
COVID-19 Lockdown Effects on Mood: Impact of Sex, Age, and Underlying Disease

 ,
,  , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Methods
Data Analysis
3. Results
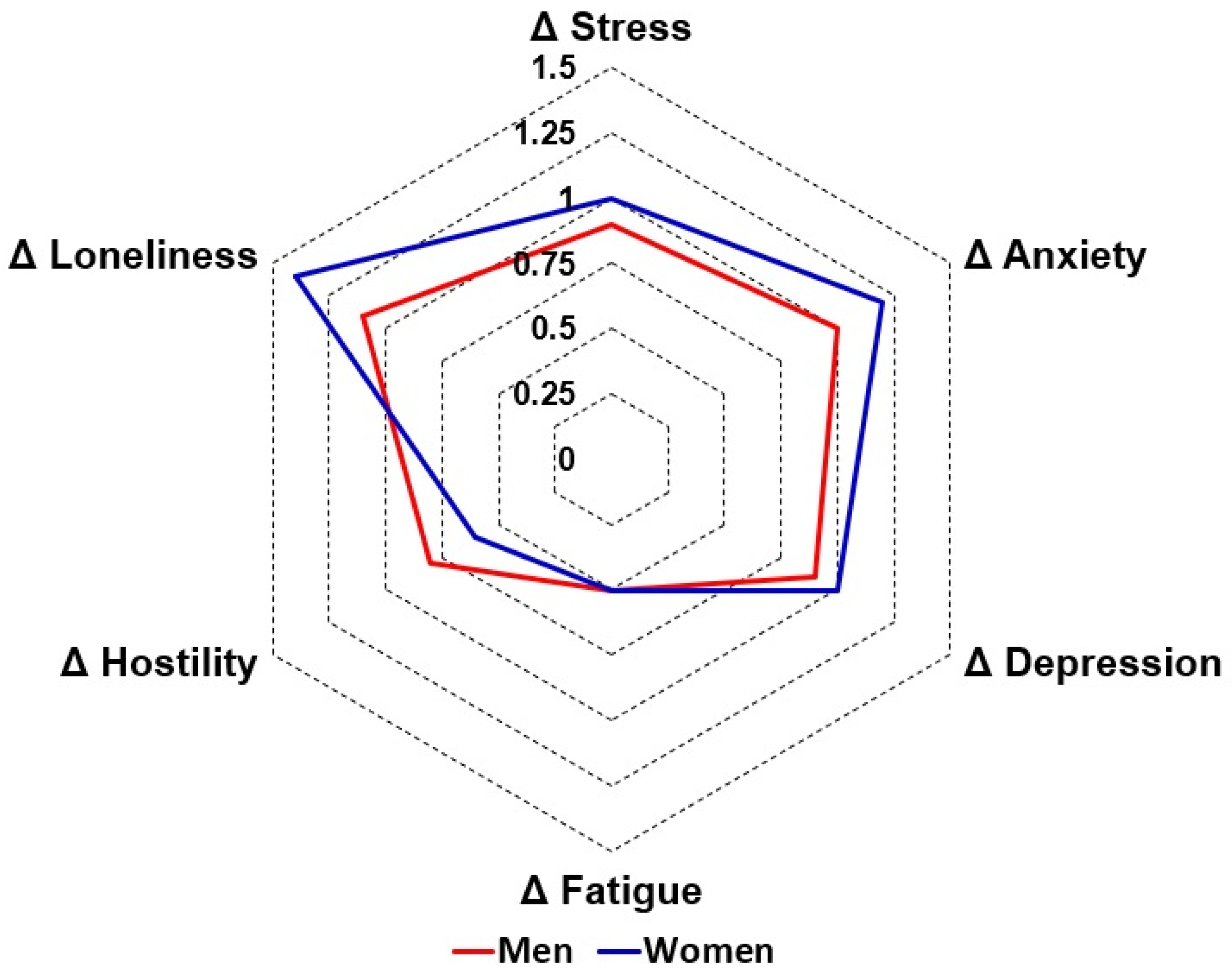
3.1. Sex
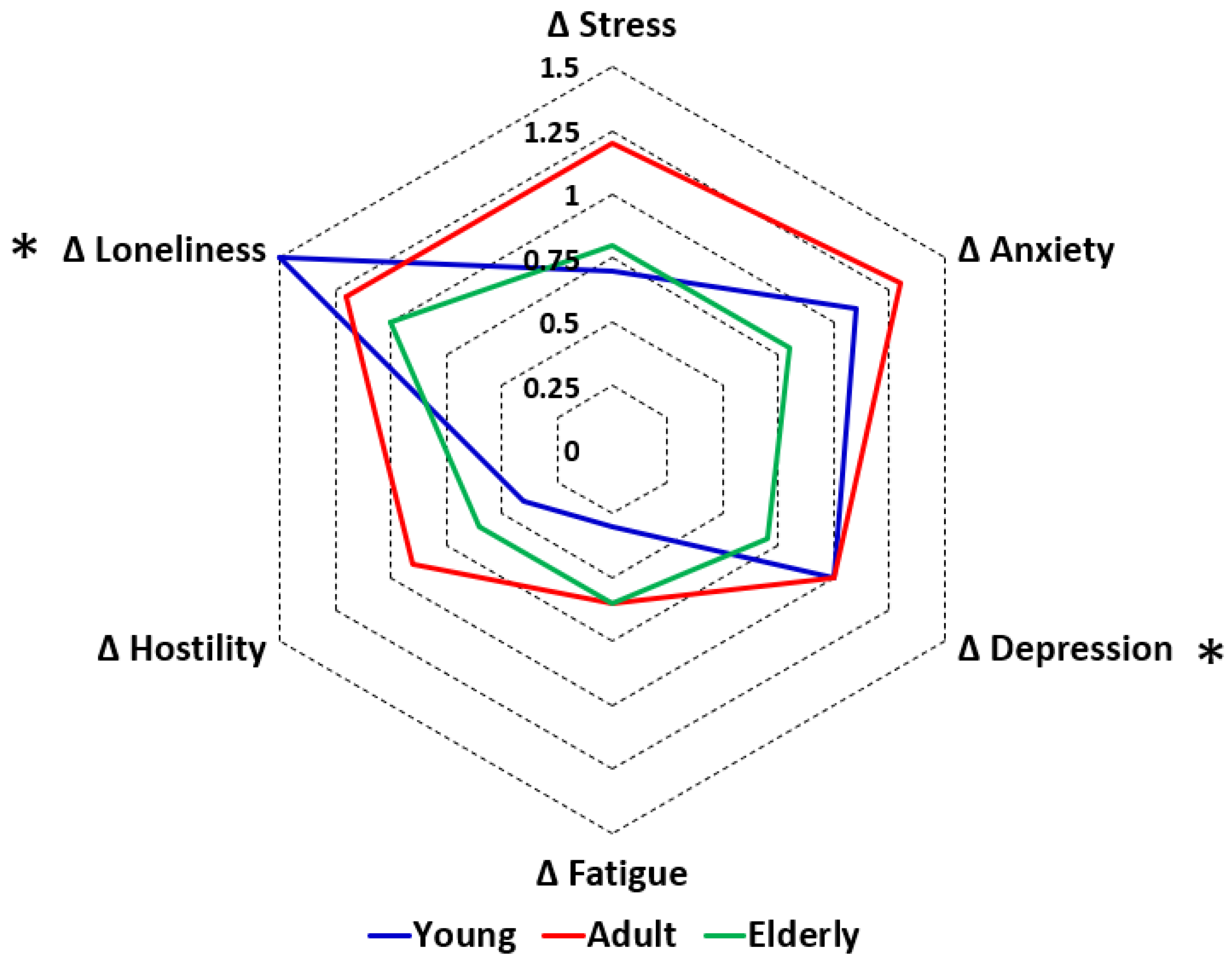
3.2. Age
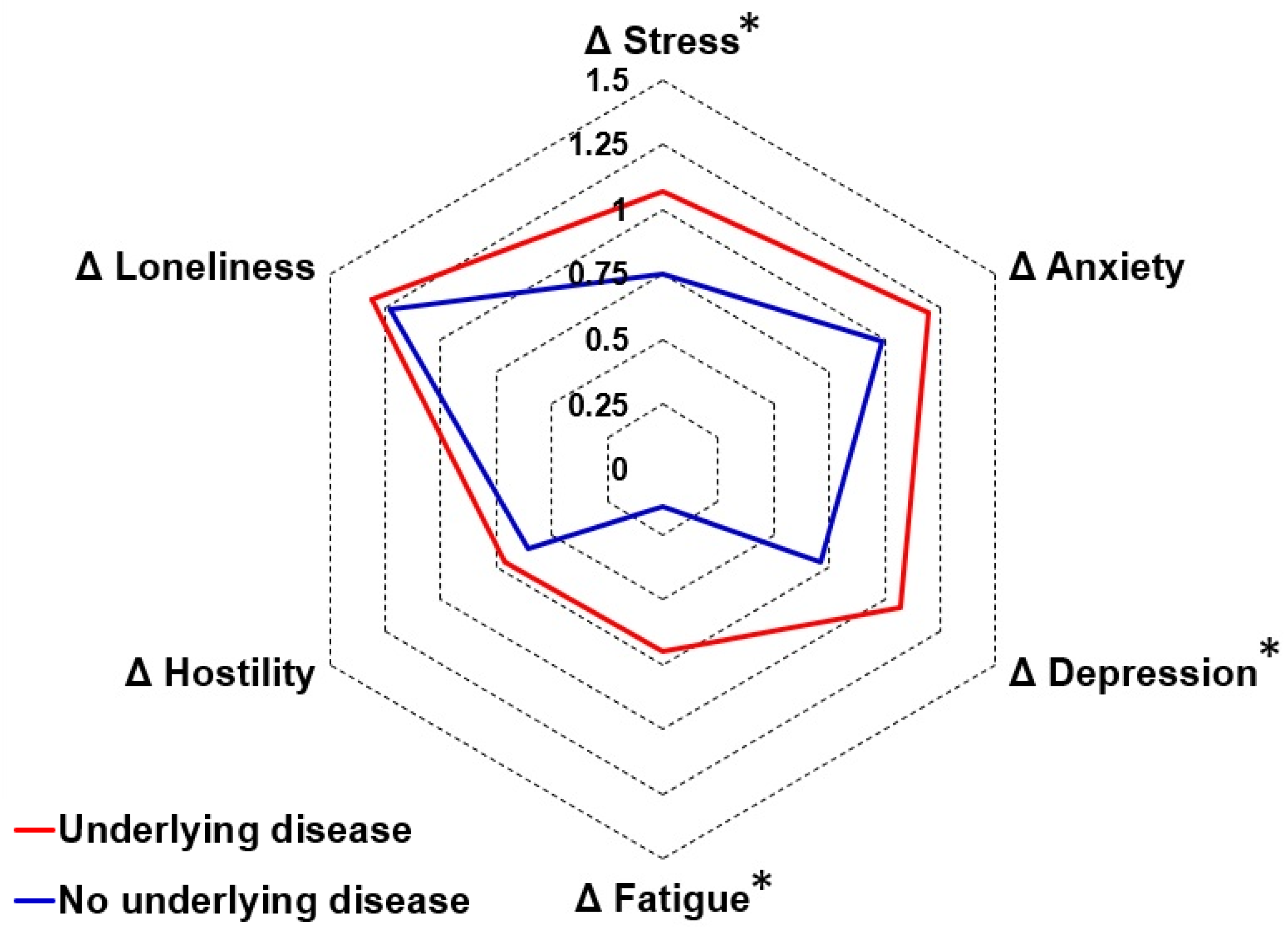
3.3. Underlying Disease
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Before Lockdown | During Lockdown | Difference Score 1 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Sex | Men | Women | p-Value | Men | Women | p-Value | Men | Women | p-Value |
| Mood | |||||||||
| Anxiety | 1.3 (2.0) | 1.8 (2.5) | 0.001 S | 2.2 (2.7) * | 3.1 (3.1) * | <0.001 S | 1.0 (2.0) | 1.2 (2.5) | 0.048 |
| Depression | 1.3 (2.2) | 1.8 (2.5) | 0.001 S | 2.2 (2.9) * | 2.7 (3.1) * | 0.004 S | 0.9 (2.0) | 1.0 (2.2) | 0.423 |
| Loneliness | 1.8 (2.6) | 2.1 (2.6) | 0.026 | 2.9 (3.2) * | 3.5 (3.4) * | 0.001 S | 1.1 (2.3) | 1.4 (2.5) | 0.020 |
| Fatigue | 3.2 (2.8) | 4.2 (3.0) | <0.001 S | 3.7 (2.9) * | 4.7 (3.1) * | <0.001 S | 0.5 (2.1) | 0.5 (2.6) | 0.800 |
| Hostility | 1.0 (2.0) | 0.9 (1.8) | 0.018 | 1.8 (2.7) * | 1.5 (2.5) * | 0.010 | 0.8 (2.0) | 0.6 (1.8) | 0.210 |
| Happiness | 6.9 (2.3) | 6.8 (2.3) | 0.122 | 6.0 (2.5) * | 5.9 (2.5) * | 0.228 | −0.9 (2.0) | −0.9 (2.3) | 0.955 |
| Stress | 2.2 (2.6) | 3.2 (2.9) | <0.001 S | 3.1 (3.1) * | 4.2 (3.1) * | 0.001 S | 0.9 (2.4) | 1.0 (2.8) | 0.658 |
| Lifestyle factors and coping | |||||||||
| Optimism | 3.2 (0.9) | 3.0 (1.0) | 0.039 | 3.0 (1.0) | 2.7 (1.1) * | 0.005 S | −0.2 (0.7) | −0.3 (0.8) | 0.152 |
| Coping with stress | 6.5 (1.5) | 5.7 (1.8) | <0.001 S | 6.2 (1.7) | 5.4 (2.0) * | <0.001 S | −0.3 (1.1) | −0.3 (1.3) | 0.557 |
| Support of family and friends | 5.6 (2.1) | 6.2 (1.8) | 0.001 S | 5.8 (1.9) | 6.3 (1.7) | 0.014 | 0.2 (0.9) | 0.1 (1.0) | 0.004 S |
| Nutrition | 7.5 (3.0) | 7.9 (2.7) | 0.268 | 7.6 (2.8) | 7.5 (2.8) * | 0.518 | 0.1 (1.4) | −0.4 (1.6) | <0.001 S |
| Being active | 6.5 (2.6) | 6.5 (2.5) | 0.780 | 5.6 (2.8) * | 5.4 (2.7) * | 0.148 | −0.9 (2.5) | −1.1 (2.8) | 0.438 |
| Physical activity level | 4.8 (2.1) | 5.2 (2.0) | 0.047 | 4.5 (2.0) | 4.7 (2.1) * | 0.785 | −0.3 (1.6) | −0.6 (1.8) | 0.071 |
| Sleep | 2.8 (1.1) | 2.5 (1.1) | 0.003 S | 2.8 (1.1) | 2.4 (1.2) * | 0.001 S | −0.1 (0.7) | −0.1 (0.8) | 0.333 |
| Health correlates | |||||||||
| Quality of life | 7.2 (2.2) | 7.1 (2.1) | 0.222 | 6.2 (2.4) * | 6.3 (2.4) * | 0.906 | −1.0 (2.0) | −0.9 (2.2) | 0.525 |
| Immune fitness | 7.6 (1.7) | 7.2 (1.9) | <0.001 S | 7.4 (1.8) * | 6.9 (2.1) * | <0.001 S | −0.2 (1.2) | −0.3 (1.3) | 0.582 |
| COVID-19 Symptom—presence | 2.4 (2.1) | 3.9 (4.0) | 0.081 | 2.4 (2.1) | 4.3 (4.4) | 0.010 S | 0.0 (1.8) | 0.1 (2.1) | 0.354 |
| COVID-19 Symptom—severity | 3.3 (3.4) | 2.7 (2.2) | 0.030 S | 3.4 (3.7) | 2.8 (2.3) | 0.001 S | 0.1 (3.4) | 0.4 (4.3) | 0.306 |
| Time Period | Before Lockdown | During Lockdown | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | p-Value Paired Comparison | Mean (SD) | p-Value Paired Comparison | |||||||||
| Age Range | Young (18–35) | Adult (36–65) | Elderly (>65) | Young—Adult | Adult—Elderly | Young—Elderly | Young (18–35) | Adult (36–65) | Elderly (>65) | Young—Adult | Adult—Elderly | Young—Elderly |
| Mood | ||||||||||||
| Anxiety | 2.1 (2.5) | 1.5 (2.4) | 0.9 (1.9) | <0.001 A | 0.002 A | <0.001 A | 3.1 (2.9) * | 2.8 (3.2) * | 1.7 (2.6) * | 0.002 A | <0.001 A | <0.001 A |
| Depression | 2.0 (2.4) | 1.5 (2.4) | 0.9 (1.8) | <0.001 A | 0.001 A | <0.001 A | 3.1 (3.0) * | 2.5 (3.1) * | 1.6 (2.7) * | <0.001 A | <0.001 A | <0.001 A |
| Loneliness | 2.1 (2.4) | 1.9 (2.8) | 1.9 (2.8) | <0.001 A | 0.559 | 0.001 A | 3.7 (3.1) * | 3.1 (3.5) * | 2.9 (3.4) * | <0.001 A | 0.577 | <0.001 A |
| Fatigue | 4.5 (2.7) | 3.7 (3.1) | 2.3 (2.5) | <0.001 A | <0.001 A | <0.001 A | 4.8 (2.7) | 4.4 (3.2) * | 2.9 (2.8) * | 0.016 A | <0.001 A | <0.001 A |
| Hostile | 1.5 (2.4) | 0.9 (1.9) | 0.6 (1.6) | 0.012 A | 0.004 A | <0.001 A | 2.1 (2.4) * | 1.8 (2.8) * | 1.2 (2.4) * | 0.505 | <0.001 A | 0.002 A |
| Happy | 7.0 (1.9) | 6.8 (2.5) | 6.7 (2.6) | - | - | - | 6.1 (2.1) * | 5.8 (2.7) * | 5.9 (2.8) * | - | - | - |
| Stress | 4.1 (2.7) | 2.3 (2.7) | 1.2 (2.1) | <0.001 A | <0.001 A | <0.001 A | 4.8 (2.7) * | 3.6 (3.3) * | 2.0 (2.9) * | <0.001 A | <0.001 A | <0.001 A |
| Lifestyle factors and coping | ||||||||||||
| Optimism | 3.0 (1.0) | 3.1 (1.0) | 3.4 (0.9) | 0.100 | 0.008 A | <0.001 A | 2.7 (1.0) * | 2.9 (1.1) * | 3.2 (0.9) | 0.011 A | 0.008 A | <0.001 A |
| Coping with stress | 5.5 (1.7) | 6.2 (1.7) | 6.8 (1.3) | <0.001 A | 0.005 A | <0.001 A | 5.2 (1.8) * | 5.9 (2.0) * | 6.6 (1.5) * | 0.001 A | 0.010 A | 0.001 A |
| Support of family and friends | 6.3 (1.8) | 5.8 (2.0) | 5.6 (1.9) | 0.018 | 0.263 | 0.003 A | 6.4 (1.6) | 5.9 (1.9) * | 5.9 (1.7) * | - | - | - |
| Nutrition | 8.3 (2.8) | 7.1 (2.7) | 8.1 (2.7) | <0.001 A | 0.007 A | 0.588 | 7.9 (2.8) * | 7.0 (2.8) | 7.9 (2.7) | 0.001 A | 0.006 A | 0.900 |
| Being active | 6.7 (2.2) | 6.5 (2.7) | 6.2 (2.8) | - | - | - | 5.5 (2.4) * | 5.5 (2.9) * | 5.6 (2.9) * | - | - | - |
| Physical activity level | 5.4 (2.0) | 5.0 (2.1) | 4.4 (2.1) | 0.018 | 0.042 | <0.001 A | 4.6 (2.1) * | 4.7 (2.1) * | 4.4 (2.1) | - | - | - |
| Sleep | 2.7 (1.0) | 2.6 (1.2) | 2.9 (1.2) | - | - | - | 2.6 (1.0) | 2.5 (1.3) | 2.7 (1.2) | - | - | - |
| Health correlates | ||||||||||||
| Quality of life | 7.3 (1.8) | 7.1 (2.3) | 7.2 (2.4) | - | - | - | 6.3 (2.1) * | 6.2 (2.7) * | 6.5 (2.5) * | - | - | - |
| Immune fitness | 7.4 (1.7) | 7.2 (2.1) | 7.5 (1.7) | - | - | - | 7.2 (1.8) | 6.9 (2.2) * | 7.2 (2.0) * | - | - | - |
| COVID-19 Symptom—presence | 2.8 (2.2) | 2.4 (2.2) | 2.4 (1.8) | 0.002 A | 0.634 | 0.063 | 2.8 (2.2) | 2.6 (2.4) * | 2.3 (1.8) | - | - | - |
| COVID-19 Symptom—severity | 4.0 (3.8) | 3.5 (3.9) | 3.5 (3.3) | 0.011 A | 0.476 | 0.242 | 4.1 (4.2) | 4.1 (4.5) * | 3.5 (3.5) | - | - | - |
| Difference Score 1 | p-Value | ||||||
|---|---|---|---|---|---|---|---|
| Age Range | Young (18–35) | Adult (36–65) | Elderly (>65) | Overall | Young—Adult | Adult—Elderly | Young—Elderly |
| Mood | |||||||
| Anxiety | 1.1 (2.3) | 1.3 (2.6) | 0.8 (1.7) | 0.009 | - | - | - |
| Depression | 1.0 (2.2) | 1.0 (2.2) | 0.7 (1.7) | 0.004 A | 0.002 A | 0.183 | 0.014 |
| Loneliness | 1.5 (2.4) | 1.2 (2.5) | 1.0 (2.3) | <0.001 A | <0.001 A | 0.790 | <0.001 A |
| Fatigue | 0.3 (2.7) | 0.6 (2.3) | 0.6 (1.7) | 0.249 | - | - | - |
| Hostility | 0.4 (1.5) | 0.9 (2.2) | 0.6 (1.8) | 0.017 | - | - | - |
| Happiness | −0.9 (2.1) | −1.0 (2.3) | -0.8 (1.9) | 0.288 | - | - | - |
| Stress | 0.7 (2.8) | 1.2 (2.7) | 0.8 (2.0) | 0.030 | - | - | - |
| Lifestyle factors and coping | |||||||
| Optimism | −0.3 (0.9) | −0.2 (0.6) | −0.1 (0.6) | 0.071 | - | - | - |
| Coping with stress | −0.3 (1.5) | −0.3 (1.0) | −0.3 (0.9) | 0.759 | - | - | - |
| Support of family and friends | 0.1 (1.1) | 0.1 (1.0) | 0.3 (0.6) | 0.140 | - | - | - |
| Nutrition | −0.4 (2.0) | −0.1 (1.4) | −0.1 (0.8) | 0.214 | - | - | - |
| Being active | −1.2 (3.0) | −1.0 (2.6) | −0.6 (2.1) | 0.005 A | 0.023 | 0.142 | 0.002 A |
| Physical activity level | −0.8 (2.1) | −0.3 (1.5) | 0.0 (1.2) | <0.001 A | 0.002 A | 0.108 | <0.001 A |
| Sleep | −0.1 (1.0) | −0.1 (0.6) | −0.1 (0.5) | 0.445 | - | - | - |
| Health correlates | |||||||
| Quality of life | −1.0 (1.9) | −0.9 (2.4) | −0.7 (1.9) | 0.013 A | 0.092 | 0.087 | 0.004 A |
| Immune fitness | −0.2 (1.3) | −0.2 (1.3) | −0.3 (1.2) | 0.422 | - | - | - |
| COVID-19 Symptom—presence | 0.0 (2.1) | 0.2 (2.0) | 0.0 (1.1) | 0.194 | - | - | - |
| COVID-19 Symptom—severity | 0.1 (4.2) | 0.5 (4.2) | 0.0 (2.4) | 0.332 | - | - | - |
| Before Lockdown | During Lockdown | Difference Score 1 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Underlying Disease | Yes | No | p-Value | Yes | No | p-Value | Yes | No | p-Value |
| Mood | |||||||||
| Anxiety | 2.0 (2.6) | 1.0 (1.8) | <0.001 U | 3.2 (3.1) * | 2.0 (2.6) * | <0.001 U | 1.2 (2.5) | 1.0 (2.0) | 0.086 |
| Depression | 1.9 (2.6) | 1.0 (1.7) | <0.001 U | 3.0 (3.2) * | 1.7 (2.4) * | <0.001 U | 1.1 (2.2) | 0.7 (1.9) | 0.003 U |
| Loneliness | 2.3 (2.8) | 1.3 (2.1) | <0.001 U | 3.7 (3.5) * | 2.6 (3.0) * | <0.001 U | 1.3 (2.5) | 1.2 (2.4) | 0.427 |
| Fatigue | 4.2 (3.0) | 3.1 (2.7) | <0.001 U | 4.9 (3.0) * | 3.2 (2.7) | <0.001 U | 0.7 (2.5) | 0.1 (2.3) | <0.001 U |
| Hostility | 1.0 (2.0) | 0.7 (1.6) | 0.001 U | 1.8 (2.7) * | 1.3 (2.4) * | <0.001 U | 0.7 (1.9) | 0.6 (1.8) | 0.232 |
| Happiness | 6.7 (2.4) | 7.2 (2.1) | <0.001 U | 5.7 (2.5) * | 6.4 (2.3) * | <0.001 U | −1.0 (2.3) | −0.8 (1.9) | 0.027 |
| Stress | 3.0 (2.9) | 2.5 (2.6) | 0.003 U | 4.1 (3.2) * | 3.2 (2.9) * | <0.001 U | 1.1 (2.8) | 0.8 (2.5) | 0.006 U |
| Lifestyle factors and coping | |||||||||
| Optimism | 3.0 (1.0) | 3.3 (0.8) | 0.001 U | 2.7 (1.1) * | 3.0 (0.9) * | 0.013 | −0.2 (0.7) | −0.43 (0.7) | 0.218 |
| Coping with stress | 5.8 (1.8) | 6.4 (1.6) | <0.001 U | 5.5 (2.0) * | 6.1 (1.6) | 0.001 U | −0.3 (1.2) | −0.3 (1.3) | 0.440 |
| Support of family and friends | 5.8 (1.9) | 6.3 (1.9) | 0.004 U | 6.0 (1.7) * | 6.3 (1.9) | 0.028 | 0.2 (1.0) | 0.0 (1.0) | 0.015 |
| Nutrition | 7.6 (2.8) | 8.1 (2.8) | 0.047 | 7.2 (2.8) * | 8.1 (2.7) | 0.001 U | −0.4 (1.7) | 0.0 (1.4) | 0.030 |
| Being active | 6.4 (2.6) | 6.8 (2.5) | 0.003 U | 5.3 (2.7) * | 5.9 (2.7) * | <0.001 U | −1.1 (2.8) | −0.9 (2.5) | 0.151 |
| Physical activity level | 4.9 (2.0) | 5.4 (2.1) | 0.009 | 4.4 (2.1) * | 4.9 (2.1) * | 0.017 | −0.5 (1.8) | −0.5 (1.8) | 0.658 |
| Sleep | 2.5 (1.2) | 3.0 (0.9) | <0.001 U | 2.4 (1.2) | 2.9 (0.9) | <0.001 U | −0.1 (0.7) | −0.1 (0.8) | 0.914 |
| Health correlates | |||||||||
| Quality of life | 7.0 (2.2) | 7.5 (2.0) | <0.001 U | 6.0 (2.5) * | 6.8 (2.3) * | <0.001 U | −1.0 (2.2) | −0.8 (1.9) | 0.106 |
| Immune fitness | 7.0 (1.9) | 7.9 (1.5) | <0.001 U | 6.7 (2.1) * | 7.8 (1.6) * | <0.001 U | −0.3 (1.4) | −0.1 (1.1) | 0.244 |
| COVID-19 Symptom—presence | 2.9 (2.2) | 2.0 (2.0) | <0.001 U | 3.0 (2.3) | 2.0 (1.9) | <0.001 U | 0.2 (2.0) | −0.1 (1.9) | 0.331 |
| COVID-19 Symptom—severity | 4.3 (4.0) | 2.6 (3.0) | <0.001 U | 4.7 (4.5) * | 2.6 (3.4) | <0.001 U | 0.4 (4.2) | 0.0 (3.5) | 0.167 |
References
- Panchal, U.; Salazar de Pablo, G.; Franco, M.; Moreno, C.; Parellada, M.; Arango, C.; Fusar-Poli, P. The impact of COVID-19 lockdown on child and adolescent mental health: Systematic review. Eur. Child. Adolesc. Psychiatry 2023, 32, 1151–1177. [Google Scholar] [CrossRef]
- Cénat, J.M.; Blais-Rochette, C.; Kokou-Kpolou, C.K.; Noorishad, P.G.; Mukunzi, J.N.; McIntee, S.E.; Dalexis, R.D.; Goulet, M.A.; Labelle, P.R. Prevalence of symptoms of depression, anxiety, insomnia, posttraumatic stress disorder, and psychological distress among populations affected by the COVID-19 pandemic: A systematic review and meta-analysis. Psychiatry Res. 2021, 295, 113599. [Google Scholar] [CrossRef] [PubMed]
- Solé, B.; Verdolini, N.; Amoretti, S.; Montejo, L.; Rosa, A.R.; Hogg, B.; Garcia-Rizo, C.; Mezquida, G.; Bernardo, M.; Martinez-Aran, A.; et al. Effects of the COVID-19 pandemic and lockdown in Spain: Comparison between community controls and patients with a psychiatric disorder. Preliminary results from the BRIS-MHC STUDY. J. Affect. Disord. 2021, 281, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Fullana, M.A.; Hidalgo-Mazzei, D.; Vieta, E.; Radua, J. Coping behaviors associated with decreased anxiety and depressive symptoms during the COVID-19 pandemic and lockdown. J. Affect. Disord. 2020, 275, 80–81. [Google Scholar] [CrossRef] [PubMed]
- Petzold, M.B.; Bendau, A.; Plag, J.; Pyrkosch, L.; Mascarell Maricic, L.; Betzler, F.; Rogoll, J.; Große, J.; Ströhle, A. Risk, resilience, psychological distress, and anxiety at the beginning of the COVID-19 pandemic in Germany. Brain Behav. 2020, 10, e01745. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Hendriksen, P.A.; Kiani, P.; Garssen, J.; Bruce, G.; Verster, J.C. Living alone or together during lockdown: Association with mood, immune fitness and experiencing COVID-19 symptoms. Psychol. Res. Behav. Manag. 2021, 14, 1947–1957. [Google Scholar] [CrossRef] [PubMed]
- Kaur, W.; Balakrishnan, V.; Chen, Y.Y.; Periasamy, J. Mental health risk factors and coping strategies among students in Asia Pacific during COVID-19 pandemic—A scoping review. Int. J. Environ. Res. Public Health 2022, 19, 8894. [Google Scholar] [CrossRef]
- Merlo, A.; Severeijns, N.R.; Benson, S.; Scholey, A.; Garssen, J.; Bruce, G.; Verster, J.C. Mood and changes in alcohol consumption in young adults during COVID-19 lockdown: A model explaining associations with perceived immune fitness and experiencing COVID-19 symptoms. Int. J. Environ. Res. Public Health 2021, 18, 10028. [Google Scholar] [CrossRef]
- Statistics Netherlands. Overledenen; Geslacht en Leeftijd, per Week. 2023. Available online: https://opendata.cbs.nl/statline/#/CBS/nl/dataset/70895ned/table?fromstatweb (accessed on 1 November 2020).
- National Institute for Public Health and the Environment (RIVM). Available online: https://www.rivm.nl/en/node/154271 (accessed on 1 November 2020).
- Lee, K.; Jeong, G.-C.; Yim, J. Consideration of the Psychological and Mental Health of the Elderly during COVID-19: A Theoretical Review. Int. J. Environ. Res. Public Health 2020, 17, 8098. [Google Scholar] [CrossRef]
- Kompaniyets, L.; Pennington, A.F.; Goodman, A.B.; Rosenblum, H.G.; Belay, B.; Ko, J.Y.; Chevinsky, J.R.; Schieber, L.Z.; Summers, A.D.; Lavery, A.M.; et al. Underlying medical conditions and severe illness among 540,667 adults hospitalized with COVID-19, March 2020–March 2021. Prev. Chronic Dis. 2021, 18, 210123. [Google Scholar] [CrossRef]
- Phillips, L.J.; Francey, S.M.; Edwards, J.; McMurray, N. Strategies used by psychotic individuals to cope with life stress and symptoms of illness: A systematic review. Anxiety Stress Coping 2009, 22, 371–410. [Google Scholar] [CrossRef]
- Kozloff, N.; Mulsant, B.H.; Stergiopoulos, V.; Voineskos, A.N. The COVID-19 global pandemic: Implications for people with schizophrenia and related disorders. Schizophr. Bull. 2020, 46, 752–757. [Google Scholar] [CrossRef]
- Nam, S.H.; Nam, J.H.; Kwon, C.Y. Comparison of the mental health impact of COVID-19 on vulnerable and non-vulnerable groups: A systematic review and meta-analysis of observational studies. Int. J. Environ. Res. Public Health 2021, 18, 10830. [Google Scholar] [CrossRef]
- Carstensen, L.L.; Shavit, Y.Z.; Barnes, J.T. Age advantages in emotional experience persist even under threat from the COVID-19 pandemic. Psychol. Sci. 2020, 31, 1374–1385. [Google Scholar] [CrossRef]
- Ceccato, I.; Palumbo, R.; Di Crosta, A.; La Malva, P.; Marchetti, D.; Maiella, R.; Verrocchio, M.C.; Marin, A.; Mammarella, N.; Palumbo, R.; et al. Age-related differences in the perception of COVID-19 emergency during the Italian outbreak. Aging Ment. Health 2021, 25, 1305–1313. [Google Scholar] [CrossRef] [PubMed]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A Nationwide survey of psychological distress among Italian people during the COVID-19 pandemic: Immediate psychological responses and associated factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef] [PubMed]
- Power, E.; Hughes, S.; Cotter, D.; Cannon, M. Youth mental health in the time of COVID-19. Ir. J. Psychol. Med. 2020, 37, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Carbone, E.; Palumbo, R.; Sella, E.; Lenti, G.; Di Domenico, A.; Borella, E. Emotional, psychological, and cognitive changes throughout the COVID-19 pandemic in Italy: Is there an advantage of being an older adult? Front. Aging Neurosci. 2021, 13, 712369. [Google Scholar] [CrossRef] [PubMed]
- Bruine de Bruin, W. Age differences in COVID-19 risk perceptions and mental health: Evidence from a National, U.S. survey conducted in March 2020. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, e24–e29. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.C.; Nguyen, M.H.; Do, B.N.; Tran, C.Q.; Nguyen, T.T.P.; Pham, K.M.; Pham, L.V.; Tran, K.V.; Duong, T.T.; Tran, T.V.; et al. People with suspected COVID-19 symptoms were more likely depressed and had lower health-related quality of life: The potential benefit of health literacy. J. Clin. Med. 2020, 31, 965. [Google Scholar] [CrossRef]
- Lei, L.; Huang, X.; Zhang, S.; Yang, J.; Yang, L.; Xu, M. Comparison of prevalence and associated factors of anxiety and depression among people affected by versus people unaffected by quarantine during the COVID-19 epidemic in Southwestern China. Med. Sci. Monit. 2020, 26, e924609. [Google Scholar] [CrossRef]
- Sepúlveda-Loyola, W.; Rodríguez-Sánchez, I.; Pérez-Rodríguez, P.; Ganz, F.; Torralba, R.; Oliveira, D.V.; Rodríguez-Mañas, L. Impact of social isolation due to COVID-19 on health in older people: Mental and physical effects and recommendations. J. Nutr. Health Aging 2020, 24, 938–947. [Google Scholar] [CrossRef]
- Santini, Z.I.; Jose, P.E.; Cornwell, E.Y.; Koyanagi, A.; Nielsen, L.; Hinrichsen, C.; Meilstrup, C.; Madsen, K.R.; Koushede, V. Social disconnectedness, perceived isolation, and symptoms of depression and anxiety among older Americans (NSHAP): A longitudinal mediation analysis. Lancet Public Health 2020, 5, e62–e70. [Google Scholar] [CrossRef]
- Dalise, S.; Tramonti, F.; Armienti, E.; Niccolini, V.; Caniglia Tenaglia, M.; Morganti, R.; Chisari, C. Psycho-social impact of social distancing and isolation due to the COVID-19 containment measures on patients with physical disabilities. Eur. J. Phys. Rehabil. Med. 2021, 57, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Sud, A.; Jones, M.E.; Broggio, J.; Loveday, C.; Torr, B.; Garrett, A.; Nicol, D.L.; Jhanji, S.; Boyce, S.A.; Gronthoud, F.; et al. Collateral damage: The impact on outcomes from cancer surgery of the COVID-19 pandemic. Ann. Oncol. 2020, 31, 1065–1074. [Google Scholar] [CrossRef]
- Negrini, S.; Grabljevec, K.; Boldrini, P.; Kiekens, C.; Moslavac, S.; Zampolini, M.; Christodoulou, N. Up to 2.2 million people experiencing disability suffer collateral damage each day of COVID-19 lockdown in Europe. Eur. J. Phys. Rehabil. Med. 2020, 56, 361–365. [Google Scholar] [CrossRef]
- Physical, E.; Alliance, R.M.B. White book on physical and rehabilitation medicine in Europe. Chapter 2. Why rehabilitation is needed by individual and society. Eur. J. Phys. Rehabil. Med. 2018, 54, 166–176. [Google Scholar]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiat. 2020, 33, e100213. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Ma, Z.F. Impact of the COVID-19 Pandemic on Mental Health and Quality of Life among Local Residents in Liaoning Province, China: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 2381. [Google Scholar] [CrossRef]
- Zaninotto, P.; Iob, E.; Demakakos, P.; Steptoe, A. Immediate and longer-term changes in the mental health and well-being of older adults in England during the COVID-19 pandemic. JAMA Psychiatry 2022, 79, 151–159. [Google Scholar] [CrossRef]
- Verster, J.C.; Kraneveld, A.D.; Garssen, J. The assessment of immune fitness. J. Clin. Med. 2023, 12, 22. [Google Scholar] [CrossRef]
- Kiani, P.; Balikji, J.; Kraneveld, A.D.; Garssen, J.; Bruce, G.; Verster, J.C. Pandemic preparedness: The importance of adequate immune fitness. J. Clin. Med. 2022, 11, 2442. [Google Scholar] [CrossRef] [PubMed]
- Kiani, P.; Merlo, A.; Saeed, H.M.; Benson, S.; Bruce, G.; Hoorn, R.; Kraneveld, A.D.; Severeijns, N.R.; Sips, A.S.M.; Scholey, A.; et al. Immune fitness, and the psychosocial and health consequences of the COVID-19 pandemic lockdown in The Netherlands: Methodology and design of the CLOFIT study. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 199–218. [Google Scholar] [CrossRef]
- National Institute for Public Health and the Environment (RIVM). Aandoeningen—Welke Aandoeningen Hebben we in de Toekomst? Available online: https://www.vtv2018.nl/aandoeningen (accessed on 5 October 2020).
- Verster, J.C.; Sandalova, E.; Garssen, J.; Bruce, G. The use of single-item ratings versus traditional multiple-item questionnaires to assess mood and health. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 183–198. [Google Scholar] [CrossRef]
- De Boer, A.G.; van Lanschot, J.J.; Stalmeier, P.F.; van Sandick, J.W.; Hulscher, J.B.; de Haes, J.C.; Sprangers, M.A. Is a single-item visual analogue scale as valid, reliable and responsive as multi-item scales in measuring quality of life? Qual. Life Res. 2004, 13, 311–320. [Google Scholar] [CrossRef] [PubMed]
- Verster, J.C.; Mulder, K.E.W.; Hendriksen, P.A.; Verheul, M.C.E.; van Oostrom, E.C.; Scholey, A.; Garssen, J. Test-retest reliability of single-item assessments of immune fitness, mood and quality of life. Heliyon 2023, 9, e15280. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D.M.C.; Nielsen, E.; Ciliska, D. Lifestyle assessment: Testing the FANTASTIC Instrument. Can. Fam. Physician 1984, 30, 1863–1866. [Google Scholar]
- Sharratt, J.K.; Sharratt, M.T.; Smith, D.M.; Howell, N.J.; Davenport, L. FANTASTIC Lifestyle survey of University of Waterloo employees. Can. Fam. Physician 1984, 30, 1869–1872. [Google Scholar]
- Wilson, D.M.C.; Ciliska, D. Development and use of the FANTASTIC checklist. Can. Fam. Physician 1984, 30, 1527–1532. [Google Scholar]
- Canadian Society for Exercise Physiology. Fantastic Lifestyle Checklist. Available online: https://rowingbc.ca/wp-content/uploads/2016/12/Fantastic-Lifestyle-Checklist.pdf (accessed on 10 October 2020).
- Hendriksen, P.A.; Garssen, J.; Bijlsma, E.Y.; Engels, F.; Bruce, G.; Verster, J.C. COVID-19 lockdown-related changes in mood, health and academic functioning. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 1440–1461. [Google Scholar] [CrossRef] [PubMed]
- Balikji, J.; Koyun, A.H.; Hendriksen, P.A.; Kiani, P.; Stock, A.-K.; Garssen, J.; Hoogbergen, M.M.; Verster, J.C. The impact of COVID-19 lockdowns in Germany on mood, attention control, immune fitness, and quality of life of young adults with self-reported impaired wound healing. J. Clin. Med. 2023, 12, 3205. [Google Scholar] [CrossRef] [PubMed]
- AlSamman, M.; Caggiula, A.; Ganguli, S.; Misak, M.; Pourmand, A. Non-respiratory presentations of COVID-19, a clinical review. Am. J. Emerg. Med. 2020, 38, 2444–2454. [Google Scholar] [CrossRef]
- De Haan, L.; de Haan, H.; Olivier, B.; Verster, J.C. Alcohol mixed with energy drinks: Methodology and design of the Utrecht Student Survey. Int. J. Gen. Med. 2012, 5, 889–898. [Google Scholar]



| Overall | Men | Women | p-Value | |
|---|---|---|---|---|
| N (%) | 1415 (100%) | 503 (35.5%) | 912 (64.5%) | <0.001 * |
| Age (year) | 45.0 (18.5) | 49.7 (18.4) | 42.4 (18.0) | <0.001 * |
| Height (m) | 1.73 (0.09) | 1.80 (0.08) | 1.69 (0.07) | <0.001 * |
| Weight (kg) | 79.3 (18.8) | 87.6 (17.4) | 74.8 (17.9) | <0.001 * |
| BMI (kg/m2) | 26.4 (5.8) | 26.9 (5.3) | 26.2 (6.1) | <0.001 * |
| Before COVID-19 | During Lockdown | p-Value | |
|---|---|---|---|
| Mood | |||
| Anxiety | 1.6 (2.4) | 2.8 (3.0) | <0.001 * |
| Depression | 1.6 (2.4) | 2.6 (3.1) | <0.001 * |
| Fatigue | 3.8 (2.9) | 4.3 (3.0) | <0.001 * |
| Loneliness | 2.0 (2.6) | 3.3 (3.4) | <0.001 * |
| Hostile | 0.9 (1.9) | 1.6 (2.6) | <0.001 * |
| Happy | 6.8 (2.3) | 5.9 (2.5) | <0.001 * |
| Stress | 2.8 (2.8) | 3.8 (3.1) | <0.001 * |
| Lifestyle factors and coping 1 | |||
| Optimism | 3.1 (1.0) | 2.8 (1.1) | <0.001 * |
| Coping with stress | 6.0 (1.7) | 5.7 (1.9) | <0.001 * |
| Support of family and friends | 6.0 (1.9) | 6.1 (1.8) | <0.001 * |
| Nutrition | 7.8 (2.8) | 7.5 (2.8) | <0.001 * |
| Being active | 6.5 (2.5) | 5.5 (2.7) | <0.001 * |
| Physical activity level | 5.1 (2.0) | 4.6 (2.1) | <0.001 * |
| Sleep | 2.7 (1.1) | 2.5 (1.2) | 0.001 * |
| Health correlates | |||
| Quality of life | 7.2 (2.2) | 6.3 (2.4) | <0.001 * |
| Immune fitness | 7.3 (1.9) | 7.1 (2.0) | <0.001 * |
| COVID-19 Symptoms—number | 2.6 (2.1) | 2.7 (2.2) | 0.265 |
| COVID-19 Symptoms—severity | 3.7 (3.8) | 4.0 (4.2) | 0.018 * |
| Δ Immune Fitness | Δ COVID-19 Number of Symptoms | Δ COVID-19 Symptom Severity | ||||
|---|---|---|---|---|---|---|
| r | p-Value | r | p-Value | r | p-Value | |
| Mood | ||||||
| Δ Anxiety | −0.225 | <0.001 * | 0.041 | 0.194 | 0.045 | 0.147 |
| Δ Depression | −0.291 | <0.001 * | 0.149 | <0.001 * | 0.151 | <0.001 * |
| Δ Fatigue | −0.304 | <0.001 * | 0.116 | <0.001 * | 0.151 | <0.001 * |
| Δ Loneliness | −0.242 | <0.001 * | 0.104 | <0.001 * | 0.098 | 0.002 * |
| Δ Hostile | −0.183 | <0.001 * | 0.064 | 0.040 | 0.065 | 0.039 |
| Δ Happy | 0.299 | <0.001 * | −0.107 | 0.001 * | −0.109 | 0.001 * |
| Δ Stress | −0.279 | <0.001 * | 0.109 | <0.001 * | 0.113 | <0.001 * |
| Lifestyle factors and coping 1 | ||||||
| Optimism | 0.239 | <0.001 * | −0.103 | 0.020 | −0.095 | 0.032 |
| Coping with stress | 0.341 | <0.001 * | −0.161 | <0.001 * | −0.197 | <0.001 * |
| Support of family and friends | 0.117 | 0.008 | −0.049 | 0.271 | −0.016 | 0.711 |
| Nutrition | 0.222 | <0.001 * | −0.017 | 0.695 | −0.052 | 0.241 |
| Being active | 0.348 | <0.001 * | −0.087 | 0.006 * | −0.106 | <0.001 * |
| Physical activity level | 0.278 | <0.001 * | −0.172 | <0.001 * | −0.193 | <0.001 * |
| Sleep | 0.307 | <0.001 * | −0.151 | 0.001 * | −0.185 | <0.001 * |
| Health correlates | ||||||
| Δ Quality of life | 0.326 | <0.001 * | −0.061 | 0.052 | −0.082 | 0.009 * |
| Δ Immune fitness | - | 0.160 | <0.001 * | −0.165 | <0.001 * | |
| Δ COVID-19 Symptoms—number | −0.160 | <0.001 * | - | - | 0.905 | <0.001 * |
| Δ COVID-19 Symptoms—severity | −0.165 | <0.001 * | 0.905 | <0.001 * | - | - |
| Underlying Disease | Overall | Alone | In Combination | |||
|---|---|---|---|---|---|---|
| Type | N | % | N | % | N | % |
| Allergy | 322 | 35.0% | 135 | 41.9% | 187 | 58.1% |
| Cardiovascular | 230 | 25.0% | 74 | 32.2% | 156 | 67.8% |
| Sleep disorders | 188 | 20.4% | 45 | 23.9% | 143 | 76.1% |
| Lung | 176 | 19.1% | 45 | 25.6% | 131 | 74.4% |
| Depression | 147 | 16.0% | 22 | 15.0% | 125 | 85.0% |
| Neurological | 115 | 12.5% | 32 | 27.8% | 83 | 72.2% |
| Diabetes | 114 | 12.4% | 28 | 24.6% | 86 | 75.4% |
| Immune | 113 | 12.3% | 38 | 33.6% | 75 | 66.4% |
| Anxiety | 85 | 9.2% | 10 | 11.8% | 75 | 88.2% |
| Psychiatric—other 1 | 35 | 3.8% | 19 | 54.3% | 16 | 45.7% |
| Pain | 31 | 3.4% | 19 | 61.3% | 12 | 38.7% |
| Other 2 | 31 | 3.4% | 24 | 77.4% | 7 | 22.6% |
| Kidney | 25 | 2.7% | 4 | 16.0% | 21 | 84.0% |
| Endocrinologic | 23 | 2.5% | 17 | 73.9% | 6 | 26.1% |
| Liver | 11 | 1.2% | 1 | 9.1 | 10 | 90.9% |
| Gastrointestinal | 10 | 1.1% | 5 | 50.0% | 5 | 50.0% |
| Overall underlying disease | 920 | 65.5% | 518 | 56.3% | 402 | 43.7% |
| No underlying disease | 484 | 34.5% | 484 | 100% | 0 | 0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiani, P.; Hendriksen, P.A.; Balikji, J.; Severeijns, N.R.; Sips, A.S.M.; Bruce, G.; Garssen, J.; Verster, J.C. COVID-19 Lockdown Effects on Mood: Impact of Sex, Age, and Underlying Disease. Psychiatry Int. 2023, 4, 307-323. https://doi.org/10.3390/psychiatryint4040030
Kiani P, Hendriksen PA, Balikji J, Severeijns NR, Sips ASM, Bruce G, Garssen J, Verster JC. COVID-19 Lockdown Effects on Mood: Impact of Sex, Age, and Underlying Disease. Psychiatry International. 2023; 4(4):307-323. https://doi.org/10.3390/psychiatryint4040030
Chicago/Turabian StyleKiani, Pantea, Pauline A. Hendriksen, Jessica Balikji, Noortje R. Severeijns, Annabel S. M. Sips, Gillian Bruce, Johan Garssen, and Joris C. Verster. 2023. "COVID-19 Lockdown Effects on Mood: Impact of Sex, Age, and Underlying Disease" Psychiatry International 4, no. 4: 307-323. https://doi.org/10.3390/psychiatryint4040030
APA StyleKiani, P., Hendriksen, P. A., Balikji, J., Severeijns, N. R., Sips, A. S. M., Bruce, G., Garssen, J., & Verster, J. C. (2023). COVID-19 Lockdown Effects on Mood: Impact of Sex, Age, and Underlying Disease. Psychiatry International, 4(4), 307-323. https://doi.org/10.3390/psychiatryint4040030