
Impact of 18F-FDG PET/CT in Predicting Recurrence in Neurolymphomatosis

 , ,
, ,
Abstract
:1. Introduction
1.1. Subjects and Data Extraction
1.2. 18F-FDG PET/CT Protocol
1.3. Statistical Analysis
2. Results
2.1. Patient Characteristics and 18F-FDG PET/CT Findings
2.2. Comparison between Clinical and 18F-FDG PET/CT Findings
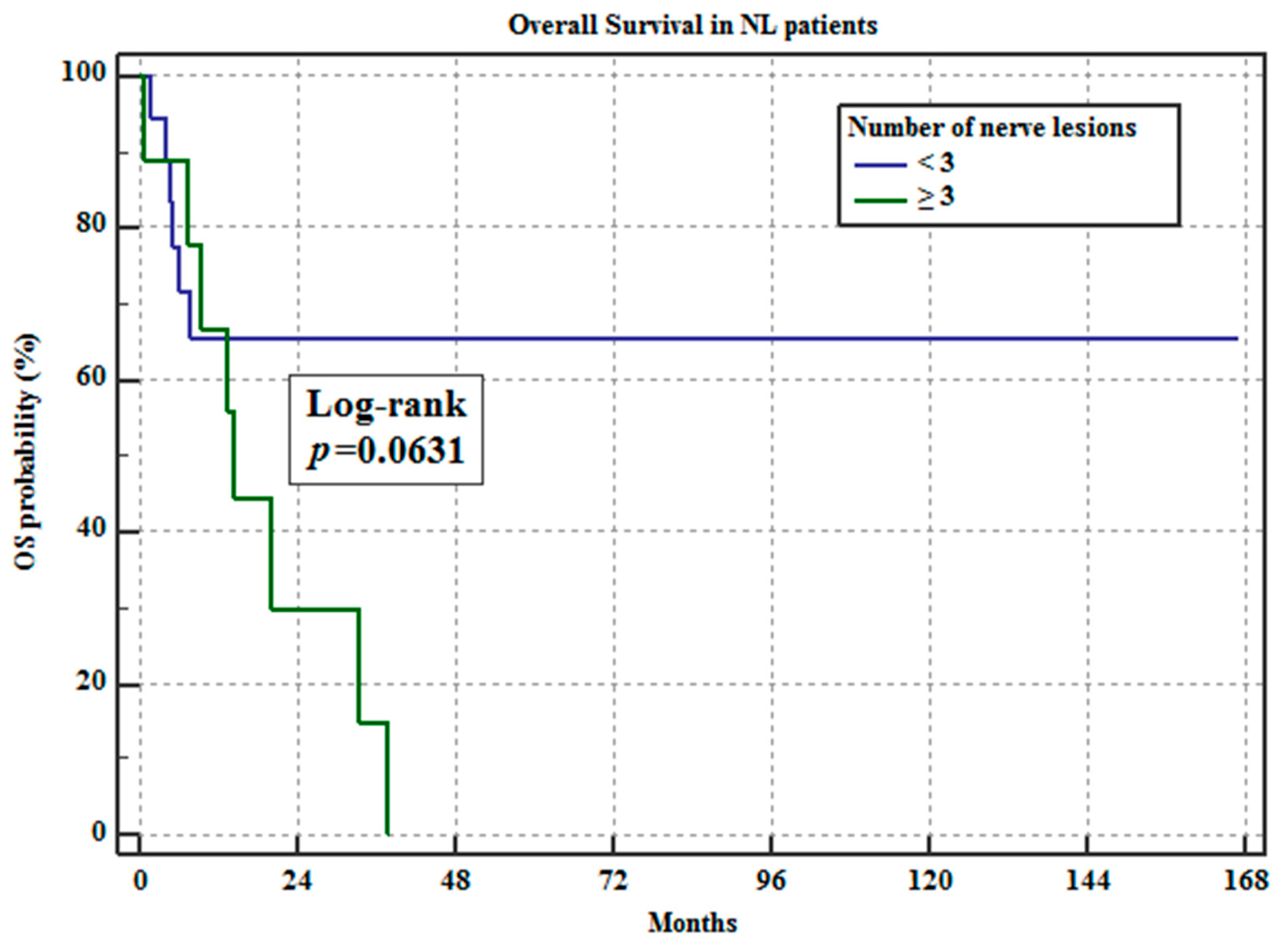
2.3. RFS and OS Analyses
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grisariu, S.; Avni, B.; Batchelor, T.T.; van den Bent, M.J.; Bokstein, F.; Schiff, D.; Roth, P.; Nemets, A.; Shalom, E.; Siegal, T.; et al. Neurolymphomatosis: An International Primary CNS Lymphoma Collaborative Group report. Blood 2010, 115, 5005–5011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baehring, J.M.; Damek, D.; Martin, E.C.; Betensky, R.A.; Hochberg, F.H. Neurolymphomatosis. Neuro-Oncol. 2003, 5, 104–115. [Google Scholar] [CrossRef] [PubMed]
- Bourque, P.R.; Sampaio, M.L.; Warman-Chardon, J.; Samaan, S.; Torres, C. Neurolymphomatosis of the lumbosacral plexus and its branches: Case series and literature review. BMC Cancer 2019, 19, 1149. [Google Scholar] [CrossRef]
- Jeong, J.; Kim, S.W.; Sung, D.H. Neurolymphomatosis: A single-center experience of neuromuscular manifestations, treatments, and outcomes. J. Neurol. 2020, 268, 851–859. [Google Scholar] [CrossRef]
- Tomita, M.; Koike, H.; Kawagashira, Y.; Iijima, M.; Adachi, H.; Taguchi, J.; Sobue, G.; Sako, K.; Tsuji, Y.; Nakagawa, M.; et al. Clinicopathological features of neuropathy associated with lymphoma. Brain 2013, 136, 2563–2578. [Google Scholar] [CrossRef] [Green Version]
- Van den Bent, M.J.; de Bruin, H.G.; Bos, G.M.; Brutel de la Rivière, G.; Sillevis Smitt, P.A. Negative sural nerve biopsy in neurolymphomatosis. J. Neurol. 1999, 246, 1159–1163. [Google Scholar] [CrossRef]
- Shree, R.; Goyal, M.K.; Modi, M.; Gaspar, B.L.; Radotra, B.D.; Ahuja, C.K.; Prakash, G.; Mittal, B.R. The Diagnostic Dilemma of Neurolymphomatosis. J. Clin. Neurol. 2016, 12, 274–281. [Google Scholar] [CrossRef] [Green Version]
- DeVries, A.H.; Howe, B.M.; Spinner, R.J.; Broski, S.M. B-cell peripheral neurolymphomatosis: MRI and 18F-FDG PET/CT imaging characteristics. Skelet. Radiol. 2019, 48, 1043–1050. [Google Scholar] [CrossRef]
- Salm, L.P.; Van der Hiel, B.; Stokkel, M.P.M. Increasing importance of 18F-FDG PET in the diagnosis of neurolymphomatosis. Nucl. Med. Commun. 2012, 33, 907–916. [Google Scholar] [CrossRef]
- Davidson, T.; Kedmi, M.; Avigdor, A.; Komisar, O.; Chikman, B.; Lidar, M.; Ben-Haim, S.; Goshen, E.; Zwas, S.T. FDG PET-CT evaluation in neurolymphomatosis: Imaging characteristics and clinical outcomes. Leuk. Lymphoma 2018, 59, 348–356. [Google Scholar] [CrossRef]
- Kamiya-Matsuoka, C.; Shroff, S.; Gildersleeve, K.; Hormozdi, B.; Manning, J.T.; Woodman, K.H. Neurolymphomatosis: A case series of clinical manifestations, treatments, and outcomes. J. Neurol. Sci. 2014, 343, 144–148. [Google Scholar] [CrossRef]
- Jellinger, K.; Radaszkiewicz, T. Involvement of the central nervous system in malignant lymphomas. Virchows Arch. A 1976, 370, 345–362. [Google Scholar] [CrossRef]
- Matsue, K.; Hayama, B.Y.; Iwama, K.; Koyama, T.; Fujiwara, H.; Yamakura, M.; O'uchi, T.; Takeuchi, M. High frequency of neurolymphomatosis as a relapse disease of intravascular large B-cell lymphoma. Cancer 2011, 117, 4512–4521. [Google Scholar] [CrossRef] [PubMed]
- Oner, A.O.; Okuyucu, K.; Alagoz, E.; Battal, B.; Arslan, N. An Extremely Rare Intersection: Neurolymphomatosis in a Patient with Burkitt Lymphoma Detected by 18F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography. World J. Nucl. Med. 2016, 15, 209–211. [Google Scholar] [CrossRef] [PubMed]
- Pan, Q.; Luo, Y. Recurrence of nasal type NK/T cell lymphoma presenting as neurolymphomatosis on 18F-FDG PET/CT: A case report and literature review. Medicine. 2020, 99, e18640. [Google Scholar] [CrossRef] [PubMed]
- Stübgen, J.P. Lymphoma-associated dysimmune polyneuropathies. J. Neurol. Sci. 2015, 355, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Briani, C.; Visentin, A.; Campagnolo, M.; Salvalaggio, A.; Ferrari, S.; Cavallaro, T.; Piazza, F.; Manara, R.; Gasparotti, R. Peripheral nervous system involvement in lymphomas. J. Peripher. Nerv. Syst. 2019, 24, 5–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baehring, J.M.; Batchelor, T.T. Diagnosis and management of neurolymphomatosis. Cancer J. 2012, 18, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Gan, H.K.; Azad, A.; Cher, L.; Mitchell, P.L.R. Neurolymphomatosis: Diagnosis, management, and outcomes in patients treated with rituximab. Neuro-Oncol. 2010, 12, 212–215. [Google Scholar] [CrossRef] [PubMed]
- Ekstein, D.; Ben-Yehuda, D.; Slyusarevsky, E.; Lossos, A.; Linetsky, E.; Siegal, T. CSF analysis of IgH gene rearrangement in CNS lymphoma: Relationship to the disease course. J. Neurol. Sci. 2006, 247, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Scott, B.J.; Douglas, V.C.; Tihan, T.; Rubenstein, J.L.; Josephson, S.A. A systematic approach to the diagnosis of suspected central nervous system lymphoma. JAMA Neurol. 2013, 70, 311–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Findings | |
|---|---|
| Age, years; mean ± SD (range) | 70.1 ± 10.1 (44–87) |
| Sex, n (%) | |
| Female | 15 (53.6) |
| Male | 13 (46.4) |
| Subtype of lymphoma, n (%) | |
| DLBCL | 21 (75.0) |
| IVL | 5 (17.9) |
| MCL | 2 (7.1) |
| IPI at the initial diagnosis of lymphoma | |
| 5 | 3 (10.7) |
| 4 | 15 (53.6) |
| 3 | 5 (17.9) |
| 2 | 2 (7.1) |
| 1 | 1 (3.6) |
| 0 | 0 (0) |
| NA | 2 (7.1) |
| FDG PET/CT findings, n (%) | |
| Number of nerve lesions | |
| <3 | 19 (67.9) |
| ≧3 | 9 (32.1) |
| ENL | |
| + | 18 (64.3) |
| − | 10 (35.7) |
| Outcome, n (%) | |
| Recurrence | |
| + | 7 (25.0) |
| − | 21 (75.0) |
| Status at final follow-up | |
| Dead | 14 (50.0) |
| Alive | 14 (50.0) |
| FDG PET/CT Findings | ||||||
|---|---|---|---|---|---|---|
| Number of Nerve Lesions | ENL | |||||
| <3 (n = 19) | ≧3 (n = 9) | p | + (n = 18) | − (n = 10) | p | |
| Age, years; mean ± SD | 72.9 ± 11.1 | 70.4 ± 8.8 | 0.5593 | 74.3 ± 8.1 | 68.3 ± 13.1 | 0.1446 |
| Sex, n (%) | 0.8869 | 0.7815 | ||||
| Female | 10 (52.6) | 5 (55.6) | 10 (55.6) | 5 (50) | ||
| Male | 9 (47.4) | 4 (44.4) | 8 (44.4) | 5 (50) | ||
| Subtype of ML, n (%) | 0.757 | 0.0748 | ||||
| DLBCL | 15 (71.4) | 6 (28.6) | 11 (52.3) | 10 (47.7) | ||
| IVL | 3 (60) | 2 (40) | 5 (100) | 0 (0.0) | ||
| MCL | 1 (50) | 1 (50) | 2 (100) | 0 (0.0) | ||
| Recurrence, n (%) | 0.0085 | 0.6547 | ||||
| + | 1 (14.3) | 6 (85.7) | 4 (57.1) | 3 (42.9) | ||
| − | 18 (85.7) | 3 (14.3) | 14 (66.7) | 7 (33.3) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uemichi, M.; Yokoyama, K.; Tsuchiya, J.; Terao, T.; Machida, Y.; Matsue, K.; Tateishi, U. Impact of 18F-FDG PET/CT in Predicting Recurrence in Neurolymphomatosis. Hemato 2021, 2, 596-606. https://doi.org/10.3390/hemato2030038
Uemichi M, Yokoyama K, Tsuchiya J, Terao T, Machida Y, Matsue K, Tateishi U. Impact of 18F-FDG PET/CT in Predicting Recurrence in Neurolymphomatosis. Hemato. 2021; 2(3):596-606. https://doi.org/10.3390/hemato2030038
Chicago/Turabian StyleUemichi, Megumi, Kota Yokoyama, Junichi Tsuchiya, Toshiki Terao, Youichi Machida, Kosei Matsue, and Ukihide Tateishi. 2021. "Impact of 18F-FDG PET/CT in Predicting Recurrence in Neurolymphomatosis" Hemato 2, no. 3: 596-606. https://doi.org/10.3390/hemato2030038
APA StyleUemichi, M., Yokoyama, K., Tsuchiya, J., Terao, T., Machida, Y., Matsue, K., & Tateishi, U. (2021). Impact of 18F-FDG PET/CT in Predicting Recurrence in Neurolymphomatosis. Hemato, 2(3), 596-606. https://doi.org/10.3390/hemato2030038