
Friction-Induced Biphasic Cutaneous Amyloidosis



{kind=link}
{kind=link}
Abstract
:1. Introduction
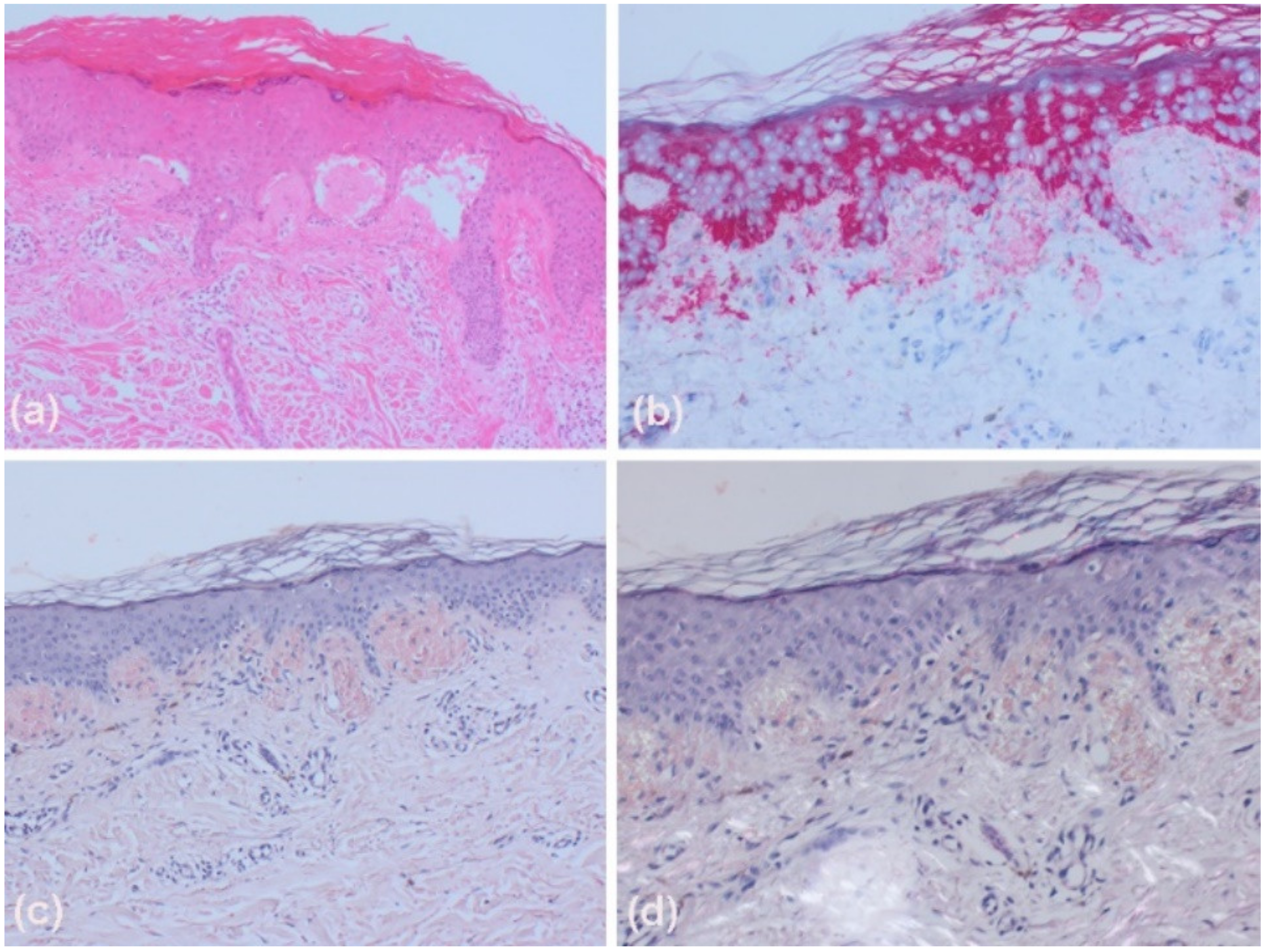
2. Case
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schreml, S.; Szeimies, R.M.; Landthaler, M.; Babilas, P. Kutane Amyloidosen [Cutaneous amyloidosis]. Hautarzt 2011, 62, 55–61. [Google Scholar] [CrossRef]
- Fernandez-Flores, A. Cutaneous amyloidosis: A concept review. Am. J. Dermatopathol. 2012, 34, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Siragusa, M.; Ferri, R.; Cavallari, V.; Schepis, C. Friction melanosis, friction amyloidosis, macular amyloidosis, towel melanosis: Many names for the same clinical entity. Eur. J. Dermatol. 2001, 11, 545–548. [Google Scholar] [PubMed]
- Iwasaki, K.; Mihara, M.; Nishiura, S.; Shimao, S. Biphasic amyloidosis arising from friction melanosis. J. Dermatol. 1991, 18, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Inoue, K.; Takahashi, M.; Hamamoto, Y.; Muto, M.; Ishihara, T. An immunohistochemical study of cytokeratins in skin-limited amyloidosis. Amyloid 2000, 7, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Chapman, J.R.; Liu, A.; Yi, S.S.; Hernandez, E.; Ritorto, M.S.; Jungbluth, A.A.; Pulitzer, M.; Dogan, A. Proteomic analysis shows that the main constituent of subepidermal localised cutaneous amyloidosis is not galectin-7. Amyloid 2021, 28, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Baba, A.; Taniguchi, K.; Orihara, T.; Furuya, T. 6 cases of friction melanosis with amyloid deposition and frequency of friction melanosis in general population by questionnaires. Nihon Hifuka Gakkai Zasshi 1986, 96, 1215–1223. [Google Scholar] [PubMed]
- Hernández-Núñez, A.; Daudén, E.; Moreno de Vega, M.J.; Fraga, J.; Aragüés, M.; García-Díez, A. Widespread biphasic amyloidosis: Response to acitretin. Clin. Exp. Dermatol. 2001, 26, 256–259. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gambichler, T.; Susok, L.; Segert, M.H. Friction-Induced Biphasic Cutaneous Amyloidosis. Dermato 2021, 1, 31-34. https://doi.org/10.3390/dermato1010005
Gambichler T, Susok L, Segert MH. Friction-Induced Biphasic Cutaneous Amyloidosis. Dermato. 2021; 1(1):31-34. https://doi.org/10.3390/dermato1010005
Chicago/Turabian StyleGambichler, Thilo, Laura Susok, and Marc H. Segert. 2021. "Friction-Induced Biphasic Cutaneous Amyloidosis" Dermato 1, no. 1: 31-34. https://doi.org/10.3390/dermato1010005
APA StyleGambichler, T., Susok, L., & Segert, M. H. (2021). Friction-Induced Biphasic Cutaneous Amyloidosis. Dermato, 1(1), 31-34. https://doi.org/10.3390/dermato1010005