A Case of Unilateral Hyperpigmentation

 , , and
, , and 
Abstract
1. Introduction
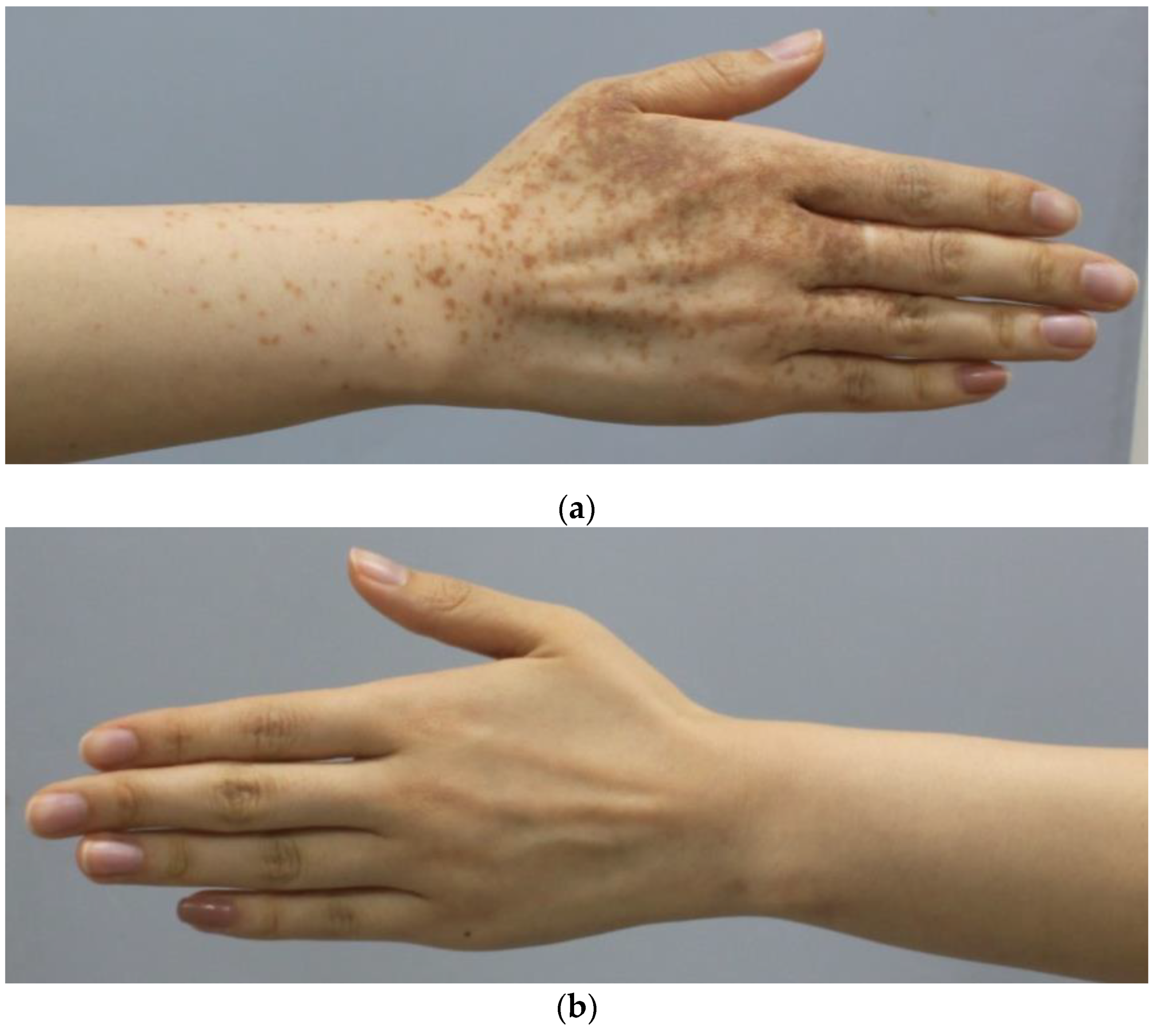
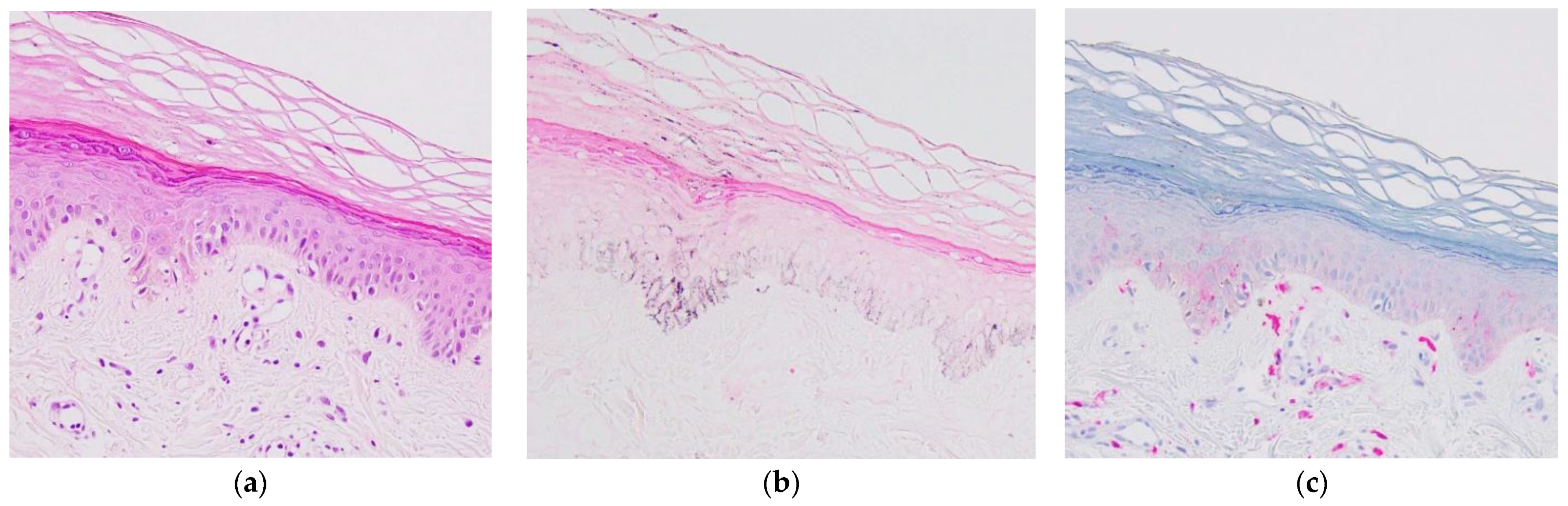
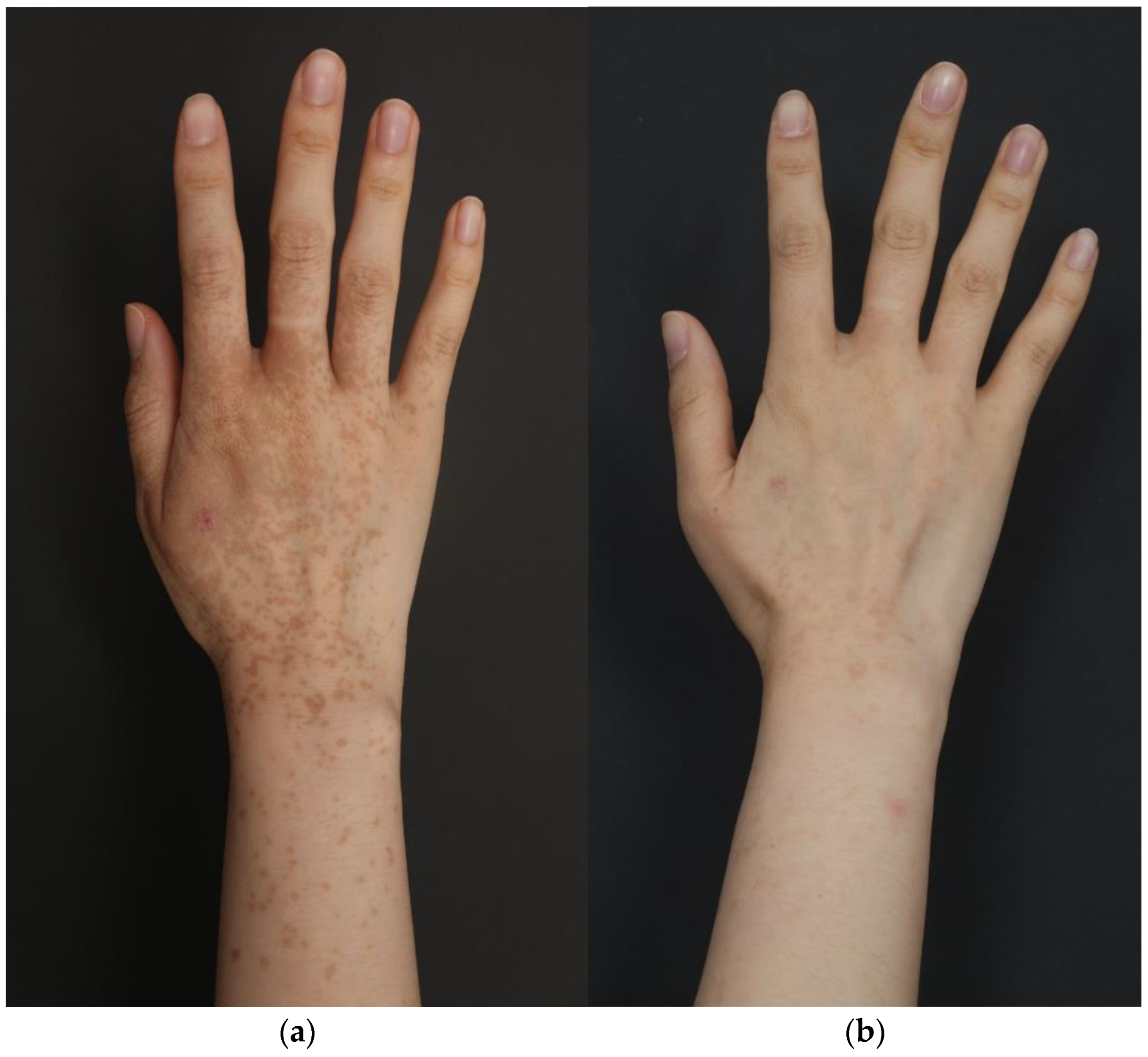
2. Case
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pomeranz, M.K.; Karen, J.K. Phytophotodermatitis and Limes. N. Engl. J. Med. 2007, 357, e1. [Google Scholar] [CrossRef] [PubMed]
- Abugroun, A.; Gaznabi, S.; Natarajan, A.; Daoud, H. Lime-induced phytophotodermatitis. Oxf. Med. Case Rep. 2019, 2019, 470–472. [Google Scholar] [CrossRef] [PubMed]
- Bonamonte, D.; Foti, C.; Lionetti, N.; Rigano, L.; Angelini, G. Photoallergic contact dermatitis to 8-methoxypsoralen in Ficus carica. Contact Dermat. 2010, 62, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Son, J.-H.; Jin, H.; You, H.-S.; Shim, W.-H.; Kim, J.-M.; Kim, G.-W.; Kim, H.-S.; Ko, H.-C.; Kim, M.-B.; Kim, B.-S. Five Cases of Phytophotodermatitis Caused by Fig Leaves and Relevant Literature Review. Ann. Dermatol. 2017, 29, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Klaber, R. Phytophotodermatitis. Br. J. Dermatol. 1942, 54, 193–211. [Google Scholar] [CrossRef]
- Walling, A.; Walling, H.W. Phytophotodermatitis induced by wild parsnip. Dermatol. Online J. 2018, 24. [Google Scholar] [CrossRef]
- Carlsen, K.; Weismann, K. Phytophotodermatitis in 19 children admitted to hospital and their differential diagnoses: Child abuse and herpes simplex virus infection. J. Am. Acad. Dermatol. 2007, 57 (Suppl. 5), S88–S91. [Google Scholar] [CrossRef] [PubMed]
- Walling, A.L.; Walling, H.W. Prolonged hyperpigmentation induced by wild parsnip phytophotodermatitis. Arch. Clin. Exp. Dermatol. 2020, 2, 116. [Google Scholar]
- Tse, Y.; Levine, V.J.; A McClain, S.; Ashinoff, R. The removal of cutaneous pigmented lesions with the Q-switched ruby laser and the Q-switched neodymium: Yttrium-aluminum-garnet laser. A comparative study. J. Dermatol. Surg. Oncol. 1994, 20, 795–800. [Google Scholar] [CrossRef] [PubMed]
- Babilas, P.; Schreml, S.; Szeimies, R.-M.; Landthaler, M. Intense pulsed light (IPL): A review. Lasers Surg. Med. 2010, 42, 93–104. [Google Scholar] [CrossRef] [PubMed]
- Coffman, K.; Boyce, W.T.; Hansen, R.C. Phytophotodermatitis Simulating Child Abuse. Arch. Pediatr. Adolesc. Med. 1985, 139, 239–240. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.M.; Wu, J.J.; Hansen, R.C.; Nigg, H.N.; Beiere, R.C. Bullous Phytophotodermatitis Associated with High Natural Concentrations of Furanocoumarins in Limes. Am. J. Contact. Dermat. 2002, 13, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Hankinson, A.; Lloyd, B.; Alweis, R. Lime-induced phytophotodermatitis. J. Community Hosp. Intern. Med. Perspect. 2014, 4. [Google Scholar] [CrossRef] [PubMed]
- Mioduszewski, M.; Beecker, J. Phytophotodermatitis from making sangria: A phototoxic reaction to lime and lemon juice. Can. Med. Assoc. J. 2015, 187, 756. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Galvan-Perez del Pulgar, J.I.; Linares-Barrios, M.; Galvañ-Pozo, J.I., Jr. Acropigmentation of the Dorsum of the Hands from Preparing Mojitos: A Lime-Induced Phytophotodermatosis. Actas Dermosifiliogr. 2016, 107, 253–255. [Google Scholar] [CrossRef] [PubMed]
- Snaidr, V.A.; Lowe, P.M. Phytophotodermatitis from lime juice. Med. J. Aust. 2017, 207, 328. [Google Scholar] [CrossRef] [PubMed]
- Safran, T.; Kanevsky, J.; Ferland-Caron, G.; Mereniuk, A.; Perreault, I.; Lee, J. Blistering phytophotodermatitis of the hands after contact with lime juice. Contact Dermat. 2017, 77, 53–54. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, J.K.; Kohlwes, J. Lime-Induced Phytophotodermatitis. J. Gen. Intern. Med. 2018, 33, 975. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Ma, L. Lime-induced phytophotodermatitis occurred in two family members presented as hyperpigmentation. Photodermatol. Photoimmunol. Photomed. 2021. [Google Scholar] [CrossRef] [PubMed]
- Hamid, R.N.; I Aleisa, A.; Elston, D.M. Pink Patches with a Hyperpigmented Rim. Cutis 2021, 107, 79–86. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| No. | Publication | Age (yr)/Sex | Cutaneous Findings | Location | Contact History |
|---|---|---|---|---|---|
| 1 | Coffman et al. [11] 1985 | 4/F | Hyperpigmentation | Chest, upper back, and wrist | Squeezing lime |
| 2 | Coffman et al. [11] 1985 | 1/M | Hyperpigmentation | Chest and back | Squeezing lime |
| 3 | Wagner et al. [12] 2002 | 6/M | Erythema and bullae | Hand | Squeezing lime |
| 4 | Pomeranz et al. [1] 2007 | 23/F | Erythema and bullae | Back, arm, and hand | Preparing mojitos |
| 3 | Hankinson et al. [13] 2014 | 24/F | Erythema and bullae | Hand | Squeezing lime while cooking |
| 4 | Mioduszewski and Beecker [14] 2015 | 26/F | Erythema and bullae | Hand | Squeezing lime while making sangria |
| 5 | Galvañ-Pérez et al. [15] 2016 | 23/F | Hyperpigmentation | Hand | Preparing mojitos |
| 6 | Galvañ-Pérez et al. [15] 2016 | 25/F | Hyperpigmentation | Hand | Preparing mojitos |
| 7 | Galvañ-Pérez et al. [15] 2016 | 31/F | Hyperpigmentation | Hand | Preparing mojitos |
| 8 | Galvañ-Pérez et al. [15] 2016 | 19/F | Hyperpigmentation | Hand | Preparing mojitos |
| 9 | Galvañ-Pérez et al. [15] 2016 | 41/M | Hyperpigmentation | Hand | Preparing mojitos |
| 10 | Galvañ-Pérez et al. [15] 2016 | 40/M | Hyperpigmentation | Hand | Preparing mojitos |
| 11 | Galvañ-Pérez et al. [15] 2016 | 21/F | Hyperpigmentation | Hand | Preparing mojitos |
| 12 | Galvañ-Pérez et al. [15] 2016 | 14/F | Hyperpigmentation | Hand | Preparing mojitos |
| 13 | Galvañ-Pérez et al. [15] 2016 | 16/F | Hyperpigmentation | Hand | Preparing mojitos |
| 14 | Snaidr and Lowe [16] 2017 | 36/F | Erythema and bullae | Hand | Lime juice |
| 15 | Safran et al. [17] 2017 | 17/F | Erythema and bullae | Hand | Squeezing lime while cooking |
| 16 | Fitzpatrick et al. [18] 2018 | 31/M | Hyperpigmented macules | Hand | Squeezing lime while mixing margaritas |
| 17 | Abugroun A et al. [2] 2019 | 26/M | Erythema and bullae | Hand | Squeezing lime |
| 18 | Wang and Ma [19] 2021 | 6/F | Hyperpigmented macules | Shoulder | Squeezing lime during the hot spring |
| 19 | Wang and Ma [19] 2021 | -/M (No.18′s father) | Hyperpigmented macules | Upper back | Squeezing lime during the hot spring |
| 20 | Hamid et al. [20] 2021 | 25/M | Hyperpigmented macules | Hand | Drinking beer with lime |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, Y.; Lee, S.-H.; Cho, M.; Cho, S.-H.; Lee, J.-D.; Woo, Y.-R.; Kim, H.-S. A Case of Unilateral Hyperpigmentation. Dermato 2021, 1, 26-30. https://doi.org/10.3390/dermato1010004
Han Y, Lee S-H, Cho M, Cho S-H, Lee J-D, Woo Y-R, Kim H-S. A Case of Unilateral Hyperpigmentation. Dermato. 2021; 1(1):26-30. https://doi.org/10.3390/dermato1010004
Chicago/Turabian StyleHan, Yujin, Se-Hoon Lee, Minah Cho, Sang-Hyun Cho, Jeong-Deuk Lee, Yu-Ri Woo, and Hei-Sung Kim. 2021. "A Case of Unilateral Hyperpigmentation" Dermato 1, no. 1: 26-30. https://doi.org/10.3390/dermato1010004
APA StyleHan, Y., Lee, S.-H., Cho, M., Cho, S.-H., Lee, J.-D., Woo, Y.-R., & Kim, H.-S. (2021). A Case of Unilateral Hyperpigmentation. Dermato, 1(1), 26-30. https://doi.org/10.3390/dermato1010004