
Effectiveness of Ginseng, Rutin and Moringa for the Treatment of Erectile Dysfunction: A Systematic Review

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
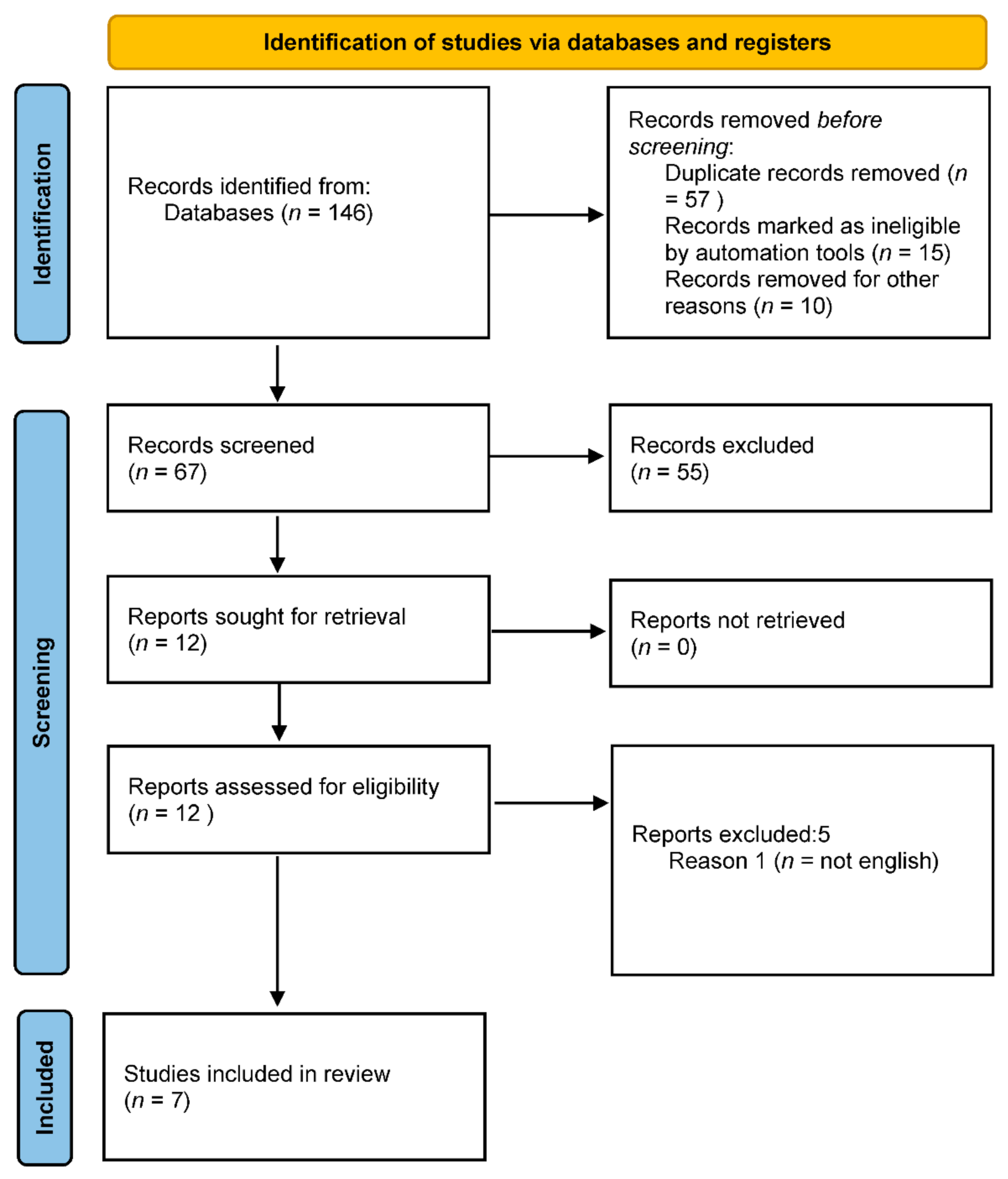
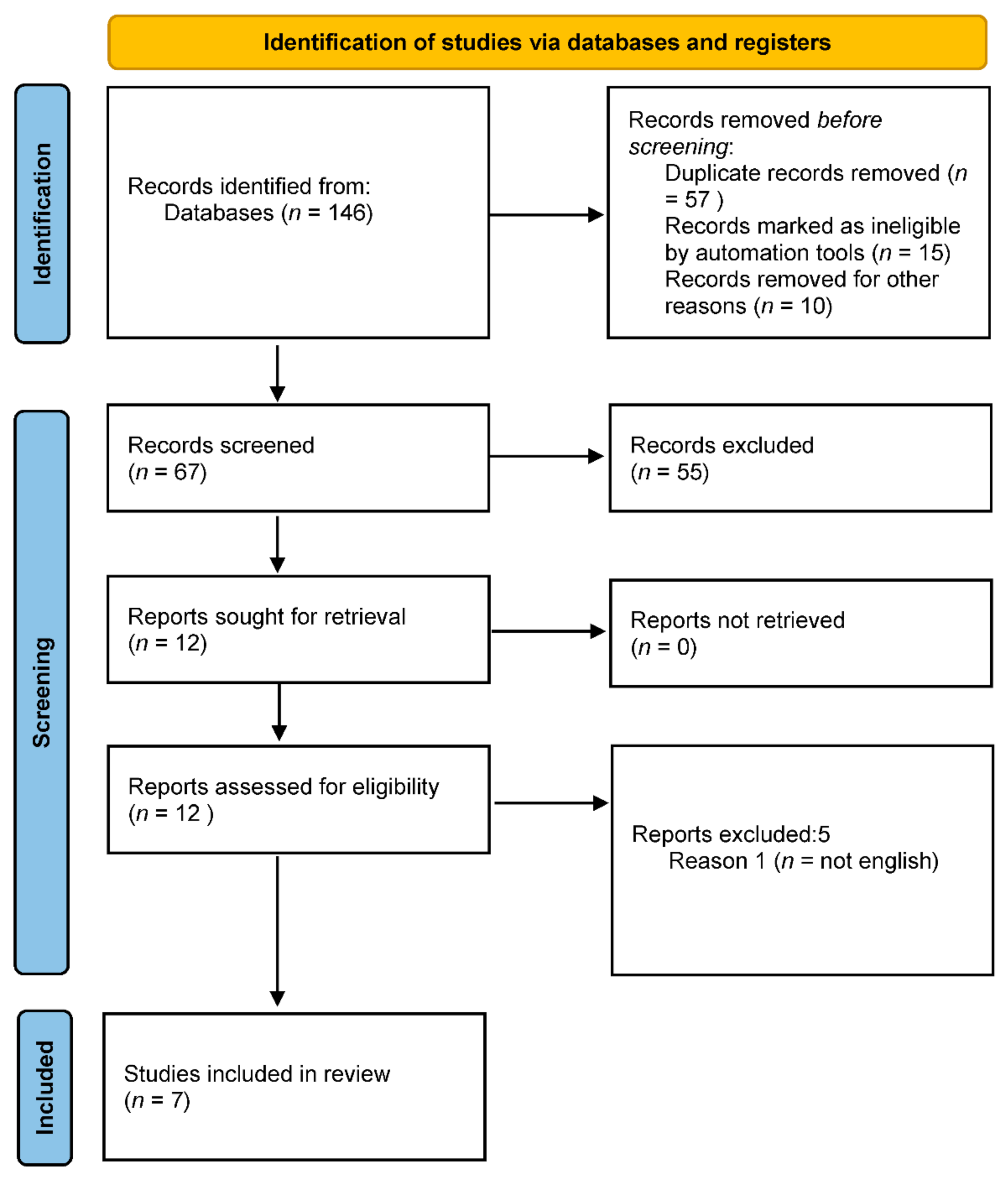
2.1. Search Strategy
2.2. Study Selection
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction
2.5. Assessment of the Risk of Bias
3. Results
3.1. Risk of Bias and Methodological Quality
3.2. Study Characteristics
3.3. Erectile Function Outcomes
4. Discussion
4.1. Limitations
4.2. Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Salonia, A.; Bettocchi, C.; Boeri, L.; Capogrosso, P.; Carvalho, J.; Cilesiz, N.C.; Cocci, A.; Corona, G.; Dimitropoulos, K.; Gül, M.; et al. European Association of Urology Guidelines on Sexual and Reproductive Health-2021 Update: Male Sexual Dysfunction. Eur. Urol. 2021, 80, 333–357. [Google Scholar] [CrossRef] [PubMed]
- Eardley, I. The Incidence, Prevalence, and Natural History of Erectile Dysfunction. Sex. Med. Rev. 2013, 1, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Ma, M.; Yu, B.; Qin, F.; Yuan, J. Current approaches to the diagnosis of vascular erectile dysfunction. Transl. Androl. Urol. 2020, 9, 709. [Google Scholar] [CrossRef] [PubMed]
- Rosen, R.C.; Kupelian, V. Epidemiology of Erectile Dysfunction and Key Risk Factors. In Contemporary Treatment of Erectile Dysfunction; Humana Press: Cham, Switzerland, 2016; pp. 45–56. [Google Scholar] [CrossRef]
- Dong, J.Y.; Zhang, Y.H.; Qin, L.Q. Erectile dysfunction and risk of cardiovascular disease: Meta-analysis of prospective cohort studies. J. Am. Coll. Cardiol. 2011, 58, 1378–1385. [Google Scholar] [CrossRef] [Green Version]
- Gandaglia, G.; Briganti, A.; Jackson, G.; Kloner, R.A.; Montorsi, F.; Montorsi, P.; Vlachopoulos, C. A systematic review of the association between erectile dysfunction and cardiovascular disease. Eur. Urol. 2014, 65, 968–978. [Google Scholar] [CrossRef]
- Raheem, A.A.; Kell, P. Patient preference and satisfaction in erectile dysfunction therapy: A comparison of the three phosphodiesterase-5 inhibitors sildenafil, vardenafil and tadalafil. Patient Prefer. Adherence 2009, 3, 99–104. [Google Scholar] [CrossRef] [Green Version]
- Sin, V.J.E.; Anand, G.S.; Koh, H.L. Botanical Medicine and Natural Products Used for Erectile Dysfunction. Sex. Med. Rev. 2021, 9, 568–592. [Google Scholar] [CrossRef]
- Cui, T.; Kovell, R.C.; Brooks, D.C.; Terlecki, R.P. A Urologist’s Guide to Ingredients Found in Top-Selling Nutraceuticals for Men’s Sexual Health. J. Sex. Med. 2015, 12, 2105–2117. [Google Scholar] [CrossRef]
- Leung, K.W.; Wong, A.S. Ginseng and male reproductive function. Spermatogenesis 2013, 3, e26391. [Google Scholar] [CrossRef] [Green Version]
- Jang, D.J.; Lee, M.S.; Shin, B.C.; Lee, Y.C.; Ernst, E. Red ginseng for treating erectile dysfunction: A systematic review. Br. J. Clin. Pharmacol. 2008, 66, 444–450. [Google Scholar] [CrossRef] [Green Version]
- Patel, D.P.; Pastuszak, A.W.; Hotaling, J.M. Emerging Treatments for Erectile Dysfunction: A Review of Novel, Non-surgical Options. Curr. Urol. Rep. 2019, 20, 44. [Google Scholar] [CrossRef]
- De Andrade, E.; De Mesquita, A.A.; de Almeida Claro, J.; De Andrade, P.M.; Ortiz, V.; Paranhos, M.; Srougi, M.; Erdogrun, T. Study of the efficacy of Korean Red Ginseng in the treatment of erectile dysfunction. Asian J. Androl. 2007, 9, 241–244. [Google Scholar] [CrossRef] [Green Version]
- Atawodi, S.E.; Atawodi, J.C.; Idakwo, G.A.; Pfundstein, B.; Haubner, R.; Wurtele, G.; Bartsch, H.; Owen, R.W. Evaluation of the polyphenol content and antioxidant properties of methanol extracts of the leaves, stem, and root barks of Moringa oleifera Lam. J. Med. Food 2010, 13, 710–716. [Google Scholar] [CrossRef]
- Mirone, V.; Napolitano, L.; di Villa Bianca, R.D.E.; Mitidieri, E.; Sorrentino, R.; Vanelli, A.; Vanacore, D.; Turnaturi, C.; La Rocca, R.; Celentano, G.; et al. A new original nutraceutical formulation ameliorates the effect of Tadalafil on clinical score and cGMP accumulation. Arch. Ital. Urol. Androl. 2021, 93, 221–226. [Google Scholar] [CrossRef]
- Stewart, L.A.; Clarke, M.; Rovers, M.; Riley, R.D.; Simmonds, M.; Stewart, G.; Tierney, J.F. Preferred reporting items for a systematic review and meta-analysis of individual participant data: The PRISMA-IPD statement. JAMA J. Am. Med. Assoc. 2015, 313, 1657–1665. [Google Scholar] [CrossRef]
- RoB 2: A Revised Cochrane Risk-Of-Bias Tool for Randomized Trials. Cochrane Bias. Available online: https://methods.cochrane.org/bias/resources/rob-2-revised-cochrane-risk-bias-tool-randomized-trials (accessed on 10 January 2022).
- Farnia, V.; Alikhani, M.; Ebrahimi, A.; Golshani, S.; Sadeghi Bahmani, D.; Brand, S. Ginseng treatment improves the sexual side effects of methadone maintenance treatment. Psychiatry Res. 2019, 276, 142–150. [Google Scholar] [CrossRef]
- Choi, H.K.; Seong, D.H.; Rha, K.H. Clinical efficacy of Korean red ginseng for erectile dysfunction. Int. J. Impot. Res. 1995, 7, 181–186. [Google Scholar]
- Hong, B.; Ji, Y.H.; Hong, J.H.; Nam, K.I.Y.; Ahn, T.Y. A double-blind crossover study evaluating the efficacy of korean red ginseng in patients with erectile dysfunction: A preliminary report. J. Urol. 2002, 168, 2070–2073. [Google Scholar] [CrossRef]
- Kim, T.H.; Jeon, S.H.; Hahn, E.J.; Paek, K.Y.; Park, J.K.; Youn, N.Y.; Lee, H.L. Effects of tissue-cultured mountain ginseng (Panax ginseng CA Meyer) extract on male patients with erectile dysfunction. Asian J. Androl. 2009, 11, 356–361. [Google Scholar] [CrossRef] [Green Version]
- Carvalheira, A.A.; Pereira, N.M.; Maroco, J.; Forjaz, V. Dropout in the treatment of erectile dysfunction with PDE5: A study on predictors and a qualitative analysis of reasons for discontinuation. J. Sex. Med. 2012, 9, 2361–2369. [Google Scholar] [CrossRef] [Green Version]
- Kiefer, D.; Pantuso, T. Panax ginseng. Am. Fam. Physician 2003, 68, 1539–1542. [Google Scholar] [CrossRef]
- Choi, Y.D.; Park, C.W.; Jang, J.; Kim, S.H.; Jeon, H.Y.; Kim, W.G.; Lee, S.J.; Chung, W.S. Effects of Korean ginseng berry extract on sexual function in men with erectile dysfunction: A multicenter, placebo-controlled, double-blind clinical study. Int. J. Impot. Res. 2013, 25, 45–50. [Google Scholar] [CrossRef]
- Jaiswal, D.; Kumar Rai, P.; Kumar, A.; Mehta, S.; Watal, G. Effect of Moringa oleifera Lam. leaves aqueous extract therapy on hyperglycemic rats. J. Ethnopharmacol. 2009, 123, 392–396. [Google Scholar] [CrossRef]
- Al-Roujeaie, A.S.; Abuohashish, H.M.; Ahmed, M.M.; Alkhamees, O.A. Effect of rutin on diabetic-induced erectile dysfunction: Possible involvement of testicular biomarkers in male rats. Andrologia 2017, 49, e12737. [Google Scholar] [CrossRef]
- Oboh, G.; Adebayo, A.A.; Ademosun, A.O.; Boligon, A.A. In vitro inhibition of phosphodiesterase-5 and arginase activities from rat penile tissue by two Nigerian herbs (Hunteria umbellata and Anogeissus leiocarpus). J. Basic Clin. Physiol. Pharmacol. 2017, 28, 393–401. [Google Scholar] [CrossRef]

{kind=link}
| Author | Year | Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Incomplete Outcome Data | Selective Reporting | Other Bias |
|---|---|---|---|---|---|---|---|
| Kim | 2009 | No | No | Yes | No | No | No |
| Choi | 2012 | Yes | Unclear | Yes | No | No | No |
| de Andrade | 2007 | Yes | Unclear | Yes | No | No | No |
| Hong | 2002 | Yes | Unclear | Yes | No | No | No |
| Farnia | 2019 | Yes | Yes | Yes | No | No | No |
| Choi | 1995 | Yes | Unclear | NR | No | No | IIEF not evalueted |
| Mirone | 2021 | Yes | Unclear | Yes | No | No | No |
| a: Main Study Characteristics | |||||||||||||
| Author | Year | Number of Centers | Type of Center | Country | Study Design | Time Point for Outcome | Tool Use to Assess Erectile Function | N of Patients (Total Cohort) | Mean/Median Age of Patients (Range) | ||||
| Kim | 2009 | Single | University Hospital | Korea | Prospective | 8 weeks | IIEF-5 | 143 | 58.1 (33–79) | ||||
| Choi | 2012 | Multicenter | University Hospital | Korea | Prospective | 4/8 weeks | IIEF-5 | 118 | 57.5 (7.9) | ||||
| de Andrade | 2007 | Single | University Hospital | Brazil | Prospective | 12 weeks | IIEF-5 | 60 | 52.6 (26–70) | ||||
| Hong | 2002 | Single | University Hospital | Korea | Prospective | 8 weeks | IIEF-duplex sonography-RigiScan | 45 | 54 | ||||
| Farnia | 2019 | Single | University Hospital | Iran | Prospective | 4 weeks | IIEF-BSFI | 54 | 38.25 | ||||
| Choi | 1995 | Single | University Hospital | Korea | Prospective | 12 weeks | NR | 90 | 45 (26–70) | ||||
| Mirone | 2021 | Multicenter | University Hospital | Italy | Prospective | 12 weeks | IIEF-5 | 86 | 59.98 (38–69) | ||||
| b: Main Study Outcomes. | |||||||||||||
| Author | Year | Baseline IIEF-EF Mean (Range)-INTERVENTION | Baseline IIEF-EF Mean (Range)-COMPARATOR | IIEF-EF Mean (Range)-INTERVENTION | IIEF-EF Mean (Range)-COMPARATOR | p-Value | Baseline IIEF-5 Mean (Range)-INTERVENTION | Baseline IIEF-5 Mean (Range)-COMPARATOR | IIEF-5 Mean (Range)-INTERVENTION | IIEF-5 Mean (Range)-COMPARATOR | p-Value | Adverse Events | Limitations |
| Kim | 2009 | 11.0 | 11.9 | 16.4 (±7.1) | 13 (±4.2) | 0.01 | 11.0 (±5.1) | 11.9 (±4.4) | 15.3 (±6.1) | 13.5 (±4.4) | 0.06 | 3 (minor hedaches) | No random sequence generation and no allocation concealment |
| Choi | 2012 | 14.3 | 14.6 | 4 weeks: 17.7 (4.7); 8 weeks: 18.6 (5.9) | 4 weeks: 16.3 (5.3); 8 weeks: 18.0 (5.1) | 4 weeks: 0.06; 8 weeks: 0.5 | 14.3 (±1.8) | 14.6 (±1.8) | NR | NR | NR | 0 | Unclear allocation concealment |
| de Andrade | 2007 | 16.4 (±2.9 ) | 17.0 (±3.1) | NR | NR | NR | 16.4 (±2.9) | 17.0 (±3.1) | 21.0 (±3.3) | 17.7 (±5.6) | <0.01 | 3 (headache-insomnia) | Unclear allocation concealment |
| Hong | 2002 | 8.93 (±6.14) | 8.93 ± 6.14 | 38.13 (±16.64) | 30.92 (±15.67) | 0.01 | 8.93 (±6.14) | 8.93 (±6.14) | 12.70 (± 6.38) | 10.33 (5.46) | <0.01 | 0 | Unclear allocation concealment and crossover studio |
| Farnia | 2019 | NR | NR | 15.14 (±3.99) | 12.04 (±2.46) | NR | NR | NR | NR | NR | NR | 4 (sleeplessness agitation) | No statistical results |
| Choi | 1995 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | No standardized outcome measure |
| Mirone | 2021 | 13.18 (±7) | 14.15 (±6.4) | NR | NR | NR | 13.18 (±3.75) | 14.15 (±5) | 20.48( ±2.24) | 14.15 (±4.4) | <0.01 | 20 (headache flushing) | Unclear allocation concealment |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rebez, G.; Capogrosso, P.; Boeri, L.; Rizzo, M.; Miacola, C.; Cai, T.; Palumbo, F.; Ortensi, I.; Ceruti, C.; Lauretti, S.; et al. Effectiveness of Ginseng, Rutin and Moringa for the Treatment of Erectile Dysfunction: A Systematic Review. Uro 2022, 2, 65-73. https://doi.org/10.3390/uro2020009
Rebez G, Capogrosso P, Boeri L, Rizzo M, Miacola C, Cai T, Palumbo F, Ortensi I, Ceruti C, Lauretti S, et al. Effectiveness of Ginseng, Rutin and Moringa for the Treatment of Erectile Dysfunction: A Systematic Review. Uro. 2022; 2(2):65-73. https://doi.org/10.3390/uro2020009
Chicago/Turabian StyleRebez, Giacomo, Paolo Capogrosso, Luca Boeri, Michele Rizzo, Carlos Miacola, Tommaso Cai, Fabrizio Palumbo, Ilaria Ortensi, Carlo Ceruti, Stefano Lauretti, and et al. 2022. "Effectiveness of Ginseng, Rutin and Moringa for the Treatment of Erectile Dysfunction: A Systematic Review" Uro 2, no. 2: 65-73. https://doi.org/10.3390/uro2020009
APA StyleRebez, G., Capogrosso, P., Boeri, L., Rizzo, M., Miacola, C., Cai, T., Palumbo, F., Ortensi, I., Ceruti, C., Lauretti, S., Bitelli, M., Liguori, G., Di Trapani, D., Palmieri, A., & on behalf of the Italian Society of Andrology. (2022). Effectiveness of Ginseng, Rutin and Moringa for the Treatment of Erectile Dysfunction: A Systematic Review. Uro, 2(2), 65-73. https://doi.org/10.3390/uro2020009