1. Introduction
Depressive disorders are now common in both developed and developing countries. Chronic depressive conditions are also increasingly observed in the working-age population and threaten to become a serious and costly problem, both at the level of individual households and the economy as a whole. The World Health Organisation [
1] estimates that depressive disorders currently affect 3.8% of the population, including 5% of adults (4% of men and 6% of women). According to data from the Institute for Health Metrics and Evaluation [
2] from the resulting
Global Burden of Disease Study 2019, depression was found to be the fourth leading cause of disability worldwide. The contribution of depressive disorders to total years lived with disability (YLD) due to all chronic diseases was 6.1% for men and 7.3% for women. Over the past three decades, the number of years lived with disability due to depressive disorders per 100,000 people has increased from 409.3 to 468.3 for men and from 536.2 to 551.0 for women. In 2019, depressive disorders accounted for 32.0% of the burden of mental illness for men and 41.9% for women. Worldwide, they are estimated to have caused more than 46.9 million years of disability over this period, of which 61.2% were attributable to women.
Mental disorders, such as depression, are a common problem that also affect people of working age [
3]. In many highly developed countries, they are the most common cause of long-term sickness absence and loss of working capacity [
4]. These disorders reduce the productivity of workers who continue to work despite their illness (a phenomenon known as presenteeism). The high burden of depressive disorders in highly developed economies is particularly evident in the very young population, which significantly determines the potential of labour resources.
According to IHME data for 2019 [
2], the most burdened group in the United States were people aged 20–24, which is reflected in the high rates of years lived with disability (YLD) per 100,000 people, i.e., 1759.4 for women and 993.2 for men. In this age group, depression is estimated to account for 12.4% of all causes of YLD in women and 8.9% in men. In the case of the United States, it is characteristic that the burden rate and the share of depressive disorders in the total burden of disability from any cause decrease with age. In the same age group (i.e., 20–24 years) in the world in 2019, the YLD rate per 100,000 people was 844.7 for women and 546.8 for men. In the group of EU countries, the rates were 1020.1 for women and 568.0 for men. However, the cited IHME data indicate different specificities of the effect of age on the burden of depressive disorders observed in the European Union countries. The highest burden, measured in years lived with disability per 100 000 people of that age, was observed in older populations in the labour market. For women, the highest burden was observed in the 45–49 age group, where the burden rate was 1172.8 (compared with 1161.3 in the USA and 1078.3 worldwide). In the working-age male population, the most affected group was the 50–54 age group, with a burden rate of 703.6 YLD due to depressive disorders per 100,000 people in this group (with a corresponding rate in the USA of 639.4 and globally of 708.8). In the EU age group indicated, depression accounted for 7.5% of YLD from all causes among women and 5.2% among men. In the EU area, the lowest burden of depressive disorders in the working-age population was generally observed in young people. The above dimension of the burden of depressive disorders in working-age people translates into measurable economic and social costs, estimated in terms of lost productivity of affected workers. According to the OECD [
5], more than 30% of these costs are due to the lower employment rate and lower productivity at work of people with mental health problems.
The aim of this study is to assess the impact of depressive disorders on the potential of labour markets in European Union countries, with particular reference to inequalities between ‘old’ and ‘new’ EU countries. The study attempts to assess the convergence taking place in this area, assuming a process of levelling out possible initial differences in the level of this phenomenon determined by the socio-economic integration of the EU-27 area. The phenomenon of the impact of mental health disorders, particularly depressive disorders, on the reduced productivity of people of working age has been the subject of numerous studies, but the results presented usually ignore the context of heterogeneity in socio-economic and institutional health determinants observed between the highly developed countries of ‘old’ Western Europe and the ‘new’ EU Member States with experience of systemic transformation. Using data from the Institute for Health Metrics and Evaluation’s Global Burden of Disease Study 2019 on the level of burden of depressive disorders in the 27 EU countries, the analysis presented here aims to answer the following research questions:
- (1)
Does the variation in socio-economic and institutional determinants of health observed across the EU-27 group of countries significantly determine the quality of the psychophysical components of human resources with a particular focus on mental health, including depressive disorders?
- (2)
Are there persistent inequalities between ‘old’ and ‘new’ EU countries in the burden of health resource limitations caused by depressive disorders?
- (3)
What patterns of convergence (or divergence) can be observed in the levelling out of initial inequalities in the mental health capital of working-age people across the EU-27 group of countries?
The impact of depressive disorders on the burden of individual EU-27 economies is expressed in terms of years lived with disability (YLD) caused by the disorder in the working-age population. This measurement allows for an objective evaluation of the long-term consequences.
The presentation of the results was preceded by a review of the evidence on the impact of mental disorders, including depressive disorders, on the efficiency and productivity of the workforce. Attention was also drawn to the paucity of research in the area of inequalities in the burden of depression due to socio-economic and institutional determinants of mental health between the ‘old’ and ‘new’ EU. This study expands upon the existing literature on the impact of mental illness, specifically depressive disorders, on labour productivity. It introduces the perspective of inequalities observed between EU-27 economies with varying levels of socio-economic development.
2. Mental Illness and Labour Market Outcomes—A Review of the Evidence
The impact of mental illness, including depressive disorders, on labour market outcomes has been the subject of much well-documented research. There is strong evidence that mental illness, mainly measured as depression and/or anxiety, is associated with productivity losses due to absenteeism or presenteeism [
6]. These studies provide empirical evidence that mental disorders are associated with a higher risk of unemployment and lower earnings [
7] and increased absenteeism and reduced labour supply [
8,
9,
10]. At the same time, these studies show a strong impact of mental illness on employment and clear evidence of reduced levels of work ability. According to Cornwell et al. [
11], each mental disorder reduces the probability of labour market participation by 1.3 percentage points, which is significant given that most people with mental disorders have several categories of disorders at the same time. Frijters et al. [
12] found strong evidence from Australian panel data that a deterioration in mental health leads to a significant reduction in employment. They showed that a one standard deviation deterioration in mental health leads to a 30-percent point reduction in the probability of employment. This effect holds for both men and women. According to Banerjee et al. [
13], improving mental health to the level of those without any mental illness can increase the probability of employment by 18 and 11 percentage points for men and women, respectively.
Research into the impact of mental disorders on labour market outcomes is also paying increasing attention to the problem of presenteeism, which results in reduced productivity of those who are ill at work. Marlowe’s research [
14] identifies mental health issues, such as depression and stress, as the primary causes of acute presenteeism. This is followed by musculoskeletal and respiratory disorders. The findings of Johnston et al. [
15] confirm the existence of a significant relationship between the severity of depression and absenteeism and presenteeism, indicating an increase in absenteeism and a decrease in productivity as the severity of illness increases. The relationship between decreasing levels of mental wellbeing (MWB) and increasing loss of productivity was demonstrated in a study by Santini et al. [
16]. The results of a study by Stewart et al. [
17] showed that employees suffering from depression reported significantly more total health-related LTP (lost productive time) than employees without depression—an average of 5.6 h/week compared to the expected 1.5 h/week. According to the researchers, as much as 81% of the cost of LTP could be explained by reduced productivity at work due to depressive illness.
According to Vigo et al. [
18], the economic cost of mental illness is underestimated, leading to an underestimation of the global burden of mental illness. They identified five main reasons for this. Firstly, there is an overlap between psychiatric and neurological disorders. Secondly, suicide and self-harm are included as a separate outcome category. Thirdly, all chronic pain syndromes are combined with musculoskeletal disorders. Fourthly, personality disorders are excluded from the calculation of the burden of mental illness. Finally, the impact of severe mental illness on all-cause mortality is inadequately considered. Based on published data, the authors estimated that mental illness accounted for 32.4% of total years lived with disability (YLD) and 13.0% of disability-adjusted life years (DALYs) globally.
In the case of mental disorders, additional mechanisms determining the labour market performance of people with disabilities should also be identified. These stem both from employers’ attitudes towards people with mental disorders and from discrimination in the workplace. A study conducted by Sander et al. [
19] on a group of more than 5000 German employees found that the risk of presenteeism worsens with increasing levels of mental health stigma. The results obtained by these researchers showed that 55% of respondents experienced a current deterioration in mental wellbeing and 65% of respondents would feel at least some shame if they suffered from a mental illness. In the case of experiencing a mental illness, 54% of respondents indicated probable presenteeism, and the same number of people with mental illness would go to work without informing their managers and colleagues. Brouwers [
20] suggests in his research that the high unemployment of people with mental illness and mental health problems is largely due to the stigma they experience at work. Employers and immediate supervisors have negative attitudes towards people with mental health problems, which significantly reduces their chances of employment. Bonaccio et al. [
21] point out that a common concern of employers is the low productivity of employees with chronic diseases. Economic, institutional, and cultural determinants influence employers’ attitudes towards the recruitment and employment of people with health limitations, especially when these limitations are due to mental disorders. Cybula-Fujiwara et al. [
22], who conducted research in this area, confirmed that there is a prevailing view among employers that people with mental illness have a limited ability to work and that social attitudes towards these people tend to be marked and stigmatised. As a result, employers avoid hiring employees with disabilities resulting from mental disorders by trying to overlook this segment of the labour market [
23].
Detailed research has explored the interactions resulting from the endogeneity of the relationship between the level of mental disorders observed in the working-age population and the work efficiency of sick people. The results suggest that work stress affects a range of health outcomes for workers, including their mental health. Brunner et al. [
24] used cross-sectional data from Swiss workers to demonstrate that work resources can mitigate the negative impact of stressors on productivity. Their findings indicate that a 1% increase in work stressors has a greater impact on health-related productivity losses than a 1% decrease in work resources over the same period. According to Sørensen et al. [
25], work stress, which is measured as a combination of job strain and an imbalance between effort and reward, was found to be associated with a higher incidence of chronic disease in the future, based on an 18-year follow-up of the Danish workforce. Burns et al. [
26] and Limmer and Schütz [
27] also confirmed that time pressure, job insecurity, and conflict negatively predicted employees’ mental health. Mental health is a crucial component of an individual’s overall health and productivity [
28]. Additionally, the conditions of the work environment can impact employees’ exposure to mental disorders [
29].
Researchers measuring the burden of chronic diseases in terms of labour market outcomes point out that there is still a need for research on how to measure the value of lost productivity caused by long-term health limitations in workers. Indeed, standardised methods for measuring this phenomenon have not yet been developed in this area [
30,
31]. The most widely used approach to assessing productivity losses from an employer’s perspective is derived from human capital theory, according to which the loss of healthy life years represents a loss of productivity, the value of which in competitive markets can be assessed on the basis of the amount of wages lost or the value of the potentially producible product during this period [
32,
33,
34]. The findings of Zhang et al. [
35], on the other hand, provide convincing evidence that productivity losses due to employee absenteeism exceed the wages of team workers, especially in small firms. Given the shortcomings of the human capital method, an alternative approach to the valuation of lost output based on the so-called frictional cost theory has been proposed in the literature. This approach limits the productivity costs resulting from the absence of a sick employee to those associated with the time needed to hire and train a replacement employee [
36,
37,
38]. Similarly, with regard to presenteeism caused by the effects of illness, most studies focus on the possibility of measuring it, identifying this issue as a necessary step in establishing the link between health and productivity [
39]. Brouwer et al. [
40] emphasise that the cost of lost productivity can be an important component of total costs in the economic assessment of the burden of disease and that estimating productivity losses is a key element in calculating productivity costs.
The phenomenon of the impact of mental disorders, particularly depression, on the reduced productivity of people of working age has been the subject of numerous studies; but, the results presented have tended to ignore the context of the heterogeneity of the socio-economic and institutional determinants of health in the ‘old’ and ‘new’ EU systems, which determine the variation in the quality of the psycho-physical components of human resources. The limitations in this respect were largely determined by the lack of available data on the burden of disease comparable at the level of the EU economies [
41,
42,
43]. The results presented on the study of inequalities in exposure to depressive disorders generally focused on the impact of social inequalities on the prevalence of common mental disorders in selected European countries [
44,
45] and on the impact of the social gradient on the prevalence of depression, which is relatively well established in studies conducted in Western European countries [
46,
47].
Given the lack of research on inequalities in the burden of depression between the highly developed countries of ‘old’ Western Europe (EU-14) and the ‘new’ EU Member States with experience of systemic transformation (EU-CEE), this study attempts to identify these inequalities and assess their persistence, taking into account the impact of the period of accession of the new Central and Eastern European countries on EU structures. This study hypothesises that that membership of certain groups of EU countries has a significant impact on the level of health burden of depressive illness. Statistically significant differences were found between the EU-14 and EU-CEE study groups in terms of the average number of healthy years lost to depressive disorders. However, ongoing socio-economic integration processes in the EU-27 have reduced the observed differences over time. The reduction in inequalities in the burden of depressive illness in the EU-27 economies is expected to lead to a process of convergence, resulting in a decrease in the average level of the studied indicators over time, as well as a decrease in their dispersion.
3. Materials and Methods
The economic burden of depressive disorders on the EU workforce was analysed using indicators of years lived with disability (YLD) caused by the illness. The variables analysed were chosen based on a review of methodologies proposed in the literature to assess the phenomenon under study [
48,
49]. The selected indicators illustrate the lost time of healthy life, including the potential lost time of effective work of people of working age. This also indicates the level of burden on national economies caused by selected diseases. The assessment of the value of healthy life years lost due to disability, known as YLD (often combined with an indicator of years of life lost due to disease, or YLL), is used to estimate production losses. However, there is a lack of methodological consensus in this area [
50,
51].
To ensure comparability of data across EU Member States, intensity indicators have been utilised. These indicators relate the number of observed cases to a specific population size. The analysis utilised an indicator to determine the number of potential years of life with disability (YLD) resulting from depressive disorders (DD) per 100,000 individuals. This indicator, YLD (DD), was observed in the group of individuals aged 20–54. The population for the indicated age group was selected based on the assumption that they represent potential labour resources with high productivity, including a lower burden of other chronic diseases. Additionally, aggregated data availability was taken into consideration. The data used in the analysis was obtained from the Institute for Health Metrics and Evaluation (IHME) [
2] and is based on the
Global Burden of Disease Study 2019. The study aimed to determine the number of years lived with disability (YLD) caused by depressive disorders in the working-age population of individual EU-27 countries. The aim of this study was to compare the prevalence of depression in two groups of countries: (a) the 14 EU countries that joined the EU before 2004; (b) the Central and Eastern European countries that joined the EU after 2004 and were in transition. The analysis was conducted separately for males and females due to significant gender differences in the phenomena studied.
The level of inequality in the analysed process was assessed using the relative health gap (RHG) indicator. This indicator helps to determine the statistical likelihood of experiencing negative consequences of depressive disorders (such as loss of health) in the EU-14 compared to the EU-CEE. The formula used to estimate the relative health gap (RHG) in the burden of chronic disease consequences, which determines the level of inequality between study groups, is as follows:
where
h(
A) is group A’s health burden measure and
h(
B) is group B’s corresponding measure.
Before conducting a thorough analysis of the studied inequalities, a statistical evaluation was performed to determine the significance of the observed differences in the analysed parameters among the various groups of EU-27 countries. In order to show the basis of the phenomenon under study, data on the severity of depressive symptoms in the EU-27 were collected. The data presented are based on Eurostat data [
52]. The study assessed the statistical significance of differences in mean values among select EU groups using the adopted testing scheme. If the p-test probability was less than the assumed significance level of α = 0.05, the null hypothesis was rejected. Statistica 13 software was used for calculations.
The anticipated outcome of reducing disparities in disease burden on EU economies is a noticeable convergence process, characterised by a decline over time in the mean level of the studied indicators as their variability diminishes. The system under review has been assessed using the concepts of beta (β) convergence and sigma (σ) convergence. Beta convergence takes into account different initial conditions and predicts that outliers will catch up more quickly with the target, while sigma convergence is defined as a reduction in the dispersion of performance.
To test the beta convergence hypothesis using cross-sectional data, in an explanatory model the growth of the characteristic considered was modelled in each EU-27 country (
i = 1, …,
N) between period
t0 and
t0+T, using the initial value of the characteristic in each Member State according to the following formula:
where
yit is the value of the characteristic
y in area
i in period
t and
uit is the random biases.
Beta convergence is supported by a statistically significant negative value of estimator
b:
A negative sign of the parameter b indicates the presence of beta convergence between the Member States.
This study assumes that positive beta convergence, indicated by the ratio of the parameters yit0+T/yit0 tending towards the lowest possible value, occurs when countries with a higher initial disease burden catch up by moving faster to the expected state. It assumes that all countries converge to a common long-run equilibrium but that countries with a worse initial situation have a further way to go.
Sigma convergence indicates an expected decrease in scattering of a characteristic over time. The amount of variance from the population in period
t(
) was used as a measure of the dispersion of the given characteristic to verify this hypothesis in the system studied, according to the following formula:
where
yit represents the value of characteristic
y in area
I during period
t, and
ȳt represents the arithmetic mean of characteristic
yi (for
I = 1, …,
N countries) during the same period.
To test the sigma convergence hypothesis, the variances in the variables analysed were compared in the extreme periods: t0 and t0+T. It was assumed that sigma convergence will occur if the value of the assumed dispersion index at the end of the analysed period (t0+T) is significantly lower than at the beginning (t0). Considering the specificity of the studied process, the convergence process is expected to have a positive effect on the economic development of the European Community area. This effect will be reflected in a decrease in the average level of the studied parameters over time (, along with a simultaneous decrease in the level of their dispersion (). These results will enable the evaluation of the convergence pattern in the studied system. Beta convergence is necessary but not a sufficient condition for sigma convergence to occur.
4. The Problem of the Burden of Depressive Disorders in Developed Economies
Based on a preliminary analysis of the data, it appears that the level of socio-economic development in a region is correlated with the burden of health restrictions resulting from depressive disorders (DD). It is important to note that this correlation is not absolute and may vary depending on the specific area. According to data from the Institute for Health Metrics and Evaluation [
2], in 2019, the YLD(DD) rate (i.e., YLD per 100,000 people) for women varied between 669.2 (low SDI countries) and 855.0 (high SDI countries), while for men it ranged from 433.2 (medium SDI countries) to 530.8 (high SDI countries), depending on the level of socio-economic development (SDI measure). Therefore, the level of the examined burdens does not show significant differences between individual groups, with low levels of these burdens visible in countries with low and medium levels of development. For both women and men, the highest levels of YLD(DD) rate were recorded in countries with the highest level of development (refer to
Table 1). Depressive disorders account for 6% of the total years lived with disability due to health impairments for women and 5% for men, on average. The contribution of these diseases to the total burden of disability is estimated to be highest in countries with low levels of development, with 6.5% of total years lived with disability for women and 5.3% for men, and lowest in the most developed countries, with 5.4% of total years lived with disability for women and 4.2% for men.
Between 1990 and 2019, the burden of depressive disorders increased in all country groups. The rate of increase was highest in medium SDI countries and lowest in low SDI countries. Notably, the share of depressive disorders in the total disease burden decreased in high SDI countries but increased significantly in low SDI countries (refer to
Table 1).
A characteristic feature of the approach to estimating the burden of depressive disorders used in the GBD study is that it focuses exclusively on the impact of the disease on years lived with disability (YLD). Due to methodological problems in attributing deaths to a specific mental disorder, the GBD estimates of the burden of depressive disorders in terms of years of life lost (YLL)—as is the case with these statistics for most chronic diseases—are not available. Therefore, in the case of the data presented, the problem of the burden of depressive disorders is represented only by the degree of disability of those affected; this effect is particularly severe in the case of women.
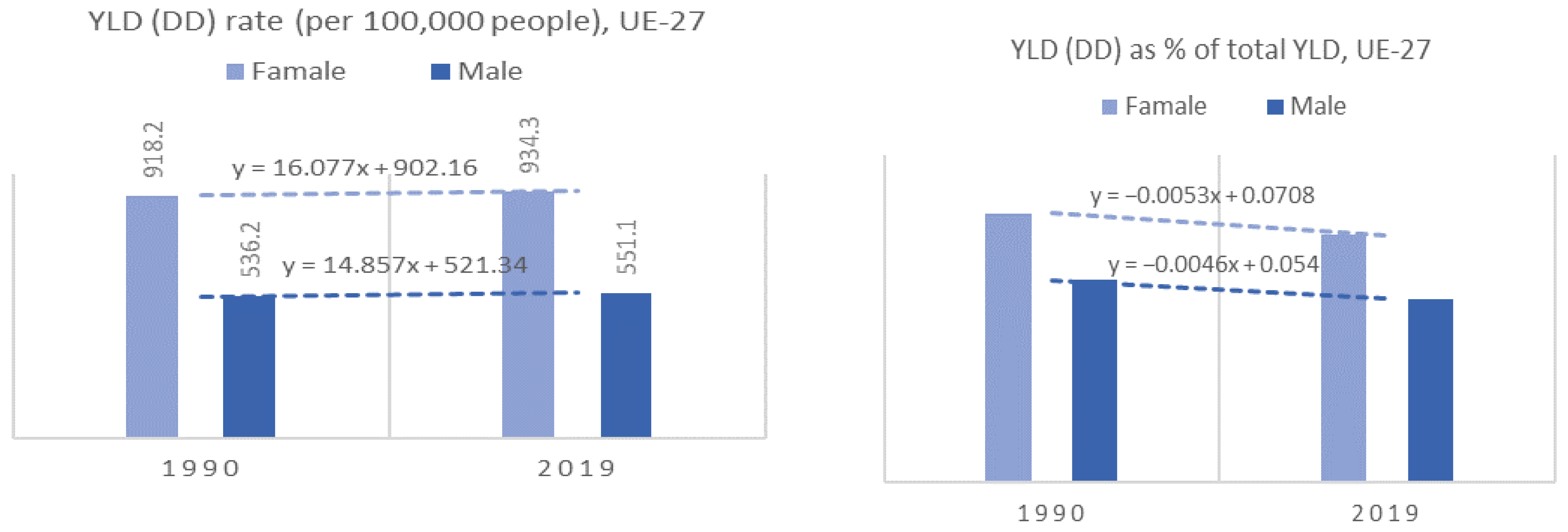
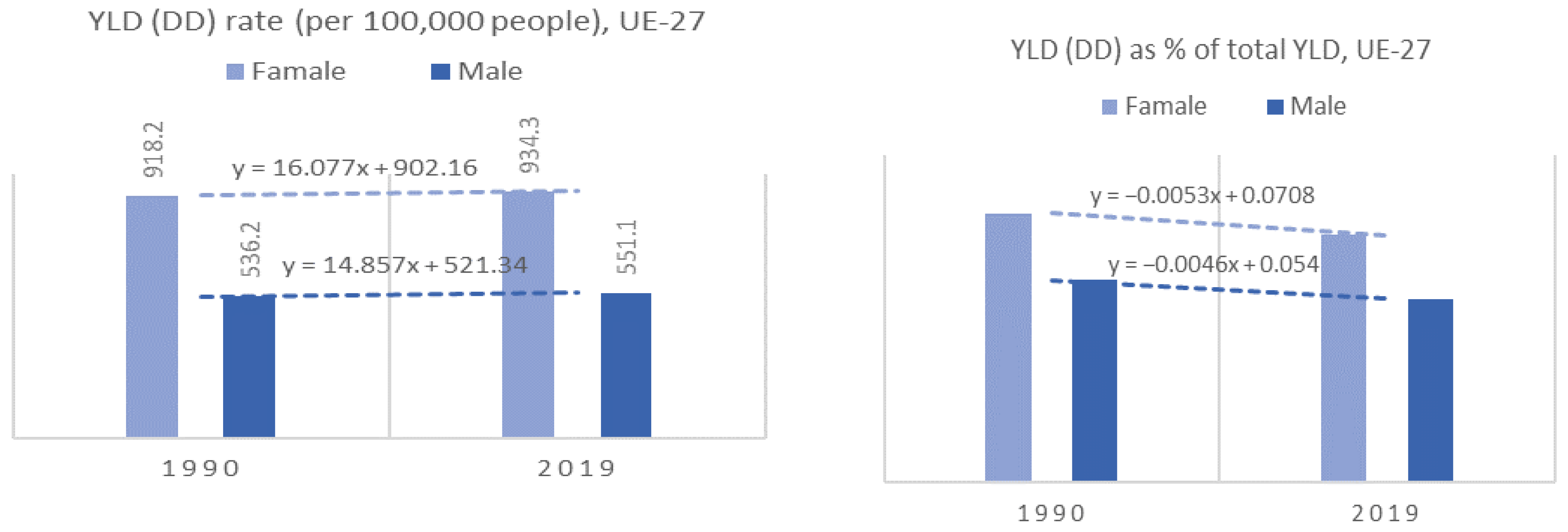
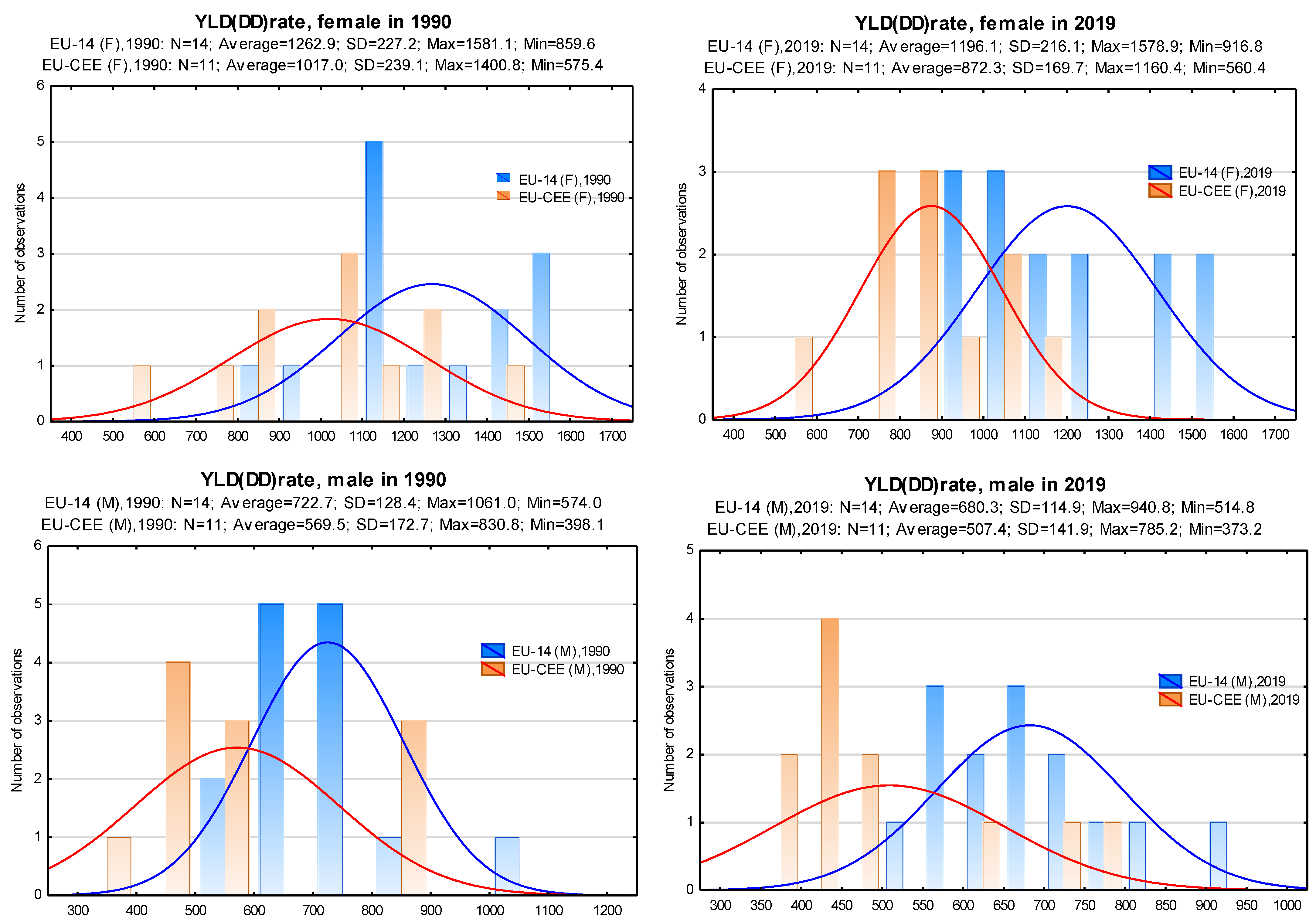
For EU countries, the total number of years of (healthy) life lost due to depressive disorders in 2019 was more than 3.8 million. The observed levels and trends in the burden of depressive disorders allow the EU-27 to fit into the patterns observed in the group of countries with the highest level of development but with a higher YLD (DD) index than this group (and, consequently, has much higher levels than those observed in the other SDI groups). In 2019, the average YLD (DD) rate in the EU-27 was 934.3 for women and 551.0 for men. These rates increased slightly between 1990 and 2019, by 1.8% for women and 2.8% for men (
Figure 1).
The patterns of the share of depressive disorders in the total burden of disease are also similar to those in the most developed countries. In the group of EU-27 countries in 2019, this share was 6.0% for women and 4.5% for men of the total number of years lived with disability (YLD) due to all diseases. Over the period 1990–2019, in the EU-27, a decrease in this share is also observed at the level of the burden studied (a decrease of 8.0% for the group of women and 9.4% for the group of men). The decrease over time in the share of depressive disorders in the total burden of disease is a constant feature of the most developed economies. In economies with low levels of development (low SDI and low-middle SDI), the share of depressive disorders in the total burden of disease, estimated in terms of years lived with disability, is increasing (see
Table 1).
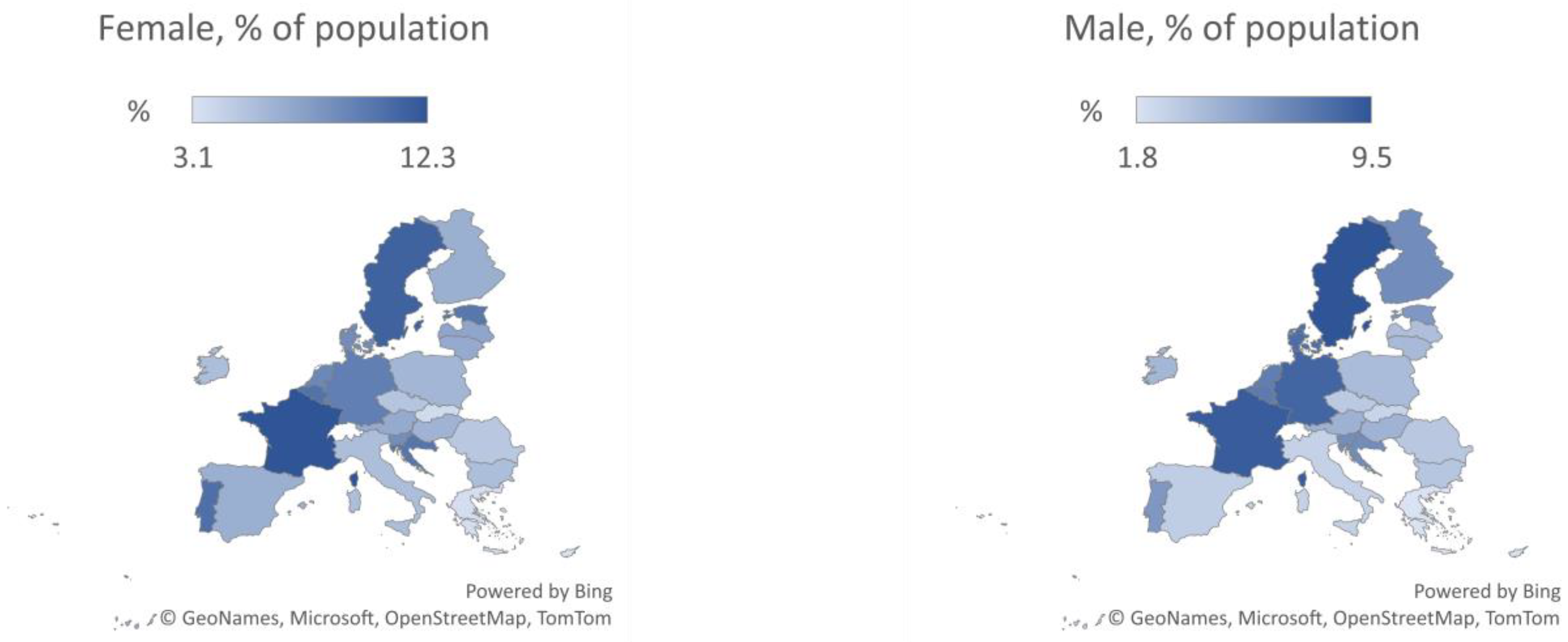
Eurostat data for 2019 [
52] describing the intensity of depressive symptoms in the EU-27 show a high degree of variation between individual EU countries. For women, the incidence of depressive symptoms ranged from 3.1% (Cyprus) to 12.3% (France) of the population, depending on the Member State. Similarly, among men, the proportion reporting depressive symptoms ranged from 1.8% (Greece) to 9.5% (Sweden), depending on the country. Analysis of the spatial distribution of the prevalence of depressive symptoms across the EU-27 shows that a significantly higher intensity of depressive symptoms is observed in the EU group of Northern and Western European countries (
Figure 2).
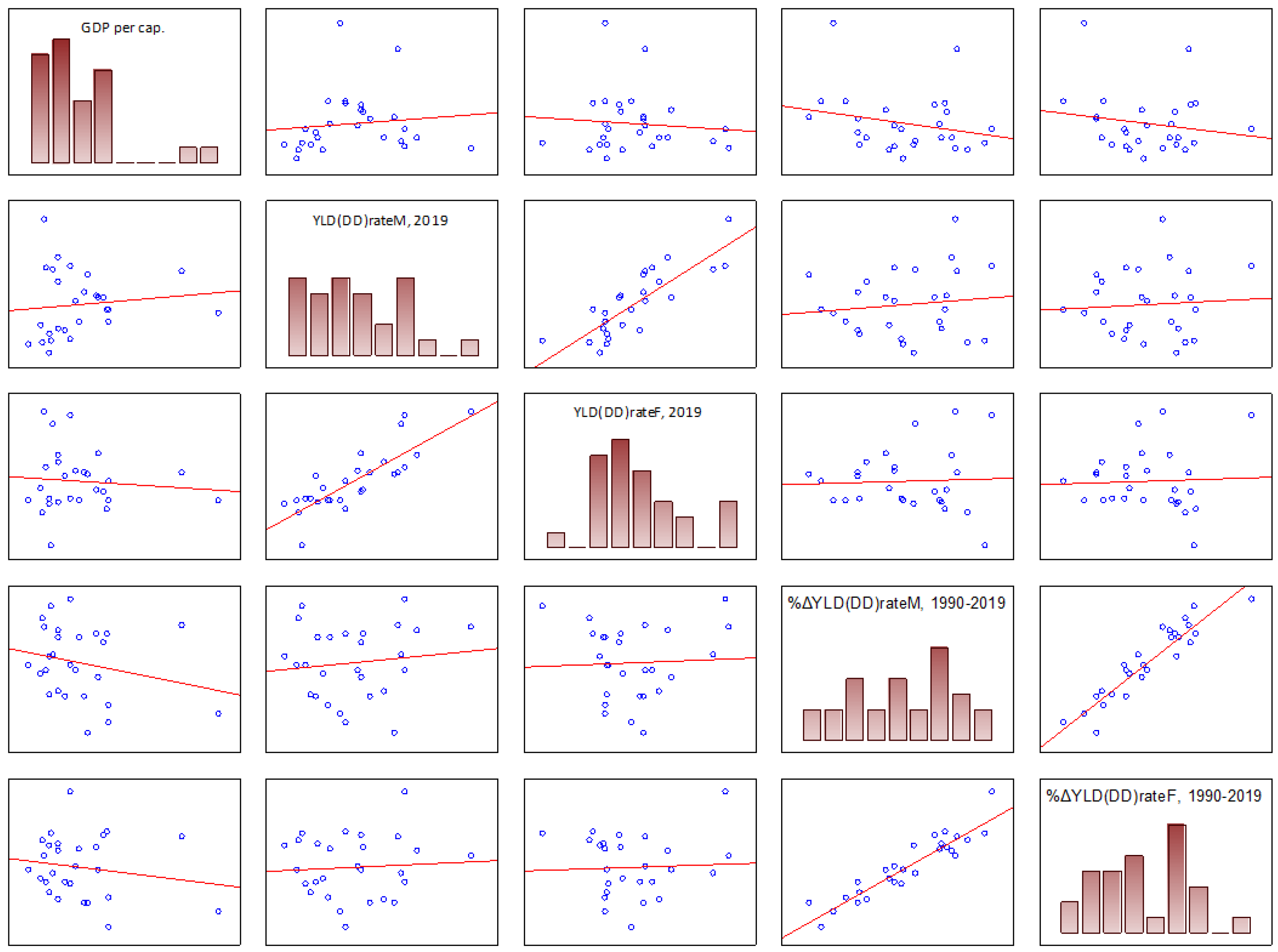
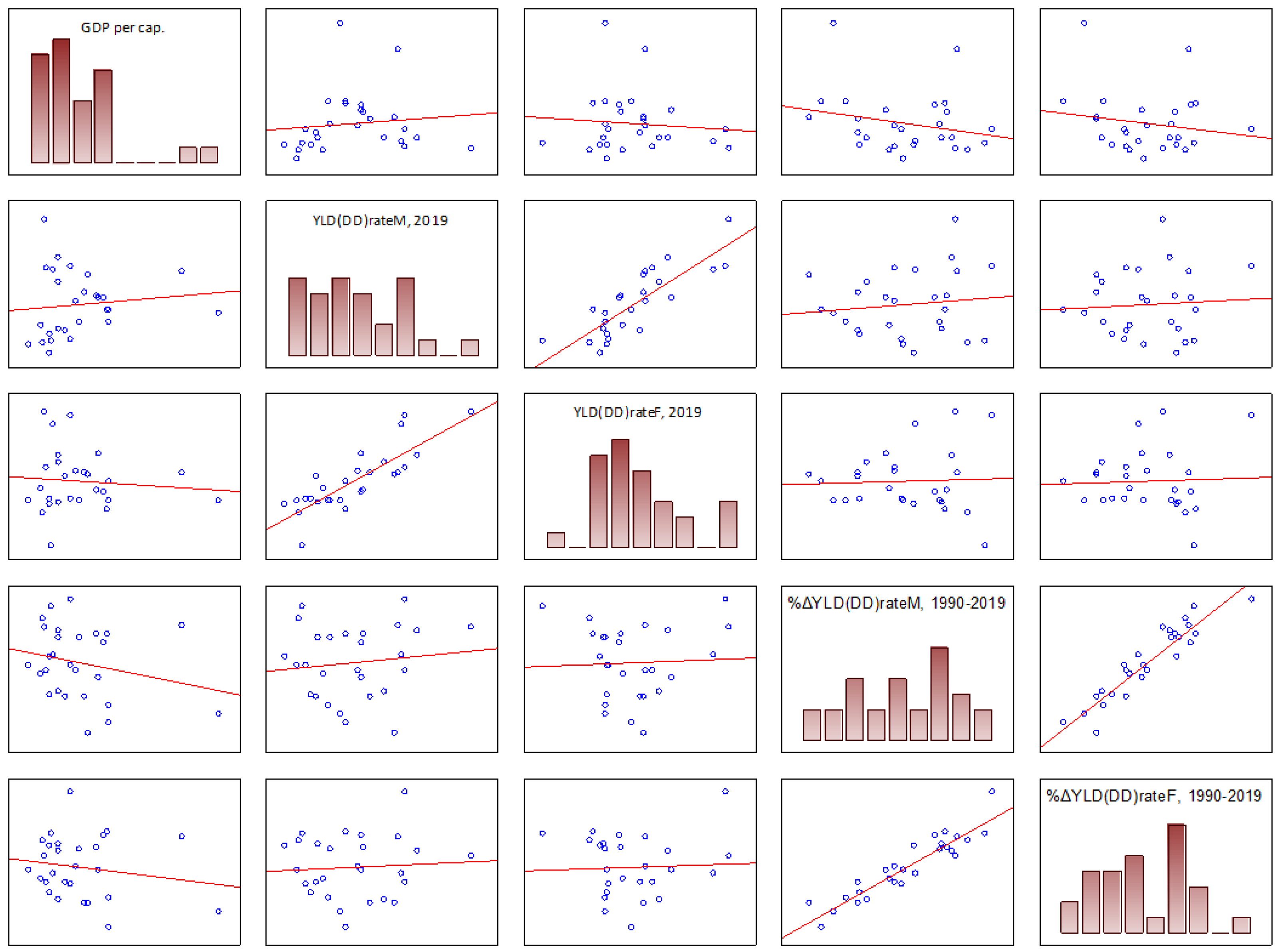
This study evaluated the relationship between a country’s level of socio-economic development and the burden of depressive disorders. However, no significant correlation was found between these parameters in the EU-27 countries, as shown in
Table 2. The number of years lived with disability due to depressive disorders (YLD (DD) rate) in EU countries does not seem to be clearly correlated with the country’s level of economic development, as measured by its Gross Domestic Product per capita (GDP per capita). There was no significant correlation found between the level of economic development of a country and the direction and rate of change in the YLD (DD) rate parameter over time. Both variables analysed showed weak (−0.2 < r < 0.1) and statistically insignificant correlation levels (see
Table 2 and
Figure 3).
The correlation results of the study variables (
Table 2) further indicate country-specific trends in the burden of depressive disorders, which are observed independent of gender. Indeed, there was a strong and statistically significant positive correlation between the country-specific observed levels of depressive disorder burden for women (YLD (DD) rate M, 2019) and men (YLD (DD) rate M, 2019). The correlation coefficient between these variables was 0.83 with statistical significance (
p > 0.05, for α = 0.05). A strong positive correlation was also observed for the rate of change of the variables studied between men and women in the Member States between 1990 and 2019 (ΔYLD (DD) rate, 1990–2019). The estimated correlation coefficient for this relationship was 0.93, at (
p > 0.05, for α = 0.05).
5. Results
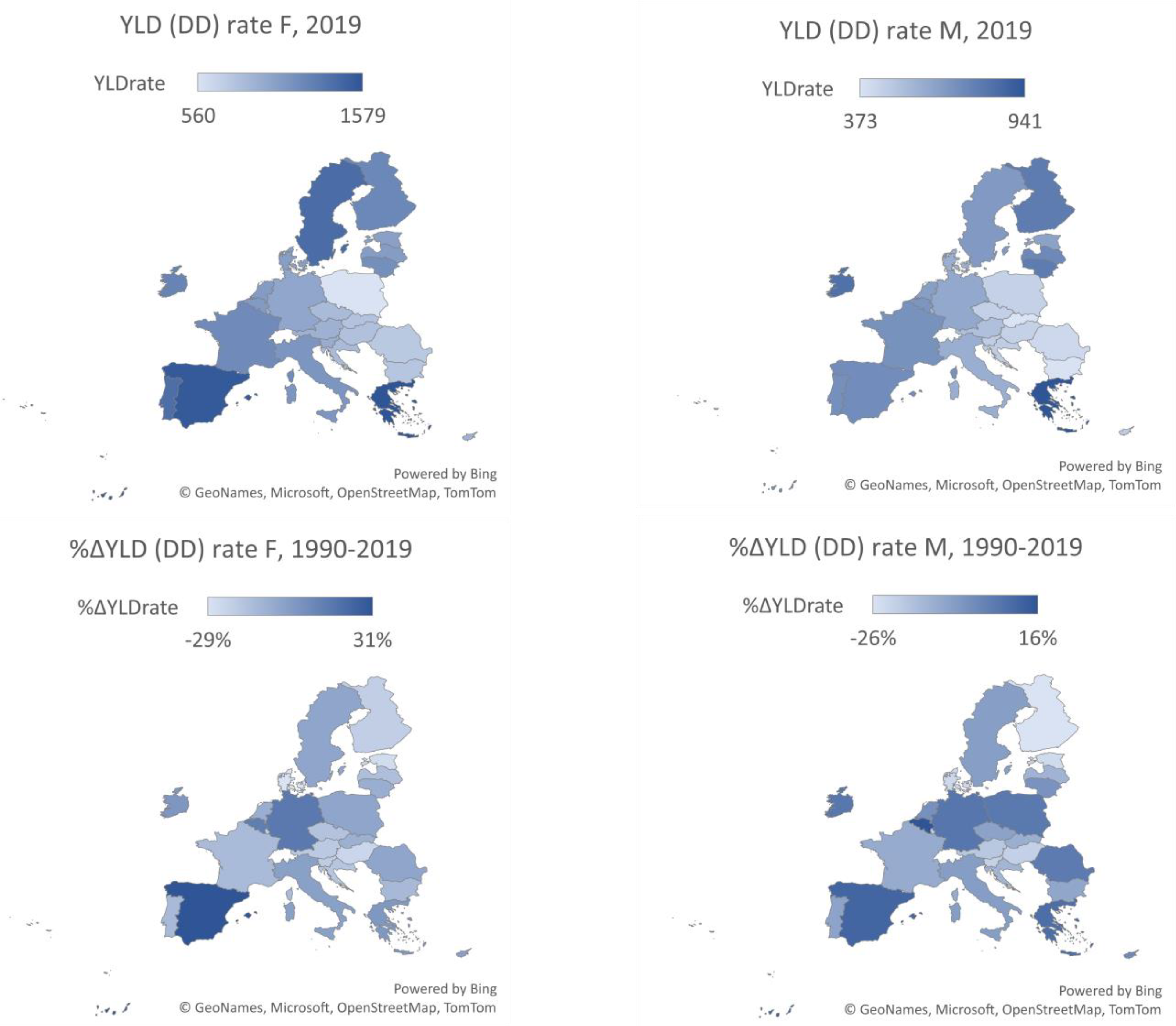
The impact of depressive disorders on the working-age population, measured in terms of years of disability caused by the illness, varies significantly across EU-27 Member States (see
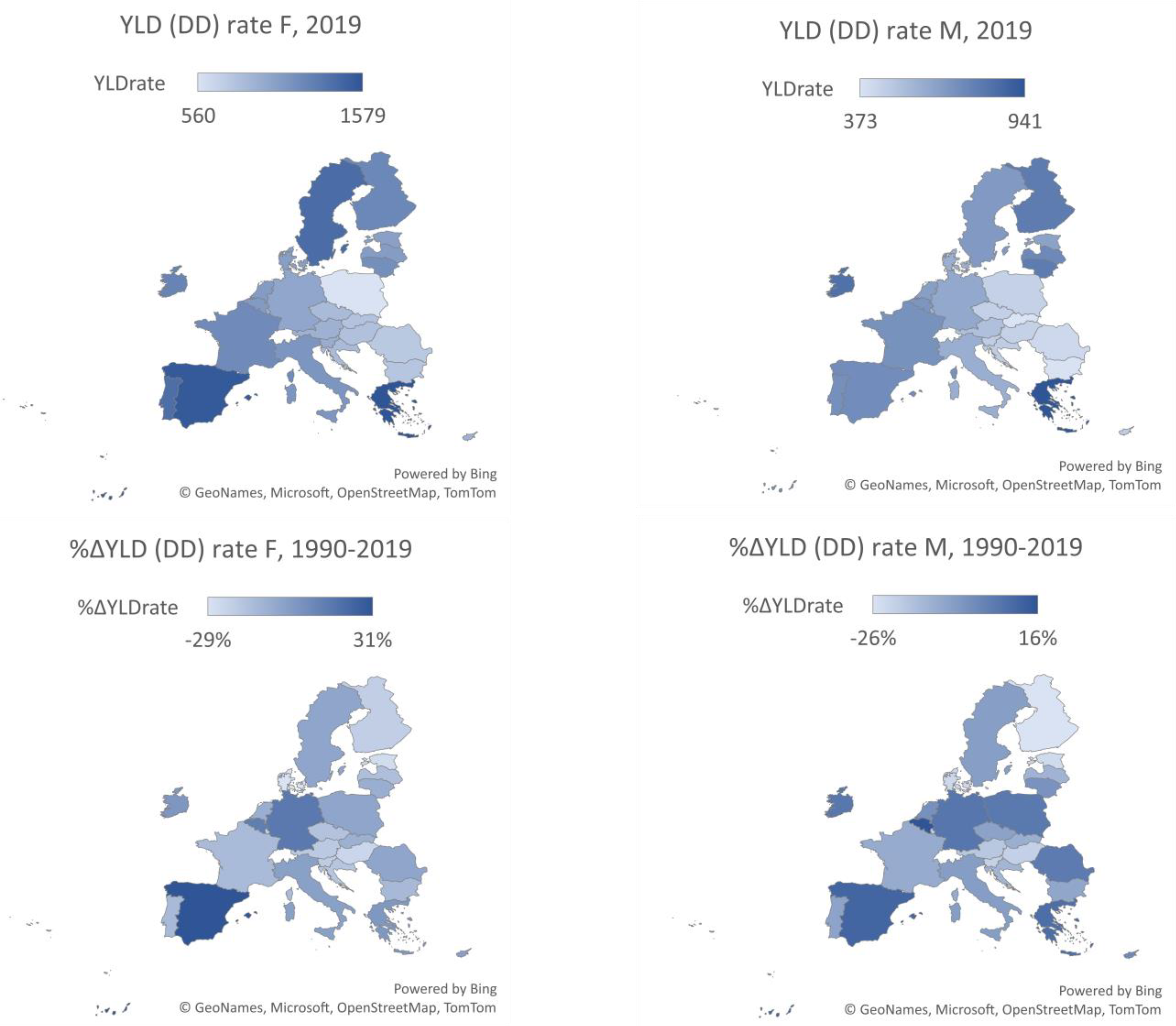
Table 3). In 2019, the average rate of disease burden resulting in disability (YLD (DD) rate) for individuals aged 20–54 in EU Member States was 1043 (women) and 594 (men) years of healthy life lost per 100,000 people in this age group. The YLD (DD) rate for women ranged from 560 (Poland) to 1579 (Greece), while for men it ranged from 373 (Slovakia) to 941 (Greece). Between 1990 and 2019, the YLD (DD) rate decreased by an average of 7.4% for women and 6.6% for men aged 20–54 in the EU-27 countries. Most EU-27 countries observed a downward trend in this indicator, with the largest reductions in the burden of long-term disability due to depressive disorders for women in Denmark (−29%) and for men in Finland (−26%). The YLD (DD) rate saw a significant increase in Spain, with a 31% rise for women and an 11% increase for men, as well as in Belgium, where women experienced a 14% increase and men a 16% increase.
Analysis of the spatial distribution of the burden of depressive disorders among the working-age population in the Member States shows that the risk of negative consequences is significantly lower for both men and women in the Central and Eastern European EU countries (see
Figure 4). These countries have lower rates of years of life lost due to disability as a result of depressive disorders than the rest of the EU-27. Notable exceptions are Lithuania, Latvia, and Estonia, whose YLD (DD) rates for both women and men are in line with the average levels observed in the group of EU-14 countries. At the same time, the results of the analysis show a wide variation in both the direction and the rate of change in the level of the burden of disability due to depressive disorders in the working-age population.
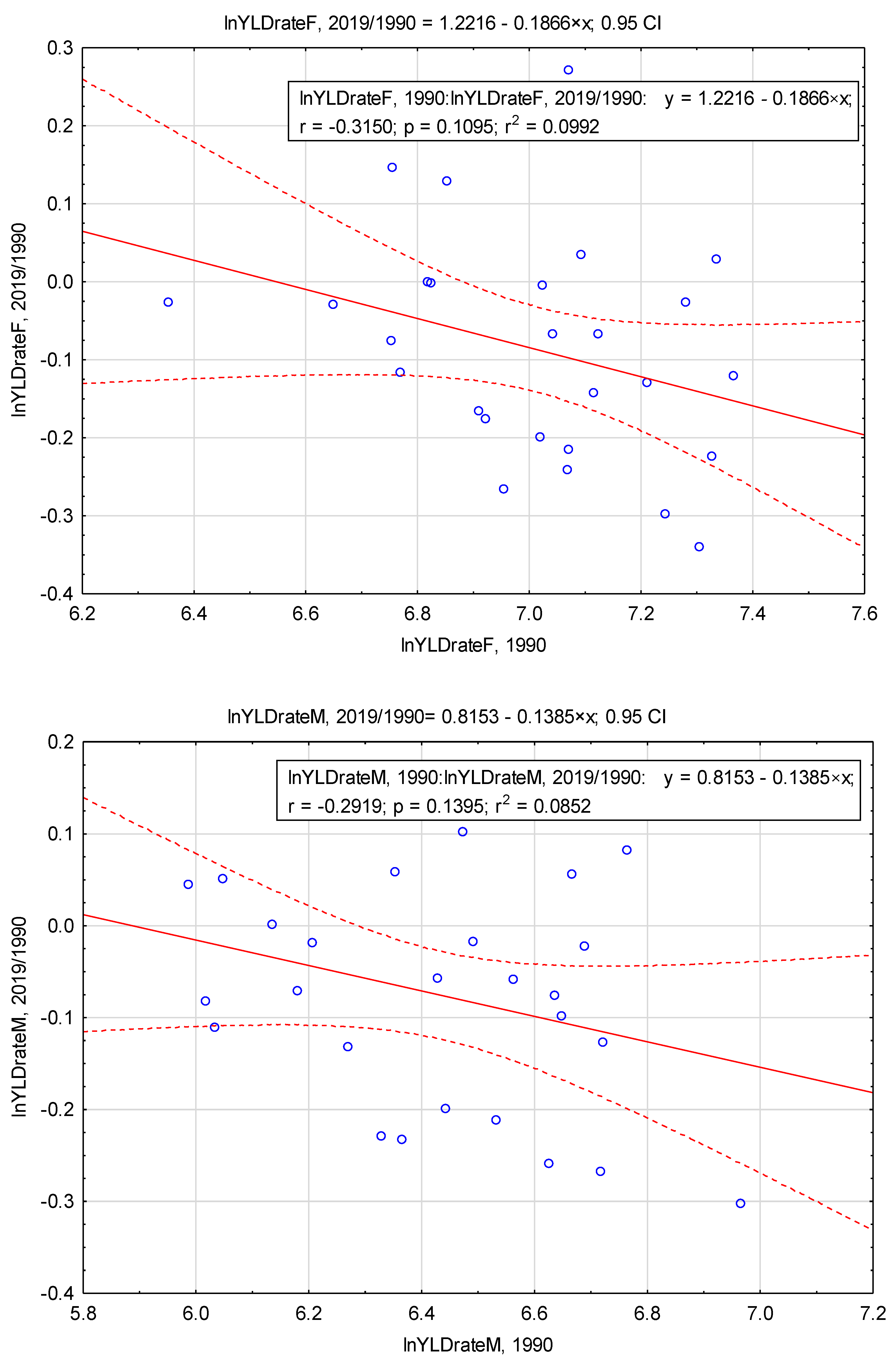
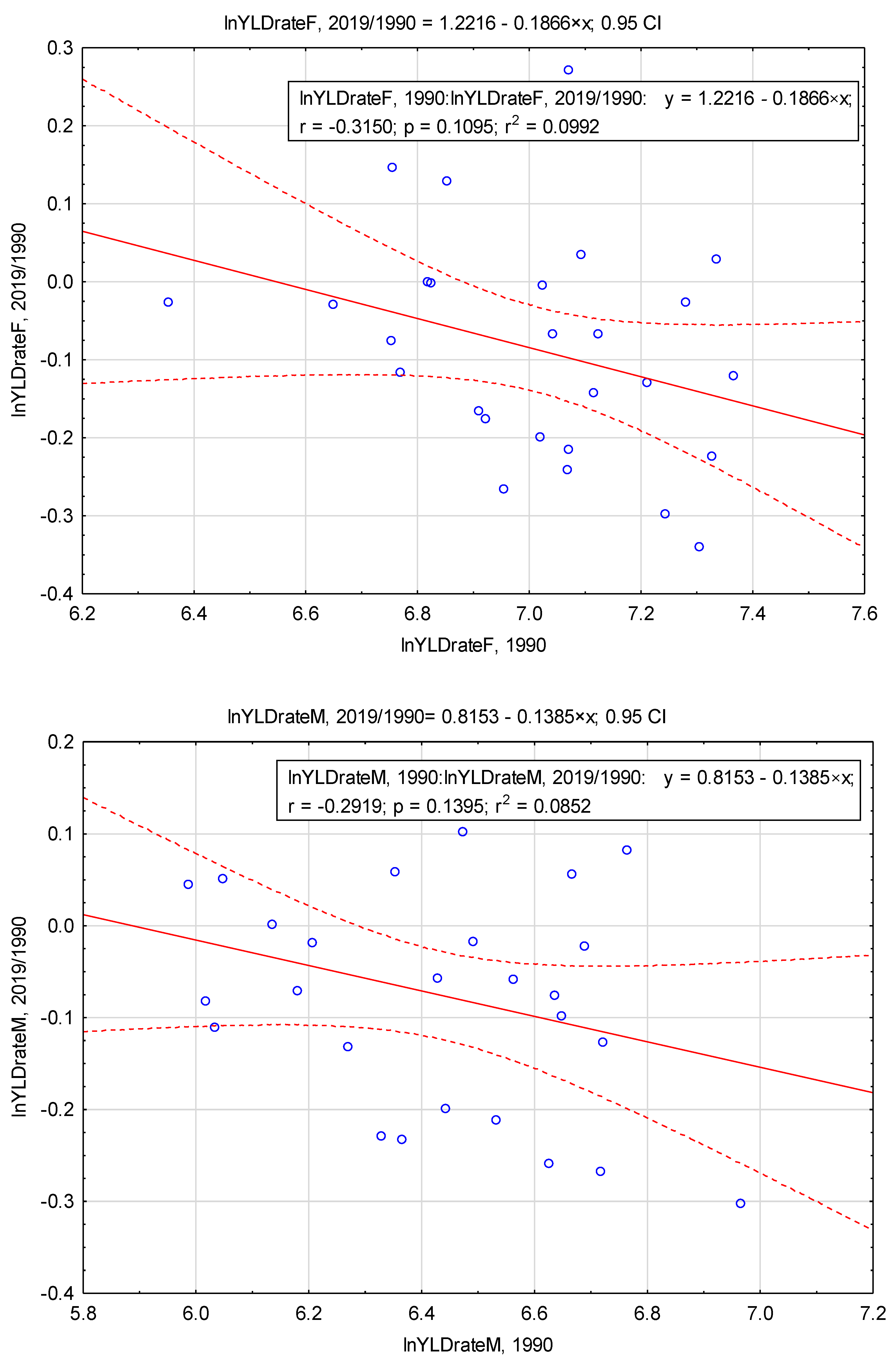
In order to test the hypothesis of beta convergence in the reduction of the burden of depressive disorders on labour resources in the EU-27, an explanatory model based on Equation (2) was used to examine the growth of this characteristic in each of the EU-27 countries. The rate of change of the analysed parameters in each EU country between 1990 and 2019 (relation 2019/1990) was determined, assuming different initial conditions for each country based on the level of the YLD (DD) index in 1990. It was assumed that for Member States with worse initial conditions (i.e., high initial levels of the variable) this indicator should be as low as possible. This shows a quick decrease in the analysed parameter, resulting in catching up with the group (beta convergence).
The regression models estimated from Formula (2), explaining the growth of the indicators examined that determine the level of disability burden (YLD rate) following depressive disorders in the group of EU-27 countries, were determined as follows:
- (a)
- (b)
variable YLD (DD) rate M
where
i = 1, …, 27.
Figure 5 shows the linear regression results for the parameters studied.
The results of beta convergence suggest that, for the parameters analysed (YLD (DD) rate in the female and male populations aged 20–54), the b-estimator value is negative. This may indicate slow convergence processes in the group. However, the low level of fit of the regression models (R
2) to the observed variables indicates that the process of equalisation of the health burden in the EU-27 group cannot be adequately explained by the process of convergence. The obtained results of the statistical significance of the estimators determined using the regression equations (
Figure 5) indicate that in the case of the variables YLD (DD) rate F and YLD (DD) rate M there is no possibility of using them for further inference (statistically insignificant parameters assuming α = 0.05). This indicates that it is not possible to confirm the existence of beta convergence in the EU-27 group with regard to the burden of disability on labour resources due to depressive disorders.
In addition, the assessment of the level of dispersion of the studied variable in the extreme periods of analysis
t0 (year 1990) and
t0+T (year 2019) shows that the level of dispersion of the parameter YLD (DD) rate has decreased over time both in the group of women and men, which indicates the effect of the reduction in disparities between the EU-27 countries. The statistical test of the hypothesis, which assumes the existence of sigma convergence in the group studied, showed that the variances of the variables studied in the initial and final periods are not statistically significantly different (for α = 0.05). This indicates that the hypothesised condition for the existence of sigma convergence is not met for both study populations (
Table 4).
Taking into account the disparities between the EU-27 economies identified in the study, as well as the indicated lack of real convergence effects in the level of burden on national labour resources due to health impairment caused by depressive disorders in the working-age population, an analysis of the extent of existing inequalities was carried out for the separate countries of the ‘old’ and ‘new’ European Union. The evidence presented confirms that the burden of depressive disorders is significantly higher for both sexes in the EU-14 economies than in the EU-CEE group. The gap that existed in 1990 did not decrease significantly over the period. The decreasing trends in both groups over time have a positive impact on the overall burden of the health effects of depressive disorders in the European Union. However, the rate of decline of the parameters studied in the EU-14 countries, which were already in a worse position to begin with, is too low compared to the EU-CEE countries. As a result, the observed differences persist over time (see
Figure 6).
To confirm the measurable differences observed between the study groups, their statistical significance was assessed. If the normality of the distribution of the variables was confirmed for both study groups at the α = 0.05 level (parameters YLD (DD) rate F, 1990 and YLD (DD) rate F, 2019), the Brown–Forsythe test was applied to confirm the equality of variance, followed by Student’s
t-test. For variables for which the normality of the distribution was not confirmed for both study groups, i.e., the parameters YLD (DD) rate M, 1990 and YLD (DD) rate M, 2019, the non-parametric Mann–Whitney test was used. The obtained test probability values
p (for α = 0.05) allowed the rejection of the null hypothesis in all cases. This means that the differences in the mean levels of all parameters tested are statistically significant.
Table 5 displays the obtained results.
The extent of variation in the economic burden of depressive disorders across the EU-27 is demonstrated by the relative health gap (RHG) estimates for both old and new EU countries. These estimates reveal existing inequalities in this regard. The RHG (YLD (DD)) index results suggest that residents of the EU-14 area are more likely to experience the negative effects of depressive disorders (long-term disability) compared to residents of the EU-CEE area. In 2019, the RHG (YLD (DD)) index was 1.37 for women and 1.34 for men. Additionally, the results indicate an increase in inequality between 1990 and 2019, with the RHG (YLD (DD)) index being 1.24 for women and 1.27 for men in 1990.
6. Discussion
The impact of mental disorders on national economies presents challenges to achieving health equity in societies. Depressive disorders significantly affect individuals, disrupting their work and family life and increasing the risk of suicide. Maintaining a healthy and productive workforce is becoming increasingly challenging due to ongoing structural changes in the work environment, an ageing workforce, and a growing number of workers experiencing work-related stress. Major Depressive Disorder (MDD) is a prevalent mental disorder worldwide and a leading cause of disability.
The economic impact of health constraints on society is a crucial area of research in health and pharmacoeconomics. Studies on the costs of chronic diseases demonstrate that mental disorders in working-age individuals result in significant costs due to disability, sickness absence, and lost productivity at work. Therefore, it is important to address depression symptoms as they can cause distress and impair social, work, and other important areas of life. However, some individuals may be reluctant to seek treatment due to the stigma surrounding mental health and concerns about potential negative consequences, such as job loss or missed opportunities for promotion. According to
Survey of U.S. Workers Reveals Impact on Productivity from Depression [
54], 64% of participants diagnosed with depression reported that cognitive difficulties, such as difficulty concentrating, indecisiveness, and forgetfulness, had the greatest impact on their ability to perform work-related tasks. Moreover, cognitive challenges were found to exacerbate presenteeism. A significant proportion (58%) of individuals diagnosed with depression chose not to inform their employer due to the risk of losing their job. Additionally, 24% of respondents felt that disclosing this information in the current economic climate was risky.
The analysis shows that depressive disorders have a significant impact on the health of the EU population and limit the economies of EU-27 countries. Therefore, preventive measures in the field of mental health are necessary. The burden of depressive disorders varies among the working-age population in the EU-27, highlighting the need to recognize the specificity of this phenomenon in relation to national conditions. The data indicate that countries with higher levels of socio-economic development experience a greater burden of depressive disorders. Therefore, it is necessary to investigate alternative methods to reduce both the incidence and long-term negative effects of these disorders. In the EU-27 countries, there is a positive correlation between citizens’ wealth and effective policies to reduce the long-term health consequences of chronic non-communicable diseases (NCDs) that cause physical health limitations [
55]. The differences in the burden of depressive disorders between ‘old’ and ‘new’ EU countries suggest that the severity of risk factors increases with the level of economic development of the country. These results are consistent with previous studies on interregional differences in the prevalence of depressive disorders and their sociodemographic determinants, such as those conducted by Gutiérrez-Rojas et al. [
56], Huijts et al. [
57], and Lim et al. [
58]. Arias-de la Torre et al. [
59] demonstrate that depressive disorders are prevalent in Europe, but their prevalence varies significantly between countries. Rai et al. [
60] revealed that individual-level factors account for most of the international variation in depression prevalence, but country-level factors also play a role.
The information provided is based on data prior to 2020, as determined by the availability of NTS-1 comparisons and the specificity of behavioural, social, and economic mental disorders. It is important to note that the COVID-19 pandemic and its associated disruptions to personal and professional life have exacerbated many risk factors associated with poor mental health, leading to an unprecedented decline in mental health [
61]. According to the OECD, the incidence of anxiety and depression in some European countries doubled in 2020 compared to the previous year [
5]. Available data suggest that depressive symptoms were lower in the first half of 2022 than during the peaks in 2020 and 2021 but still higher than before the pandemic [
62]. In France, the isolation period saw a peak in depressive symptoms among adults, with over 20% experiencing symptoms. By May 2022, the rate had fallen to 15%, which is still higher than the pre-pandemic rate of 13.5%. In Belgium, the prevalence of depressive symptoms among adults increased significantly during the peak of the COVID-19 pandemic in 2020 and 2021, reaching at least 20%, compared to less than 10% in 2018. Santomauro et al. [
63] and Twenge and Joiner [
64] confirmed that the burden of major depressive and anxiety disorders increased due to the pandemic. According to Ettman et al. [
65], the prevalence of depressive symptoms in the USA during COVID-19 was more than three times higher than before the pandemic. According to Ettman et al. [
65], the prevalence of depressive symptoms in the USA during COVID-19 was more than three times higher than before the pandemic. Similarly, Żolnierczyk-Zreda [
66] reported a significant increase in depression levels among working Poles between 2019 and 2022, along with an increase in symptom severity, likely due to the pandemic outbreak. Further research is required to estimate the economic and social costs associated with the pandemic.
This study builds upon the existing literature on the impact of mental illness, particularly depressive disorders, on labour productivity. It also draws attention to the inequalities that currently exist within the economies of the EU-27 in this area. The presented approach for addressing the impact of depression on the working-age population, considering the limited number of potentially productive years of life, also serves as a foundation for estimating the measurable economic effects of implementing effective interventions to enhance the mental health of the population.
7. Conclusions
The objective of the study was to assess the impact of depressive disorders on the labour market potential in European Union countries, with a particular focus on the disparities between the ‘old’ and ‘new’ EU Member States. The results show that depressive disorders have a significant impact on potential labour resources in EU economies. An assessment revealed significant differences between the ‘old’ and ‘new’ EU countries, with the former experiencing a considerably more adverse impact. The impact of health determinants on the level of mental health in a group of EU-27 countries, as determined by the level of socio-economic development and institutional differentiation, reveals persistent inequalities between ‘old’ and ‘new’ EU countries. The burden on labour resources due to depressive disorders is higher in ‘old’ EU countries, on average.
The study analysed the convergence of YLD (DD) rates in the 27 EU countries from 1990 to 2019. The results suggest that there was no significant catching-up effect over time for the more favoured economies (EU-CEE) in the system studied. Additionally, the inequalities observed at the beginning of the period analysed have deepened. There are persistent and statistically significant differences between the EU-14 group (the ‘old EU’ countries) and the EU-CEE group (the CEE-EU countries) in the area under study.
The previous literature has primarily examined the impact of mental illness, specifically depressive disorders, on labour productivity. This study contributes to the existing literature by introducing the perspective of inequalities in the field of study among EU-27 economies with varying levels of socio-economic development. The economic effects of effective interventions to improve mental health can be estimated by considering the burden of depression on the working-age population and its impact on potentially productive years of life.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}