Quantitative Data to Evaluate Clinical Pilates Efficacy in Chronic Low Back Pain Using Inertial Measurement Units †

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
- 6-axis accelerometer BMI160 + gyroscope;
- LTR-329ALS ambient light sensor;
- 3-axis magnetometer BMM150;
- 9-axis sensor fusion by BOSCH;
- 8 MB memory;
- Rechargeable lithium-ion battery;
- Vibration motor;
- Low-power Bluetooth, CPU, power button, LED, and GPIO.
2.1. Phase 1—Calibration
2.2. Phase 2—Unit Installation
2.3. Phase 3—Bluetooth Protocol and Data Transmission
2.4. Phase 4—Initial Recording Observation
2.5. Phase 5—Data Collection for Functional Tests
2.6. Clinical Pilates Intervention Program
3. Results
3.1. Supine Bridge Test (SBT)
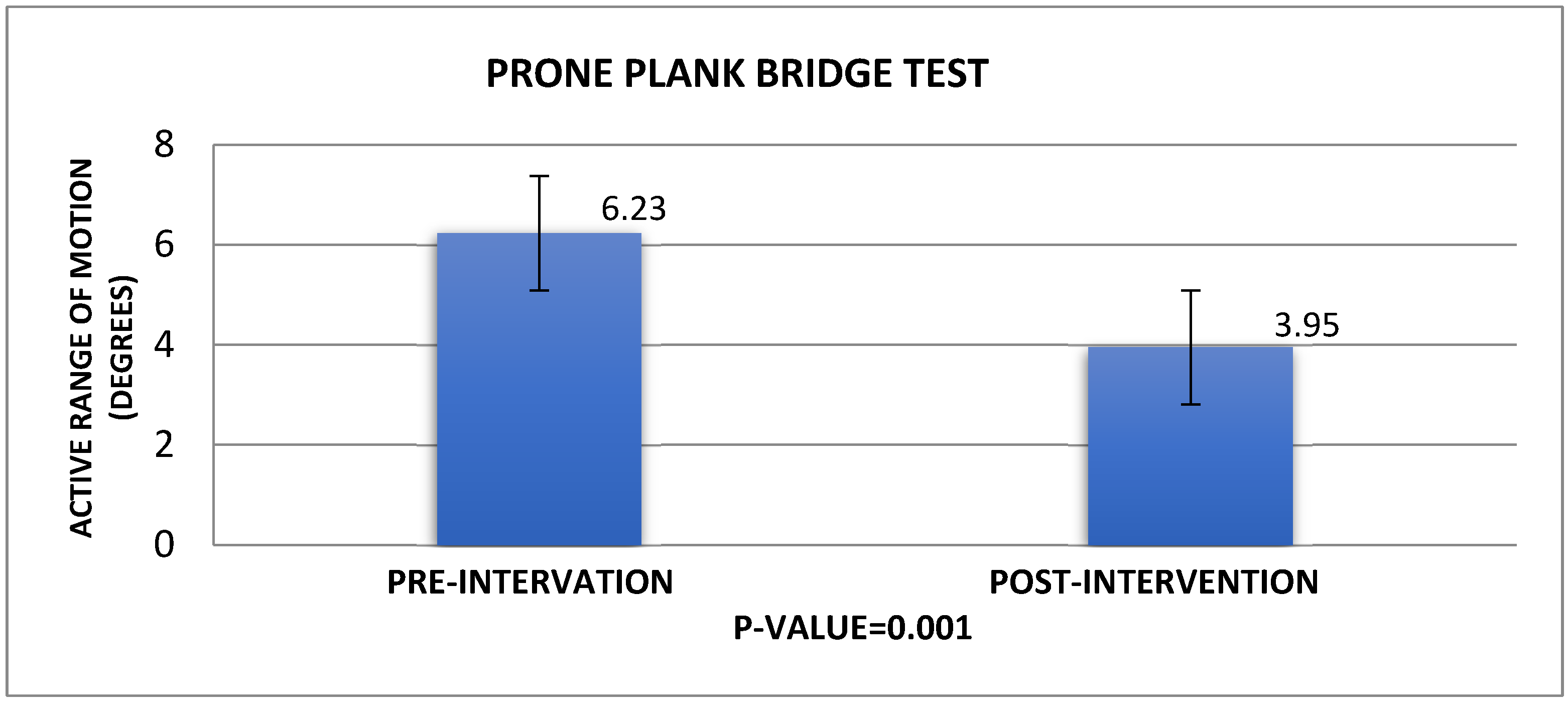
3.2. Prone Bridge Test (PBT)
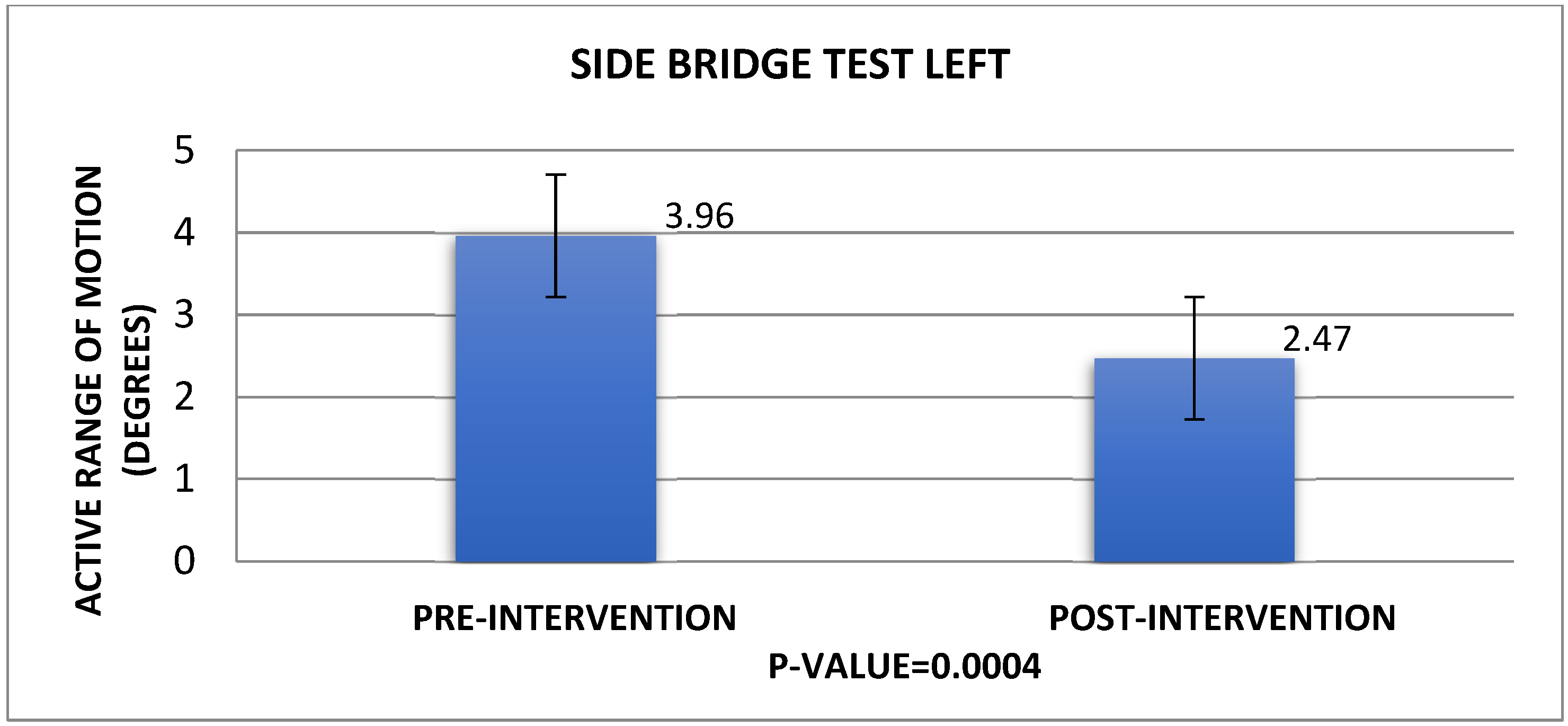
3.3. Side Bridge Test Left (SBTL)
3.4. Side Bridge Test Right (SBTR)
3.5. Wearable Sensors—Functional Test Duration Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hoy, D.; Bain, C.; Williams, G.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Vos, T.; Buchbinder, R. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012, 64, 2028–2037. [Google Scholar] [CrossRef]
- Waddell, G. The Back Pain Revolution, 2nd ed; Elsevier Health Sciences: London, UK, 2004. [Google Scholar]
- Papagiannis, G.I.; Triantafyllou, A.I.; Konstantina, Y.G.; Koulouvaris, P.; Anastasiou, A.; Papadopoulos, E.C.; Papagelopoulos, P.J.; Babis, G.C. Biomechanical Factors could Affect Lumbar Disc Reherniation after Microdiscectomy. J. Orthop. Sports Med. 2019, 1, 46–50. [Google Scholar] [CrossRef]
- Manchikanti, L. Epidemiology of low back pain. Pain Physician 2000, 3, 167–192. [Google Scholar] [CrossRef] [PubMed]
- Triantafyllou, A.; Papagiannis, G.; Stasi, S.; Gkrilias, P.; Kyriakidou, M.; Kampouroglou, E.; Skouras, A.-Z.; Tsolakis, C.; Georgoudis, G.; Savvidou, O.; et al. Lumbar Kinematics Assessment of Patients with Chronic Low Back Pain in Three Bridge Tests Using Miniaturized Sensors. Bioengineering 2023, 10, 339. [Google Scholar] [CrossRef] [PubMed]
- Hani, H.; Souchereau, R.; Kachlan, A.; Harris, H.; Dufour, J.; Aurand, A.; Mageswaran, P.; Hyer, M.; Marras, W. Reliability of a Wearable Motion System for Clinical Evaluation of Dynamic Lumbar Spine Function. Adv. Complement. Altern. Med. 2022, 7, 672–683. [Google Scholar] [CrossRef] [PubMed]
- Eliks, M.; Zgorzalewicz-Stachowiak, M.; Zeńczak-Praga, K. Application of Pilates-based exercises in the treatment of chronic non-specific low back pain: State of the art. Postgrad. Med. J. 2019, 95, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Kwok, B.C.; Lim, J.X.L.; Kong, P.W. The Theoretical Framework of the Clinical Pilates Exercise Method in Managing Non-Specific Chronic Low Back Pain: A Narrative Review. Biology 2021, 10, 1096. [Google Scholar] [CrossRef]
- Valenza, M.C.; Rodríguez-Torres, J.; Cabrera-Martos, I.; Díaz-Pelegrina, A.; Aguilar-Ferrándiz, M.E.; Castellote-Caballero, Y. Results of a Pilates exercise program in patients with chronic non-specific low back pain: A randomized controlled trial. Clin. Rehabil. 2017, 31, 753–760. [Google Scholar] [CrossRef]
- Silva, M.L.D.; Miyamoto, G.C.; Franco, K.F.M.; Franco, Y.R.D.S.; Cabral, C.M.N. Different weekly frequencies of Pilates did not accelerate pain improvement in patients with chronic low back pain. Braz. J. Phys. Ther. 2020, 24, 287–292. [Google Scholar] [CrossRef]
- Glowinski, S.; Blazejewski, A.; Krzyzynski, T. Inertial Sensors and Wavelets Analysis as a Tool for Pathological Gait Identification. In Innovations in Biomedical Engineering; Advances in Intelligent Systems and Computing; Gzik, M., Tkacz, E., Paszenda, Z., Piętka, E., Eds.; Springer: Cham, Switzerland, 2017; Volume 526. [Google Scholar] [CrossRef]
- Amaral, S.; Pássaro, A.C.; Casarotto, R.A. Effect of the association of continuous shortwave diathermy and Pilates-based exercises on pain, depression, and anxiety in chronic non-specific low back pain: A randomized clinical trial. Braz. J. Med. Biol. Res. 2023, 56, e12338. [Google Scholar] [CrossRef]
- Bhadauria, E.A.; Gurudut, P. Comparative effectiveness of lumbar stabilization, dynamic strengthening, and Pilates on chronic low back pain: Randomized clinical trial. J. Exerc. Rehabil. 2017, 13, 477–485. [Google Scholar] [CrossRef]
- Cruz-Díaz, D.; Romeu, M.; Velasco-González, C.; Martínez-Amat, A.; Hita-Contreras, F. The effectiveness of 12 weeks of Pilates intervention on disability, pain and kinesiophobia in patients with chronic low back pain: A randomized controlled trial. Clin. Rehabil. 2018, 32, 1249–1257. [Google Scholar] [CrossRef] [PubMed]
- Natour, J.; Cazotti Lde, A.; Ribeiro, L.H.; Baptista, A.S.; Jones, A. Pilates improves pain, function and quality of life in patients with chronic low back pain: A randomized controlled trial. Clin. Rehabil. 2015, 29, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Wajswelner, H.; Metcalf, B.; Bennell, K. Clinical pilates versus general exercise for chronic low back pain: Randomized trial. Med. Sci. Sports Exerc. 2012, 44, 1197–1205. [Google Scholar] [CrossRef] [PubMed]
- McGill, S.M.; Childs, A.; Liebenson, C. Endurance times for low back stabilization exercises: Clinical targets for testing and training from a normal database. Arch. Phys. Med. Rehabil. 1999, 80, 941–944. [Google Scholar] [CrossRef]
- Owen, P.J.; Miller, C.T.; Mundell, N.L.; Verswijveren, S.J.J.M.; Tagliaferri, S.D.; Brisby, H.; Bowe, S.J.; Belavy, D.L. Which specific modes of exercise training are most effective for treating low back pain? Network meta-analysis. Br. J. Sports Med. 2020, 54, 1279–1287. [Google Scholar] [CrossRef]
- Hayden, J.A.; Wilson, M.N.; Stewart, S.; Cartwright, J.L.; Smith, A.O.; Riley, R.D.; van Tulder, M.; Bendix, T.; Cecchi, F.; Costa, L.O.P.; et al. Exercise treatment effect modifiers in persistent low back pain: An individual participant data meta-analysis of 3514 participants from 27 randomised controlled trials. Br. J. Sports Med. 2020, 54, 1277–1278. [Google Scholar] [CrossRef]
- Fernández-Rodríguez, R.; Álvarez-Bueno, C.; Cavero-Redondo, I.; Torres-Costoso, A.; Pozuelo-Carrascosa, D.P.; Reina-Gutiérrez, S.; Pascual-Morena, C.; Martínez-Vizcaíno, V. Best Exercise Options for Reducing Pain and Disability in Adults With Chronic Low Back Pain: Pilates, Strength, Core-Based, and Mind-Body. A Network Meta-analysis. J. Orthop. Sports Phys. Ther. 2022, 52, 505–521. [Google Scholar] [CrossRef]
- Shi, J.; Hu, Z.Y.; Wen, Y.R.; Wang, Y.F.; Lin, Y.Y.; Zhao, H.Z.; Lin, Y.T.; Wang, Y.L. Optimal modes of mind-body exercise for treating chronic non-specific low back pain: Systematic review and network meta-analysis. Front. Neurosci. 2022, 16, 1046518. [Google Scholar] [CrossRef]
- Ha, T.H.; Saber-Sheikh, K.; Moore, A.P.; Jones, M.P. Measurement of lumbar spine range of movement and coupled motion using inertial sensors—A protocol validity study. Man. Ther. 2013, 1, 87–91. [Google Scholar] [CrossRef]
- Gombatto, S.P.; Collins, D.R.; Sahrmann, S.A.; Engsberg, J.R.; Van Dillen, L.R. Patterns of lumbar region movement during trunk lateral bending in 2 subgroups of people with low back pain. Phys. Ther. 2007, 87, 441–454. [Google Scholar] [CrossRef] [PubMed]
- Van Dillen, L.R.; Gombatto, S.P.; Collins, D.R.; Engsberg, J.R.; Sahrmann, S.A. Symmetry of timing of hip and lumbopelvic rotation motion in 2 different subgroups of people with low back pain. Arch. Phys. Med. Rehabil. 2007, 88, 351–360. [Google Scholar] [CrossRef]
- WHO Guideline for Non-Surgical Management of Chronic Primary Low Back Pain in Adults in Primary and Community Care Settings. World Health Organization: Geneva, Switzerland, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK599212/ (accessed on 19 April 2024).
- Mazzarino, M.; Kerr, D.; Wajswelner, H.; Morris, M.E. Pilates Method for Women’s Health: Systematic Review of Randomized Controlled Trials. Arch. Phys. Med. Rehabil. 2015, 96, 2231–2242. [Google Scholar] [CrossRef] [PubMed]
- García-Garro, P.A.; Hita-Contreras, F.; Martínez-Amat, A.; Achalandabaso-Ochoa, A.; Jiménez-García, J.D.; Cruz-Díaz, D.; Aibar-Almazán, A. Effectiveness of A Pilates Training Program on Cognitive and Functional Abilities in Postmenopausal Women. Int. J. Environ. Res. Public Health 2020, 17, 3580. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Rodríguez, R.; Alvarez-Bueno, C.; Reina-Gutiérrez, S.; Torres-Costoso, A.; Nuñez de Arenas-Arroyo, S.; Martínez-Vizcaíno, V. Effectiveness of Pilates and Yoga to improve bone density in adult women: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0251391. [Google Scholar] [CrossRef]
- Zhang, T.T.; Liu, Z.; Liu, Y.L.; Zhao, J.J.; Liu, D.W.; Tian, Q.B. Obesity as a Risk Factor for Low Back Pain: A Meta-Analysis. Clin. Spine Surg. 2018, 31, 22–27. [Google Scholar] [CrossRef]
- Xi, X.; Ling, Z.; Wang, C.; Gu, C.; Zhan, X.; Yu, H.; Lu, S.; Tsai, T.Y.; Yu, Y.; Cheng, L. Lumbar segment-dependent soft tissue artifacts of skin markers during in vivo weight-bearing forward-Backward bending. Front. Bioeng. Biotechnol. 2022, 10, 960063. [Google Scholar] [CrossRef]
- Zemp, R.; List, R.; Gülay, T.; Elsig, J.P.; Naxera, J.; Taylor, W.R.; Lorenzetti, S. Soft tissue artefacts of the human back: Comparison of the sagittal curvature of the spine measured using skin markers and an open upright MRI. PLoS ONE 2014, 9, e95426. [Google Scholar] [CrossRef]
- Fotaki, A.; Triantafyllou, A.; Papagiannis, G.; Stasi, S.; Georgios, P.; Olga, S.; Koulouvaris, P. The science of biomechanics can promote dancers’ injury prevention strategies. Phys. Ther. Rev. 2020, 26, 94–101. [Google Scholar] [CrossRef]
- Beatriz, M. Musculoskeletal spine pain in adolescents: Epidemiology of non-specific neck and low back pain and risk factors. J. Orthop. Sci. Off. J. Jpn. Orthop. Assoc. 2020, 25, 776–780. [Google Scholar] [CrossRef]
- Miyamoto, G.C.; Lin, C.C.; Cabral, C.M.N.; van Dongen, J.M.; van Tulder, M.W. Cost-effectiveness of exercise therapy in the treatment of non-specific neck pain and low back pain: A systematic review with meta-analysis. Br. J. Sports Med. 2019, 53, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Papagiannis, G.I.; Roumpelakis, I.M.; Triantafyllou, A.I.; Makris, I.N.; Babis, G.C. Response to Letter to the Editor on “No Differences Identified in Transverse Plane Biomechanics between Medial Pivot and Rotating Platform Total Knee Implant Designs”. J. Arthroplast. 2016, 31, 2373. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Assessment Test | Pre-Intervention (Average Value (s)/±Standard Deviation) | Post-Intervention (Average Value (s)/±Standard Deviation) | p-Value |
| SUBT | 72.3/±29.43 | 162.5/±31.24 | 0.001 |
| PBT | 34.31/±20.51 | 65.3/±25.45 | 0.00003 |
| SBT(L) | 10.2/±8.49 | 27.42/±4.33 | 0.002 |
| SBT(R) | 9.22/±7.34 | 29.19/±4.45 | 0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsirmpini, N.M.; Foti, E.; Triantafyllou, A.; Kyriakidou, M.; Gkrilias, P.; Papagiannis, G. Quantitative Data to Evaluate Clinical Pilates Efficacy in Chronic Low Back Pain Using Inertial Measurement Units. Eng. Proc. 2024, 81, 15. https://doi.org/10.3390/engproc2024081015
Tsirmpini NM, Foti E, Triantafyllou A, Kyriakidou M, Gkrilias P, Papagiannis G. Quantitative Data to Evaluate Clinical Pilates Efficacy in Chronic Low Back Pain Using Inertial Measurement Units. Engineering Proceedings. 2024; 81(1):15. https://doi.org/10.3390/engproc2024081015
Chicago/Turabian StyleTsirmpini, Nefeli Maria, Elpida Foti, Athanasios Triantafyllou, Maria Kyriakidou, Panagiotis Gkrilias, and Georgios Papagiannis. 2024. "Quantitative Data to Evaluate Clinical Pilates Efficacy in Chronic Low Back Pain Using Inertial Measurement Units" Engineering Proceedings 81, no. 1: 15. https://doi.org/10.3390/engproc2024081015
APA StyleTsirmpini, N. M., Foti, E., Triantafyllou, A., Kyriakidou, M., Gkrilias, P., & Papagiannis, G. (2024). Quantitative Data to Evaluate Clinical Pilates Efficacy in Chronic Low Back Pain Using Inertial Measurement Units. Engineering Proceedings, 81(1), 15. https://doi.org/10.3390/engproc2024081015