1. Introduction
We describe, herein, a case report for the usage of continuous glucose monitoring technology for two years in a 38-year-old, brittle, female type 1 diabetic diagnosed approximately 19 years prior.
The benefit(s) of exercise in type 1 diabetes have been extensively reported, and include positive changes in body composition, reduced risk of developing associated co-morbidities, and, most importantly for a type 1 diabetic, improved blood glucose control. A review by Samodien et al. (2021) described, amongst other things, the beneficial effect of exercise on mental wellbeing [
1], which is an extremely important but often neglected aspect of diabetes care. Despite the numerous positive outcomes associated with exercise for people with type 1 diabetes [
2], the risk of a severe hypoglycemic event is at the forefront of any patient’s apprehensions; particularly when the form of exercise entails being limited in terms of access to fast acting carbohydrates. Furthermore, avoiding overt hyperglycemia during exercise is important as this can rapidly lead to diabetic ketoacidosis or long-term secondary damage, particularly neuropathy [
3].
The development of real-time continuous glucose monitoring (CGM) devices has been a technological feat that is set to change the way diabetes, both type 1 and type 2, is managed. Galindo et al. (2020) and Jafri et al. (2020) succinctly reviewed several devices with both their advantages and drawbacks [
4,
5]; overall, the greatest limitation to these devices is the cost involved, particularly in a developing country such as South Africa. The Dexcom G6 was used to improve patient care due to accessibility and affordability at the time. Dexcom employs a subcutaneous implantable electrochemical glucose sensor with a separate clip-in Bluetooth transmitter to relay interstitial glucose concentration data to a receiver (which can be an Android or iOS mobile device) [
6]. Interstitial glucose data is then translated into a comparative blood glucose value that is displayed on the receiver. This technology offers the end user more insight into glucose trends and allows real-time tracking and intervention to maintain acceptable glycemia.
Background Case Report: The earliest available medical reports from a specialist physician and diabetologist, in 2003, indicated that the patient, at the age of 18, was poorly controlled and minimally compliant. At the time of assessment, the patient presented with no neurological or vascular complications of diabetes, however, she had a glycated hemoglobin (HbA1C) of 13.2%. Total cholesterol was 5.56 mmol/L (with HDL at 1.54 mmol/L) with an albumin/creatine ratio (ACR) of 7.97 mg/mmol. Normal ranges of these parameters in healthy individuals are: HbA1C 4.0–5.6%, total cholesterol < 5.17 mmol/L, HDL > 1.6 mmol/L, and ACR < 1 mg/mmol. The patient had no known maternal or paternal family history of type 2 diabetes. In 2006, the patient relocated from Kwa-Zulu Natal to the Western Cape and, in 2007, reported an HbA1C of 10.5% under the care of a new physician, with diagnosis as a “brittle” type 1 diabetic. The patient’s HbA1C remained between 8.0 and 9.5% between 2007 and 2016, but record keeping was not adequately accurate for publication purposes. Insulin dosages changed from 18U Actrapid three times a day and 3U Protophane at night to 15U Novorapid three times a day and upward adjustments to 20U Levermir at night. Several incidences of asymptomatic hypoglycemic events were reported, three of which resulted in the patient experiencing mild seizures. The patient was prescribed a glucagon hypokit to keep on her person at all times. The patient’s exercise regimen was limited to 1–2 times per week, and only within the confines of a gymnasium prior to introduction of the Dexcom G6 as part of standard patient care. Dietary intake was as per dietician recommendations over the reporting period, with an emphasis on reducing the intake of refined carbohydrates and saturated fats, and increasing protein and nutritious vegetables intake.
2. Clinical Course and Management
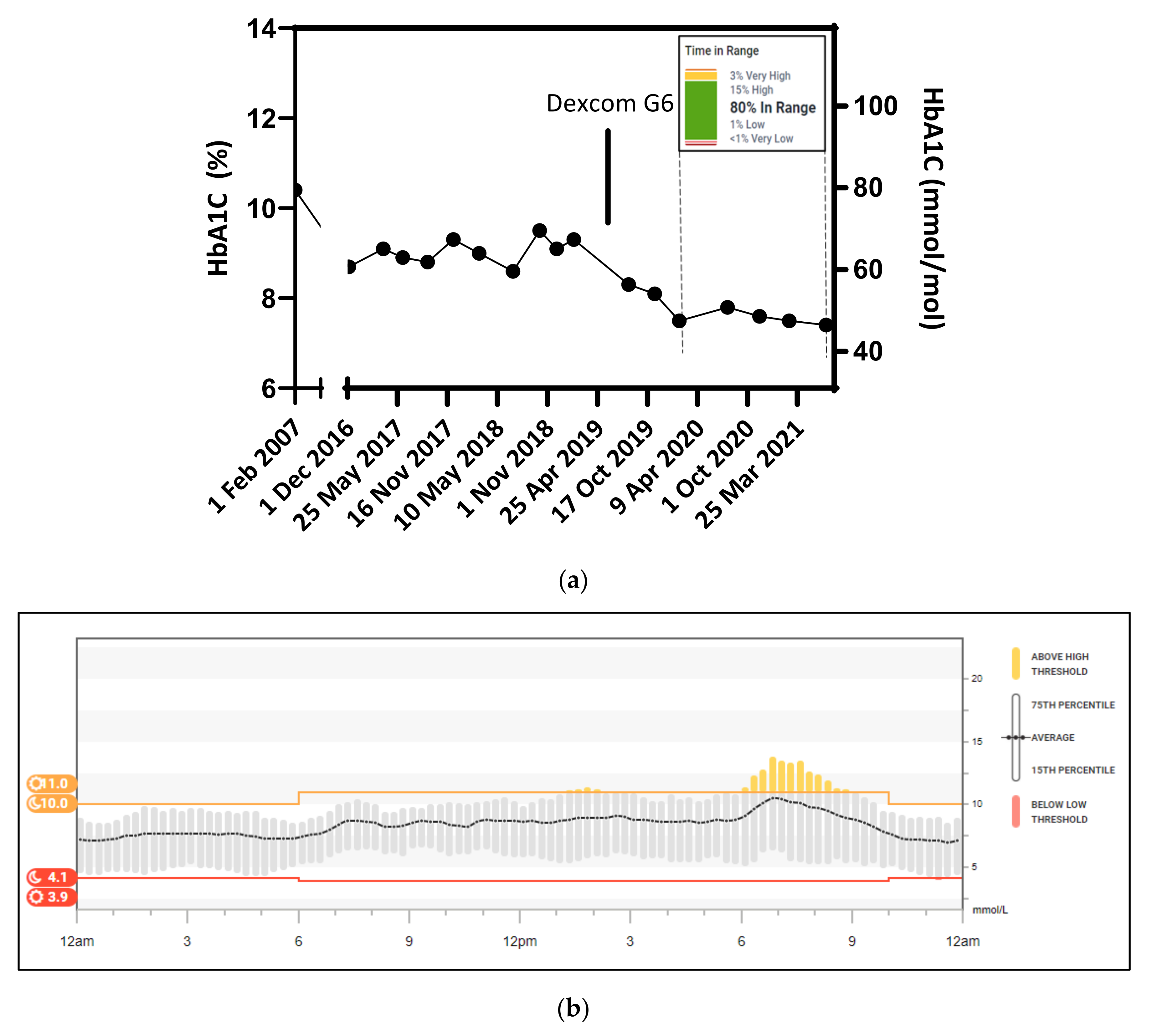
With significant input from Professor Ascott-Evans, some glycemic control was achieved between 2007 and 2019. Under the care of specialist physician Dr. HFM Nortje, the patient was introduced to a sliding scale for rapid acting insulin (Novorapid) administration and an insulin to carbohydrate ratio estimated. This resulted in a reduction in HbA1C to 9.1%, however, this remained largely above 9% for more than 2 years (
Figure 1) despite numerous insulin adjustments, including a transition from insulin determir (Levermir) to Optisulin (insulin glargine) at a split dosage of 15U at night and 15U in the morning.
In 2019, the Dexcom G6 plus became available in South Africa (and limited countries overseas). It differed from the global offering of the standard G6 sensor and transmitter package in that the sensor lasted 14 days and required only one hour for warmup and initialization. Most importantly, the sensor cost ZAR 1, 295 each, making it remotely affordable to the patient, with use of the medical aid savings benefit. Data obtained from the real-time CGM system was shared with the diabetes care Sister at Dr. Nortje’s practice and minute adjustments to insulin dosages and timing were made. The result thereof reduced the patient’s HbA1C almost two-fold from 13.2% in January 2003 to 7.4% in July 2021; with a decrease of nearly 2 noted from before Dexcom usage in February 2019 to 7.4% in July 2021 (
Figure 1a). Currently, the patient’s ACR remains within 0.3 and 1.7 mg/mmol, as compared with 7.97 mg/mmol as initially reported. The patient still presented with no neurological or vascular complications. There have since been no reports of asymptomatic hypoglycemic events and the patient now runs on average four times per week, covering distances from 5–21 km without any adverse glycemic events; having the continuous glucose data feed transmitted to a smart watch aided this achievement substantially. The patient commenced running as an additional form of cardiovascular exercise in 2018 but was limited to less than 5 km per run due to numerous hypoglycemic events—a finger prick blood glucose test while running is grossly impractical. Running intensity was increased soon after use of real-time CGM was initiated. The use of real-time CGM revealed several trends, including a pronounced increase in blood glucose levels at the start of early morning runs (likely a response to an adrenaline surge) and a tendency to drop into hypoglycemic ranges during evening runs (when insulin sensitivity tends to be increased in the patient). Both running distance and the frequency of runs increased by 133% and 112%, respectively, following continuous glucose monitoring, i.e., 57 runs with a total of 475.3 km in 2020 vs. 121 runs and 1108.1 km in 2021 as generated using Strava Inc. (v140.10) GPS tracking data. Corresponding real-time CGM data indicates that the patient remains 80% within range (i.e., between 3.9 and 11.0 mmol/L), with severe hypoglycemic events reduced to less than 1% (
Figure 1a inset). Using trend data accrued over 90 days (
Figure 1b), Optisulin dosages were amended to 10U in the morning and 5U at night; this presented a reduction of 21% in total insulin usage from 57U in January 2003 to approximately 45U currently, with the concurrent nearly two-fold reduction in HbA1C. The patient once more presented no neurological or vascular complications of diabetes. Body weight records (
Table 1) show a 13.9% decrease in body weight from 72 kg in July 2019 to 62 kg in July 2020, moving from an overweight BMI to one within the normal range. This normal body weight range was maintained a year later.
3. Discussion and Conclusions
At the forefront of type 1 diabetic patient care and management is improved glycemic control. Several factors contribute to this, including medical care, diet, physical activity, and mental wellbeing. Continuous glucose monitoring devices, such as the Dexcom G6, affords the user real-time insight into blood glucose levels without the inconvenience of numerous finger pricks for traditional glucometer tests. Real-time readings impart new insights into the glycemic effect(s) of certain foods, activities, or other external stimuli and, thus, the user can respond accordingly.
The case report presented herein demonstrates significantly improved glycemic control following the introduction of the Dexcom G6 as a part of standard patient care. The implications of a 2% reduction in HbA1C are far reaching in terms of reducing the co-morbidities associated with type 1 diabetes, as well as in improving patient overall wellbeing A 1% reduction in HbA1C, as demonstrated in two large-scale studies in the United Kingdom, showed that patients significantly reduced the risk of developing cataracts by 19% and were 16% less likely to suffer heart failure [
7,
8]. Although these large studies focused on patients with type 2 diabetes, similar benefits associated with reduced HbA1C have been reported in other studies [
9,
10]. Overwhelmingly, the largest benefit attributed to the reduction in HbA1C in these studies was that patients with a 1% reduction in HbA1C were 43% less likely to suffer from amputation or death due to peripheral vascular disease and had a 37% reduction in microvascular complications [
7,
8,
9,
10]. Interestingly, a recent study also showed that a 1% reduction in HbA1C was associated with a 1.7% reduction in total healthcare costs [
11]; which has significant implications for healthcare insurance and patient personal expenditure. Another study showed that reduced HbA1C lowered the risk of composite cardiovascular related end points and fewer outpatient visits for diabetes-related incidents [
12].
Such a large reduction in HbA1C as reported herein is often accompanied by a substantial increase in insulin dosage, which also poses the risk of adverse hypoglycemic events [
13]. This was, however, contrary in this study, with a 21% reduction in insulin usage reported. In this regard, the benefits of exercise (running in this instance), as an intervention to burn calories, improve insulin sensitivity, and reduce body weight (the latter by 13.9%) are evident. Maintaining a healthy body weight (BMI 18.5–24.9 kg/m
2) is an imperative part of good glycemic control [
14], thus, the freedom offered by real-time blood glucose readings for a patient to safely run longer distances and intensities to achieve high cardio-metabolic benefits is invaluable.
The introduction of longer, more intense physical activity in the form of running following use of real-time CGM technology would also have considerably contributed to improved diabetes management and overall patient wellbeing in the last two years of the patient’s records [
1,
2,
3]. Regular exercise has been shown to release endorphins that contribute to improved mental health, which is a crucial part of diabetes management, since diabetics are prone to depression and other related mood disorders. Furthermore, regular exercise significantly improves gluco-metabolic profiles by increasing muscle mass and reducing total body fat [
2]. The increased muscle mass may have contributed to a reduction in hypoglycemic events during a run by providing a more substantial source of glucose in the form of glycogen. Reduced body fat would also infer a healthier disposition with the expected concomitant reduction in proinflammatory cytokines. Taken together, the use of real-time CGM technology to progress physical activity in the form of running has multiple benefits in diabetes care and management and provides an additional dimension in patient care.
Accessibility to medical technological advances remains a challenge globally, even more so in developing countries such as South Africa. From the data presented in this report, continuous glucose monitoring afforded the patient improved glycemic control and increased running capacity, both of which contribute to mental wellbeing and potentially improved quality of life. Of course, the reliability and expediency of the data is dependent on the end user taking responsibility for the correct management and use thereof.




{kind=link}