; Karmarkar, S. Early detection of oral cancer: Detector lies within. Oral Oncol. 2012, 48, 193194. [Google Scholar] [CrossRef] [PubMed]
- Porter, S.; Gueiros, L.A.; Leão, J.C.; Fedele, S. Risk factors and etiopathogenesis of potentially premalignant oral epithelial lesions. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Ali, J.; Sabiha, B.; Jan, H.U.; Haider, S.A.; Khan, A.A.; Ali, S.S. Genetic etiology of oral cancer. Oral Oncol. 2017, 70, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Zygogianni, A.G.; Kyrgias, G.; Karakitsos, P.; Psyrri, A.; Kouvaris, J.; Kelekis, N.; Kouloulias, V. Oral squamous cell cancer: Early detection and the role of alcohol and smoking. Head Neck Oncol. 2011, 3, 2. [Google Scholar] [CrossRef] [PubMed]
- Herrero, R.; Castellsagué, X.; Pawlita, M.; Lissowska, J.; Kee, F.; Balaram, P.; Rajkumar, T.; Sridhar, H.; Rose, B.; Pintos, J. Human papillomavirus and oral cancer: The International Agency for Research on Cancer multicenter study. J. Natl. Cancer Inst. 2003, 95, 1772–1783. [Google Scholar] [CrossRef] [PubMed]
- Scully, C.; Porter, S. ABC of oral health. Oral Cancer BMJ. 2000, 321, 97–100. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Baykul, T.; Yilmaz, H.H.; Aydin, U.; Aydin, M.A.; Aksoy, M.; Yildirim, D. Early diagnosis of oral cancer. J. Int. Med. Res. 2010, 38, 737–749. [Google Scholar] [CrossRef] [PubMed]
- Warnakulasuriya, S.; Johnson, N.W.; van der Waal, I. Nomenclature and classification of potentially malignant disorders of the oral mucosa. J. Oral Pathol. Med. 2007, 36, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Webster, J.D.; Batstone, M.; Farah, C.S. Missed opportunities for oral cancer screening in Australia. J. Oral Pathol. Med. 2019, 48, 595–603. [Google Scholar] [CrossRef] [PubMed]
- Stanley, R.J.; Stoecker, W.V.; Moss, R.H. A relative color approach to color discrimination for malignant melanoma detection in dermoscopy images. Skin Res. Technol. 2007, 13, 62–72. [Google Scholar] [CrossRef]
- Rader, R.K.; Payne, K.S.; Guntupalli, U.; Rabinovitz, H.; Oliviero, M.C.; Drugge, R.J.; Malters, J.J.; Stoecker, W.V. The pink rim sign: Location of pink as an indicator of melanoma in dermoscopic images. J. Skin Cancer 2014, 2014, 1–7. [Google Scholar] [CrossRef]
- Sagar, S.; Hiwale, K.; Gadkari, P.; Agrawal, A.K.; Naseri, S.; Khan, S. Beyond the norm: Navigating a unique papillary carcinoma journey in breast cancer. Cureus 2024, 16, e59795. [Google Scholar] [CrossRef]
- MacCarthy, D.; Flint, S.R.; Healy, C.; Stassen, L.F. Oral and neck examination for early detection of oral cancer—A practical guide. J. Ir. Dent. Assoc. 2011, 57, 195–199. [Google Scholar]
- Abati, S.; Bramati, C.; Bondi, S.; Lissoni, A.; Trimarchi, M. Oral Cancer and Precancer: A Narrative Review on the Relevance of Early Diagnosis. Int. J. Environ. Res. Public. Health 2020, 17, 9160. [Google Scholar] [CrossRef] [PubMed]
- Joseph, B.K. Oral cancer: Prevention and detection. Med. Princ. Pract. 2002, 11, 32–35. [Google Scholar] [CrossRef] [PubMed]
- Silverman, S., Jr.; Kerr, A.R.; Epstein, J.B. Oral and pharyngeal cancer control and early detection. J. Cancer Educ. 2010, 25, 279–281. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, L.M.; Aiden, L.E.; Wiggins, J.S.; Pincus, A.L. Inventory of Interpersonal Problems Manual; The Psychological Corporation: Odessa, FL, USA, 2000. [Google Scholar]
- Bhattacharjee, T.; Kerketa, M.; Babu, N. Differences of oral cancer in men and women of west bengal, india. J. Oral. Maxillofac. Pathol. 2021, 25, 200. [Google Scholar] [CrossRef] [PubMed]
- Shigeishi, H.; Sugiyama, M. Risk factors for oral human papillomavirus infection in healthy individuals: A systematic review and meta-analysis. J. Clin. Med. Res. 2016, 8, 721–729. [Google Scholar] [CrossRef] [PubMed]
- Kumar, K.V.V.; Suresan, V. Knowledge, attitude and screening practices of general dentists concerning oral cancer in Bangalore city. Indian J. Cancer 2012, 49, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Hertrampf, K.; Wenz, H.J.; Koller, M.; Grund, S.; Wiltfang, J. The oral cancer knowledge of dentists in Northern Germany after educational intervention. Eur. J. Cancer Prev. 2011, 20, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Decuseara, G.; MacCarthy, D.; Menezes, G. Oral cancer: Knowledge, practices and opinions of dentists in Ireland. J. Ir. Dent. Assoc. 2011, 57, 209–214. [Google Scholar] [PubMed]
- Bauluck-Nujoo, B.; Singh, S. Self-reported oral health status: Perspectives of patients undergoing therapy for cancer of the head and neck region, in the ethekwini district, KZN. South Afr. Dent. J. 2022, 77, 600–607. [Google Scholar] [CrossRef]
- Dhanuthai, K.; Rojanawatsirivej, S.; Thosaporn, W.; Kintarak, S.; Subarnbhesaj, A.; Darling, M.; Kryshtalskyj, E.; Chiang, C.-P.; Shin, H.-I.; Choi, S.-Y.; et al. Oral cancer: A multicenter study. Medicina Oral Patol. Oral Cir. Bucal 2018, 23, e23–e29. [Google Scholar] [CrossRef]
- Zhang, J.; Gao, F.; Yang, A.; Chen, W.; Chen, S.; Li, H.; Zhang, X.; Yang, Z.-Y.; Chen, X.-L.; Song, M. Epidemiologic characteristics of oral cancer: Single-center analysis of 4097 patients from the sun yat-sen university cancer center. Chin. J. Cancer. 2016, 35, 24. [Google Scholar] [CrossRef]
- Ashat, M.; Puri, S.; Pandey, A.; Goel, N.; Singh, A.; Kaushal, V. Socio-demographic characteristics of cancer patients: Hospital based cancer registry in a tertiary care hospital of india. Ind. J. Cancer 2014, 51, 1. [Google Scholar] [CrossRef]
- Mello, F.; Miguel, A.; Dutra, K.; Porporatti, A.; Warnakulasuriya, S.; Guerra, E.; Rivero, E. Prevalence of oral potentially malignant disorders: A systematic review and meta-analysis. J. Oral Pathol. Med. 2018, 47, 633–640. [Google Scholar] [CrossRef]
- Ahmad, W.M.A.W.; Ghazali, F.M.M.; Yaqoob, M.A.; Alawthah, G.H.; Srivastava, K.C.; Shrivastava, D.; Alam, M.K. A comprehensive cross-tabulation analysis of oral carcinoma patients. J. Pharm. Bioallied. Sci. 2021, 13 (Suppl. S2), S1074–S1078. [Google Scholar] [CrossRef] [PubMed]
- Nath, A.; Priyanka, P.; Singh, J.K.; Singh, S.; Jain, P.; Sardhana, M.; Kumar, A.; Ranjan, S.K.; Singh, M.K. High level of estrogen in male oral cancer patients and consumption of smokeless tobacco. J. Ecophysiol. Occupat. Health 2014, 14, 159–164. [Google Scholar] [CrossRef][Green Version]
- Silva, S.R.J.Y.; Novo, N.F.; Weinfeld, I. Comparative study of knowledge about oral cancer among undergraduate dental students. Einstein 2016, 14, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Fotedar, S.; Bhardwaj, V.; Manchanda, K.; Fotedar, V.; Sarkar, A.; Sood, N. Knowledge, attitude and practices about oral cancers among dental students in HP Government Dental College, Shimla, Himachal Pradesh. South. Asian J. Cancer 2015, 4, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Uti, O.G.; Fashina, A.A. Oral cancer education in dental schools: Knowledge and experience of Nigerian undergraduate students. J. Dent. Educ. 2006, 70, 676–680. [Google Scholar] [CrossRef] [PubMed]
- Öien, R.; Roxenius, J.; Boström, M.; Wickström, H. Management and outcomes among patients with hard-to-heal ulcers in sweden: A national mapping of data from medical records, focusing on diagnoses, ulcer healing, ulcer treatment time, pain and prescription of analgesics and antibiotics. BMJ Open 2024, 14, e087894. [Google Scholar] [CrossRef] [PubMed]
- Tunç, S.; Toprak, M.; Yüce, E.; Efe, N.; Topbaş, C. Comparison of knowledge, awareness, and behaviors toward oral cancer among dental students and dentists: An online cross-sectional questionnaire in Türkiye. BMC Oral Health 2024, 24, 502. [Google Scholar] [CrossRef]
- Jafer, M.; Crutzen, R.; Moafa, I.; Borne, B. What do dentists and dental students think of oral cancer and its control and prevention strategies? a qualitative study in jazan dental school. J. Cancer Educ. 2019, 36, 134–142. [Google Scholar] [CrossRef]
- Jafer, M.; Crutzen, R.; Halboub, E.; Moafa, I.; Borne, B.; Bajonaid, A.; Jafer, A.; Hedad, I. Dentists behavioral factors influencing early detection of oral cancer: Direct clinical observational study. J. Cancer Educ. 2022, 37, 932–941. [Google Scholar] [CrossRef]
- Fanaras, N.; Warnakulasuriya, S. Oral cancer diagnosis in primary care. Prim. Dent. J. 2016, 5, 64–68. [Google Scholar] [CrossRef]
- Li, H.; Guo, L.; Chen, S.W.; Zhao, X.H.; Zhuang, S.M.; Wang, L.P.; Song, L.B.; Song, M. GOLPH3 overexpression correlates with tumor progression and poor prognosis in patients with clinically N0 oral tongue cancer. J. Transl. Med. 2012, 10, 168. [Google Scholar] [CrossRef] [PubMed]
- Essat, M.; Cooper, K.; Bessey, A.; Clowes, M.; Chilcott, J.B.; Hunter, K.D. Diagnostic accuracy of conventional oral examination for detecting oral cavity cancer and potentially malignant disorders in patients with clinically evident oral lesions: Systematic review and meta-analysis. Head Neck 2022, 44, 998–1013. [Google Scholar] [CrossRef] [PubMed]
- Colella, G.; Gaeta, G.M.; Moscariello, A.; Angelillo, I.F. Oral cancer and dentists: Knowledge, attitudes, and practices in Italy. Oral Oncol. 2008, 44, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, B.; Subedi, S. Knowledge, Attitude and Practice of Oral Biopsy Procedures among Dental Surgeons Registered with Nepal Dental Association. J. Nepal Health Res. Counc. 2020, 18, 70–74. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).