
Low-Grade Myofibroblastic Sarcoma in the Oral Cavity: Case Report and Clinical Insights


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
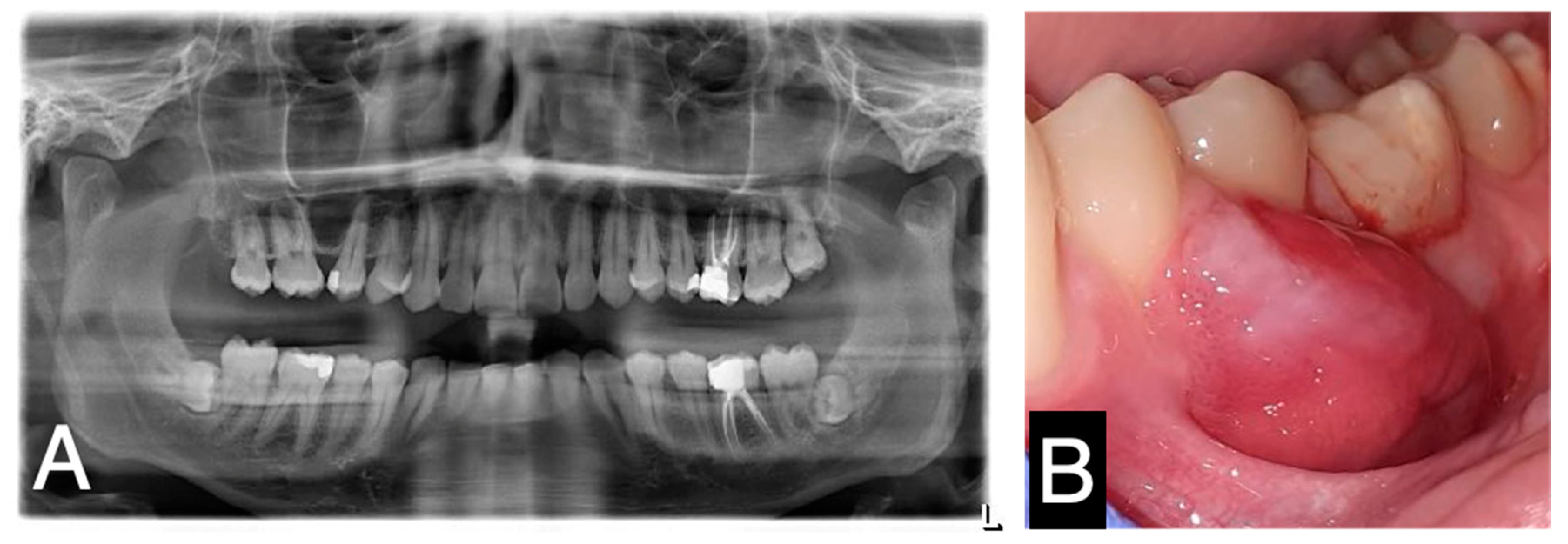
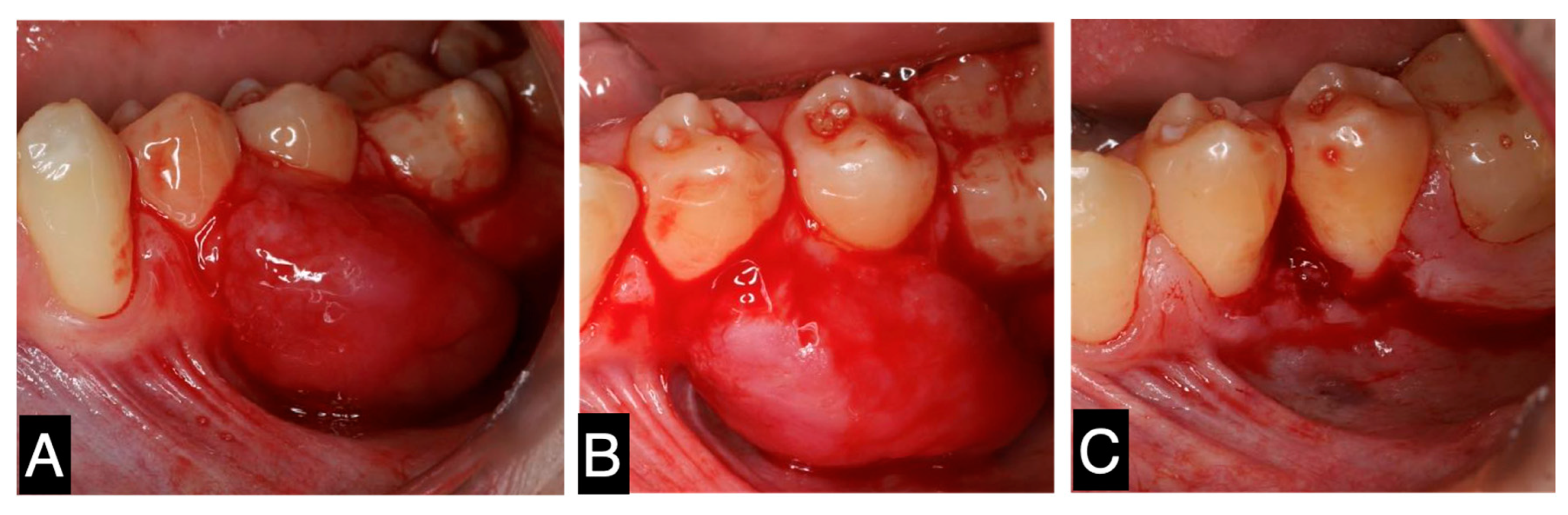
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gómez-Oliveira, G.; Arribas-García, I.; Serrano Alvarez-Buylla, A.; Sánchez-Burgos, R.; Martínez-Pérez, F.; Alvarez-Flores, M. Low-grade myofibroblastic sarcoma. Two rare tumors in two rare locations. Rev. Española Cirugía Oral Maxilofacial 2015, 37, 108–112. [Google Scholar] [CrossRef]
- Wang, L.; Li, L.X.; Chen, D.Q.; Yang, L.; Li, S.K.; Cheng, C. Low-grade Myofibroblastic sarcoma: Clinical and imaging findings. BMC Med. Imaging 2019, 19, 1471–2342. [Google Scholar] [CrossRef] [PubMed]
- Jayasooriya, P.R.; Athukorala, C.; Attygalla, M.; Mendis, B.; Lombardi, T. Low-Grade Myofibroblastic Sarcoma of the Oral Cavity: A Report of Three Cases Illustrating an Emerging Disease in Children. Dermatopathology 2021, 8, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, E.; Goldblum, J.R.; Fisher, C. Myofibrosarcoma: A clinicopathologic study. Am. J. Surg. Pathol. 2001, 25, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Cai, C.; Dehner, L.P.; El-Mofty, S.K. In myofibroblastic sarcomas of the head and neck, mitotic activity and necrosis define grade: A case study and literature review. Virchows Arch. 2013, 463, 827–836. [Google Scholar] [CrossRef]
- Giraldo-Roldan, D.; Louredo, B.V.R.; Penafort, P.V.M.; Pontes, H.A.R.; Alves, A.P.; Lima, F.C.A.; Fonseca, T.C.; Abrahão, A.C.; Romañach, M.J.; Fonseca, F.P.; et al. Low-Grade Myofibroblastic Sarcoma of the Oral and Maxillofacial Region: An International Clinicopathologic Study of 13 Cases and Literature Review. Head Neck Pathol. 2023, 17, 832–850. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, A.; Bandopadhyay, A.; Sarkar, R. Low-grade myofibroblastic sarcoma of maxillary sinus and buccal mucosa: Two rare cases and review of the literature. Indian J. Pathol. Microbiol. 2019, 62, 119–121. [Google Scholar] [CrossRef]
- Demarosi, F.; Bay, A.; Moneghini, L.; Carrassi, A. Low-grade myofibroblastic sarcoma of the oral cavity. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 108, 248–254. [Google Scholar] [CrossRef]
- Schenker, A.; Gutjahr, E.A.-O.; Lehner, B.; Mechtersheimer, G.; Wardelmann, E.A.-O.; Klotz, R.A.-O.X.; Kalkum, E.; Schiltenwolf, M.; Harhaus, L.; Renkawitz, T.; et al. A Systematic Review and Illustrative Case Presentation of Low-Grade Myofibroblastic Sarcoma (LGMS) of the Extremities. J. Clin. Med. 2023, 12, 7027. [Google Scholar] [CrossRef]
- Feng, Y.; Du, Y.; Li, M.; Jia, G.; Gong, L.; Li, L. Low-Grade malignant myofibroblastic sarcoma of the larynx: A case report. J. Int. Med. Res. 2023, 51, 3000605231193929. [Google Scholar] [CrossRef] [PubMed]
- Padmawar, N.S.; Bhadange, S.; Mustilwar, R.G.; Mopagar, V.P.; Vadvadgi, V.H.; Joshi, S.R. Aberrant Location of Low-Grade Myofibroblastic Sarcoma of the Gingiva in Posterior Maxilla. Int. J. Clin. Pediatr. Dent. 2021, 14, 816–819. [Google Scholar] [CrossRef] [PubMed]
- Coyne, J.D. Low-grade myofibroblastic sarcoma of the piriform fossa: A case report with a literature review of a tumour with a predilection for the head and neck. Br. J. Oral Maxillofac. Surg. 2007, 45, 335–337. [Google Scholar] [CrossRef] [PubMed]
- Mentzel, T.; Dry, S.; Katenkamp, D.; Christopher, F. Low-grade myofibroblastic sarcoma: Analysis of 18 cases in the spectrum of myofibroblastic tumors. Am. J. Surg. Pathol. 1998, 22, 1228–1238. [Google Scholar] [CrossRef] [PubMed]
- Fisher, C. Myofibrosarcoma. Virchows Arch. 2004, 445, 215–223. [Google Scholar] [CrossRef]
- Magro, G. Differential Diagnosis of Benign Spindle Cell Lesions. Surg. Pathol. Clin. 2018, 11, 91–121. [Google Scholar] [CrossRef]
- Christopher, D.M.; Fletcher, K.K.U.; Mertens, F. Pathology and Genetics of Tumours of Soft Tissue and Bone; IARC Press: Lyon, France, 2002; pp. 94–95. [Google Scholar]
- Velez Torres, J.M.; Martinez Duarte, E.; Diaz-Perez, J.A.; Leibowitz, J.; Weed, D.T.; Thomas, G.; Civantos, F.J.; Arnold, D.J.; Gomez-Fernandez, C.; Rosenberg, A.E. Primary Sarcomas of the Larynx: A Clinicopathologic Study of 27 Cases. Head Neck Pathol. 2021, 15, 905–916. [Google Scholar] [CrossRef]
- Jay, A.; Piper, K.; Farthing, P.M.; Carter, J.; Diwakar, A. Low-grade myofibroblastic sarcoma of the tongue. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2007, 104, e52–e58. [Google Scholar] [CrossRef] [PubMed]
- Vlad, D.; Albu, S. Low-Grade Myofibroblastic Sarcoma of the Larynx. J. Craniofac. Surg. 2016, 27, e270–e271. [Google Scholar] [CrossRef] [PubMed]
- Kordač, P.; Nikolov, D.H.; Smatanová, K.; Kalfeřt, D. Low-Grade Myofibroblastic Sarcoma of the LARYNX: Case Report and Review of Literature. Acta Medica 2014, 57, 162–164. [Google Scholar] [CrossRef]
- Qiu, J.Y.; Liu, P.; Shi, C.; Han, B. Low-grade myofibroblastic sarcomas of the maxilla. Oncol. Lett. 2015, 9, 619–625. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Azevedo, M.; de Araújo, P.; Faria-Almeida, R.; Correia, F. Low-Grade Myofibroblastic Sarcoma in the Oral Cavity: Case Report and Clinical Insights. Oral 2025, 5, 6. https://doi.org/10.3390/oral5010006
Azevedo M, de Araújo P, Faria-Almeida R, Correia F. Low-Grade Myofibroblastic Sarcoma in the Oral Cavity: Case Report and Clinical Insights. Oral. 2025; 5(1):6. https://doi.org/10.3390/oral5010006
Chicago/Turabian StyleAzevedo, Mafalda, Paulo de Araújo, Ricardo Faria-Almeida, and Francisco Correia. 2025. "Low-Grade Myofibroblastic Sarcoma in the Oral Cavity: Case Report and Clinical Insights" Oral 5, no. 1: 6. https://doi.org/10.3390/oral5010006
APA StyleAzevedo, M., de Araújo, P., Faria-Almeida, R., & Correia, F. (2025). Low-Grade Myofibroblastic Sarcoma in the Oral Cavity: Case Report and Clinical Insights. Oral, 5(1), 6. https://doi.org/10.3390/oral5010006