1. Introduction
Anorexia nervosa (AN) is defined as a serious mental health disorder characterised by low body weight and restrictive eating behaviours that are maintained by disturbances in self-perceived weight and shape, and an intense fear of weight gain [
1]. AN is widely reported to have the highest mortality rate of any mental health disorder [
2] with the two most common causes of death being physical deterioration due to sustained low weight [
3,
4] and suicide [
2,
5].
The experience of AN through the lens of the person with a lived experience has multiple meanings including being perceived as concurrently harmful (for example, posing significant health risks) and helpful (for example, numbing unwanted thoughts or emotions) [
6]. In addition to complicating the course of AN, childhood trauma and abuse have been found to compromise treatment outcomes [
7,
8]. A notable proportion (21–59%) of individuals diagnosed with AN report a history of trauma, including physical, emotional, or sexual abuse [
9,
10], with more severe ED symptoms being associated with higher post-traumatic stress disorder (PTSD) symptomatology [
11]. Further, in the US national comorbidity survey-replication study, all the women reporting a lifetime history of AN (
n = 18) reported trauma (any form) and 71.6% reported interpersonal trauma exposure [
12]. In research in Italy, the majority of individuals being treated in an inpatient setting (95.2% under the age of 25 [
13]; 66.7% of total [
14]) reported lifetime interpersonal trauma events.
Social support has been found to be a significant predictor for PTSD symptomatology in AN [
11] and difficulties with emotion regulation may mediate this relationship [
15]. A history of trauma and/or PTSD have been found to be associated with more severe ED symptoms post-treatment and treatment attrition [
16]. Although there is preliminary evidence for the effectiveness of ED-specific treatments [
16] and CBT for trauma [
15] in individuals who have a history of AN and trauma/PTSD, there is a need for integrated treatment approaches that more comprehensively address the sequelae of eating disorders, including AN, and trauma-related symptomatology [
16,
17,
18,
19]. It is likely that the relationships between trauma experiences and AN are bi-directional, etiological, and can increase AN symptomatology and/or hamper treatment and that there exists a complex inter-relationship between these.
To better understand the complexities of a combined AN and trauma profile, some researchers have utilised a qualitative research approach, seeking to provide novel insights into trauma-related factors that are maintaining AN through exploring the experiences of people with a lived experience [
18]. These researchers adopted a broad perspective on what constitutes trauma, recognising the diversity and subjectivity of traumatic experiences and their complex inter-relationships with AN [
20]. In doing so, they capture “big T traumas” which are covered in medical definitions of trauma (i.e., direct or indirect exposure to serious injury, death, or sexual violence) [
21] as well as “hidden traumata” or “little t trauma” such as grief, loss, bullying, critical parenting, neglect, and emotional abuse [
22] (p. xxii).
Following this approach, the research has elucidated a complex relationship between AN and trauma, whereby AN is used as a way of coping with the emotional and psychological effects of trauma and abuse [
18]. While the specific functions of AN vary from person to person, one key theme present in the literature is its function in managing abuse-related emotions [
23,
24,
25], such that difficulties with emotional regulation are theorised to be a key etiological pathway in the development of AN after trauma [
26]. Emotions experienced during abuse—such as guilt and shame—are particularly difficult to regulate due to their sheer overwhelming and foreign nature for which the experiencing person (or child) did not have the resources to deal with them [
27]. In connection with this, AN has been found to function as a form of self-punishment and atonement for abuse [
18,
24,
28], which results from shame and blame being internalised—a process that is perpetuated by societal and perpetrator victim-blaming attitudes as well as a cognitive tendency for survivors to make sense of the abuse by developing a system of beliefs around their own inherent “badness” [
27,
29]. To mitigate against these problematic identities, a valuing of AN itself may also go some way towards reinstating a sense of self-worth. This is through the AN experience being central to the person’s sense of ‘ideal identity’, perceived to be consistent with their ‘real self’, and valued as their ‘best self’ [
30,
31].
In addition, AN is perceived by some to serve interpersonal functions including protecting the self from further abuse by creating an emaciated body that is unwanted, ‘ugly’, or ‘invisible’ to perpetrators [
18,
32,
33,
34]. These functions may be related to the need to regain a sense of relational safety that was lost during abuse, as well as internalised victim blaming attitudes that conflate fault for abuse with one’s physical appearance [
34]. On the other hand, AN may also be described as serving psychological protection by offering a ‘safe world’ that individuals can retreat into for respite from trauma-related internal and external turmoil [
35,
36].
These perceived benefits of AN are counteracted by a number of significant negative consequences, resulting in an intrapsychic tension between AN as both helpful and harmful [
6]. Of note are the debilitating health conditions arising from starvation, which contribute to AN having the highest mortality rate of any mental health disorder [
2,
3]. Furthermore, a qualitative synthesis of the AN experience reported themes of loneliness and isolation due to increased preoccupation with AN thoughts and adherence to strict exercise and dieting regimes, as well as feelings of being controlled by the disorder [
37]. AN can also become deeply entrenched in a person’s sense of self, manifesting as an internal ‘anorexic voice’ that infuses a sense of achievement as the thin body fits in with gendered cultural norms yet also criticises and denigrates for any deviations from AN-adjacent thoughts or behaviours [
38,
39,
40,
41].
Notwithstanding the contributions of this research in better understanding AN through a trauma lens, studies on this topic are limited by their cross-sectional designs [
42], which may oversimplify complex life narratives [
43]. Longitudinal studies, on the other hand, have the benefit of enriching constructed narratives by capturing the participants’ dynamic and unfolding AN and trauma journeys more fully than is possible in single qualitative interviews [
44]. Moreover, longitudinal studies can offer useful insights into longer-term illness outcomes and quality of life, thereby assisting in the development of treatment approaches [
45].
The current study will extend the existing research on this topic by exploring the narratives of a sample of women who reported AN and trauma longitudinally over 10 years. By prioritising the voices of lived experience and adopting a qualitative, narrative approach [
43], this paper aims to offer valuable insights into perceived inter-relationships between AN and trauma and identify shifts and changes in the meanings of these inter-relationships over time [
44,
46]. By adopting a broad definition of trauma that encompasses both “big T” and “little t” traumas, the researchers sought to flexibly explore AN in the context of a diverse range of life experiences [
22] (p. xxii). The research was guided by the following questions: How do women make meaning of their experiences of AN in the context of trauma? And in what ways do women’s narratives shift over time in relation to the meanings they ascribe to the experiences of AN and trauma (and their perceived inter-relationships, if any)?
3. Results
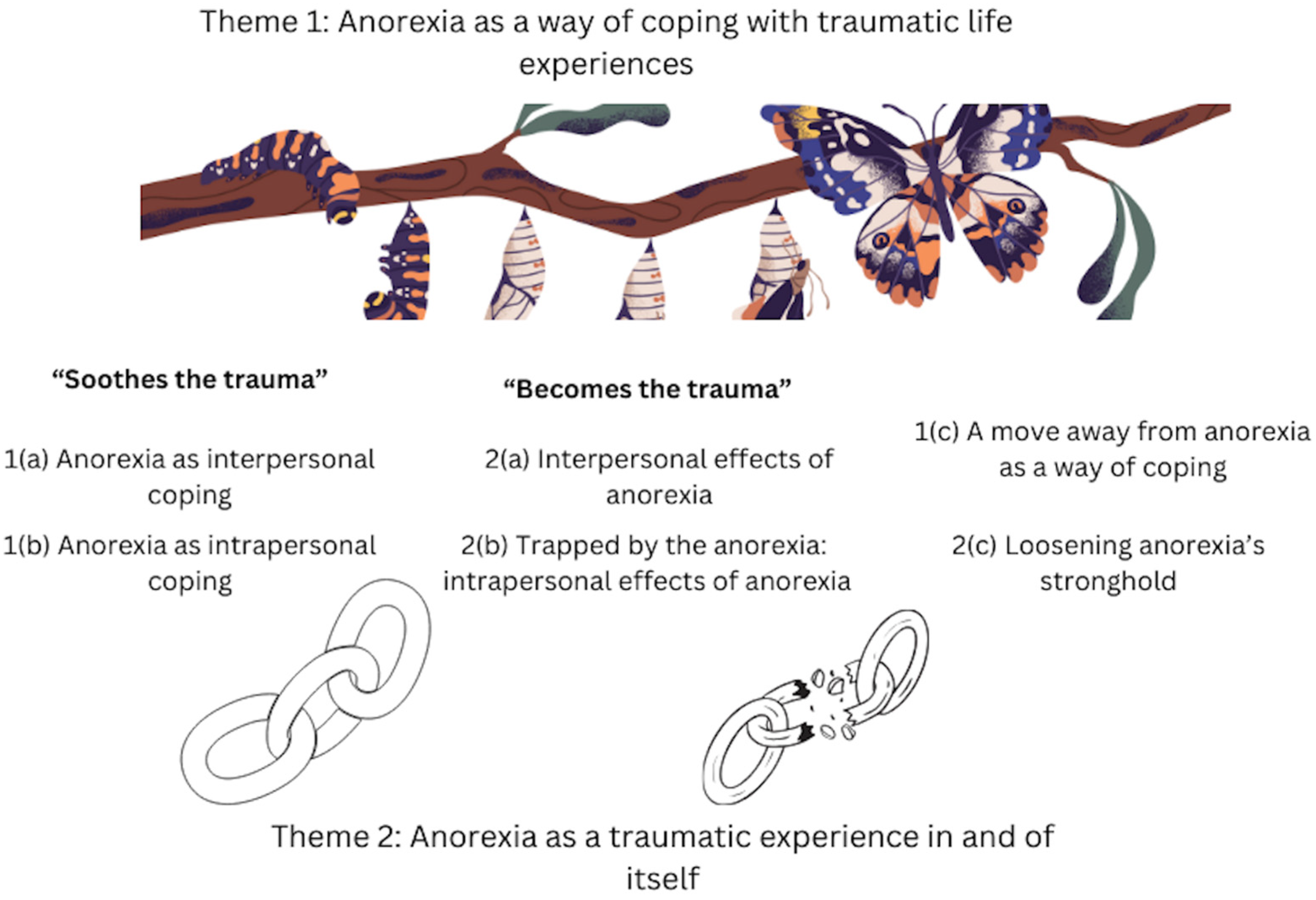
Two overarching themes were generated during the analysis. Theme 1 was anorexia as a way of coping with traumatic life experiences, and Theme 2 was anorexia as a traumatic experience in and of itself, each with three subthemes with their inter-relationship depicted by
Figure 1. This figure provides a visual representation of the identified themes. Rather than linear, the inter-relationship between AN and trauma over time was described by the women as recursive where anorexia may re-enter their lives to assist with coping with interpersonal and intrapersonal demands.
The metaphors that were chosen to depict the thematic map were drawn from two participants’ narratives of their experiences: (i) “Katie” who in her member feedback depicted her experience as a chain/broken chain and the combined titles for “Soothes the trauma” (Themes 1a and 1b) and “Becomes the trauma” (Themes 2a and 2b) and (ii) “Anne” in her interviews during the 10 year follow up depicted her shifting relationship with AN over time as “It [AN] is like the (pause) the slug, the caterpillar with the big cocoon thing… If I got rid of that big sack of (pause) stuff that was holding me into this pattern of, and, you know, eating disorder mentality, um, maybe the freedom would be quite (pause) resemble a butterfly” (second telling) [
48].
3.1. Theme 1: Anorexia as a Way of Coping with Traumatic Life Experiences
All the nine women disclosed experiencing ‘big T’ and/or ‘little t’ traumatic life events for which anorexia provided a way of coping. Anorexia was expressed as a way to cope with both the interpersonal (Subtheme 1a) and intrapersonal (Subtheme 1b) challenges brought about by these traumas. Of note, some women experienced a high number of adversities and traumas in their lives; however, only traumas that were explicitly connected to the anorexia experience are discussed in this paper and were included in the analysis.
Childhood sexual abuse was disclosed by three participants, which meets the criteria for ‘big T’ trauma, as described in the DSM-5-TR [
1]. Other disclosed childhood experiences may constitute ‘little t’ traumas [
22] (p. xxii), and included witnessing physical domestic violence (
n = 2), physical discipline (
n = 1), weight-based ridicule in a sporting environment (
n = 1), emotional neglect as a form of discipline (
n = 1), familial and/or peer bullying focused on weight (
n = 2), emotional needs not being met by family (
n = 1), verbal insults from a parent (
n = 1), emotional neglect (
n = 1), invalidation, criticism, and control from a parent (
n = 1), and death of multiple close friends and family members (
n = 1).
Relevant ‘big T’ trauma occurring in adulthood included rape by a partner (n = 1) and a major bereavement (n = 2). Adulthood ‘little t’ traumas included verbal insults and emotional neglect by a partner (n = 1), unethical practice by a health practitioner that resembled past abuse experiences (n = 1), and a significant relationship breakdown (n = 1).
3.1.1. Subtheme 1(a): Anorexia as Interpersonal Coping
In the context of emotional abuse and/or neglect, four women described anorexia as a means to be who they perceived others wanted them to be: “I suppose it’s about fitting in… Maybe with the anorexia the control was all about being something that I thought that other people wanted” (Sally, first telling), “This [being thin] was something that [significant family member] could be really proud of me for and I was finally accepted into the family” (Lisa, first telling) (details of family members have been omitted from extracts related to abuse or neglect to safeguard participant confidentiality). These extracts locate the anorexia experience within an interpersonal context and as an embodied way for the women to shape themselves into being a person they perceived would be accepted and valued by others.
Moreover, for four of the women, a smaller physical form was perceived as a way to protect themselves by eliciting care and protection from others, for example, “You want to have a little girl’s body because little girls are perfect… [being small] meant no one could hurt me because this person [one of parents] […] was here to look after me” (Katie, first telling). As exemplified by Katie, embodying a “little girl” presented her with a refuge from harm and an escape from the sense of herself as anything other than “perfect”. On starting high school, and in response to “find a place that I fitted in”, the meaning of a smaller body for Katie shifted to “the only way that I could be accepted […] to have the best body” (first telling).
Living in a smaller or “invisible” (Sarah, first telling) physical form for two of the women was perceived to protect them by minimising unwanted attention from others who might abuse them: “When I was being abused…I believed that it was my fault because of the way I looked because I think I was quite attractive when I was a child… if I was thin and ugly no one would touch me” (Susan, first telling). Here, Susan internalised an ego-centric child worldview that the abuse was her “fault”, and therefore perceived it as within her sphere of influence to protect herself from further abuse through an emaciated body.
3.1.2. Subtheme 1(b): Anorexia as Intrapersonal Coping
Five of the women described anorexia as a way to cope with challenging intrapersonal experiences (i.e., experiences that occurred within their minds and bodies). Specifically, one woman described attempting to control her emotions in the context of uncontrollable grief and loss (Naomi, first telling) and five women described anorexia as offering a mental escape from emotions altogether: “[Anorexia] is a safe place, it’s a little haven that you create for yourself that’s yours alone, it’s your own creation” (Anne, second telling). Moreover, Sarah shared, “I can feel angry at [perpetrator of abuse]…[but] I rage against myself, probably eating disorders is part of it. I know a lot of behaviours that have been a part of my life have been anger that’s gone inwards towards myself” (second telling). In contexts that were experienced as uncontrollable, anorexia became for Anne “a safe place” and for Sarah, anger as an act of resistance [
54] (against the abuse) became conflated with anger towards herself.
Furthermore, three of the women identified anorexia as a way to punish the body for abuse or, in the case of Jane, a period of emotional neglect: “I just felt so guilty, so bad inside, like I wasn’t worth anything, like I just had to punish my body” (first telling). Similarly, Sarah shared that “you continue to inflict the punishment upon yourself that the family inflicted upon you for being unacceptable” (first telling). For these women, anorexia was a response to a sense of themselves as “bad” (Jane) or “unacceptable” (Sarah) and therefore deserving of punishment.
In addition, anorexia was a way of reclaiming a sense of personal power taken away from two of the women who experienced childhood abuse: “It’s a hunger strike… It’s a protest against other people’s power over you. It’s an attempt to take power back for yourself” (Sarah, second telling); “One of the things about [significant family member] was that [they were] very forceful with food. And so very early on… I started vomiting and that felt like I was taking that control there” (Susan, second telling). For these women, anorexia was perceived as an embodied way of reclaiming power from family members whose actions were abusive and disempowering.
Importantly, four of the women also described a later traumatic experience to which anorexia served a different function compared to the initial function it served them during their traumatic childhood experience. For example, Anne, in the context of childhood ridicule, utilised anorexia as her internal “safe place” (second telling) that she could retreat into. Later in life, however, she experienced grief during a relationship breakup, and her relationship with anorexia shifted to become a means to elicit care from others (“take notice of me, take care of me”, first telling) and manage overwhelming feelings of anger (“because I can’t express the anger, I express it through that silent deprivation”, first telling). As further explored in Subtheme 1c below, this captures the way that the perceived function of anorexia is not static but rather shifts and changes over time as the women navigate new contexts and ways of coping.
3.1.3. Subtheme 1(c): A Move Away from Anorexia as a Way of Coping
A longitudinal shift emerged across all nine women’s narratives such that within the third telling, their narratives positioned anorexia as playing a less dominant role in their lives. While six women indicated that anorexia may re-enter their lives in times of adversity to assist with coping (“once again it becomes a friend in times of adversity” (Sarah, third telling)), alternative means of coping had also become available to four of the women over time: “I still see a hundred and one hurdles ahead but think I can get there, over those hurdles. Whereas before sometimes I couldn’t, and I needed to ask for help and that’s why I starved myself really” (Lisa, third telling); “You can have that power, the power that you think the anorexia […] is going to give you, you can achieve that in different ways” (Katie, third telling). Lisa described life challenges as “hurdles” that were no longer insurmountable with a process of claiming her voice, including “to ask for help” rather than starving herself as a way of coping. Furthermore, Katie spoke to a sense of empowerment whereby she leant less on anorexia as a way of regaining a sense of power that had been lost when she was younger in the context of violence.
Four of the women also described feeling disconnected from the function anorexia previously served: “I liked it at the time because it gave me something else to think about… but it’s really hard to get in touch with that now” (Susan, third telling); “I would not fall back into those patterns again… I don’t need that anymore” (Anne, third telling). Over time these women constructed anorexia as “hard to get in touch with” (Susan) and “I don’t need that anymore” (Anne), instead aligning themselves more closely with a sense of themselves that no longer turned to anorexia as a means of coping.
3.2. Theme 2: Anorexia as a Traumatic Experience in and of Itself
Two of the women referred explicitly to anorexia as “traumatic” (Naomi, first telling; Jane, third telling); however, more frequently, the women constructed anorexia as traumatic by describing the significant interpersonal (Subtheme 2a) and intrapersonal (Subtheme 2b) effects that are characteristic of the anorexia experience.
3.2.1. Subtheme 2(a): Interpersonal Effects of Anorexia
Eight of the women described the anorexia experience as isolating: “Not eating cuts you off socially from just about everything… I couldn’t go out with the new friends I’d made … because I might have to eat” (Susan, second telling); “I wish I had somebody to ring or to talk to and I just felt so sad, so lonely, so withdrawn from everybody else” (Jane, first telling). In this way, anorexia became a barrier to meaningful social interactions and consequentially, the women perceived themselves as “cut off” (Susan), “withdrawn” (Jane), and disconnected from their valued social identities.
Furthermore, six women described anorexia as having a negative impact on their family relationships: “My mother had a breakdown when I was sick… it can really destroy families” (Naomi, first telling); “Mum says more than anything that she wondered where I went for a few years, because like her daughter just disappeared” (Jane, first telling). In discursively constructing anorexia as “it”, Naomi was able to talk about the anorexia experience itself as destroying families, and Jane used the metaphor of disappearing from her mother’s life to illustrate the interpersonal effects of anorexia.
3.2.2. Subtheme 2(b): Trapped by Anorexia—Intrapersonal Effects of Anorexia
Five women described the general experience of being trapped by anorexia: “It was like having shackles around your ankles, steel chains holding you down” (Kelly, first telling). In this extract, Kelly uses an experience-near metaphor to depict the real effects of anorexia on her life, including a sense of powerlessness. These metaphors have been previously analysed in detail in this sample of women [
44].
Eight women also described a sense of feeling trapped in a perpetual internal battle that for some, was experienced as a war with parts of oneself, for example: “[there were] two me’s… the bit that knew what I was doing was wrong or damaging and then the other bit that didn’t really care” (Sally, first telling). This extract highlights the interweaving of dissociation of self into parts (“two me’s”) that was evident in the women’s narratives as they navigated traumatic life experiences including the experience of anorexia itself. Furthermore, understanding herself as “two me’s” enabled Sally to author the experience as a simultaneous desire to resist (“the bit that knew what I was doing was wrong”) and accommodate (“the other bit that didn’t really care”) the anorexia.
For the women who experienced this internal battle, five framed it as the internalisation of traumatic events: “I see it [anorexia] as fighting a war when the enemy’s gone home…the war was over… it ended a long time ago really. It didn’t end in my mind” (Sarah, second telling). Three women also described the voice of anorexia as aligned with the voice of the people who had abused them or were key figures in their traumatic experiences: “It was just like another form of my mother in some ways…she was still there even though she wasn’t” (Susan, first telling). Implicit in these descriptions is the construction of anorexia as a form of self-abuse that mirrors or replicates prior abuse even when the “enemy’s gone home” (Sarah). In this way, the unintended effect of anorexia formed part of the enduring legacy of harm and abuse.
Moreover, all nine women spoke to the inadvertent ‘trapping’ effect of anorexia by describing the way that it deteriorated their physical forms, causing them to live and move in bodies impacted by chronic health problems: “I’m a forty-three-year-old [woman] who has the spine of a sixty-year-old because of calcium depletion” (Anne, first telling); “I had no muscles left in my legs, just had these little tendon things, all the muscles had been eaten away by just exercising too much” (Jane, first telling).
Furthermore, for seven of the women, as they became increasingly trapped by the anorexia experience, they lost a valued sense of identity: “All people saw was a shell… if you want to draw a picture of me inside it would’ve just been black, nothing there” (Jane, first telling); “I had no time, no energy, no mental capacity to think of anything else besides anorexia. What was I without anorexia? Who was I? What was left? There was nothing left” (Naomi, first telling). These extracts highlight how anorexia took up space that would otherwise be occupied by valued identities, resulting in a perceived absence of self, such that “it would’ve just been black” (Jane) and “there was nothing left” (Naomi).
3.2.3. Subtheme 2(c): Loosening Anorexia’s Stronghold
A longitudinal shift emerged across the women’s narratives such that within the third telling, five women described feeling less trapped by anorexia generally: “It was just…an unloosening of the mental trap I put myself into” (Anne, third telling). And for those who experienced internal battles, seven described a shift in the relationship with the warring voices: “It’s my relationship with me, the way Kelly treats Kelly is a lot nicer” (Kelly, third telling). For the women, moving away from anorexia was a gradual process that unfolded over time, as exemplified by the “loosening” of the “mental trap” for Anne and a shift towards Kelly experiencing a “nicer” relationship with herself.
In addition, eight women described resisting anorexia by resisting the negative interpersonal and intrapersonal effects it had brought into their lives. For some, this involved strengthening connections with family: “I have too many other people dependent on me and … so I just keep on moving…” (Susan, third telling). In Susan’s case, moving forward meant anchoring herself to her family and aligning more closely with the sense of herself that others were “dependent on”. Moreover, some women described resisting the physical health effects brought about by anorexia by redefining their relationships with their physical bodies: “I can’t believe how amazing my body is […] that it can take so much abuse and then still perform all these functions” (Katie, third telling). For Katie, her body became perceived as “amazing”, and a vessel through which she could perform meaningful “functions” such as having a child. Implied in her narrative was her reclaiming a sense of personal identity and—through the process of becoming a mother—re-establishing a way of living in her body that more closely aligned with a valued sense of self.
3.3. More Than 2 Decades Later…Participant Member Reflections and Feedback
Four of the nine participants responded to the invitation to comment on the present paper’s findings nearly two decades after the final interview: Kelly and Jane, each in an email summary, Susan, who inserted reflections directly onto a copy of the paper using the Microsoft Word ‘comment’ function, and Katie who talked through her reflections on the paper with one of the authors (JC). With Katie’s feedback, JC reviewed the original transcripts to highlight how the meaning of AN shifted for Katie when she commenced high school and became what she retrospectively termed the “golden ticket” for acceptance by her peers (see Theme 1a)
The four women affirmed the themes generated in this analysis, with Kelly expressing that she viewed the analysis as “comprehensive” and felt “enlightened and validated” while reading the paper. She aligned herself with a belief in the capacity of women to move away from anorexia and a hope in research to further an understanding of how professionals can support them to do so: “I hope [this research] contributes to educating professionals and their understanding of the illness along with their ability to help sufferers overcome it”. Jane wrote in response to reading this paper: “It blew my mind. I thought when I was reading it “where was this information when I was suffering?” and “It reminded me of the reasons why I put myself through AN, bulimia and binge eating and why I responded to my trauma the way I did”. She also said, “This paper is important to continue to learn about AN, its causes and how to help. I hope it receives lots of publicity. While we can’t prevent trauma, as it’s part of life, papers like this provide understanding to help prevent AN, shorten its length, decrease its depth, hopefully save lots of lives and give back living to sufferers”.
All four participants also extended on the longitudinal shifts outlined in the analysis (Theme 1c and Theme 2c). For example, Susan further elaborated on her move away from anorexia as a way of coping (Theme 1c) in her comment “I never did [need anorexia anymore]… I continue at times to struggle with anxiety but have never revisited this extreme self-harm and abuse”. She also reflected that “I have grown older and felt like the adult that I am” as opposed to “being stuck in the childlike way of thinking” that she previously used to protect herself from abuse. Katie talked about how over time, “The answer becomes the question—the solution becomes the problem—soothes the trauma then becomes the trauma”, and how what resonated for her in the analysis was the process of losing and reclaiming a valued sense of self, and that “coming out of it—something else in life becomes more important”. Jane described how one of her proudest achievements was “overcoming AN”. She also wrote, “I realise how far I have come in my thinking, mindset and body image as I have accepted the changes (some days easier than others). I don’t judge people by their body shape and I’ve found others usually don’t judge me and if they do … they’re not worth my time” and “A trauma like my original trauma re- entered my life last year. I had the skills, wisdom and most importantly support to deal with it. I didn’t internalise it. I worked through it. I didn’t fall into AN or food or any other drug”. While Kelly did not comment directly on her current relationship (if any) with anorexia, she positioned herself in the context of her valued connections with family and the strength she has drawn from these relationships to move forward in her life: “I was remarried… I have grandchildren now and have so much to look forward to. I’m lucky”. She also described a shift in her view of herself as a person who had an “expiry date” and “never thought I would live past age 30” to someone who has lived much longer and feels “fortunate to have come this far in life”.
Katie also reflected how the other women’s experiences also resonated with her own in including in the following subthemes:
Theme 1(a): AN being a way of interpersonal coping through contributing to “a sense of inherent belonging” and feeling “beautiful and invisible” in the context of feeling “further behind” others in a social context in school. AN was “like a golden ticket” to acceptance by others through inhabiting a thin body.
Theme 1(b): AN as an act of resistance and a “weapon” to “reclaim power”—like a “superpower”.
Theme 2(b): Resonating with the sense of feeling trapped in a perpetual internal battle, Katie reflected “That war between parts of myself—one part that knew what I was doing but didn’t care […] I related to this, the duality of it”. And in this subtheme of being trapped by AN, she stated, “You lose such a sense of self-worth that have to find something that they would like me for—always not fitting in—being enough—or being popular—if only could see that was part of something that didn’t need to look for way out”.
In reflecting on her shifting relationship with AN, Katie said, “the beast matures” and “the coming out of the end of it there has to be something that becomes bigger, something more important than yourself, and finding a different tactic because this one is not going to work” and “the beast matures over time”.
4. Discussion
The majority of research has focused on trauma as a risk factor for AN and more severe eating disorder symptoms [
13,
14], and associated it with treatment attrition and more severe ED symptoms post-treatment [
16]. Within this context, there is a need for a more in-depth understanding of the complex intertwining of the experience of AN and trauma, including from the perspective of those with a lived experience to inform more comprehensive treatment interventions for this at-risk group. This study aimed to longitudinally explore the inter-relationships between AN and “big T” and “little t” traumatic life experiences [
22] (p. xxii) over 10 years. The participants’ self-reported duration of AN at the first interview ranged from 4 to 31 years, suggesting a long-standing AN experience [
55]. Furthermore, all women identified experiencing at least one form of abuse (i.e., emotional, physical, sexual) or other trauma (i.e., grief or loss of meaningful relationships, exposure to domestic violence) during childhood, and all except one woman reported experiencing at least one traumatic event in adulthood.
Within the narratives, AN was constructed as a way to cope with the interpersonal and intrapersonal effects of trauma. Regarding the former, the women reduced their physical forms to gain approval and acceptance from others. For some of the women, having an emaciated body was perceived as a way of seeking protection by either eliciting care and love from others (i.e., by replicating a ‘childlike’ form), or minimising unwanted attention to safeguard against further abuse (i.e., by becoming ‘ugly’ or ‘invisible’). These functions have been recognised as a way of re-establishing feelings of safety, personal power, and ways of being in the world that have been lost or obscured by trauma and abuse [
18,
32,
33].
Intrapersonal coping involved managing trauma-related emotions, thoughts, and memories. In line with previous research, self-starvation was used to self-punish for abuse [
18,
24,
28] as well as to regain a sense of power that was lost during abuse [
18]. Furthermore, some women utilised AN as a means of regulating their emotions, which supports etiological models of AN and trauma [
26]. However, the nature of emotional regulation varied from controlling, re-enacting, or escaping emotions altogether. While these differing responses have been captured in previous research [
23,
24,
25,
35,
36], the variability present in the current study reinforces the individualised nature of emotional regulation and highlights the limitations of models that seek to capture these complexities using a single etiological pathway [
34].
Importantly, by tracking traumatic experiences that occurred across the lifespan, the current study found that for four women, the function of AN was reported as changing from childhood to adulthood. This finding indicates that the perceived functions of AN may change over time as women navigate new adverse contexts and diverse coping needs. Similar shifts in functionality were noted by Broomfield and colleagues [
28]; however, contrary to the current study, these authors did not consistently link these functions to context or explore their inter-relationships with traumatic life events, leaving the functions decontextualised and interpreting them as a time-based phenomenon that corresponded with participants entering a later stage of longstanding AN.
In addition to providing a means of coping, the women in the current study constructed AN as traumatic in and of itself. This juxtaposition of AN as both helping and harming has been explored in previous research and illustrates the intrapsychic tensions characteristic of the AN experience [
6]. The conceptualisation of AN as ‘traumatic’ may align with ‘little t trauma’ and had significant effects on the women’s lives and sense of self, including debilitating interpersonal effects (i.e., social isolation, disharmony in family relationships) and intrapersonal effects (i.e., feeling trapped by AN, experiencing an internal battle with AN, facing serious health problems, and losing a valued sense of identity).
The negative effects of AN on health, identity, and relationships are recognised within the literature [
37]. Furthermore, the internal battle of “two me’s” described by the women aligns with the concept of the ‘anorexic voice’ [
39]. Some participants connected the ‘voice’ to past emotional abuses—a finding that is corroborated by theories of the voice as emblematic of past emotional abuses [
40] and comparable to the experience of being in a violent and toxic relationship [
41].
Importantly, by the final telling, the women had moved away from using AN as a way of coping, described feeling less trapped and at war in their minds, and were actively resisting the unwanted interpersonal and intrapersonal effects AN had previously brought into their lives. For most women, AN was still present and might remerge in times of stress; however, it was a less dominant part of their lives, and other coping strategies (e.g., asking for help) and intrapersonal experiences (e.g., improved relationships with themselves, improved health, identity reconstruction through motherhood) had become available to them. In this way, the women were able to reach a more settled narrative and relationship with AN [
48]. Additionally, the women resisted the health consequences caused by AN and strengthened meaningful family connections. These findings align with a post-traumatic growth framework, which recognises the personal growth and strengthening of values, wisdoms, and identity that occurs in the aftermath of trauma [
56]. Furthermore, the process of anchoring to family is reflected in trauma healing literature such that “through human relationships, a traumatized person retethers to the world” [
57] (p. 754).
4.1. Study Strengths and Limitations
To the authors’ knowledge, this study is the first of its kind to apply a longitudinal qualitative methodology to the topic of AN and trauma. This approach allowed for the construction of broad shifts in the women’s narratives and, in doing so, was able to better capture the resilience of the participants beyond what would have been possible using a single-point, cross-sectional design [
44,
46]. Furthermore, to our knowledge, the current study is the first to identify shifts in AN functionality over time and outline how these functions inter-relate with both childhood and adulthood traumas. In doing so, it extends previous research that tended to conceptualise the coping component of AN as being a static and perpetual response to early (unresolved) traumas [
58]. By considering the inter-relationships between AN and adult traumas, the current study offers important insights into the maintenance of longstanding AN and the way it can be enlisted and re-enlisted to cope with novel adversities in novel ways [
59]. A further strength of the current paper was the process of regular collaboration between three authors in the identification and refinement of themes, as well as immersion in the data by SB and JC. While the main thematic extraction was conducted by SB, regular input was provided by JC, who collected and analysed the data for a number of projects [
44,
47,
48] and was able to verify a good general ‘fit’ between the identified themes and the participant’s narratives. The feedback provided by two participants further enriched the validity of the analysis and minimised the risk of interpretative researcher bias.
On the other hand, due to being a convenience sample recruited as part of previous research [
44,
47,
48], the sample size has implications for data saturation and may limit the capacity of the study to put forward a complete understanding of the topic [
60]. While the overarching themes regarding the inter-relationships between AN and trauma were ‘saturated’ (i.e., consistently endorsed across all nine participants), the particular nature of these inter-relationships (identified in the subthemes) varied between participants and did not meet saturation, as new meanings continued to be presented in each narrative [
60]. Notwithstanding this limitation, the authors argue that the subthemes add value to the analysis as they “tell a compelling, coherent and useful story in relation to the research question” [
61] (p. 207) and assist in capturing the complexities and variability experienced by a non-homogenous sample with diverse trauma experiences.
Second, the historical nature of the data may limit its representativeness of present-day AN and trauma phenomena. However, it should be noted that the identified themes have been found in more recent datasets [
18] and are therefore assumed to retain their validity and relevance. Third, the women did not reflect the contemporary diversity within the wider Australian community and further research is needed in peoples from other cultural and sociodemographic groups, including men.
4.2. Clinical Implications
The current study has several key implications. First, it questions the validity of dominant perceptions of AN as functioning primarily to achieve an ideal body image or adhere to a ‘thin ideal’, particularly when it exists in contexts of abuse and trauma [
18]. Indeed, the diverse functions AN served in assisting the women to cope with traumas, as well as the high prevalence of big T and/or little T traumas described by the women, reinforce the need for the development of evidence-based trauma-informed treatments that can target both AN and the trauma-related distress that may underpin and maintain AN, while also strengthening alternative means of coping [
62]. In particular, the current findings emphasise the need to assess, understand, and target factors that underpin and maintain AN-type behaviours, namely, the ways in which the experiencing person perceives and experiences AN as ‘helpful’ and assisting them to manage unmet interpersonal and intrapersonal needs that arise in response to trauma. Furthermore, the finding that AN re-emerged for participants in response to new adversities in adulthood indicates a strong need for treatment to focus on relapse prevention, including the recognition of early warning signs; exploration of and alignment with values and wisdoms; connection to valued identities and meaningful social or familial networks; and development of alternative (more adaptive) means of coping in response to stress. Although some of the women in this study talked about how not only was the AN experience traumatic but so too was its treatment; however, this was beyond the scope of this study. Other qualitative research has identified how AN treatment was inadvertently traumatic for some people with a lived AN experience [
28,
63,
64,
65,
66] and there is a need for more research to ensure that treatments do no harm.
Finally, the finding that the women moved away from AN in their final tellings can assist in building a more hopeful perspective for clinicians and emphasises the strength of women to exit critical stages of AN and achieve a healthier and more sustainable life course. Further research is required to explore the specific factors responsible for this move away from AN.





{kind=link}