
Lymphomas in People Living with HIV





Abstract
:1. Introduction
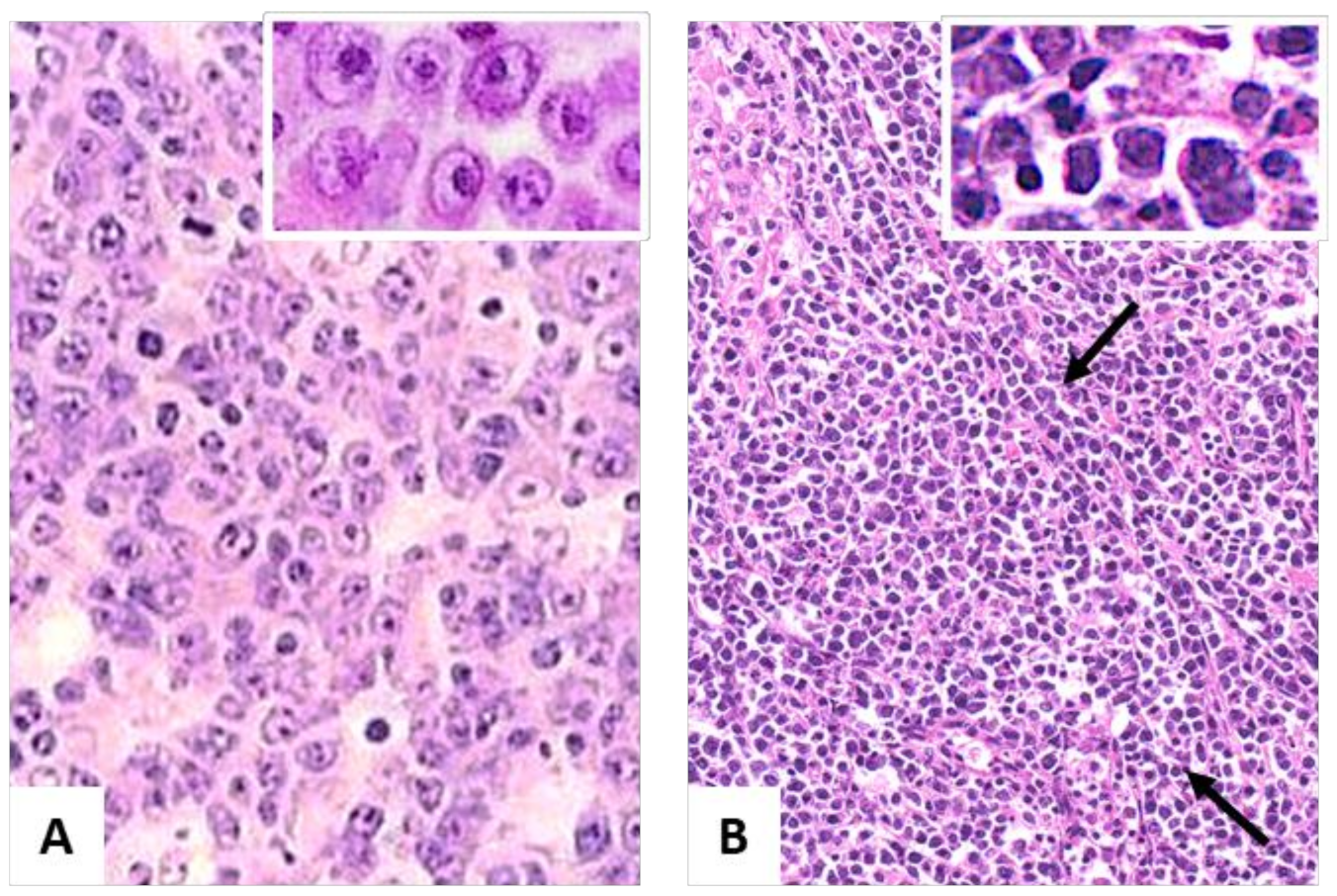
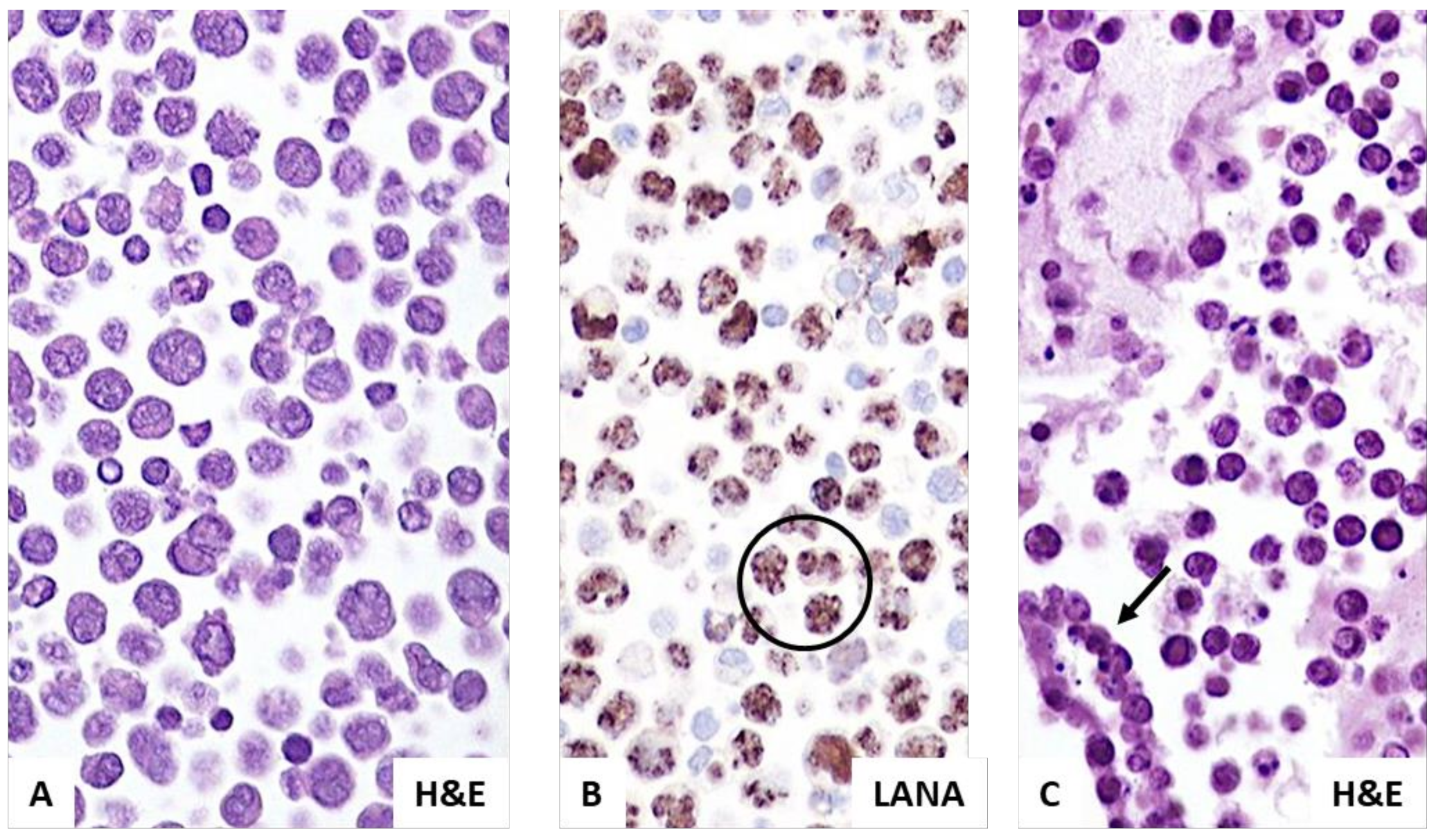
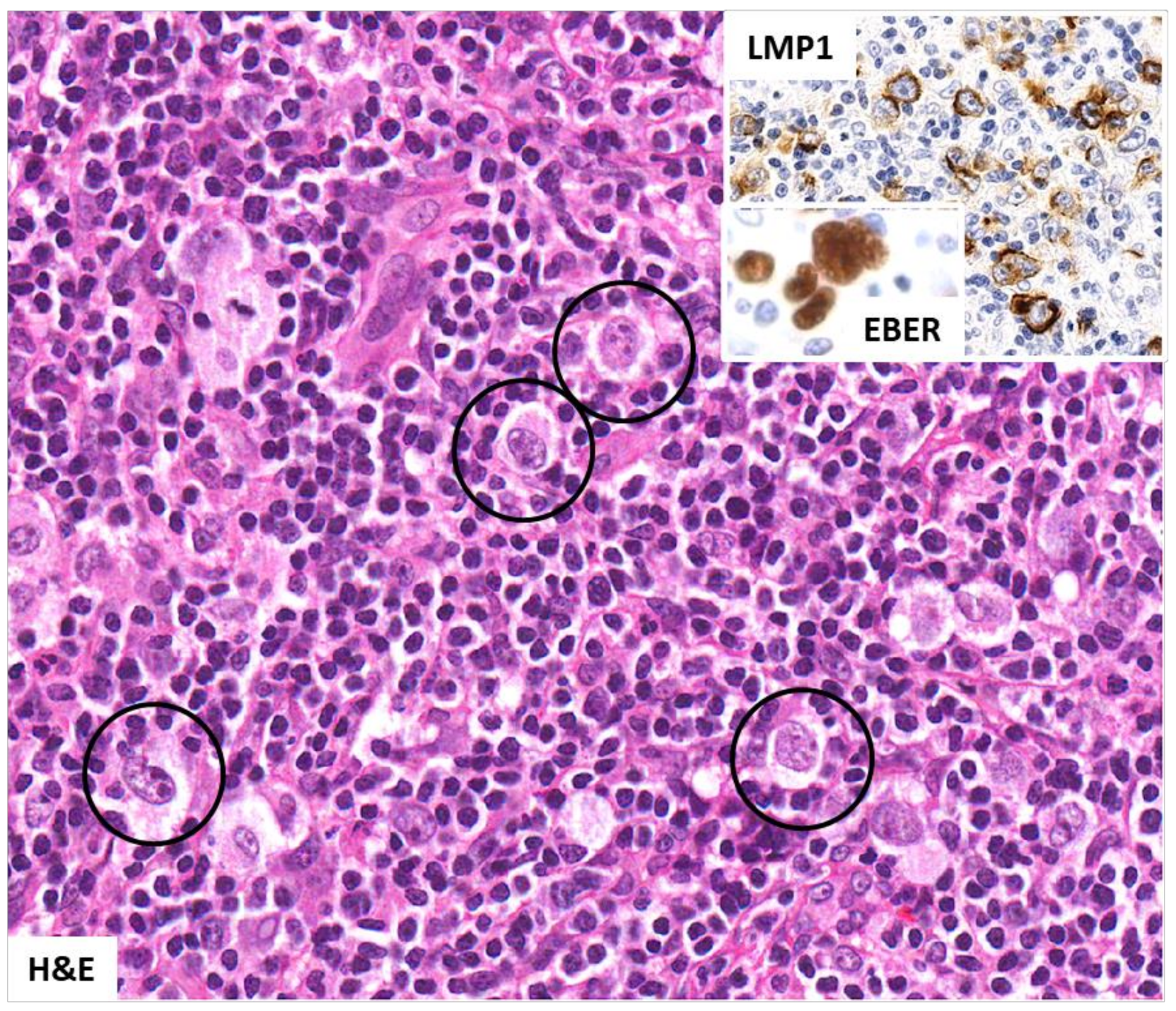
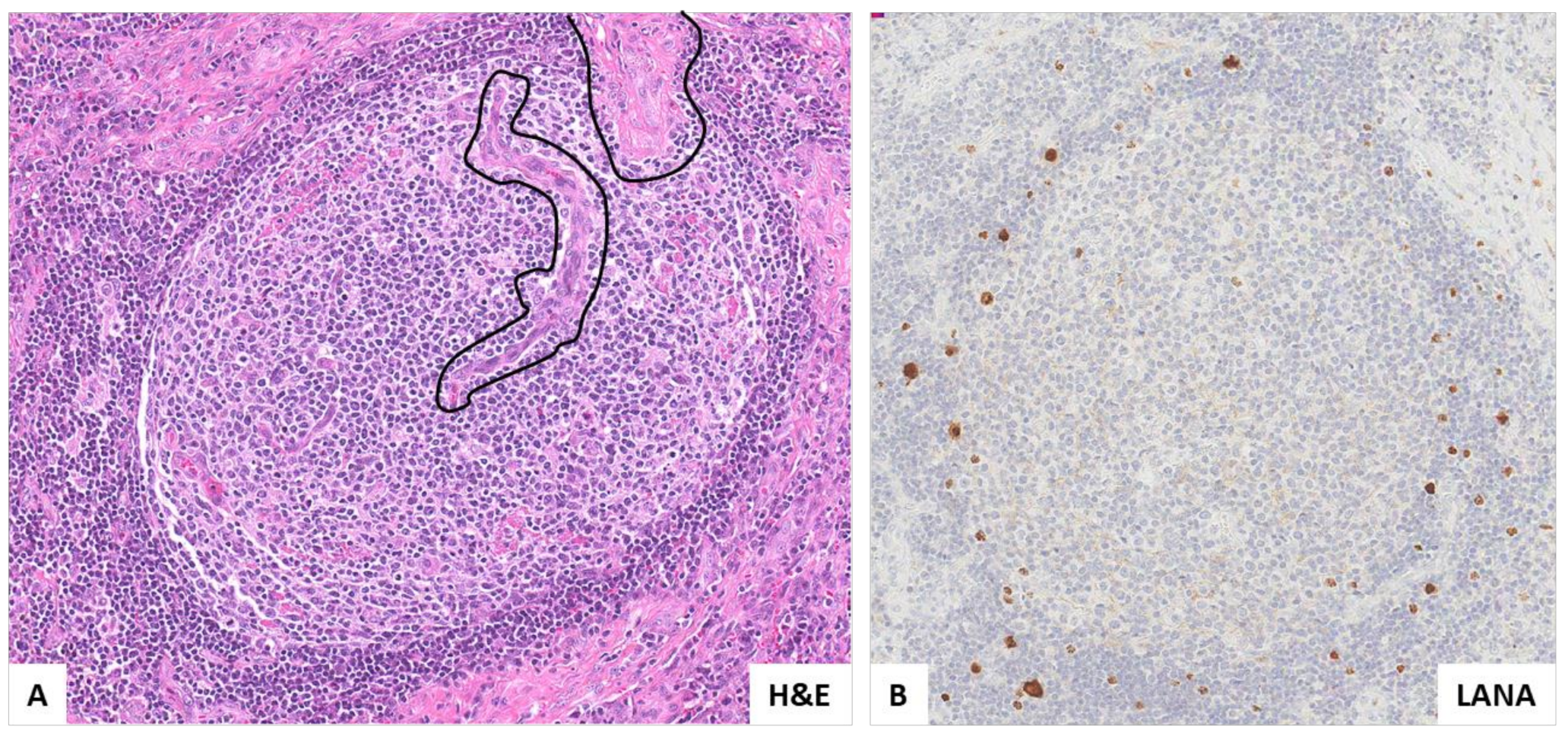
2. Pathologic and Virologic Features
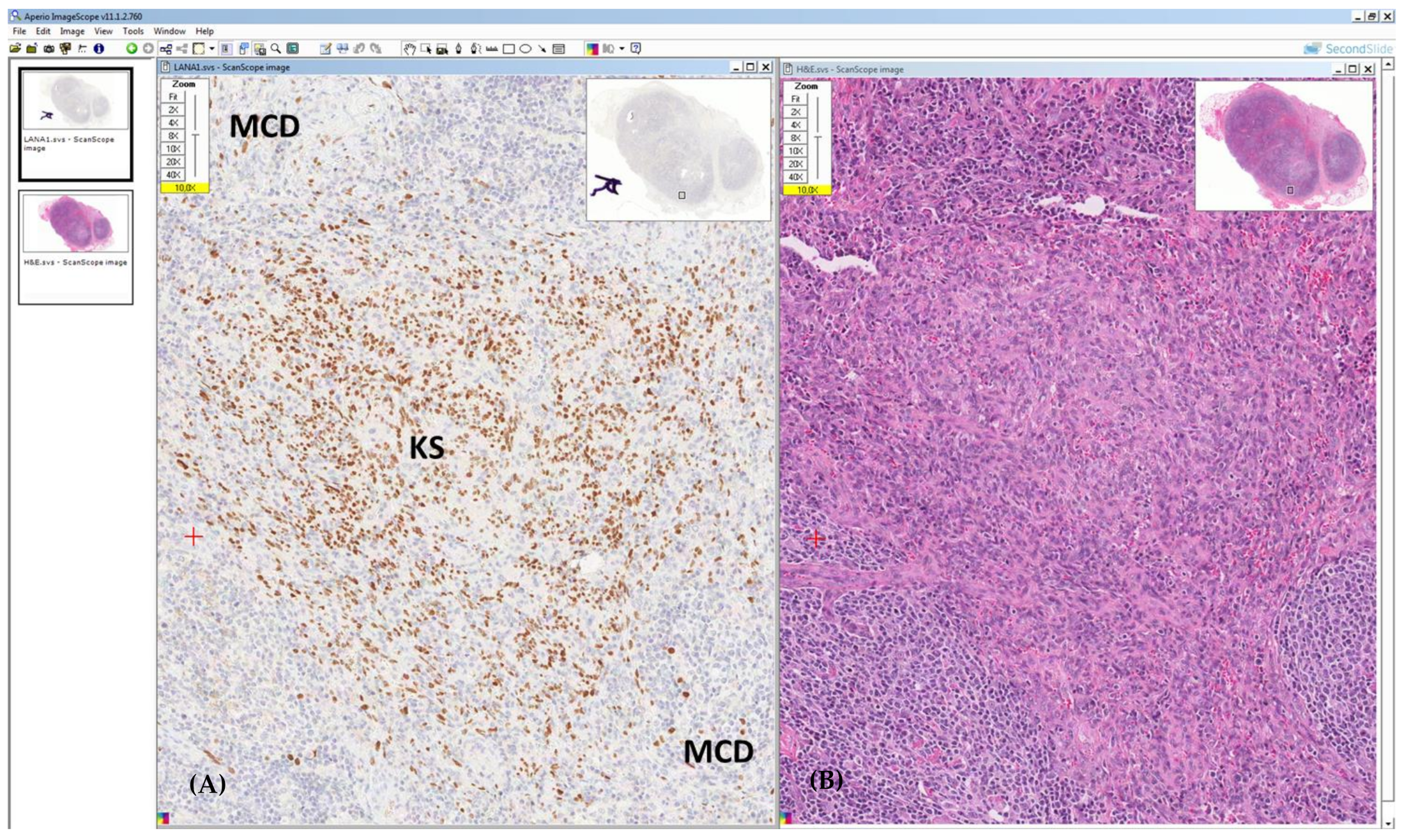
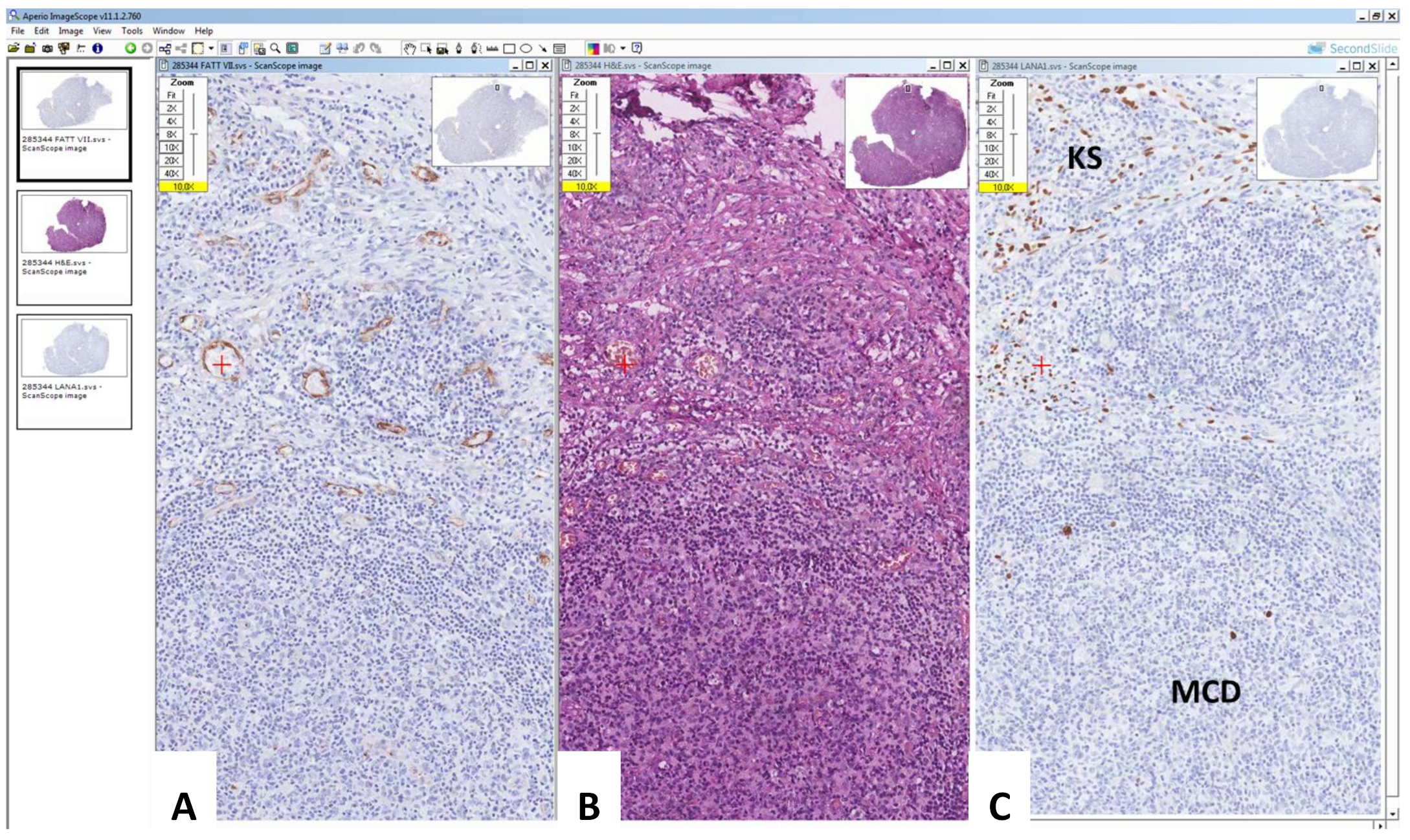
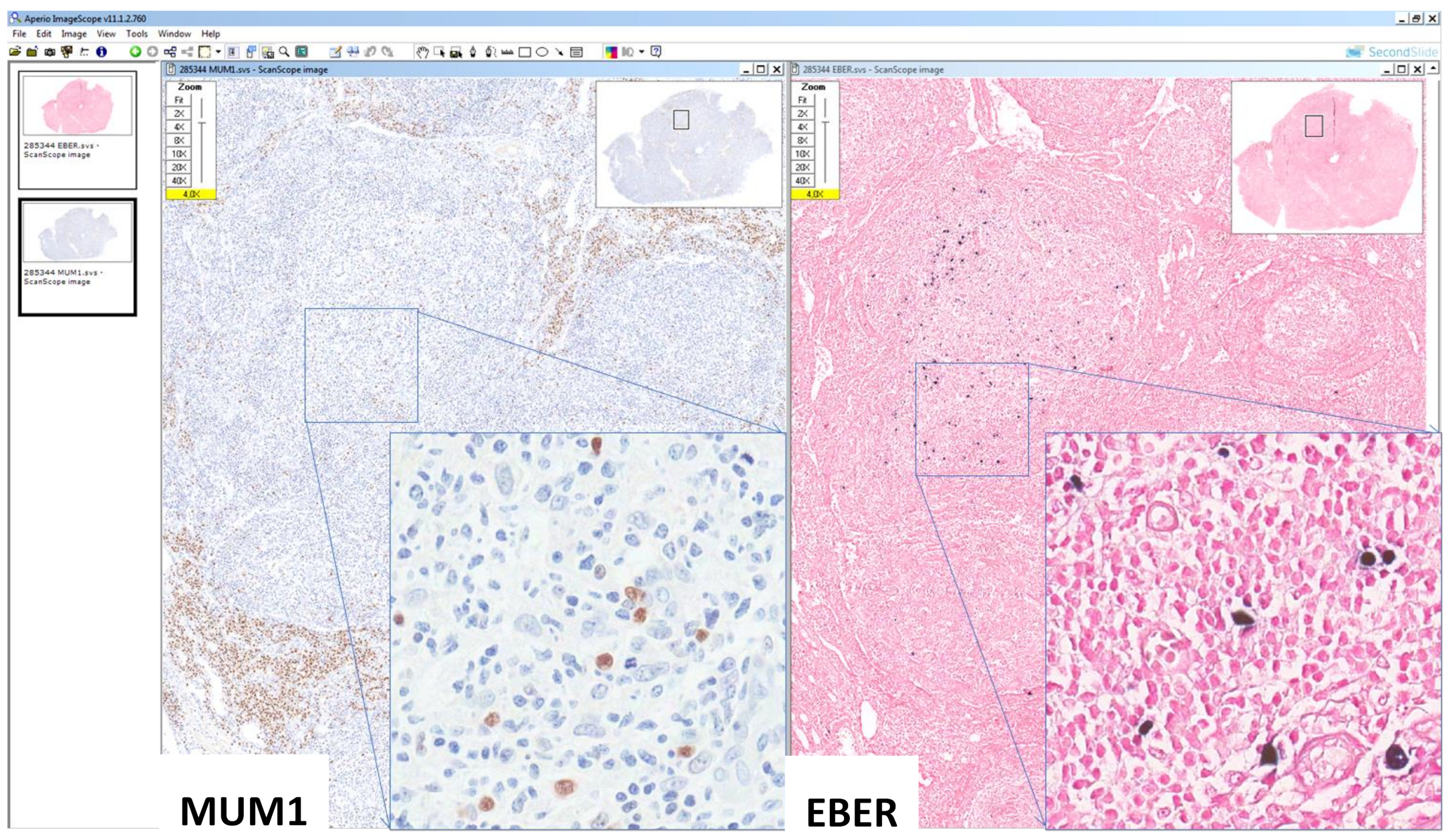
3. Simultaneous Occurrence of KSHV- and EBV-Associated Disorders in PLWH
4. Treatment Strategies
5. Front-Line Treatment for Non-Hodgkin Lymphoma
6. Treatment of Relapsed or Refractory Lymphoma
7. Hodgkin Lymphoma
8. Multicentric Castleman Disease
9. Preventive Measures
10. Concluding Remarks
Author Contributions
Funding
Institutional Review Board statement
Informed consent statement
Data availability statement
Conflicts of Interest
References
- Polesel, J.; Clifford, G.M.; Rickenbach, M.; Dal Maso, L.; Battegay, M.; Bouchardy, C.; Furrer, H.; Hasse, B.; Levi, F.; Probst-Hensch, N.M.; et al. Non-Hodgkin lymphoma incidence in the Swiss HIV Cohort Study before and after highly active antiretroviral therapy. AIDS 2008, 22, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Simard, E.P.; Pfeiffer, R.M.; Engels, E.A. Cumulative incidence of cancer among individuals with acquired immunodeficiency syndrome in the United States. Cancer 2011, 117, 1089–1096. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Jemal, A.; Hulland, E.; Simard, E.P.; Nastoupil, L.; Ward, E.; Flowers, C.R. HIV Infection and Survival of Lymphoma Patients in the Era of Highly Active Antiretroviral Therapy. Cancer Epidemiol. Biomark. Prev. 2017, 26, 303–311. [Google Scholar] [CrossRef]
- Carbone, A.; Vaccher, E.; Gloghini, A. Hematologic cancers in individuals infected by HIV. Blood 2022, 139, 995–1012. [Google Scholar] [CrossRef] [PubMed]
- Carbone, A.; Gloghini, A.; Serraino, D.; Spina, M.; Tirelli, U.; Vaccher, E. Immunodeficiency-associated Hodgkin lymphoma. Expert Rev. Hematol. 2021, 14, 547–559. [Google Scholar] [CrossRef]
- Cesarman, E.; Chadburn, A.; Rubinstein, P.G. KSHV/HHV8-mediated hematologic diseases. Blood 2022, 139, 1013–1025. [Google Scholar] [CrossRef]
- Toner, K.; Bollard, C.M. EBV+ lymphoproliferative diseases: Opportunities for leveraging EBV as a therapeutic target. Blood 2022, 139, 983–994. [Google Scholar] [CrossRef]
- Said, J.; Cesarman, E.; Rosenwald, A.; Harris, N. Lymphomas associated with HIV infection. In WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues; Swerdlow, S.H., Campo, E., Harris, N.L., Jaffe, E.S., Stein, H., Arber, D.A., Hasserjian, R.P., Beau, L., et al., Eds.; International Agency for Research on Cancer: Lyon, France, 2017; pp. 449–452. [Google Scholar]
- Bower, M.; Carbone, A. KSHV/HHV8-Associated Lymphoproliferative Disorders: Lessons Learnt from People Living with HIV. Hemato 2021, 2, 703–712. [Google Scholar] [CrossRef]
- Campo, E.; Jaffe, E.S.; Cook, J.R.; Quintanilla-Martinez, L.; Swerdlow, S.H.; Anderson, K.C.; Brousset, P.; Cerroni, L.; de Leval, L.; Dirnhofer, S.; et al. The International Consensus Classification of Mature Lymphoid Neoplasms: A Report from the Clinical Advisory Committee. Blood 2022. [Google Scholar] [CrossRef]
- Chen, X.; Jia, L.; Zhang, X.; Zhang, T.; Zhang, Y. One arrow for two targets: Potential co-treatment regimens for lymphoma and HIV. Blood Rev. 2022, 100965. [Google Scholar] [CrossRef]
- Carbone, A.; Borok, M.; Damania, B.; Gloghini, A.; Polizzotto, M.N.; Jayanthan, R.K.; Fajgenbaum, D.C.; Bower, M. Castleman disease. Nat. Rev. Dis. Primers 2021, 7, 84. [Google Scholar] [CrossRef] [PubMed]
- Carbone, A.; Vaccher, E.; Gloghini, A.; Pantanowitz, L.; Abayomi, A.; de Paoli, P.; Franceschi, S. Diagnosis and management of lymphomas and other cancers in HIV-infected patients. Nat. Rev. Clin. Oncol. 2014, 11, 223–238. [Google Scholar] [CrossRef] [PubMed]
- Du, M.Q.; Diss, T.C.; Liu, H.; Ye, H.; Hamoudi, R.A.; Cabeçadas, J.; Dong, H.Y.; Harris, N.L.; Chan, J.K.; Rees, J.W.; et al. KSHV- and EBV-associated germinotropic lymphoproliferative disorder. Blood 2002, 100, 3415–3418. [Google Scholar] [CrossRef] [PubMed]
- Natkunam, Y.; Gratzinger, D.; Chadburn, A.; Goodlad, J.R.; Chan, J.K.C.; Said, J.; Jaffe, E.S.; de Jong, D. Immunodeficiency-associated lymphoproliferative disorders: Time for reappraisal? Blood 2018, 132, 1871–1878. [Google Scholar] [CrossRef]
- Gopal, S.; Patel, M.R.; Yanik, E.L.; Cole, S.R.; Achenbach, C.J.; Napravnik, S.; Burkholder, G.A.; Reid, E.G.; Rodriguez, B.; Deeks, S.G.; et al. Temporal trends in presentation and survival for HIV-associated lymphoma in the antiretroviral therapy era. J. Natl. Cancer Inst. 2013, 105, 1221–1229. [Google Scholar] [CrossRef]
- Yarchoan, R.; Uldrick, T.S. HIV-Associated Cancers and Related Diseases. N. Engl. J. Med. 2018, 378, 1029–1041. [Google Scholar] [CrossRef]
- Noy, A. Optimizing treatment of HIV-associated lymphoma. Blood 2019, 134, 1385–1394. [Google Scholar] [CrossRef]
- Ramaswami, R.; Chia, G.; Dalla Pria, A.; Pinato, D.J.; Parker, K.; Nelson, M.; Bower, M. Evolution of HIV-Associated Lymphoma Over 3 Decades. J. Acquir. Immune Defic. Syndr. 2016, 72, 177–183. [Google Scholar] [CrossRef]
- Horner, M.J.; Shiels, M.S.; Pfeiffer, R.M.; Engels, E.A. Deaths Attributable to Cancer in the US Human Immunodeficiency Virus Population During 2001–2015. Clin. Infect. Dis. 2021, 72, e224–e231. [Google Scholar] [CrossRef]
- Olszewski, A.J.; Jakobsen, L.H.; Collins, G.P.; Cwynarski, K.; Bachanova, V.; Blum, K.A.; Boughan, K.M.; Bower, M.; Dalla Pria, A.; Danilov, A.; et al. Burkitt Lymphoma International Prognostic Index. J. Clin. Oncol. 2021, 39, 1129–1138. [Google Scholar] [CrossRef]
- Yarchoan, R.; Ramaswami, R.; Lurain, K. HIV-associated malignancies at 40: Much accomplished but much to do. Glob. Health Med. 2021, 3, 184–186. [Google Scholar] [CrossRef] [PubMed]
- Mukhtar, F.; Ilozumba, M.; Utuama, O.; Cimenler, O. Change in Pattern of Secondary Cancers After Kaposi Sarcoma in the Era of Antiretroviral Therapy. JAMA Oncol. 2018, 4, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Hessol, N.A.; Whittemore, H.; Vittinghoff, E.; Hsu, L.C.; Ma, D.; Scheer, S.; Schwarcz, S.K. Incidence of first and second primary cancers diagnosed among people with HIV, 1985-2013: A population-based, registry linkage study. Lancet HIV 2018, 5, e647–e655. [Google Scholar] [CrossRef]
- Mahale, P.; Ugoji, C.; Engels, E.A.; Shiels, M.S.; Peprah, S.; Morton, L.M. Cancer risk following lymphoid malignancies among HIV-infected people. AIDS 2020, 34, 1237–1245. [Google Scholar] [CrossRef]
- Abrahão, R.; Li, Q.W.; Malogolowkin, M.H.; Alvarez, E.M.; Ribeiro, R.C.; Wun, T.; Keegan, T.H.M. Chronic medical conditions and late effects following non-Hodgkin lymphoma in HIV-uninfected and HIV-infected adolescents and young adults: A population-based study. Br. J. Haematol. 2020, 190, 371–384. [Google Scholar] [CrossRef]
- Poizot-Martin, I.; Lions, C.; Delpierre, C.; Makinson, A.; Allavena, C.; Fresard, A.; Brégigeon, S.; Rojas Rojas, T.; Delobel, P.; Group The Dat, A.S. Prevalence and Spectrum of Second Primary Malignancies among People Living with HIV in the French Dat’AIDS Cohort. Cancers 2022, 14, 401. [Google Scholar] [CrossRef]
- Kaplan, L.D.; Lee, J.Y.; Ambinder, R.F.; Sparano, J.A.; Cesarman, E.; Chadburn, A.; Levine, A.M.; Scadden, D.T. Rituximab does not improve clinical outcome in a randomized phase 3 trial of CHOP with or without rituximab in patients with HIV-associated non-Hodgkin lymphoma: AIDS-Malignancies Consortium Trial 010. Blood 2005, 106, 1538–1543. [Google Scholar] [CrossRef]
- Sparano, J.A.; Lee, J.Y.; Kaplan, L.D.; Levine, A.M.; Ramos, J.C.; Ambinder, R.F.; Wachsman, W.; Aboulafia, D.; Noy, A.; Henry, D.H.; et al. Rituximab plus concurrent infusional EPOCH chemotherapy is highly effective in HIV-associated B-cell non-Hodgkin lymphoma. Blood 2010, 115, 3008–3016. [Google Scholar] [CrossRef]
- Dunleavy, K.; Little, R.F.; Pittaluga, S.; Grant, N.; Wayne, A.S.; Carrasquillo, J.A.; Steinberg, S.M.; Yarchoan, R.; Jaffe, E.S.; Wilson, W.H. The role of tumor histogenesis, FDG-PET, and short-course EPOCH with dose-dense rituximab (SC-EPOCH-RR) in HIV-associated diffuse large B-cell lymphoma. Blood 2010, 115, 3017–3024. [Google Scholar] [CrossRef]
- Boué, F.; Gabarre, J.; Gisselbrecht, C.; Reynes, J.; Cheret, A.; Bonnet, F.; Billaud, E.; Raphael, M.; Lancar, R.; Costagliola, D. Phase II trial of CHOP plus rituximab in patients with HIV-associated non-Hodgkin’s lymphoma. J. Clin. Oncol. 2006, 24, 4123–4128. [Google Scholar] [CrossRef]
- Ribera, J.M.; Oriol, A.; Morgades, M.; González-Barca, E.; Miralles, P.; López-Guillermo, A.; Gardella, S.; López, A.; Abella, E.; García, M. Safety and efficacy of cyclophosphamide, adriamycin, vincristine, prednisone and rituximab in patients with human immunodeficiency virus-associated diffuse large B-cell lymphoma: Results of a phase II trial. Br. J. Haematol. 2008, 140, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Spina, M.; Jaeger, U.; Sparano, J.A.; Talamini, R.; Simonelli, C.; Michieli, M.; Rossi, G.; Nigra, E.; Berretta, M.; Cattaneo, C.; et al. Rituximab plus infusional cyclophosphamide, doxorubicin, and etoposide in HIV-associated non-Hodgkin lymphoma: Pooled results from 3 phase 2 trials. Blood 2005, 105, 1891–1897. [Google Scholar] [CrossRef] [PubMed]
- Ramos, J.C.; Sparano, J.A.; Chadburn, A.; Reid, E.G.; Ambinder, R.F.; Siegel, E.R.; Moore, P.C.; Rubinstein, P.G.; Durand, C.M.; Cesarman, E.; et al. Impact of Myc in HIV-associated non-Hodgkin lymphomas treated with EPOCH and outcomes with vorinostat (AMC-075 trial). Blood 2020, 136, 1284–1297. [Google Scholar] [CrossRef] [PubMed]
- Barta, S.K.; Xue, X.; Wang, D.; Tamari, R.; Lee, J.Y.; Mounier, N.; Kaplan, L.D.; Ribera, J.M.; Spina, M.; Tirelli, U.; et al. Treatment factors affecting outcomes in HIV-associated non-Hodgkin lymphomas: A pooled analysis of 1546 patients. Blood 2013, 122, 3251–3262. [Google Scholar] [CrossRef]
- Bartlett, N.L.; Wilson, W.H.; Jung, S.H.; Hsi, E.D.; Maurer, M.J.; Pederson, L.D.; Polley, M.C.; Pitcher, B.N.; Cheson, B.D.; Kahl, B.S.; et al. Dose-Adjusted EPOCH-R Compared With R-CHOP as Frontline Therapy for Diffuse Large B-Cell Lymphoma: Clinical Outcomes of the Phase III Intergroup Trial Alliance/CALGB 50303. J. Clin. Oncol. 2019, 37, 1790–1799. [Google Scholar] [CrossRef]
- Ramos, J.C.; Sparano, J.A.; Rudek, M.A.; Moore, P.C.; Cesarman, E.; Reid, E.G.; Henry, D.; Ratner, L.; Aboulafia, D.; Lee, J.Y.; et al. Safety and Preliminary Efficacy of Vorinostat With R-EPOCH in High-risk HIV-associated Non-Hodgkin’s Lymphoma (AMC-075). Clin. Lymphoma Myeloma Leuk. 2018, 18, 180–190.e182. [Google Scholar] [CrossRef]
- Dunleavy, K.; Pittaluga, S.; Shovlin, M.; Steinberg, S.M.; Cole, D.; Grant, C.; Widemann, B.; Staudt, L.M.; Jaffe, E.S.; Little, R.F.; et al. Low-intensity therapy in adults with Burkitt’s lymphoma. N. Engl. J. Med. 2013, 369, 1915–1925. [Google Scholar] [CrossRef]
- Roschewski, M.; Dunleavy, K.; Abramson, J.S.; Powell, B.L.; Link, B.K.; Patel, P.; Bierman, P.J.; Jagadeesh, D.; Mitsuyasu, R.T.; Peace, D.; et al. Multicenter Study of Risk-Adapted Therapy With Dose-Adjusted EPOCH-R in Adults With Untreated Burkitt Lymphoma. J. Clin. Oncol. 2020, 38, 2519–2529. [Google Scholar] [CrossRef]
- Alderuccio, J.P.; Olszewski, A.J.; Evens, A.M.; Collins, G.P.; Danilov, A.V.; Bower, M.; Jagadeesh, D.; Zhu, C.; Sperling, A.; Kim, S.H.; et al. HIV-associated Burkitt lymphoma: Outcomes from a US-UK collaborative analysis. Blood Adv. 2021, 5, 2852–2862. [Google Scholar] [CrossRef]
- Vaccher, E.; Carbone, A. Simultaneous occurrence of KSHV-associated malignancies in a patient affected by HIV. Blood 2021, 137, 3149. [Google Scholar] [CrossRef]
- Re, A.; Cattaneo, C.; Michieli, M.; Casari, S.; Spina, M.; Rupolo, M.; Allione, B.; Nosari, A.; Schiantarelli, C.; Vigano, M.; et al. High-dose therapy and autologous peripheral-blood stem-cell transplantation as salvage treatment for HIV-associated lymphoma in patients receiving highly active antiretroviral therapy. J. Clin. Oncol. 2003, 21, 4423–4427. [Google Scholar] [CrossRef] [PubMed]
- Michieli, M.; Mazzucato, M.; Tirelli, U.; De Paoli, P. Stem cell transplantation for lymphoma patients with HIV infection. Cell Transpl. 2011, 20, 351–370. [Google Scholar] [CrossRef] [PubMed]
- Alvarnas, J.C.; Le Rademacher, J.; Wang, Y.; Little, R.F.; Akpek, G.; Ayala, E.; Devine, S.; Baiocchi, R.; Lozanski, G.; Kaplan, L.; et al. Autologous hematopoietic cell transplantation for HIV-related lymphoma: Results of the BMT CTN 0803/AMC 071 trial. Blood 2016, 128, 1050–1058. [Google Scholar] [CrossRef]
- Krishnan, A.; Molina, A.; Zaia, J.; Smith, D.; Vasquez, D.; Kogut, N.; Falk, P.M.; Rosenthal, J.; Alvarnas, J.; Forman, S.J. Durable remissions with autologous stem cell transplantation for high-risk HIV-associated lymphomas. Blood 2005, 105, 874–878. [Google Scholar] [CrossRef] [PubMed]
- Serrano, D.; Carrión, R.; Balsalobre, P.; Miralles, P.; Berenguer, J.; Buño, I.; Gómez-Pineda, A.; Ribera, J.M.; Conde, E.; Díez-Martín, J.L. HIV-associated lymphoma successfully treated with peripheral blood stem cell transplantation. Exp. Hematol. 2005, 33, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, T.R.; Ambinder, R.F.; Lee, J.Y.; Kaplan, L.D.; Wachsman, W.; Straus, D.J.; Aboulafia, D.M.; Scadden, D.T. Dose-reduced busulfan, cyclophosphamide, and autologous stem cell transplantation for human immunodeficiency virus-associated lymphoma: AIDS Malignancy Consortium study 020. Biol. Blood Marrow Transpl. 2008, 14, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Balsalobre, P.; Díez-Martín, J.L.; Re, A.; Michieli, M.; Ribera, J.M.; Canals, C.; Rosselet, A.; Conde, E.; Varela, R.; Cwynarski, K.; et al. Autologous stem-cell transplantation in patients with HIV-related lymphoma. J. Clin. Oncol. 2009, 27, 2192–2198. [Google Scholar] [CrossRef]
- Zanet, E.; Taborelli, M.; Rupolo, M.; Durante, C.; Mazzucato, M.; Zanussi, S.; De Paoli, P.; Serraino, D.; Tirelli, U.; Lleshi, A.; et al. Postautologous stem cell transplantation long-term outcomes in 26 HIV-positive patients affected by relapsed/refractory lymphoma. AIDS 2015, 29, 2303–2308. [Google Scholar] [CrossRef]
- Gabarre, J.; Marcelin, A.G.; Azar, N.; Choquet, S.; Lévy, V.; Lévy, Y.; Tubiana, R.; Charlotte, F.; Norol, F.; Calvez, V.; et al. High-dose therapy plus autologous hematopoietic stem cell transplantation for human immunodeficiency virus (HIV)-related lymphoma: Results and impact on HIV disease. Haematologica 2004, 89, 1100–1108. [Google Scholar]
- Díez-Martín, J.L.; Balsalobre, P.; Re, A.; Michieli, M.; Ribera, J.M.; Canals, C.; Conde, E.; Rosselet, A.; Gabriel, I.; Varela, R.; et al. Comparable survival between HIV+ and HIV- non-Hodgkin and Hodgkin lymphoma patients undergoing autologous peripheral blood stem cell transplantation. Blood 2009, 113, 6011–6014. [Google Scholar] [CrossRef]
- Krishnan, A.; Palmer, J.M.; Zaia, J.A.; Tsai, N.C.; Alvarnas, J.; Forman, S.J. HIV status does not affect the outcome of autologous stem cell transplantation (ASCT) for non-Hodgkin lymphoma (NHL). Biol. Blood Marrow Transpl. 2010, 16, 1302–1308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, R.K.; Abdul-Jawad, S.; McCoy, L.E.; Mok, H.P.; Peppa, D.; Salgado, M.; Martinez-Picado, J.; Nijhuis, M.; Wensing, A.M.J.; Lee, H.; et al. HIV-1 remission following CCR5Δ32/Δ32 haematopoietic stem-cell transplantation. Nature 2019, 568, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Ambinder, R.F.; Wu, J.; Logan, B.; Durand, C.M.; Shields, R.; Popat, U.R.; Little, R.F.; McMahon, D.K.; Cyktor, J.; Mellors, J.W.; et al. Allogeneic Hematopoietic Cell Transplant for HIV Patients with Hematologic Malignancies: The BMT CTN-0903/AMC-080 Trial. Biol. Blood Marrow Transpl. 2019, 25, 2160–2166. [Google Scholar] [CrossRef]
- Kwon, M.; Bailén, R.; Balsalobre, P.; Jurado, M.; Bermudez, A.; Badiola, J.; Esquirol, A.; Miralles, P.; López-Fernández, E.; Sanz, J.; et al. Allogeneic stem-cell transplantation in HIV-1-infected patients with high-risk hematological disorders. AIDS 2019, 33, 1441–1447. [Google Scholar] [CrossRef] [PubMed]
- Allers, K.; Hütter, G.; Hofmann, J.; Loddenkemper, C.; Rieger, K.; Thiel, E.; Schneider, T. Evidence for the cure of HIV infection by CCR5Δ32/Δ32 stem cell transplantation. Blood 2011, 117, 2791–2799. [Google Scholar] [CrossRef] [PubMed]
- Rust, B.J.; Kiem, H.P.; Uldrick, T.S. CAR T-cell therapy for cancer and HIV through novel approaches to HIV-associated haematological malignancies. Lancet Haematol. 2020, 7, e690–e696. [Google Scholar] [CrossRef]
- Anthony-Gonda, K.; Bardhi, A.; Ray, A.; Flerin, N.; Li, M.; Chen, W.; Ochsenbauer, C.; Kappes, J.C.; Krueger, W.; Worden, A.; et al. Multispecific anti-HIV duoCAR-T cells display broad in vitro antiviral activity and potent in vivo elimination of HIV-infected cells in a humanized mouse model. Sci. Transl. Med. 2019, 11, eaav5685. [Google Scholar] [CrossRef]
- Bohlius, J.; Schmidlin, K.; Boué, F.; Fätkenheuer, G.; May, M.; Caro-Murillo, A.M.; Mocroft, A.; Bonnet, F.; Clifford, G.; Paparizos, V.; et al. HIV-1-related Hodgkin lymphoma in the era of combination antiretroviral therapy: Incidence and evolution of CD4⁺ T-cell lymphocytes. Blood 2011, 117, 6100–6108. [Google Scholar] [CrossRef]
- Goedert, J.J.; Bower, M. Impact of highly effective antiretroviral therapy on the risk for Hodgkin lymphoma among people with human immunodeficiency virus infection. Curr. Opin. Oncol. 2012, 24, 531–536. [Google Scholar] [CrossRef]
- Kowalkowski, M.A.; Mims, M.P.; Amiran, E.S.; Lulla, P.; Chiao, E.Y. Effect of immune reconstitution on the incidence of HIV-related Hodgkin lymphoma. PLoS ONE 2013, 8, e77409. [Google Scholar] [CrossRef]
- Shiels, M.S.; Islam, J.Y.; Rosenberg, P.S.; Hall, H.I.; Jacobson, E.; Engels, E.A. Projected Cancer Incidence Rates and Burden of Incident Cancer Cases in HIV-Infected Adults in the United States Through 2030. Ann. Intern. Med. 2018, 168, 866–873. [Google Scholar] [CrossRef] [PubMed]
- Kimani, S.M.; Painschab, M.S.; Horner, M.J.; Muchengeti, M.; Fedoriw, Y.; Shiels, M.S.; Gopal, S. Epidemiology of haematological malignancies in people living with HIV. Lancet HIV 2020, 7, e641–e651. [Google Scholar] [CrossRef]
- Martis, N.; Mounier, N. Hodgkin lymphoma in patients with HIV infection: A review. Curr. Hematol. Malig. Rep. 2012, 7, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Swart, L.; Novitzky, N.; Mohamed, Z.; Opie, J. Hodgkin lymphoma at Groote Schuur Hospital, South Africa: The effect of HIV and bone marrow infiltration. Ann. Hematol. 2019, 98, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Moahi, K.; Ralefala, T.; Nkele, I.; Triedman, S.; Sohani, A.; Musimar, Z.; Efstathiou, J.; Armand, P.; Lockman, S.; Dryden-Peterson, S. HIV and Hodgkin Lymphoma Survival: A Prospective Study in Botswana. JCO Glob. Oncol. 2022, 8, e2100163. [Google Scholar] [CrossRef]
- Okosun, J.; Warbey, V.; Shaw, K.; Montoto, S.; Fields, P.; Marcus, R.; Virchis, A.; McNamara, C.; Bower, M.; Cwynarski, K. Interim fluoro-2-deoxy-D-glucose-PET predicts response and progression-free survival in patients with Hodgkin lymphoma and HIV infection. AIDS 2012, 26, 861–865. [Google Scholar] [CrossRef]
- Danilov, A.V.; Li, H.; Press, O.W.; Shapira, I.; Swinnen, L.J.; Noy, A.; Reid, E.; Smith, S.M.; Friedberg, J.W. Feasibility of interim positron emission tomography (PET)-adapted therapy in HIV-positive patients with advanced Hodgkin lymphoma (HL): A sub-analysis of SWOG S0816 Phase 2 trial. Leuk. Lymphoma 2017, 58, 461–465. [Google Scholar] [CrossRef]
- Louarn, N.; Galicier, L.; Bertinchamp, R.; Lussato, D.; Montravers, F.; Oksenhendler, É.; Merlet, P.; Gérard, L.; Vercellino, L. First Extensive Analysis of (18)F-Labeled Fluorodeoxyglucose Positron Emission Tomography-Computed Tomography in a Large Cohort of Patients With HIV-Associated Hodgkin Lymphoma: Baseline Total Metabolic Tumor Volume Affects Prognosis. J. Clin. Oncol. 2022, 40, 1346–1355. [Google Scholar] [CrossRef]
- Uldrick, T.S.; Gonçalves, P.H.; Abdul-Hay, M.; Claeys, A.J.; Emu, B.; Ernstoff, M.S.; Fling, S.P.; Fong, L.; Kaiser, J.C.; Lacroix, A.M.; et al. Assessment of the Safety of Pembrolizumab in Patients With HIV and Advanced Cancer-A Phase 1 Study. JAMA Oncol. 2019, 5, 1332–1339. [Google Scholar] [CrossRef]
- Gonzalez-Cao, M.; Morán, T.; Dalmau, J.; Garcia-Corbacho, J.; Bracht, J.W.P.; Bernabe, R.; Juan, O.; de Castro, J.; Blanco, R.; Drozdowskyj, A.; et al. Assessment of the Feasibility and Safety of Durvalumab for Treatment of Solid Tumors in Patients With HIV-1 Infection: The Phase 2 DURVAST Study. JAMA Oncol. 2020, 6, 1063–1067. [Google Scholar] [CrossRef]
- Ramaswami, R.; Lurain, K.; Polizzotto, M.N.; Ekwede, I.; Waldon, K.; Steinberg, S.M.; Mangusan, R.; Widell, A.; Rupert, A.; George, J.; et al. Characteristics and outcomes of KSHV-associated multicentric Castleman disease with or without other KSHV diseases. Blood Adv. 2021, 5, 1660–1670. [Google Scholar] [CrossRef] [PubMed]
- Borges, Á.H.; Neuhaus, J.; Babiker, A.G.; Henry, K.; Jain, M.K.; Palfreeman, A.; Mugyenyi, P.; Domingo, P.; Hoffmann, C.; Read, T.R.; et al. Immediate Antiretroviral Therapy Reduces Risk of Infection-Related Cancer During Early HIV Infection. Clin. Infect. Dis. 2016, 63, 1668–1676. [Google Scholar] [CrossRef] [PubMed]
- Lundgren, J.D.; Babiker, A.G.; Gordin, F.; Emery, S.; Grund, B.; Sharma, S.; Avihingsanon, A.; Cooper, D.A.; Fätkenheuer, G.; Llibre, J.M.; et al. Initiation of Antiretroviral Therapy in Early Asymptomatic HIV Infection. N. Engl. J. Med. 2015, 373, 795–807. [Google Scholar] [CrossRef] [PubMed]
- Herr, M.M.; Schonfeld, S.J.; Dores, G.M.; Engels, E.A.; Tucker, M.A.; Curtis, R.E.; Morton, L.M. Risk for malignancies of infectious etiology among adult survivors of specific non-Hodgkin lymphoma subtypes. Blood Adv. 2019, 3, 1961–1969. [Google Scholar] [CrossRef]
- Pérez-González, A.; Cachay, E.; Ocampo, A.; Poveda, E. Update on the Epidemiological Features and Clinical Implications of Human Papillomavirus Infection (HPV) and Human Immunodeficiency Virus (HIV) Coinfection. Microorganisms 2022, 10, 1047. [Google Scholar] [CrossRef]
- Osarogiagbon, R.U.; Liao, W.; Faris, N.R.; Meadows-Taylor, M.; Fehnel, C.; Lane, J.; Williams, S.C.; Patel, A.A.; Akinbobola, O.A.; Pacheco, A.; et al. Lung Cancer Diagnosed Through Screening, Lung Nodule, and Neither Program: A Prospective Observational Study of the Detecting Early Lung Cancer (DELUGE) in the Mississippi Delta Cohort. J. Clin. Oncol. 2022, 40, 2094–2105. [Google Scholar] [CrossRef]
- Lee, L.Y.; Cazier, J.B.; Angelis, V.; Arnold, R.; Bisht, V.; Campton, N.A.; Chackathayil, J.; Cheng, V.W.; Curley, H.M.; Fittall, M.W.; et al. COVID-19 mortality in patients with cancer on chemotherapy or other anticancer treatments: A prospective cohort study. Lancet 2020, 395, 1919–1926. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Categories | Lymphomas and Lymphoproliferative Disorders |
|---|---|
| B-cell malignancies | Hodgkin lymphoma |
| Diffuse large B-cell lymphoma | |
| Burkitt lymphoma | |
| Plasmablastic lymphoma | |
| NK- and T-cell malignancies | Angioimmunoblastic T-cell lymphoma # |
| Follicular T-cell lymphoma # | |
| Peripheral T-cell lymphomas | |
| Extranodal NK/T cell lymphoma, nasal type | |
| Immunodeficiency related | Post-transplant lymphoproliferative disorders |
| HIV-related |
| KSHV-Associated Disorders | Kaposi Sarcoma |
|---|---|
| Primary effusion lymphoma | |
| MCD-associated large B-cell lymphoma | |
| KSHV-positive germinotropic lymphoproliferative disorder |
| Patients N° | Study Design | CD4 Count /µL | DLBCL % | aa-IPI ≥ 2 % | CR Rate % | PFS | Overall Survival | Infectious Death % | |
|---|---|---|---|---|---|---|---|---|---|
| R-CHOP-R vs. CHOP (Kaplan et al., 2005 [28]) | 150 | Phase 3 | 130 | 81 | 43 | 58 vs. 47 | 11.3 vs. 9.5 mos | 28 vs. 35 mos | 14 °° vs. 2 * |
| R-CHOP (Bouè et al., 2006 [31]) | 61 | Phase 2 | 172 | 72 | 48 | 77 | 69% (2 yr) | 75% (2 yr) | 2 |
| R-CHOP (Ribera et al., 2008 [32]) | 95 | Phase 2 | 158 | 81 | 58 | 69 | NA | 56% (3 yr) | 7 |
| R-CDE (Spina et al., 2005 [33]) | 74 | Phase 2 * | 161 | 72 | 57 | 70 | 52% EFS (2 yr) | 64% (2 yr) | 7 |
| R-EPOCH (Sparano et al., 2010 [29]) | 106 | Randomized phase 2: R-EPOCH vs. EPOCH-R | 194 | 80 | 64 | 73 vs. 55 | 66 vs. 63% (2 yr) | 70 vs. 67% (2 yr) | 10 °° vs. 7 |
| SC-EPOCH-RR (Dunleavy et al., 2010 [30]) | 33 | Phase 2 | 208 | 100 | 76 | 91 | 84% (5yr) | 68% (5yr) | 0 |
| VORINOSTAT-R °-EPOCH (Ramos 2020 [34]) | 90 | Randomized Phase 2 | 54 % (<200) | 71 | 66 | 68 vs. 74 | 63 vs. 69% EFS (3 yr) | 70 vs. 77% (3 yr) | NA |
| References | Patients N° | Study (s) Design | Conditioning Regimen | Follow-Up Median, mos | PFS % | Overall Survival % | TRM % |
|---|---|---|---|---|---|---|---|
| Gabarre et al., 2004 [50] | 14 | Prospective Phase 2 | BEAM, TBI-based, Bu/Cy | 32 | NA | 5 pts alive | 0 |
| Krishnan et al., 2005 [45] | 20 | Retrospective Case–control s | CBV, TBI/CyEto | 32 | 85 | 85 | 5 |
| Serrano et al., 2005 [46] | 33 | Prospective phase 2 | BEAM, BEAC, TBI-based | 58 | 53 | 61 | 0 |
| Spitzer et al., 2008 [47] | 20 | Prospective phase 2 | Low dose Bu/Cy | 6 | 49 | 74 | 5 |
| Re et al., 2003 [42] | 27 | Prospective phase 2 s | BEAM | 44 | 76 | 75 | 0 |
| Balsalobre et al., 2009 [48] | 68 | Retrospective multicentric s | BEAM, TBI-based | 32 | 56 | 61 | 4 |
| Zanet et al., 2015 [49] | 26 CR | Retrospective Single-centric s | BEAM | 72 | 86 (10 yr) | 91 (10 yr) | 0 |
| Alvarnas et al., 2016 [44] | 40 | Prospective | BEAM | 25 | 80 | 82 | 5 |
| Cancer | Prevention | Patients at Risk | Screening Methods | Screening Frequency |
|---|---|---|---|---|
| Cervical cancer | HPV vaccination * | -Sexually active women -Age ≥ 21 yrs | Pap Testing (PT) Co-testing (Pap Testing+HPV Testing) Colposcopy (C) | -Age < 30 yrs: baseline, every 12 mos until 3 normal PTs, then every 3 yrs -Age ≥ 30 yrs: baseline, every 12 mos until 3 normal PTs, then every 3 yrs or every 3 yrs if normal co-testing -Annualy co-testing if normal PT and positive HR-HPV testing -Performed C if abnormal PT or positive HR-HPV testing |
| Anal cancer | HPV vaccination * | -All PLWHs -MSM -All PLWHs with a history of anogenital condylomas -Women with abnormal genital histology | -Visual inspection of perianal region plus digital rectal examination Anal Pap Testing (aPT) -HRA ** | -Annually -Baseline and annually, every 3–6 mos if abnormal aPT -Performed HRA if abnormal aPT (ASCUS, LSIL, HSIL) |
| Liver cancer | -HBV vaccination -HBV/HCV therapy -Alcohol cessation | -HCV/HIV with cirrhosis -HBV/HIV resistant to antiviral therapy | Abdominal ultrasonography+/-AFP testing | -Every 6–12 mos |
| Lung cancer | Smoking cessation | -Smokers > 20 pack-year -Current or former smokers who quit smoking within 10 yrs and age > 40 yrs | Low-dose chest CT | Annually |
| Skin cancer | Reduction/protection sun exposure | -Fair skin -White/non-Hispanic ethnicity | Skin examination | Annually |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaccher, E.; Gloghini, A.; Volpi, C.C.; Carbone, A. Lymphomas in People Living with HIV. Hemato 2022, 3, 527-542. https://doi.org/10.3390/hemato3030037
Vaccher E, Gloghini A, Volpi CC, Carbone A. Lymphomas in People Living with HIV. Hemato. 2022; 3(3):527-542. https://doi.org/10.3390/hemato3030037
Chicago/Turabian StyleVaccher, Emanuela, Annunziata Gloghini, Chiara C. Volpi, and Antonino Carbone. 2022. "Lymphomas in People Living with HIV" Hemato 3, no. 3: 527-542. https://doi.org/10.3390/hemato3030037
APA StyleVaccher, E., Gloghini, A., Volpi, C. C., & Carbone, A. (2022). Lymphomas in People Living with HIV. Hemato, 3(3), 527-542. https://doi.org/10.3390/hemato3030037