
Molecular Diagnostics of Lung Cancer in Serous Effusion Samples



Abstract
:1. Introduction
2. Materials and Methods
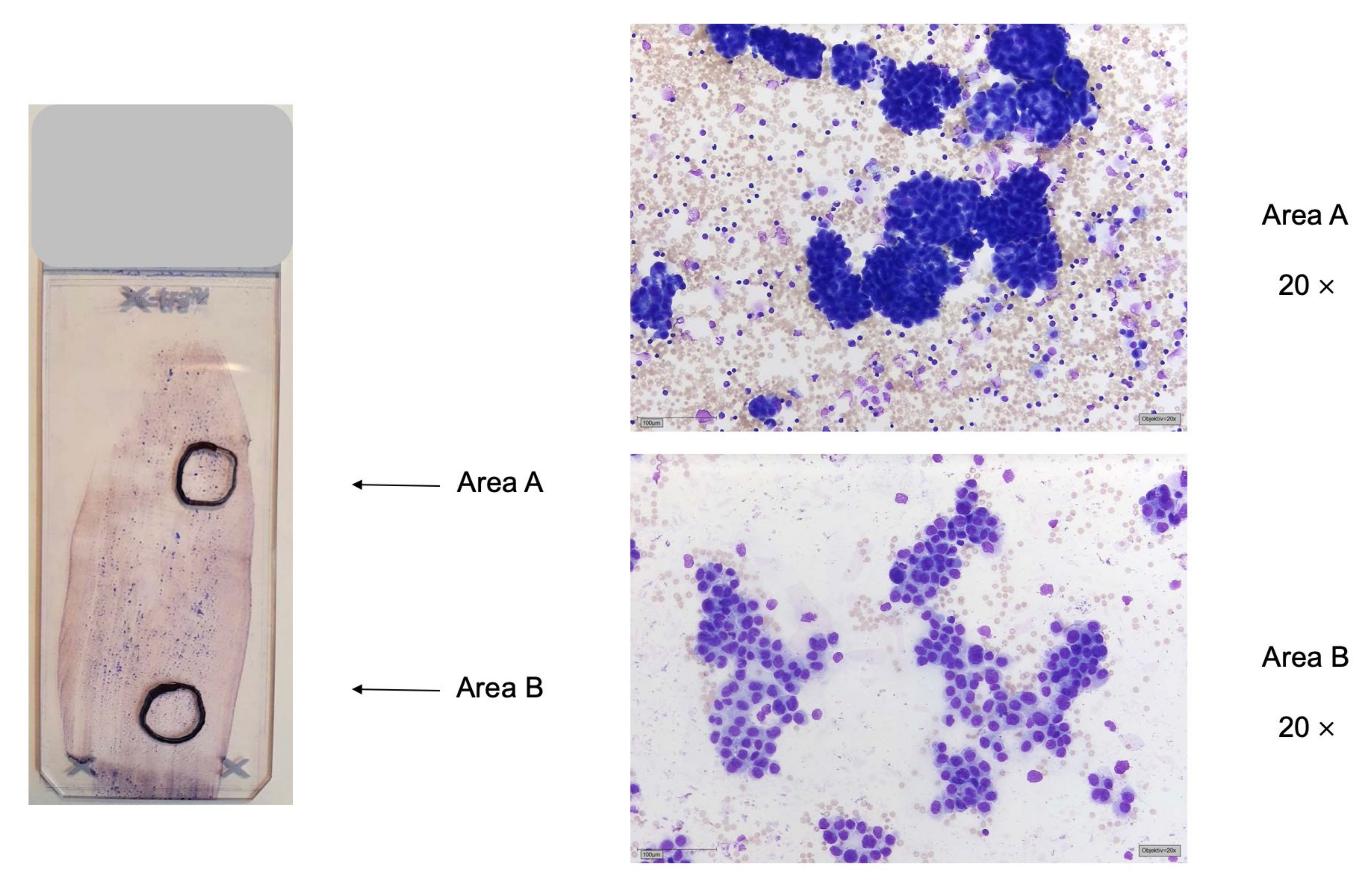
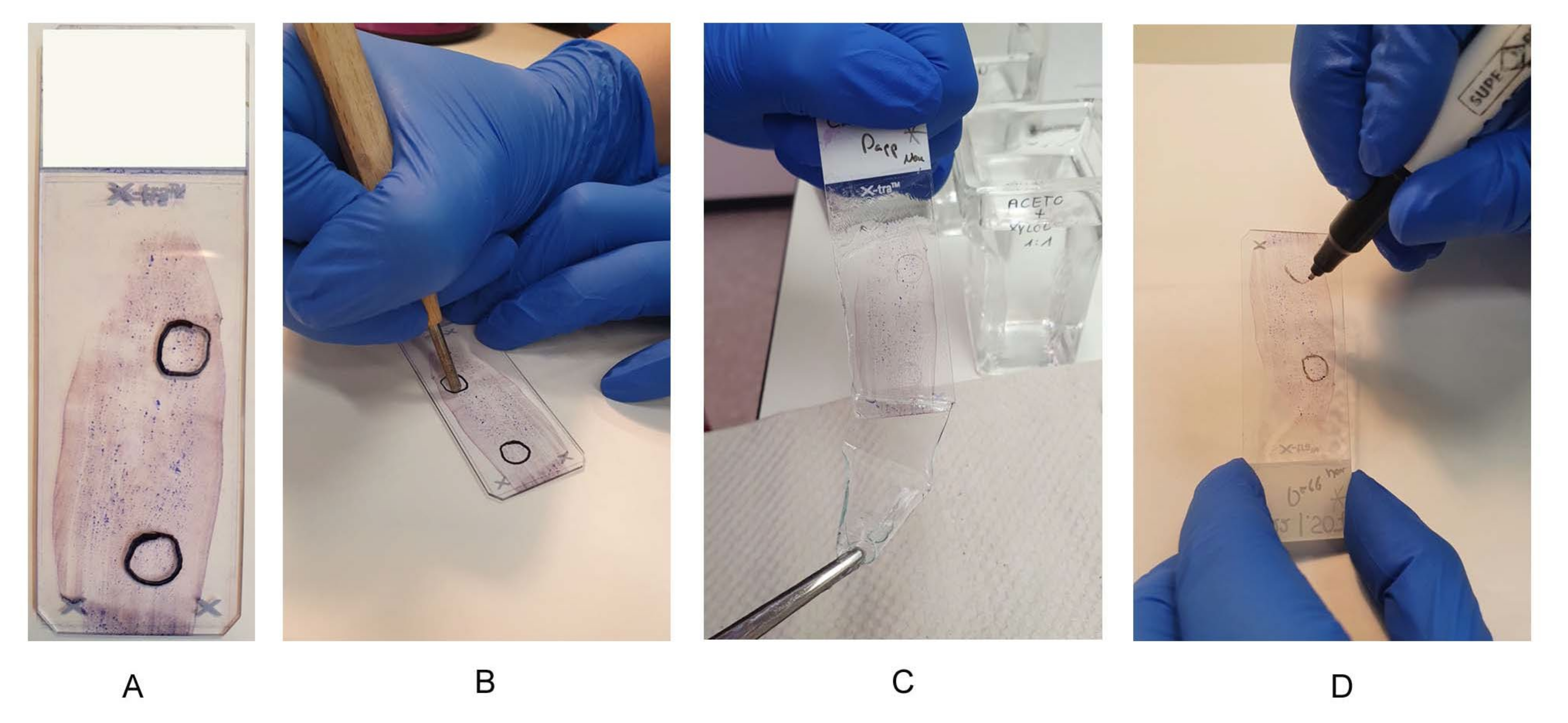
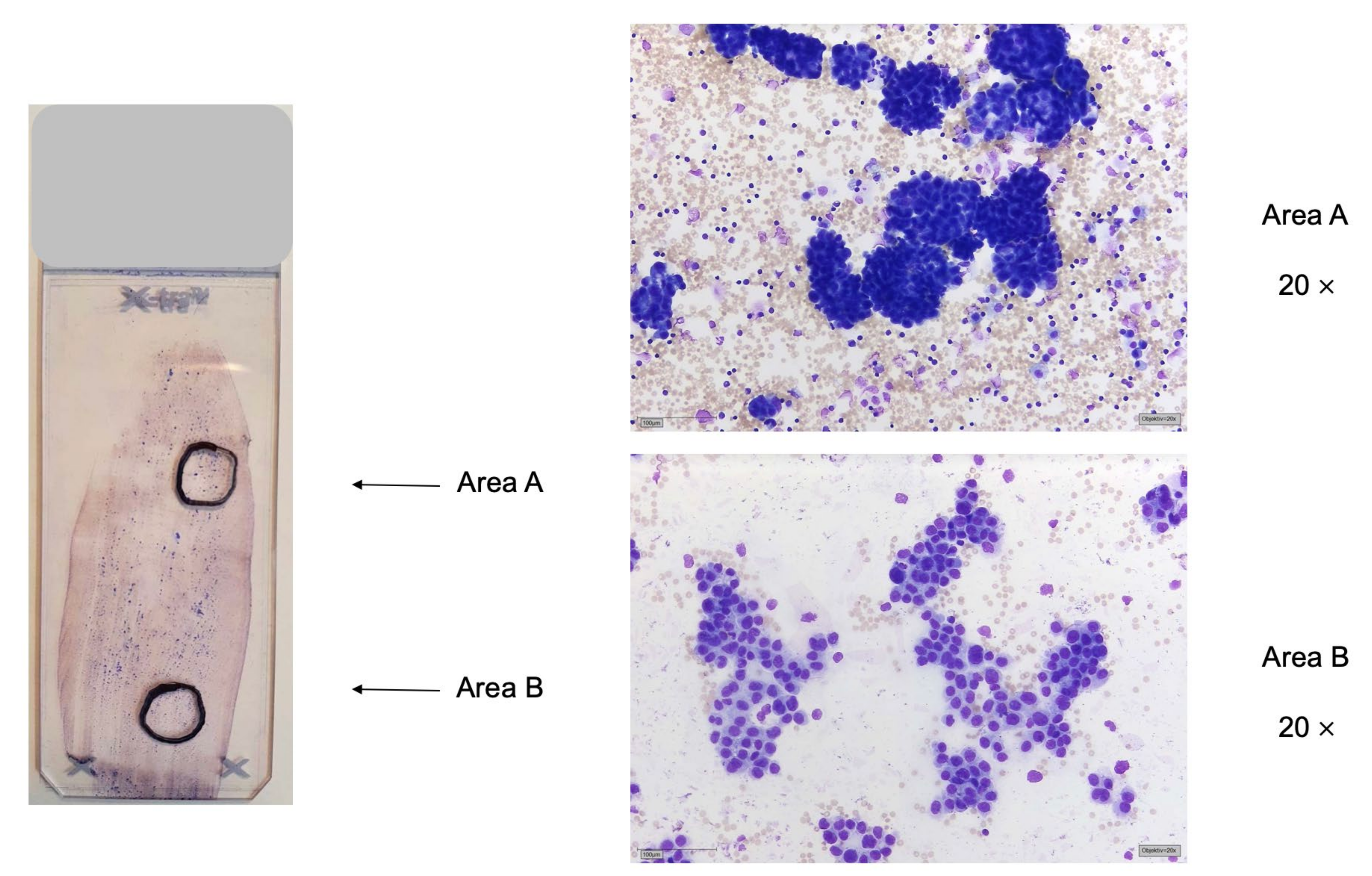
2.1. Preanalytics of Cytological Preparations
2.2. Preparation for FISH Analysis
2.3. DNA Extraction from Cytological Preparations
2.4. Fluorescence In Situ Hybridizations on Cytological Preparations
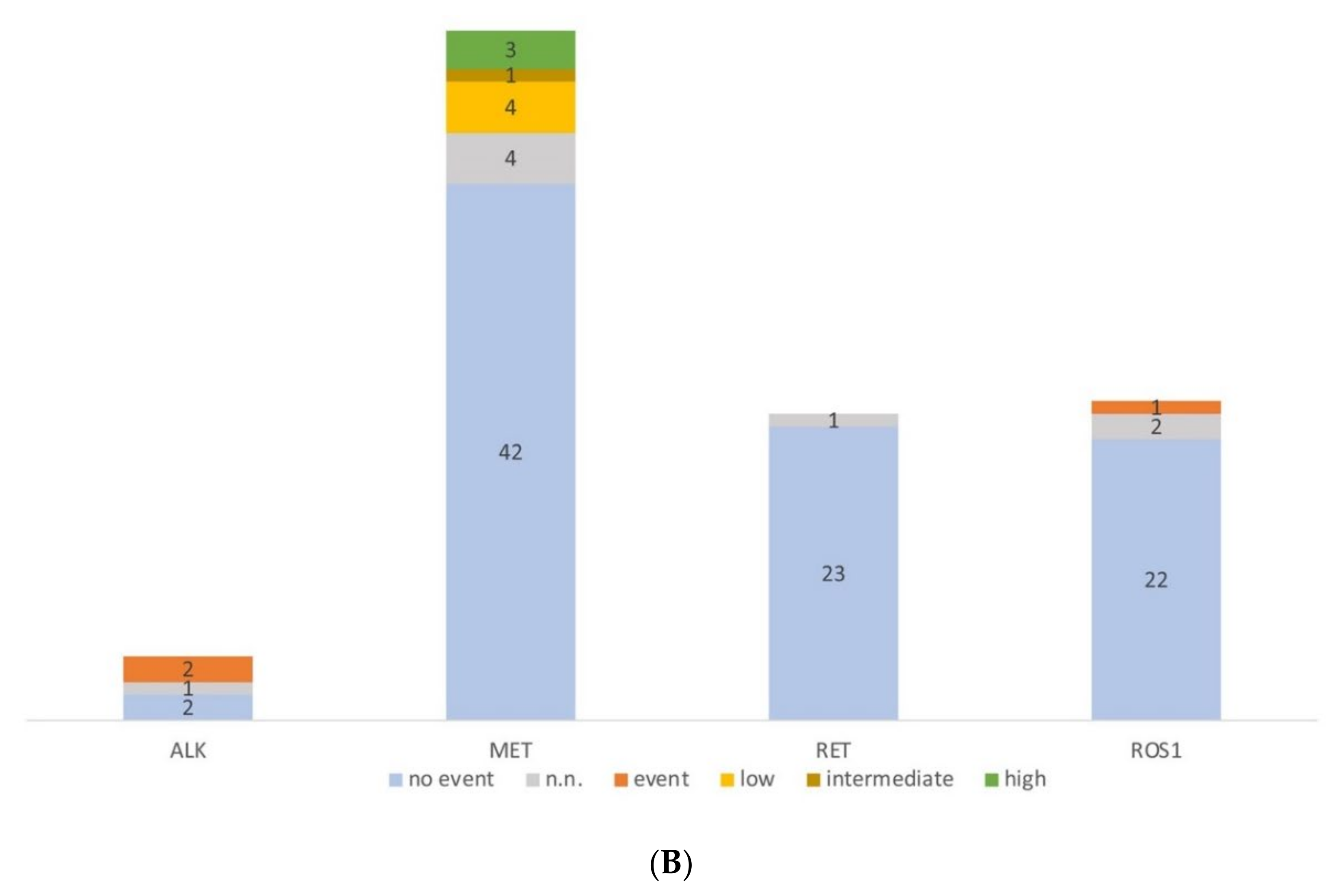
3. Results
Evaluation of Molecular Pathological Examinations of Cytological Specimens
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.; Ma, J.; Zou, Z.; Jemal, A. Cancer statistics, 2014. CA Cancer J. Clin. 2014, 64, 9–29. [Google Scholar] [CrossRef] [Green Version]
- Nicholson, A.G.; Geisinger, K.; Aisner, S.C.; Al-Dayel, F.; Bubendorf, L. Terminology and criteria in non-resection specimens. In WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart, 4th ed.; Travis, W.D., Brambilla, E., Burke, A.P., Marx, A., Nicholson, A.G., Eds.; International Agency for Research on Cancer (IARC): Lyon, France, 2015; pp. 17–21. [Google Scholar]
- Pisapia, P.; Pepe, F.; Iaccarino, A.; Sgariglia, R.; Nacchio, M.; Conticelli, F.; Salatiello, M.; Tufano, R.; Russo, G.; Gragnano, G.; et al. Next Generation Sequencing in Cytopathology: Focus on Non-Small Cell Lung Cancer. Front. Med. 2021, 8, 633923. [Google Scholar] [CrossRef]
- Passaro, A.; Mok, T.; Peters, S.; Popat, S.; Ahn, M.J.; de Marinis, F. Recent Advances on the Role of EGFR Tyrosine Kinase Inhibitors in the Management of NSCLC With Uncommon, Non Exon 20 Insertions, EGFR Mutations. J. Thorac. Oncol. 2021, 16, 764–773. [Google Scholar] [CrossRef]
- Cardarella, S.; Ogino, A.; Nishino, M.; Butaney, M.; Shen, J.; Lydon, C.; Yeap, B.Y.; Sholl, L.M.; Johnson, B.E.; Jänne, P.A. Clinical, pathologic, and biologic features associated with BRAF mutations in non-small cell lung cancer. Clin. Cancer Res. 2013, 19, 4532–4540. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.; Jain, P.; Wang, F.; Ma, P.C.; Borczuk, A.; Halmos, B. MET alterations and their impact on the future of non-small cell lung cancer (NSCLC) targeted therapies. Expert Opin. Ther. Targets 2021, 25, 249–268. [Google Scholar] [CrossRef]
- Liu, J.; Kang, R.; Tang, D. The KRAS-G12C inhibitor: Activity and resistance. Cancer Gene Ther. 2021. [Google Scholar] [CrossRef]
- Soda, M.; Choi, Y.L.; Enomoto, M.; Takada, S.; Yamashita, Y.; Ishikawa, S.; Fujiwara, S.; Watanabe, H.; Kurashina, K.; Hatanaka, H.; et al. Identification of the transforming EML4-ALK fusion gene in non-small-cell lung cancer. Nature 2007, 448, 561–566. [Google Scholar] [CrossRef]
- Mizukami, T.; Shiraishi, K.; Shimada, Y.; Ogiwara, H.; Tsuta, K.; Ichikawa, H.; Sakamoto, H.; Kato, M.; Shibata, T.; Nakano, T.; et al. Molecular mechanisms underlying oncogenic RET fusion in lung adenocarcinoma. J. Thorac. Oncol. 2014, 9, 622–630. [Google Scholar] [CrossRef] [Green Version]
- Pisapia, P.; Lozano, M.D.; Vigliar, E.; Bellevicine, C.; Pepe, F.; Malapelle, U.; Troncone, G. ALK and ROS1 testing on lung cancer cytologic samples: Perspectives. Cancer Cytopathol. 2017, 125, 817–830. [Google Scholar] [CrossRef] [Green Version]
- Heydt, C.; Wölwer, C.B.; Velazquez Camacho, O.; Wagener-Ryczek, S.; Pappesch, R.; Siemanowski, J.; Rehker, J.; Haller, F.; Agaimy, A.; Worm, K.; et al. Detection of gene fusions using targeted next-generation sequencing: A comparative evaluation. BMC Med. Genom. 2021, 14, 62. [Google Scholar] [CrossRef]
- Leichsenring, J.; Volckmar, A.L.; Kirchner, M.; Kazdal, D.; Kriegsmann, M.; Stögbauer, F.; Bockmayr, T.; Klauschen, F.; Herth, F.J.F.; Penzel, R.; et al. Targeted deep sequencing of effusion cytology samples is feasible, informs spatiotemporal tumor evolution, and has clinical and diagnostic utility. Genes Chromosomes Cancer 2018, 57, 70–79. [Google Scholar] [CrossRef]
- Roy-Chowdhuri, S.; Stewart, J. Preanalytic Variables in Cytology: Lessons Learned from Next-Generation Sequencing-The MD Anderson Experience. Arch. Pathol. Lab. Med. 2016, 140, 1191–1199. [Google Scholar] [CrossRef] [Green Version]
- Nambirajan, A.; Rana, D.; Samant, K.; Prabakaran, A.; Malik, P.; Jain, D. Multiplex fluorescence in situ hybridization testing for anaplastic lymphoma kinase and c-ros oncogene 1 gene rearrangements on cytology smears in lung adenocarcinomas: Comparative study with formalin-fixed paraffin-embedded sections. J. Am. Soc. Cytopathol. 2022, in press. [Google Scholar] [CrossRef]
- Huang, M.; Wei, S. Overview of Molecular Testing of Cytology Specimens. Acta Cytol. 2020, 64, 136–146. [Google Scholar] [CrossRef] [PubMed]
- da Cunha Santos, G.; Saieg, M.A.; Troncone, G.; Zeppa, P. Cytological preparations for molecular analysis: A review of technical procedures, advantages and limitations for referring samples for testing. Cytopathology 2018, 29, 125–132. [Google Scholar] [CrossRef]
- Bellevicine, C.; Malapelle, U.; Vigliar, E.; Pisapia, P.; Vita, G.; Troncone, G. How to prepare cytological samples for molecular testing. J. Clin. Pathol. 2017, 70, 819–826. [Google Scholar] [CrossRef]
- Herth, F.J.; Bubendorf, L.; Gütz, S.; Morresi-Hauf, A.; Hummel, M.; Junker, K.; Lehmann, U.; Petersen, I.; Schnabel, P.A.; Warth, A. Diagnose und prädiktive Analysen an zytologischen und bioptischen Tumorproben nicht-kleinzelliger Lungenkarzinome: Aktuelle Strategien und Herausforderungen [Diagnostic and predictive analyses of cytological specimens of non-small cell lung cancer: Strategies and challenges]. Pneumologie 2013, 67, 198–204. [Google Scholar] [CrossRef] [Green Version]
- Michels, S.; Heydt, C.; van Veggel, B.M.; Deschler-Baier, B.; Pardo, N.; Monkhorst, K.; Rüsseler, V.; Stratmann, J.; Griesinger, J.; Steinhauser, S.; et al. Genomic Profiling Identifies Outcome-Relevant Mechanisms of Innate and Acquired Resistance to Third-Generation Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitor Therapy in Lung Cancer. JCO Precis. Oncol. 2019, 3, 1–14. [Google Scholar] [CrossRef]
- Peifer, M.; Fernández-Cuesta, L.; Sos, M.L.; George, J.; Seidel, D.; Kasper, L.H.; Plenker, D.; Leenders, F.; Sun, R.; Zander, T.; et al. Integrative genome analyses identify key somatic driver mutations of small-cell lung cancer. Nat. Genet. 2012, 44, 1104–1110. [Google Scholar] [CrossRef]
- Heydt, C.; Kostenko, A.; Merkelbach-Bruse, S.; Wolf, J.; Büttner, R. ALK evaluation in the world of multiplex testing: Network Genomic Medicine (NGM): The Cologne model for implementing personalised oncology. Ann. Oncol. 2016, 27 (Suppl. S3), iii25–iii34. [Google Scholar] [CrossRef]
- Michels, S.; Scheel, A.H.; Scheffler, M.; Schultheis, A.M.; Gautschi, O.; Aebersold, F.; Diebold, J.; Pall, G.; Rothschild, S.; Bubendorf, L.; et al. Clinicopathological Characteristics of RET Rearranged Lung Cancer in European Patients. J. Thorac. Oncol. 2016, 11, 122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheffler, M.; Schultheis, A.; Teixido, C.; Michels, S.; Morales-Espinosa, D.; Viteri, S.; Hartmann, W.; Merkelbach-Bruse, S.; Fischer, R.; Schildhaus, H.-S.; et al. ROS1 rearrangements in lung adenocarcinoma: Prognostic impact, therapeutic options and genetic variability. Oncotarget 2015, 6, 10577–10585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolff, A.C.; Hammond, M.E.H.; Hicks, D.G.; Dowsett, M.; McShane, L.M.; Allison, K.H.; Allred, D.C.; Bartlett, J.M.S.; Bilous, M.; Fitzgibbons, P.; et al. Recommendations for Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Update. Arch. Pathol. Lab. Med. 2014, 138, 241–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schildhaus, H.U.; Schultheis, A.M.; Rüschoff, J.; Binot, E.; Merkelbach-Bruse, S.; Fassunke, J.; Schulte, W.; Ko, Y.-D.; Schlesinger, A.; Bos, M.; et al. MET amplification status in therapy-naive adeno- and squamous cell carcinomas of the lung. Clin. Cancer Res. 2015, 21, 907–915. [Google Scholar] [CrossRef] [Green Version]
- Roy-Chowdhuri, S.; Aisner, D.L.; Allen, T.C.; Beasley, M.B.; Borczuk, A.; Cagle, P.T.; Capelozzi, V.; Dacic, S.; da Cunha Santos, G.; Hariri, L.P.; et al. Biomarker testing in lung carcinoma cytology specimens: A perspective from members of the Pulmonary Pathology Society. Arch. Pathol. Lab. Med. 2016, 140, 1267–1272. [Google Scholar] [CrossRef] [Green Version]
- Pisapia, P.; Malapelle, U.; Roma, G.; Saddar, S.; Zheng, Q.; Pepe, F.; Bruzzese, D.; Vigliar, E.; Bellevicine, C.; Luthra, R.; et al. Molecular Cytopathology Meeting Group. Consistency and reproducibility of next-generation sequencing in cytopathology: A second worldwide ring trial study on improved cytological molecular reference specimens. Cancer Cytopathol. 2019, 127, 285–296. [Google Scholar] [CrossRef]
- Hagmeyer, L.; Fassunke, J.; Engels, M.; Treml, M.; Herkenrath, S.; Matthes, S.; Büttner, R.; Randerath, W. Bronchoscopic Brushing from Central Lung Cancer-Next Generation Sequencing Results are Reliable. Lung 2019, 197, 333–337. [Google Scholar] [CrossRef]
- Lou, S.K.; Grenier, S.; Care, M.; McCuaig, J.; Stockley, T.L.; Clarke, B.; Ruff, H.M.; Boerner, S.L. Validation of BRCA testing on cytologic samples of high-grade serous carcinoma. Cancer Cytopathol. 2021, 129, 907–913. [Google Scholar] [CrossRef]
- Wang, W.; Tang, Y.; Li, J.; Jiang, L.; Jiang, Y.; Su, X. Detection of ALK rearrangements in malignant pleural effusion cell blocks from patients with advanced non-small cell lung cancer: A comparison of Ventana immunohistochemistry and fluorescence in situ hybridization. Cancer Cytopathol. 2015, 123, 117–122. [Google Scholar] [CrossRef]
- Savic, S.; Bubendorf, L. Common Fluorescence in Situ Hybridization Applications in Cytology. Arch. Pathol. Lab. Med. 2016, 140, 1323–1330. [Google Scholar] [CrossRef] [Green Version]
- Malapelle, U.; Pepe, F.; Pisapia, P.; Altimari, A.; Bellevicine, C.; Brunnström, H.; Bruno, R.; Büttner, R.; Cirnes, L.; De Andrea, C.E.; et al. Reference standards for gene fusion molecular assays on cytological samples: An international validation study. J. Clin. Pathol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Ramani, N.S.; Chen, H.; Broaddus, R.R.; Lazar, A.J.; Luthra, R.; Medeiros, L.J.; Patel, K.P.; Rashid, A.; Routbort, M.J.; Stewart, J.; et al. Utilization of cytology smears improves success rates of RNA-based next-generation sequencing gene fusion assays for clinically relevant predictive biomarkers. Cancer Cytopathol. 2021, 129, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Griesinger, F.; Eberhardt, W.; Nusch, A.; Reiser, M.; Zahn, M.O.; Maintz, C.; Bernhardt, C.; Losem, C.; Stenzinger, A.; Heukamp, L.C.; et al. CRISP Registry Group. Biomarker testing in non-small cell lung cancer in routine care: Analysis of the first 3,717 patients in the German prospective, observational, nation-wide CRISP Registry (AIO-TRK-0315). Lung Cancer 2021, 152, 174–184, Erratum in Lung Cancer 2021, 157, 167. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2018 | 2019 | Total | |
|---|---|---|---|
| Cell block only | 25 | 26 | 51 |
| Smears/cytospins only | 5 | 4 | 9 |
| Cell block and smears/cytospins | 2 | 0 | 2 |
| Total | 32 | 30 | 62 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fassunke, J.; Büttner, R.; Engels, M. Molecular Diagnostics of Lung Cancer in Serous Effusion Samples. J. Mol. Pathol. 2022, 3, 78-87. https://doi.org/10.3390/jmp3020008
Fassunke J, Büttner R, Engels M. Molecular Diagnostics of Lung Cancer in Serous Effusion Samples. Journal of Molecular Pathology. 2022; 3(2):78-87. https://doi.org/10.3390/jmp3020008
Chicago/Turabian StyleFassunke, Jana, Reinhard Büttner, and Marianne Engels. 2022. "Molecular Diagnostics of Lung Cancer in Serous Effusion Samples" Journal of Molecular Pathology 3, no. 2: 78-87. https://doi.org/10.3390/jmp3020008
APA StyleFassunke, J., Büttner, R., & Engels, M. (2022). Molecular Diagnostics of Lung Cancer in Serous Effusion Samples. Journal of Molecular Pathology, 3(2), 78-87. https://doi.org/10.3390/jmp3020008