
Immune Cell–Cytokine Interplay in NSCLC and Melanoma: A Pilot Longitudinal Study of Dynamic Biomarker Interactions

 ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
2.3. Methods and Statistical Analysis
2.4. Study Objectives
3. Results
3.1. Temporal Dynamics of Immune Checkpoint Molecules
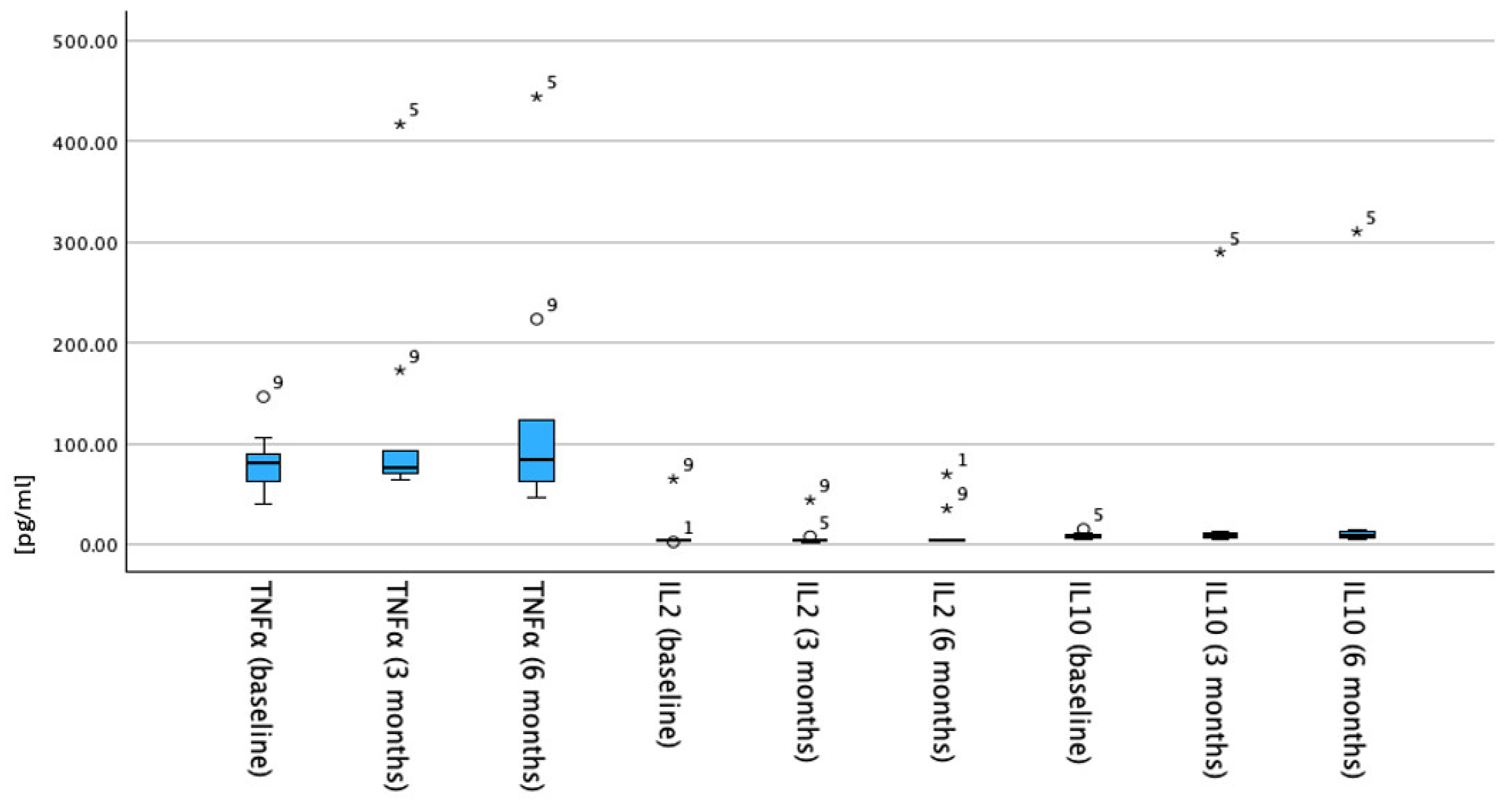
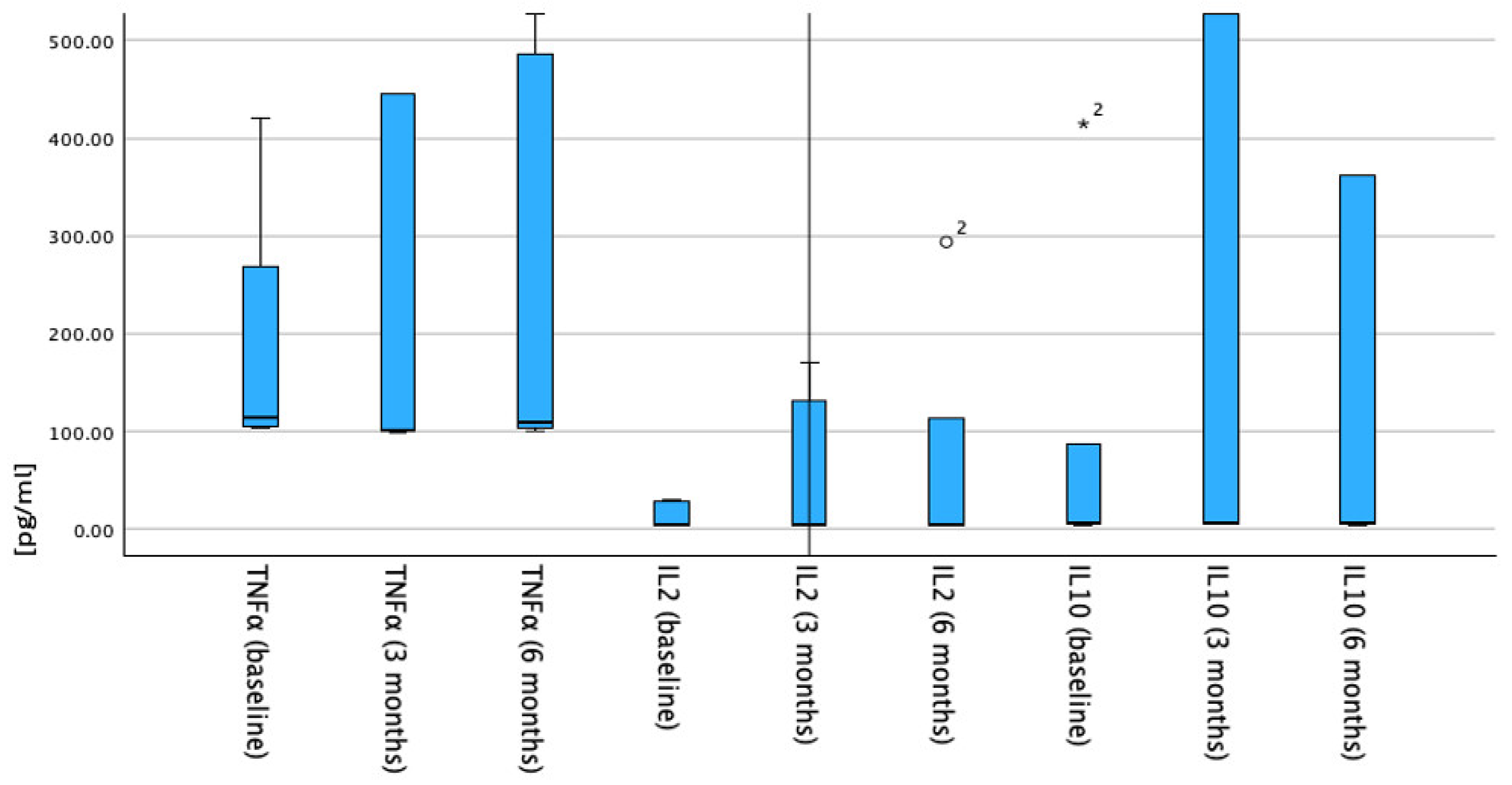
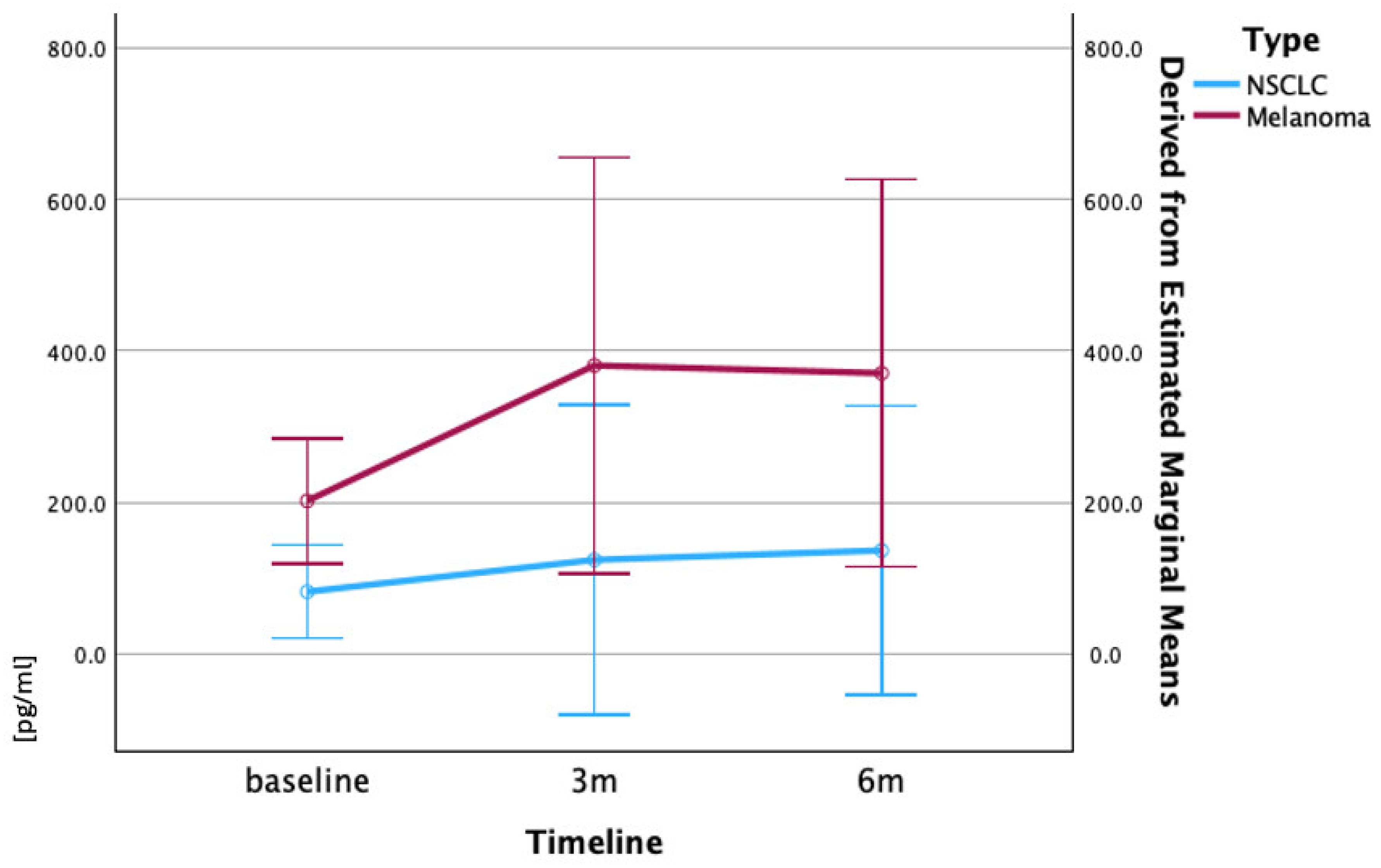
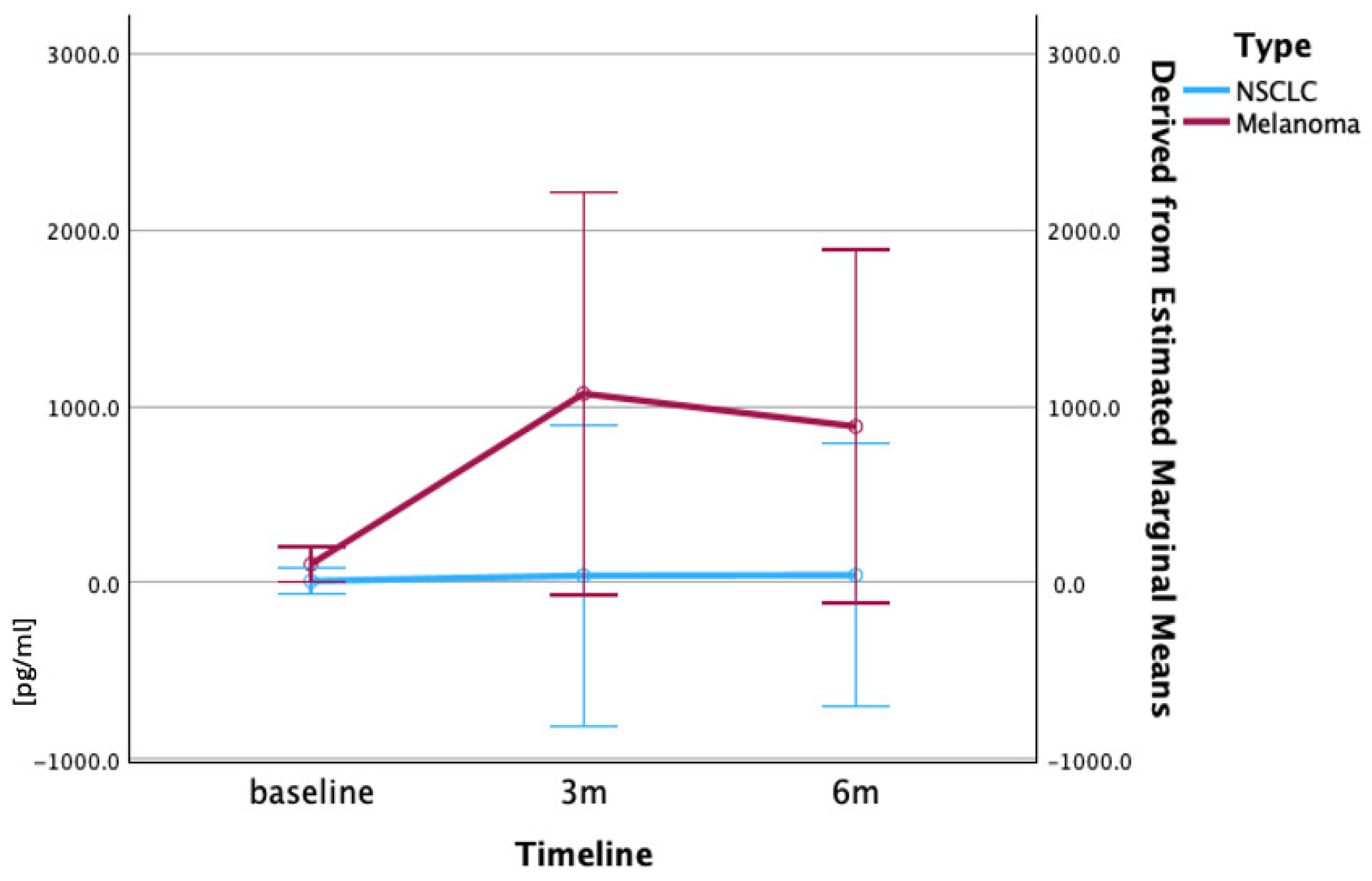
3.2. Temporal Trends of Cytokines Correlated with Survival
3.3. Correlation of Cellular and Humoral Immune Responses
4. Discussion
4.1. Immune Checkpoints: Distinct Roles and Therapeutic Implications
4.2. Biomarker Ratio Analysis and Integrated Immune Assessment
4.3. Cytokine Changes and Survival Correlation
4.4. Correlation Between Immune Profiling and Inflammatory Cytokines
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, B.; Liu, J.; Mo, Y.; Zhang, K.; Huang, B.; Shang, D. CD8+ T cell exhaustion and its regulatory mechanisms in the tumor microenvironment: Key to the success of immunotherapy. Front. Immunol. 2024, 15, 1476904. [Google Scholar] [CrossRef] [PubMed]
- Buchbinder, E.I.; Desai, A. CTLA-4 and PD-1 Pathways: Similarities, Differences, and Implications of Their Inhibition. Am. J. Clin. Oncol. 2016, 39, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Lei, Q.; Wang, D.; Sun, K.; Wang, L.; Zhang, Y. Resistance Mechanisms of Anti-PD1/PDL1 Therapy in Solid Tumors. Front. Cell Dev. Biol. 2020, 8, 672. [Google Scholar] [CrossRef] [PubMed]
- Voss, K.; Larsen, S.E.; Snow, A.L. Metabolic reprogramming and apoptosis sensitivity: Defining the contours of a T cell response. Cancer Lett. 2017, 408, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Raskov, H.; Orhan, A.; Christensen, J.P.; Gögenur, I. Cytotoxic CD8+ T cells in cancer and cancer immunotherapy. Br. J. Cancer 2021, 124, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Dolina, J.S.; Van Braeckel-Budimir, N.; Thomas, G.D.; Salek-Ardakani, S. CD8+ T Cell Exhaustion in Cancer. Front. Immunol. 2021, 12, 715234. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.; Wang, Y.; Fang, L.; Liu, C.; Feng, F.; Liu, L.; Sun, C. T cell senescence: A new perspective on immunotherapy in lung cancer. Front. Immunol. 2024, 15, 1338680. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.; Zhang, B.; Li, B.; Wu, H.; Jiang, M. Cold and hot tumors: From molecular mechanisms to targeted therapy. Signal Transduct. Target. Ther. 2024, 9, 274. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Li, Y.; Zhu, B. T-cell exhaustion in the tumor microenvironment. Cell Death Dis. 2015, 6, e1792. [Google Scholar] [CrossRef] [PubMed]
- Aksoylar, H.I.; Tijaro-Ovalle, N.M.; Boussiotis, V.A.; Patsoukis, N. T Cell Metabolism in Cancer Immunotherapy. Immunometabolism 2020, 2, e200020. Available online: https://journals.lww.com/10.20900/immunometab20200020 (accessed on 31 May 2025). [CrossRef] [PubMed]
- Gangaev, A.; Rozeman, E.A.; Rohaan, M.W.; Isaeva, O.I.; Philips, D.; Patiwael, S.; Berg, J.H.v.D.; Ribas, A.; Schadendorf, D.; Schilling, B.; et al. Differential effects of PD-1 and CTLA-4 blockade on the melanoma-reactive CD8 T cell response. Proc. Natl. Acad. Sci. USA 2021, 118, e2102849118. [Google Scholar] [CrossRef] [PubMed]
- Im, S.J.; Obeng, R.C.; Nasti, T.H.; McManus, D.; Kamphorst, A.O.; Gunisetty, S.; Prokhnevska, N.; Carlisle, J.W.; Yu, K.; Sica, G.L.; et al. Characteristics and anatomic location of PD-1+ TCF1+ stem-like CD8 T cells in chronic viral infection and cancer. Proc. Natl. Acad. Sci. USA 2023, 120, e2221985120. [Google Scholar] [CrossRef] [PubMed]
- Peter, M.E.; Hadji, A.; Murmann, A.E.; Brockway, S.; Putzbach, W.; Pattanayak, A.; Ceppi, P. The role of CD95 and CD95 ligand in cancer. Cell Death Differ. 2015, 22, 549–559. [Google Scholar] [CrossRef] [PubMed]
- Kartikasari, A.E.R.; Huertas, C.S.; Mitchell, A.; Plebanski, M. Tumor-Induced Inflammatory Cytokines and the Emerging Diagnostic Devices for Cancer Detection and Prognosis. Front. Oncol. 2021, 11, 692142. [Google Scholar] [CrossRef] [PubMed]
- Cunha, L.L.; Morari, E.C.; Nonogaki, S.; Marcello, M.A.; Soares, F.A.; Vassallo, J.; Ward, L.S. Interleukin 10 expression is related to aggressiveness and poor prognosis of patients with thyroid cancer. Cancer Immunol. Immunother. 2017, 66, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Yi, M.; Li, T.; Niu, M.; Zhang, H.; Wu, Y.; Wu, K.; Dai, Z. Targeting cytokine and chemokine signaling pathways for cancer therapy. Signal Transduct. Target. Ther. 2024, 9, 176. [Google Scholar] [CrossRef] [PubMed]
- Ren, Z.; Zhang, A.; Sun, Z.; Liang, Y.; Ye, J.; Qiao, J.; Li, B.; Fu, Y.-X. Selective delivery of low-affinity IL-2 to PD-1+ T cells rejuvenates antitumor immunity with reduced toxicity. J. Clin. Investig. 2022, 132, e153604. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wang, Z.; Tan, T. Association of CTLA-4, TNF alpha and IL 10 polymorphisms with susceptibility to hepatocellular carcinoma. Scand. J. Immunol. 2019, 90, e12819. [Google Scholar] [CrossRef] [PubMed]
- Rosner, B. Fundamentals of Biostatistics, 8th ed.; Cengage Learning: Boston, MA, USA, 2016. [Google Scholar]
- Zhang, D.; Zhao, J.; Zhang, Y.; Jiang, H.; Liu, D. Revisiting immune checkpoint inhibitors: New strategies to enhance efficacy and reduce toxicity. Front. Immunol. 2024, 15, 1490129. [Google Scholar] [CrossRef] [PubMed]
- Nagasaki, J.; Ishino, T.; Togashi, Y. Mechanisms of resistance to immune checkpoint inhibitors. Cancer Sci. 2022, 113, 3303–3312. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Chen, T.; Nie, T.Y.; Han, J.; He, Y.; Tang, X.; Zhang, L. Hyperprogressive disease in non-small cell lung cancer after PD-1/PD-L1 inhibitors immunotherapy: Underlying killer. Front. Immunol. 2023, 14, 1200875. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.G.; Kim, K.H.; Pyo, K.H.; Xin, C.F.; Hong, M.H.; Ahn, B.C.; Kim, Y.; Choi, S.J.; Yoon, H.I.; Lee, J.G. Hyperprogressive disease during PD-1/PD-L1 blockade in patients with non-small-cell lung cancer. Ann. Oncol. 2019, 30, 1104–1113. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Huang, S.; Wu, J.; Lu, Y.; Zou, Y.; Zeng, H.; Li, C.; Wang, J.; Zhang, X.; Duan, S. Efficacy and safety of first-line PD-1/PD-L1 inhibitor in combination with CTLA-4 inhibitor in the treatment of patients with advanced non-small cell lung cancer: A systemic review and meta-analysis. Front. Immunol. 2025, 16, 1515027. [Google Scholar] [CrossRef] [PubMed]
- Paulsen, M.; Janssen, O. Pro- and anti-apoptotic CD95 signaling in T cells. Cell Commun. Signal. 2011, 9, 7. [Google Scholar] [CrossRef] [PubMed]
- Risso, V.; Lafont, E.; Le Gallo, M. Therapeutic approaches targeting CD95L/CD95 signaling in cancer and autoimmune diseases. Cell Death Dis. 2022, 13, 248. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Lu, G.; Liu, Y.; Gong, L.; Zheng, X.; Zheng, H.; Gu, W.; Yang, L. Low Infiltration of CD8+ PD-L1+ T Cells and M2 Macrophages Predicts Improved Clinical Outcomes After Immune Checkpoint Inhibitor Therapy in Non-Small Cell Lung Carcinoma. Front. Oncol. 2021, 11, 658690. [Google Scholar] [CrossRef] [PubMed]
- Bai, Z.; Cheng, X.; Ma, T.; Li, G.; Wang, X.; Wang, Z.; Yi, L.; Liu, Z. CD8+ T cells infiltrating into tumors were controlled by immune status of pulmonary lymph nodes and correlated with non-small cell lung cancer (NSCLC) patients’ prognosis treated with chemoimmunotherapy. Lung Cancer 2024, 197, 107991. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Li, C.; Cai, X.; Xie, Z.; Zhou, L.; Cheng, B.; Zhong, R.; Xiong, S.; Li, J.; Chen, Z.; et al. The association between CD8+ tumor-infiltrating lymphocytes and the clinical outcome of cancer immunotherapy: A systematic review and meta-analysis. eClinicalMedicine 2021, 41, 101134. [Google Scholar] [CrossRef] [PubMed]
- Tumeh, P.C.; Harview, C.L.; Yearley, J.H.; Shintaku, I.P.; Taylor, E.J.M.; Robert, L.; Chmielowski, B.; Spasic, M.; Henry, G.; Ciobanu, V. PD-1 blockade induces responses by inhibiting adaptive immune resistance. Nature 2014, 515, 568–571. [Google Scholar] [CrossRef] [PubMed]
- Topalian, S.L.; Hodi, F.S.; Brahmer, J.R.; Gettinger, S.N.; Smith, D.C.; McDermott, D.F.; Powderly, J.D.; Carvajal, R.D.; Sosman, J.A.; Atkins, M.B. Safety, Activity, and Immune Correlates of Anti–PD-1 Antibody in Cancer. N. Engl. J. Med. 2012, 366, 2443–2454. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, A.; Saleh, S. Checkpoint inhibitors for malignant melanoma: A systematic review and meta-analysis. Clin. Cosmet. Investig. Dermatol. 2017, 10, 325–339. [Google Scholar] [CrossRef] [PubMed]
- Peter, M.E.; Budd, R.C.; Desbarats, J.; Hedrick, S.M.; Hueber, A.O.; Newell, M.K.; Owen, L.B.; Pope, R.M.; Tschopp, J.; Wajant, H. The CD95 Receptor: Apoptosis Revisited. Cell 2007, 129, 447–450. [Google Scholar] [CrossRef] [PubMed]
- Hossen, M.M.; Ma, Y.; Yin, Z.; Xia, Y.; Du, J.; Huang, J.Y.; Huang, J.J.; Zou, L.; Ye, Z.; Huang, Z. Current understanding of CTLA-4: From mechanism to autoimmune diseases. Front. Immunol. 2023, 14, 1198365. [Google Scholar] [CrossRef] [PubMed]
- Gramantieri, L.; Montagner, A.; Arleo, A.; Suzzi, F.; Bassi, C.; Tovoli, F.; Bruccoleri, M.; Alimenti, E.; Fornari, F.; Iavarone, M.; et al. Early CTLA4 increase in CD45+ blood cells: An emerging biomarker of atezolizumab–bevacizumab resistance and worse survival in advanced hepatocarcinoma. ESMO Open 2025, 10, 104289. [Google Scholar] [CrossRef] [PubMed]
- Ascierto, M.L.; Makohon-Moore, A.; Lipson, E.J.; Taube, J.M.; McMiller, T.L.; Berger, A.E.; Fan, J.; Kaunitz, G.J.; Cottrell, T.R.; Kohutek, Z.A.; et al. Transcriptional Mechanisms of Resistance to Anti–PD-1 Therapy. Clin. Cancer Res. 2017, 23, 3168–3180. [Google Scholar] [CrossRef] [PubMed]
- Chai, Q.Q.; Du, J.Y.; Zhu, J.; Wu, B. The Differences in the Safety and Tolerability of Immune Checkpoint Inhibitors as Treatment for Non–Small Cell Lung Cancer and Melanoma: Network Meta-Analysis and Systematic Review. Front. Pharmacol. 2019, 10, 1260. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.M. First-line combination immunotherapy for metastatic non-small cell lung cancer. J. Chin. Med. Assoc. 2020, 83, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Sundar, R.; Cho, B.C.; Brahmer, J.R.; Soo, R.A. Nivolumab in NSCLC: Latest evidence and clinical potential. Ther. Adv. Med. Oncol. 2015, 7, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Niyongere, S.; Saltos, A.; Gray, J.E. Immunotherapy combination strategies (non-chemotherapy) in non-small cell lung cancer. J. Thorac. Dis. 2018, 10, S433–S450. [Google Scholar] [CrossRef] [PubMed]
- Datar, I.; Sanmamed, M.F.; Wang, J.; Henick, B.S.; Choi, J.; Badri, T.; Dong, W.; Mani, N.; Toki, M.; Mejías, L.D. Expression Analysis and Significance of PD-1, LAG-3, and TIM-3 in Human Non–Small Cell Lung Cancer Using Spatially Resolved and Multiparametric Single-Cell Analysis. Clin. Cancer Res. 2019, 25, 4663–4673. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, A.B.; Barros, E.; Silva, M.J.; Evangelista, G.F.D.B.; Galdino, N.A.D.L.; Kuil, L.D.M.; Santos, I.P.; Morais, K.L.P.; Cavalcanti, C.M.; Moredo, L.F.; et al. Immune mechanisms and predictive biomarkers related to neoadjuvant immunotherapy response in stage III melanoma. Heliyon 2024, 10, e32624. [Google Scholar] [CrossRef] [PubMed]
- Chow, A.; Perica, K.; Klebanoff, C.A.; Wolchok, J.D. Clinical implications of T cell exhaustion for cancer immunotherapy. Nat. Rev. Clin. Oncol. 2022, 19, 775–790. [Google Scholar] [CrossRef] [PubMed]
- Jacquelot, N.; Roberti, M.P.; Enot, D.P.; Rusakiewicz, S.; Ternès, N.; Jegou, S.; Woods, D.M.; Sodré, A.L.; Hansen, M.; Meirow, Y.; et al. Predictors of responses to immune checkpoint blockade in advanced melanoma. Nat. Commun. 2017, 8, 592. [Google Scholar] [CrossRef] [PubMed]
- Dyck, L.; Mills, K.H.G. Immune checkpoints and their inhibition in cancer and infectious diseases. Eur. J. Immunol. 2017, 47, 765–779. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.C.; Levine, J.H.; Cogdill, A.P.; Zhao, Y.; Anang, N.A.A.S.; Andrews, M.C.; Sharma, P.; Wang, J.; Wargo, J.A.; Pe’Er, D.; et al. Distinct Cellular Mechanisms Underlie Anti-CTLA-4 and Anti-PD-1 Checkpoint Blockade. Cell 2017, 170, 1120–1133.e17. [Google Scholar] [CrossRef] [PubMed]
- Pardoll, D.M. The blockade of immune checkpoints in cancer immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef] [PubMed]
- Landskron, G.; De La Fuente, M.; Thuwajit, P.; Thuwajit, C.; Hermoso, M.A. Chronic Inflammation and Cytokines in the Tumor Microenvironment. J. Immunol. Res. 2014, 2014, 149185. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, S.; Verma, A.K.; Dev, K.; Goyal, Y.; Bhatt, D.; Alsahli, M.A.; Rahmani, A.H.; Almatroudi, A.; Almatroodi, S.A.; Alrumaihi, F.; et al. Role of Cytokines and Chemokines in NSCLC Immune Navigation and Proliferation. Oxid. Med. Cell Longev. 2021, 2021, 5563746. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhou, F.; Zhao, C.; Cheng, L.; Zhou, C.; Qiao, M.; Li, X.; Chen, X. Interleukin-10 Is a Promising Marker for Immune-Related Adverse Events in Patients With Non-Small Cell Lung Cancer Receiving Immunotherapy. Front. Immunol. 2022, 13, 840313. [Google Scholar] [CrossRef] [PubMed]
- Kucera, R.; Topolcan, O.; Treskova, I.; Kinkorova, J.; Windrichova, J.; Fuchsova, R.; Svobodova, S.; Treska, V.; Babuska, V.; Novak, J.; et al. Evaluation of IL-2, IL-6, IL-8 and IL-10 in Malignant Melanoma Diagnostics. Anticancer Res. 2015, 35, 3537–3541. [Google Scholar] [PubMed]
- Anichini, A.; Tassi, E.; Grazia, G.; Mortarini, R. The non-small cell lung cancer immune landscape: Emerging complexity, prognostic relevance and prospective significance in the context of immunotherapy. Cancer Immunol. Immunother. 2018, 67, 1011–1022. [Google Scholar] [CrossRef] [PubMed]
- Lauss, M.; Phung, B.; Borch, T.H.; Harbst, K.; Kaminska, K.; Ebbesson, A.; Hedenfalk, I.; Yuan, J.; Nielsen, K.; Ingvar, C.; et al. Molecular patterns of resistance to immune checkpoint blockade in melanoma. Nat. Commun. 2024, 15, 3075. [Google Scholar] [CrossRef] [PubMed]
- Cuevas, E.S.; Mouret, S.; Vayssière, G.; Kerboua, S.; Girard, P.; Molens, J.P.; Manceau, M.; Charles, J.; Saas, P.; Aspord, C.; et al. Circulating immune landscape in melanoma patients undergoing anti-PD1 therapy reveals key immune features according to clinical response to treatment. Front. Immunol. 2024, 15, 1507938. [Google Scholar] [CrossRef] [PubMed]
- Carbone, D.P.; Gandara, D.R.; Antonia, S.J.; Zielinski, C.; Paz-Ares, L. Non–Small-Cell Lung Cancer: Role of the Immune System and Potential for Immunotherapy. J. Thorac. Oncol. 2015, 10, 974–984. [Google Scholar] [CrossRef] [PubMed]
- Montfort, A.; Colacios, C.; Levade, T.; Andrieu-Abadie, N.; Meyer, N.; Ségui, B. The TNF Paradox in Cancer Progression and Immunotherapy. Front. Immunol. 2019, 10, 1818. [Google Scholar] [CrossRef] [PubMed]
- Bertrand, F.; Montfort, A.; Marcheteau, E.; Imbert, C.; Gilhodes, J.; Filleron, T.; Rochaix, P.; Andrieu-Abadie, N.; Levade, T.; Meyer, N.; et al. TNFα blockade overcomes resistance to anti-PD-1 in experimental melanoma. Nat. Commun. 2017, 8, 2256. [Google Scholar] [CrossRef] [PubMed]
- Gong, K.; Guo, G.; Beckley, N.; Zhang, Y.; Yang, X.; Sharma, M.; Habib, A.A. Tumor necrosis factor in lung cancer: Complex roles in biology and resistance to treatment. Neoplasia 2021, 23, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Salkeni, M.A.; Naing, A. Interleukin-10 in cancer immunotherapy: From bench to bedside. Trends Cancer. 2023, 9, 716–725. [Google Scholar] [CrossRef] [PubMed]
- Somasundaram, R.; Herlyn, M.; Wagner, S.N. The Role of Tumor Microenvironment in Melanoma Therapy Resistance. Melanoma Manag. 2016, 3, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Carlini, V.; Noonan, D.M.; Abdalalem, E.; Goletti, D.; Sansone, C.; Calabrone, L.; Albini, A. The multifaceted nature of IL-10: Regulation, role in immunological homeostasis and its relevance to cancer, COVID-19 and post-COVID conditions. Front. Immunol. 2023, 14, 1161067. [Google Scholar] [CrossRef] [PubMed]
- Yin, Y.; Sakakibara, R.; Honda, T.; Kirimura, S.; Daroonpan, P.; Kobayashi, M.; Ando, K.; Ujiie, H.; Kato, T.; Kaga, K.; et al. High density and proximity of CD8+ T cells to tumor cells are correlated with better response to nivolumab treatment in metastatic pleural mesothelioma. Thorac. Cancer. 2023, 14, 1991–2000. [Google Scholar] [CrossRef] [PubMed]
- Xiong, Y.; Neskey, D.M.; Horton, J.D.; Paulos, C.M.; Knochelmann, H.M.; Armeson, K.E.; Young, M.R.I. Immunological effects of nivolumab immunotherapy in patients with oral cavity squamous cell carcinoma. BMC Cancer. 2020, 20, 229. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Zhu, Z.; Lan, Y.; Duan, S.; Zhu, Z.; Zhang, X.; Li, G.; Qu, H.; Feng, Y.; Cai, H.; et al. Development and Validation of a CD8+ T Cell Infiltration-Related Signature for Melanoma Patients. Front. Immunol. 2021, 12, 659444. [Google Scholar] [CrossRef] [PubMed]
- Singla, N.; Nirschl, T.R.; Obradovic, A.Z.; Shenderov, E.; Lombardo, K.; Liu, X.; Pons, A.; Zarif, J.C.; Rowe, S.P.; Trock, B.J.; et al. Immunomodulatory response to neoadjuvant nivolumab in non-metastatic clear cell renal cell carcinoma. Sci. Rep. 2024, 14, 1458. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.; Li, X.; Yang, Y.; Shi, H.; Wang, S.; Gao, M. Serum cytokines and neutrophil-to-lymphocyte ratio as predictive biomarkers of benefit from PD-1 inhibitors in gastric cancer. Front. Immunol. 2023, 14, 1274431. [Google Scholar] [CrossRef] [PubMed]
- Ottonello, S.; Genova, C.; Cossu, I.; Fontana, V.; Rijavec, E.; Rossi, G.; Biello, F.; Bello, M.G.D.; Tagliamento, M.; Alama, A.; et al. Association Between Response to Nivolumab Treatment and Peripheral Blood Lymphocyte Subsets in Patients With Non-small Cell Lung Cancer. Front. Immunol. 2020, 11, 125. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Li, Y. Predictive value of co-expression patterns of immune checkpoint molecules for clinical outcomes of hematological malignancies. Chin. J. Cancer Res. 2023, 35, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Tarantino, G.; Severgnini, M.; Baginska, J.; Giobbie-Hurder, A.; Weirather, J.L.; Manos, M.; Russell, J.D.; Pfaff, K.L.; Rodig, S.J.; et al. Circulating cytokine associations with clinical outcomes in melanoma patients treated with combination nivolumab plus ipilimumab. OncoImmunology 2025, 14, 2432723. [Google Scholar] [CrossRef] [PubMed]
- Gérard, A.; Doyen, J.; Cremoni, M.; Bailly, L.; Zorzi, K.; Ruetsch-Chelli, C.; Brglez, V.; Picard-Gauci, A.; Troin, L.; Esnault, V.L.; et al. Baseline and early functional immune response is associated with subsequent clinical outcomes of PD-1 inhibition therapy in metastatic melanoma patients. J. Immunother. Cancer. 2021, 9, e002512. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Median (Min–Max) | Additional Details |
|---|---|---|
| Age at study entry (years) | 57 (30–77) | |
| Sex | 50% male, 50% female | 8 males, 8 females |
| Cancer type | 56% NSCLC, 44% melanoma | 9 NSCLC, 7 melanoma |
| Smokers | 62.5% | 7 NSCLC, 3 melanoma |
| Nivolumab cycles | 20 (8–114) | |
| Metastatic line setting of nivolumab | 2 (1–4) | |
| Subsequent treatments | 7/16 (44%) had none | Most common: Docetaxel (3); others: Gemcitabine, Carboplatin+VP16, Navelbine, Ipilimumab, Dacarbazine+Adriamycine, Dabrafenib+Trametinib |
| Overall survival (months) | 22.7 (6.1–87.4) |
| No of Tests | Patient | Type of cancer | Timeline | PD1(%) | CD95(%) | CD8 (%) | CTLA-4 (%) | PD1/CD95 (%) | CD8/CTLA4 (%) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | NSCLC | 0 | 0.8 | 47.2 | 37.3 | 0.5 | 4 | 1 | |
| 2 | 1 | 1 | 0.2 | 57.9 | 43.4 | 0.2 | 6.3 | 0.4 | |
| 3 | 2 | 1 | 45.9 | 37.2 | 0.1 | 3.1 | 0.7 | ||
| 4 | NSCLC | 0 | 1 | 48.4 | 18.2 | 0.4 | 6.2 | 0.6 | |
| 5 | 2 | 1 | 0.4 | 51.3 | 22 | 1 | 7.2 | 1.2 | |
| 6 | 2 | 5.3 | 20.1 | 21.8 | 1.4 | 6.5 | 1.4 | ||
| 7 | NSCLC | 0 | 2 | 36.1 | 27.5 | 0.3 | 12.3 | 0.3 | |
| 8 | 3 | 1 | 0.8 | 46.5 | 28.4 | 0.5 | 9 | 0.3 | |
| 9 | 2 | 74.7 | 4.4 | 26.7 | 17.7 | 4.1 | 9 | ||
| 10 | NSCLC | 0 | 3.8 | 21.5 | 30.6 | 0.2 | 3.2 | 0.2 | |
| 11 | 4 | 1 | 2.2 | 42.1 | 38.1 | 0.1 | 8.6 | 0.1 | |
| 12 | 2 | 1.4 | 5.6 | 43.2 | 0 | 3.6 | 0.5 | ||
| 13 | NSCLC | 0 | 1.4 | 43.7 | 28.2 | 1.2 | 2.6 | 1.4 | |
| 14 | 5 | 1 | 0.5 | 55.7 | 44.2 | 0.1 | 1.1 | 0.3 | |
| 15 | 2 | 0.6 | 50.2 | 40 | 0.2 | 2.1 | 0.2 | ||
| 16 | NSCLC | 0 | 1.5 | 28.8 | 22.5 | 0.1 | 2.7 | 0.2 | |
| 17 | 6 | 1 | 1.8 | 26 | 25.1 | 0.3 | 1.5 | 0.3 | |
| 18 | 2 | 0.8 | 28.4 | 19.2 | 0.2 | 1.3 | 0.1 | ||
| 19 | NSCLC | 0 | 1.1 | 52.6 | 35.3 | 0.1 | 3.3 | 0.5 | |
| 20 | 7 | 1 | 0.4 | 57.5 | 42.8 | 0.2 | 1.1 | 0.2 | |
| 21 | 2 | 0.2 | 58.8 | 33.8 | 0.4 | 0.7 | 0.4 | ||
| 22 | NSCLC | 0 | 0.1 | 63.1 | 33.1 | 0.3 | 1.1 | 0.1 | |
| 23 | 8 | 1 | 0.3 | 59.4 | 40.9 | 0.3 | 0.9 | 0.6 | |
| 24 | 2 | 0.4 | 65 | 43.6 | 0.1 | 3.6 | 0.1 | ||
| 25 | NSCLC | 0 | 0.9 | 39.5 | 21 | 0.1 | 6.7 | 0.2 | |
| 26 | 9 | 1 | 0.4 | 53.5 | 21.5 | 0.2 | 1.1 | 0.4 | |
| 27 | 2 | 1.3 | 40.4 | 21.6 | 0.2 | 6.2 | 0.2 |
| No of Tests | Patient | Type of Cancer | Timeline | PD1(%) | CD95(%) | CD8 (%) | CTLA-4 (%) | PD1/CD95 (%) | CD8/CTLA4(%) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 0 | 5.1 | 29.8 | 19.9 | 1.1 | 19 | 0.6 | ||
| 2 | 1 | melanoma | 1 | 2.7 | 37.8 | 21.2 | 0.4 | 11.5 | 0.4 |
| 3 | 2 | 4.2 | 34.2 | 16 | 0.4 | 16.9 | 0.4 | ||
| 4 | 0 | 3.5 | 28.6 | 19.5 | 0.5 | 16.9 | 0.6 | ||
| 5 | 2 | melanoma | 1 | 4.6 | 28.5 | 21.9 | 0.5 | 11.1 | 0.4 |
| 6 | 2 | 3.2 | 33.5 | 24.9 | 0.4 | 11 | 0.6 | ||
| 7 | 3 | melanoma | 0 | 5.4 | 30.8 | 23 | 0.4 | 15.4 | 0.5 |
| 8 | 1 | 2.6 | 32.4 | 29 | 0.4 | 9.9 | 0.5 | ||
| 9 | 0 | 2 | 29.4 | 20.8 | 0.6 | 11.2 | 0.3 | ||
| 10 | 4 | melanoma | 1 | 1.2 | 34.9 | 27.6 | 0.3 | 8.2 | 0.4 |
| 11 | 2 | 3.9 | 30.1 | 23.2 | 0.7 | 12.3 | 1.4 | ||
| 12 | 0 | 1.6 | 25.9 | 23.8 | 0.1 | 7.2 | 0.2 | ||
| 13 | 5 | melanoma | 1 | 2.3 | 32.9 | 26.2 | 0.3 | 2.7 | 0.6 |
| 14 | 2 | 3.1 | 29 | 23.7 | 0.4 | 9 | 0.4 | ||
| 15 | 0 | 4.3 | 29.4 | 35.7 | 0.4 | 18.3 | 2.7 | ||
| 16 | 6 | melanoma | 1 | 3.5 | 31.6 | 29.7 | 0.7 | 13.9 | 2 |
| 17 | 2 | 2.9 | 35.8 | 38.8 | 0.2 | 11.5 | 0.7 | ||
| 18 | 7 | melanoma | 0 | 2.1 | 22.9 | 23.3 | 0.2 | 13 | 0.3 |
| 19 | 1 | 1.6 | 28.3 | 20.1 | 0.2 | 11.4 | 0.4 |
| IL2 | Baseline-IL2 (pg/mL) | 3 Months-IL2 | 6 Months-IL2 | Survival in Months | ||
|---|---|---|---|---|---|---|
| Spearman’s rho | Baseline-TNFα pg/mL | Correlation Coefficient | 0.891 ** | 0.879 ** | 0.491 | 0.553 * |
| Sig. (2-tailed) | <0.001 | <0.001 | 0.074 | 0.026 | ||
| Baseline-IL2 (pg/mL) | Correlation Coefficient | 1.000 | 0.902 ** | 0.421 | 0.692 ** | |
| Sig. (2-tailed) | 0.0 | <0.001 | 0.134 | 0.003 | ||
| Baseline-IL10 (pg/mL) | Correlation Coefficient | 0.077 | 0.374 | 0.147 | 0.376 | |
| Sig. (2-tailed) | 0.778 | 0.154 | 0.615 | 0.151 | ||
| 3 months-TNFα | Correlation Coefficient | 0.876 ** | 0.915 ** | 0.444 | 0.650 ** | |
| Sig. (2-tailed) | <0.001 | <0.001 | 0.111 | 0.006 | ||
| 3 months-IL2 | Correlation Coefficient | 0.902 ** | 1.000 | 0.418 | 0.762 ** | |
| Sig. (2-tailed) | <0.001 | 0.0 | 0.137 | <0.001 | ||
| 3 months-IL10 | Correlation Coefficient | 0.169 | 0.337 | 0.416 | 0.295 | |
| Sig. (2-tailed) | 0.530 | 0.201 | 0.139 | 0.268 | ||
| 6 months-TNFα | Correlation Coefficient | 0.713 ** | 0.842 ** | 0.488 | 0.670 ** | |
| Sig. (2-tailed) | 0.004 | <0.001 | 0.076 | 0.009 | ||
| 6 months-IL2 | Correlation Coefficient | 0.421 | 0.418 | 1.000 | 0.356 | |
| Sig. (2-tailed) | 0.134 | 0.137 | 0.0 | 0.211 | ||
| 6 months-IL10 | Correlation Coefficient | 0.150 | 0.295 | 0.361 | 0.064 | |
| Sig. (2-tailed) | 0.609 | 0.306 | 0.204 | 0.828 | ||
| Survival in months | Correlation Coefficient | 0.692 ** | 0.762 ** | 0.356 | 1.000 | |
| Sig. (2-tailed) | 0.003 | <0.001 | 0.211 | 0.0 | ||
| TNF-α | Baseline-TNFα pg/mL | 3 Months-TNFα | 6 Months-TNFα | Survival in Months | ||
|---|---|---|---|---|---|---|
| Spearman’s rho | Baseline-TNFα pg/mL | Correlation Coefficient | 1.000 | 0.937 ** | 0.880 ** | 0.553 * |
| Sig. (2-tailed) | 0.0 | <0.001 | <0.001 | 0.026 | ||
| Baseline-IL2 (pg/mL) | Correlation Coefficient | 0.891 ** | 0.876 ** | 0.713 ** | 0.692 ** | |
| Sig. (2-tailed) | <0.001 | <0.001 | 0.004 | 0.003 | ||
| Baseline-IL10 (pg/mL) | Correlation Coefficient | 0.286 | 0.429 | 0.380 | 0.376 | |
| Sig. (2-tailed) | 0.284 | 0.097 | 0.180 | 0.151 | ||
| 3 months-TNFα | Correlation Coefficient | 0.937 ** | 1.000 | 0.855 ** | 0.650 ** | |
| Sig. (2-tailed) | <0.001 | 0.0 | <0.001 | 0.006 | ||
| 3 months-IL2 | Correlation Coefficient | 0.879 ** | 0.915 ** | 0.842 ** | 0.762 ** | |
| Sig. (2-tailed) | <0.001 | <0.001 | <0.001 | <0.001 | ||
| 3 months-IL10 | Correlation Coefficient | 0.338 | 0.409 | 0.392 | 0.295 | |
| Sig. (2-tailed) | 0.201 | 0.115 | 0.166 | 0.268 | ||
| 6 months-TNFα | Correlation Coefficient | 0.880 ** | 0.855 ** | 1.000 | 0.670 ** | |
| Sig. (2-tailed) | <0.001 | <0.001 | 0.0 | 0.009 | ||
| 6 months-IL2 | Correlation Coefficient | 0.491 | 0.444 | 0.488 | 0.356 | |
| Sig. (2-tailed) | 0.074 | 0.111 | 0.076 | 0.211 | ||
| 6 months-IL10 | Correlation Coefficient | 0.317 | 0.310 | 0.482 | 0.064 | |
| Sig. (2-tailed) | 0.269 | 0.280 | 0.081 | 0.828 | ||
| Survival in months | Correlation Coefficient | 0.553 * | 0.650 ** | 0.670 ** | 1.000 | |
| Sig. (2-tailed) | 0.026 | 0.006 | 0.009 | 0.0 | ||
| IL10 | Baseline-IL10 (pg/mL) | 3 Months-IL10 | 6 Months-IL10 | Survival in Months | ||
|---|---|---|---|---|---|---|
| Spearman’s rho | Baseline-TNFα pg/mL | Correlation Coefficient | 0.286 | 0.338 | 0.317 | 0.553 * |
| Sig. (2-tailed) | 0.284 | 0.201 | 0.269 | 0.026 | ||
| Baseline-IL2 (pg/mL) | Correlation Coefficient | 0.077 | 0.169 | 0.150 | 0.692 ** | |
| Sig. (2-tailed) | 0.778 | 0.530 | 0.609 | 0.003 | ||
| Baseline-IL10 (pg/mL) | Correlation Coefficient | 1.000 | 0.769 ** | 0.623 * | 0.376 | |
| Sig. (2-tailed) | 0.0 | <0.001 | 0.017 | 0.151 | ||
| 3 months-TNFα | Correlation Coefficient | 0.429 | 0.409 | 0.310 | 0.650 ** | |
| Sig. (2-tailed) | 0.097 | 0.115 | 0.280 | 0.006 | ||
| 3 months-IL2 | Correlation Coefficient | 0.374 | 0.337 | 0.295 | 0.762 ** | |
| Sig. (2-tailed) | 0.154 | 0.201 | 0.306 | <0.001 | ||
| 3 months-IL10 | Correlation Coefficient | 0.769 ** | 1.000 | 0.894 ** | 0.295 | |
| Sig. (2-tailed) | <0.001 | 0.0 | <0.001 | 0.268 | ||
| 6 months-TNFα | Correlation Coefficient | 0.380 | 0.392 | 0.482 | 0.670 ** | |
| Sig. (2-tailed) | 0.180 | 0.166 | 0.081 | 0.009 | ||
| 6 months-IL2 | Correlation Coefficient | 0.147 | 0.416 | 0.361 | 0.356 | |
| Sig. (2-tailed) | 0.615 | 0.139 | 0.204 | 0.211 | ||
| 6 months-IL10 | Correlation Coefficient | 0.623 * | 0.894 ** | 1.000 | 0.064 | |
| Sig. (2-tailed) | 0.017 | <0.001 | 0.0 | 0.828 | ||
| Survival in months | Correlation Coefficient | 0.376 | 0.295 | 0.064 | 1.000 | |
| Sig. (2-tailed) | 0.151 | 0.268 | 0.828 | 0.0 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grecea-Balaj, A.M.; Soritau, O.; Brie, I.; Perde-Schrepler, M.; Virág, P.; Todor, N.; Ciuleanu, T.E.; Cismaru, C.A. Immune Cell–Cytokine Interplay in NSCLC and Melanoma: A Pilot Longitudinal Study of Dynamic Biomarker Interactions. Immuno 2025, 5, 29. https://doi.org/10.3390/immuno5030029
Grecea-Balaj AM, Soritau O, Brie I, Perde-Schrepler M, Virág P, Todor N, Ciuleanu TE, Cismaru CA. Immune Cell–Cytokine Interplay in NSCLC and Melanoma: A Pilot Longitudinal Study of Dynamic Biomarker Interactions. Immuno. 2025; 5(3):29. https://doi.org/10.3390/immuno5030029
Chicago/Turabian StyleGrecea-Balaj, Alina Miruna, Olga Soritau, Ioana Brie, Maria Perde-Schrepler, Piroska Virág, Nicolae Todor, Tudor Eliade Ciuleanu, and Cosmin Andrei Cismaru. 2025. "Immune Cell–Cytokine Interplay in NSCLC and Melanoma: A Pilot Longitudinal Study of Dynamic Biomarker Interactions" Immuno 5, no. 3: 29. https://doi.org/10.3390/immuno5030029
APA StyleGrecea-Balaj, A. M., Soritau, O., Brie, I., Perde-Schrepler, M., Virág, P., Todor, N., Ciuleanu, T. E., & Cismaru, C. A. (2025). Immune Cell–Cytokine Interplay in NSCLC and Melanoma: A Pilot Longitudinal Study of Dynamic Biomarker Interactions. Immuno, 5(3), 29. https://doi.org/10.3390/immuno5030029