
A Combination of Insufficient Physical Activity and Sedentary Behavior Associated with Dynapenic Abdominal Obesity and Dynapenic Obesity in Older Adults: A Cross-Sectional Analysis

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
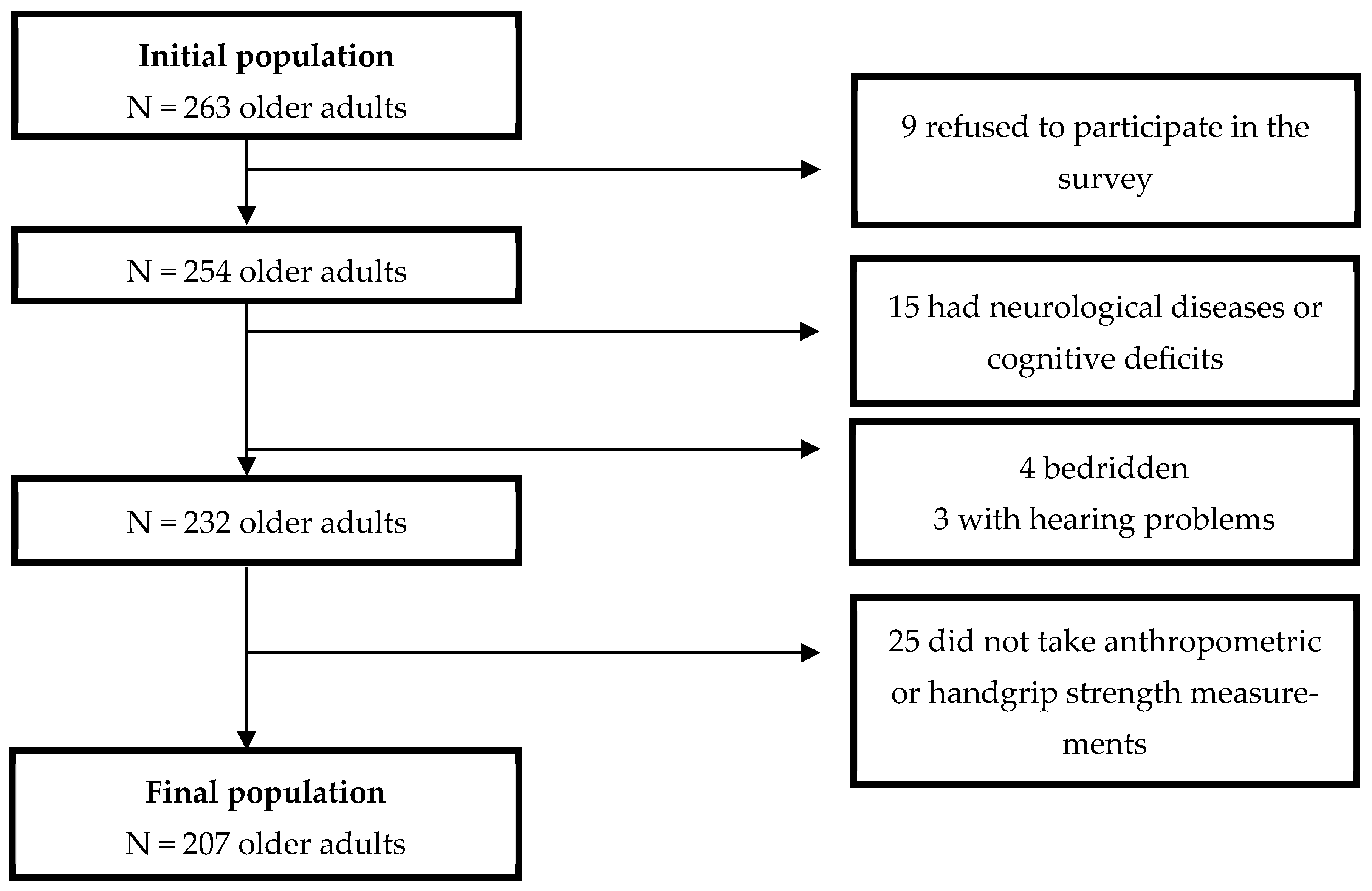
2.1. Study Design, Setting, and Population
2.2. Ethical Considerations
2.3. Eligibility Criteria
2.4. Data Collection
2.5. Independent Variables
2.6. Dependent Variables
2.7. Adjustment Variables (Covariables)
- Socioeconomic: age (continuous, in years), sex (male or female), educational attainment (formal schooling: yes or no), and monthly income (≤1 minimum wage or >1 minimum wage).
- Behavioral: tobacco use (current user: yes or no), alcohol consumption (current consumer: yes or no), fruit, vegetable, or legume intake (≥2 times/day: yes or no), dairy product (e.g., milk, cheese) consumption (daily: yes or no), and protein source (e.g., eggs, beans, lentils, soy) intake (weekly: yes or no).
- Health-related: self-reported physician diagnosis of hypertension (yes or no), self-reported physician diagnosis of diabetes mellitus (yes or no), and occurrence of fall episodes in the 12 months preceding data collection (yes or no).
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Physical Status: The Use of and Interpretation of Anthropometry, Report of a WHO Expert Committee; World Health Organization: Geneva, Switzerland, 1995; Available online: https://apps.who.int/iris/handle/10665/37003 (accessed on 10 December 2024).
- Santos, L.; Pedreira, R.B.S.; Silva, R.R.; Barbosa, R.S.; Valença Neto, P.F.; Casotti, C.A. Anthropometric indicators of adiposity as predictors of systemic arterial hypertension in older people: A cross-sectional analysis. Rev. Nutr. 2023, 36, e220137. [Google Scholar] [CrossRef]
- Tieland, M.; Trouwborst, I.; Clark, B.C. Skeletal muscle performance and ageing. J. Cachexia Sarcopenia Muscle 2018, 9, 3–19. [Google Scholar] [CrossRef] [PubMed]
- Clark, B.C.; Manini, T.M. What is dynapenia? Nutrition 2012, 28, 495–503. [Google Scholar] [CrossRef] [PubMed]
- Silva Alexandre, T.; Scholes, S.; Santos, J.L.F.; Oliveira Duarte, Y.A.; Oliveira, C. The combination of dynapenia and abdominal obesity as a risk factor for worse trajectories of IADL disability among older adults. Clin. Nutr. 2018, 37, 2045–2053. [Google Scholar] [CrossRef] [PubMed]
- Araújo, F.C.D.; Silva, K.S.D.; Ohara, D.G.; Matos, A.P.; Pinto, A.C.P.N.; Pegorari, M.S. Prevalence of and risk factors for dynapenic abdominal obesity in community-dwelling older adults: A cross-sectional study. Ciênc. Saúde Colet. 2022, 27, 761–769. [Google Scholar] [CrossRef] [PubMed]
- Batsis, J.A.; Zbehlik, A.J.; Pidgeon, D.; Bartels, S.J. Dynapenic obesity and the effect on long-term physical function and quality of life: Data from the osteoarthritis initiative. BMC Geriatr. 2015, 15, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Jiang, J.; Hao, Q.; Luo, L.; Dong, B. Dynapenic obesity and lower extremity function in elderly adults. J. Am. Med. Dir. Assoc. 2015, 16, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Sénéchal, M.; Dionne, I.J.; Brochu, M. Dynapenic abdominal obesity and metabolic risk factors in adults 50 years of age and older. J. Aging Health 2012, 24, 812–826. [Google Scholar] [CrossRef] [PubMed]
- Silva Alexandre, T.; Scholes, S.; Santos, J.F.; Oliveira Duarte, Y.A.; Oliveira, C. Dynapenic abdominal obesity increases mortality risk among English and Brazilian older adults: A 10-year follow-up of the ELSA and SABE studies. J. Nutr. Health Aging 2018, 22, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Pinto, A.J.; Bergouignan, A.; Dempsey, P.C.; Roschel, H.; Owen, N.; Gualano, B.; Dunstan, D.W. Physiology of sedentary behavior. Physiol. Rev. 2023, 103, 2561–2622. [Google Scholar] [CrossRef] [PubMed]
- Ramsey, K.A.; Rojer, A.G.; D’Andrea, L.; Otten, R.H.; Heymans, M.W.; Trappenburg, M.C.; Maier, A.B. The association of objectively measured physical activity and sedentary behavior with skeletal muscle strength and muscle power in older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2021, 67, 101266. [Google Scholar] [CrossRef] [PubMed]
- Silveira, E.A.; Mendonça, C.R.; Delpino, F.M.; Souza, G.V.E.; Souza Rosa, L.P.; Oliveira, C.; Noll, M. Sedentary behavior, physical inactivity, abdominal obesity and obesity in adults and older adults: A systematic review and meta-analysis. Clin. Nutr. ESPEN 2022, 50, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13 (Suppl. S1), S31–S34. [Google Scholar] [CrossRef] [PubMed]
- Ministério da Saúde. Política Nacional de Atenção Básica: PNAB (Portaria nº 2.436, de 21 de Setembro de 2017); Ministério da Saúde: Brasília, Brazil, 2017. [Google Scholar]
- Silva, D.J.; Santos, L.; Souza, Y.S.; Valença Neto, P.F.; Santana, P.S.; Almeida, C.B.; Casotti, C.A. Physical fitness according to the level of physical activity in older people: A cross-sectional analysis. Fisioter. Mov. 2023, 36, e36134. [Google Scholar] [CrossRef]
- Icaza, M.G.; Albala, C. Minimental State Examinations (MMSE) del Estudio de Demencia en Chile: Análisis Estadístico; Organización Panamericana de la Salud: Washington, DC, USA, 1999; pp. 18–28. [Google Scholar]
- Bertolucci, P.H.; Brucki, S.; Campacci, S.R.; Juliano, Y. O mini-exame do estado mental em uma população geral: Impacto da escolaridade. Arq. Neuro Psiquiatr. 1994, 52, 1–7. [Google Scholar] [CrossRef]
- Santos, E.S.; Santos, L.; Caires, S.S.; Silva, D.J.; Souza, Y.S.; Valença Neto, P.F.; Casotti, C.A. Functional performance indicators associated with hypertension in older people. Fisioter. Mov. 2023, 36, e36113. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Oja, P. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Benedetti, T.R.B.; Antunes, P.D.C.; Rodriguez-Añez, C.R.; Mazo, G.Z.; Petroski, É.L. Reprodutibilidade e validade do Questionário Internacional de Atividade Física (IPAQ) em homens idosos. Rev. Bras. Med. Esporte 2007, 13, 11–16. [Google Scholar] [CrossRef]
- Benedetti, T.R.B.; Mazo, G.Z.; Barros, M.V. Aplicação do questionário internacional de atividades físicas para avaliação do nível de atividades física de mulheres idosas: Validade concorrente e reprodutibilidade teste-reteste. Rev. Bras. Ciênc. Mov. 2004, 12, 25–34. [Google Scholar]
- Santos, L.; Almeida, C.B.; Valença Neto, P.F.; Silva, R.R.; Santos, I.C.; Casotti, C.A. Habitual physical activity and sedentary behavior as predictors of dynapenia in older adults: A cross-sectional study. São Paulo Med. J. 2024, 142, e2023070. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Santos, L.; Silva, R.R.; Santana, P.S.; Valença Neto, P.F.; Almeida, C.B.; Casotti, C.A. Factors associated with dynapenia in older adults in the Northeast of Brazil. J. Phys. Educ. 2022, 33, e3342. [Google Scholar] [CrossRef]
- Santos, L.; Valença Neto, P.F.; Pedreira, R.B.S.; Silva, R.R.; Galvão, L.L.; Almeida, C.B.; Santos, D.A.T.; Casotti, C.A. Association of physical activity combined with sedentary behavior with dynapenia in older adults. J. Phys. Educ. 2023, 34, e3430. [Google Scholar] [CrossRef]
- Frisancho, A.R. New standards of weight and body composition by frame size and height for assessment of nutritional status of adults and the elderly. Am. J. Clin. Nutr. 1984, 40, 808–819. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, I.M.; Sampaio, R.F.; Mancini, M.C.; Silva, F.C.M.; Souza, M.A.P. Test of grip strength using the Jamar dynamometer. Acta Fisiátr. 2007, 14, 104–110. [Google Scholar] [CrossRef]
- Santos, L.; Santana, P.S.; Caires, S.S.; Barbosa, R.S.; Rodrigues, S.C.; Almeida, C.B.; Valença Neto, P.F.; Casotti, C.A. Força e massa muscular em idosos do Nordeste brasileiro. Res. Soc. Dev. 2021, 10, e570101422270. [Google Scholar] [CrossRef]
- Gonçalves, T.J.M.; Horie, L.M.; Gonçalves, S.E.A.B.; Bacchi, M.K.; Bailer, M.C.; Barbosa-Silva, T.G. Diretriz BRASPEN de Terapia Nutricional no Envelhecimento. Braspen J. 2019, 34, 1–68. Available online: https://nutritotal.com.br/pro/wp-content/uploads/sites/3/2019/11/Material-1-diretriz-TN-no-envelhecimento.pdf (accessed on 10 December 2024).
- Mishra, P.; Pandey, C.M.; Singh, U.; Gupta, A.; Sahu, C.; Keshri, A. Descriptive statistics and normality tests for statistical data. Ann. Card. Anaesth. 2019, 22, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Coutinho, L.; Scazufca, M.; Menezes, P.R. Methods for estimating prevalence ratios in cross-sectional studies. Rev. Saúde Pública 2008, 42, 992–998. [Google Scholar] [CrossRef] [PubMed]
- Greenland, S.; Daniel, R.; Pearce, N. Outcome modelling strategies in epidemiology: Traditional methods and basic alternatives. Int. J. Epidemiol. 2016, 45, 565–575. [Google Scholar] [CrossRef] [PubMed]
- Valença Neto, P.F.; Santos, L.; Rodrigues, S.C.; Almeida, C.B.; Casotti, C.A. Prevalência e fatores associados à suspeição de transtornos mentais comuns em idosos: Um estudo populacional. J. Bras. Psiquiatr. 2023, 72, 100–110. [Google Scholar] [CrossRef]
- Smith, L.; López Sánchez, G.F.; Rahmati, M.; Tully, M.A.; Pizzol, D.; Veronese, N.; Koyanagi, A. Association between sedentary behavior and dynapenic abdominal obesity among older adults from low-and middle-income countries. Aging Clin. Exp. Res. 2024, 36, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Raffin, J.; de Souto Barreto, P.; Le Traon, A.P.; Vellas, B.; Aubertin-Leheudre, M.; Rolland, Y. Sedentary behavior and the biological hallmarks of aging. Ageing Res. Rev. 2023, 83, 101807. [Google Scholar] [CrossRef] [PubMed]
- Le Roux, E.; De Jong, N.P.; Blanc, S.; Simon, C.; Bessesen, D.H.; Bergouignan, A. Physiology of physical inactivity, sedentary behaviours and non-exercise activity: Insights from the space bedrest model. J. Physiol. 2022, 600, 1037–1051. [Google Scholar] [CrossRef] [PubMed]
- Meneguci, J.; Santos, D.A.T.; Silva, R.B.; Santos, R.G.; Sasaki, J.E.; Tribess, S.; Júnior, J.S.V. Comportamento sedentário: Conceito, implicações fisiológicas e os procedimentos de avaliação. Motricidade 2015, 11, 160–174. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Zamboni, M. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | % Response | N | % |
|---|---|---|---|
| Sex | 100.00 | ||
| Male | 85 | 41.10 | |
| Female | 122 | 58.90 | |
| Education | 97.60 | ||
| Yes | 78 | 38.60 | |
| No | 124 | 61.40 | |
| Income | 93.70 | ||
| >1 minimum wage | 25 | 12.90 | |
| ≤1 minimum wage | 195 | 87.10 | |
| Tobacco use | 100.00 | ||
| No | 188 | 90.80 | |
| Yes | 19 | 9.20 | |
| Alcohol consumption | 100.00 | ||
| No | 161 | 77.80 | |
| Yes | 46 | 22.20 | |
| C. fruits, vegetables and/or greens | 100.00 | ||
| No | 151 | 72.90 | |
| Yes | 56 | 27.10 | |
| C. eggs, beans, lentils or soya | 100.00 | ||
| No | 196 | 94.70 | |
| Yes | 11 | 5.30 | |
| C. of milk, cheese, and other dairy products | 100.00 | ||
| No | 158 | 76.30 | |
| Yes | 49 | 23.70 | |
| Level of physical activity | 100.00 | ||
| Sufficient | 101 | 48.80 | |
| Insufficient | 106 | 51.20 | |
| High exposure to SB | 100.00 | ||
| No | 158 | 76.30 | |
| Yes | 49 | 23.70 | |
| LPA combined with SB | 100.00 | ||
| ≥150 min/week and <342.85 min/day | 87 | 42.00 | |
| ≥150 min/week and ≥342.85 min/day | 14 | 6.80 | |
| <150 min/week and <342.85 min/day | 71 | 34.30 | |
| <150 min/week and ≥342.85 min/day | 35 | 16.90 | |
| Abdominal obesity | 100.00 | ||
| No | 114 | 55.10 | |
| Yes | 93 | 44.90 | |
| General obesity | 100.00 | ||
| No | 128 | 61,80 | |
| Yes | 79 | 38.20 | |
| Dynapenia | 100.00 | ||
| No | 156 | 75.40 | |
| Yes | 51 | 24.60 | |
| Dynapenic abdominal obesity | 100.00 | ||
| No | 184 | 88.90 | |
| Yes | 23 | 11.10 | |
| Dynapenic obesity | 100.00 | ||
| No | 193 | 93.20 | |
| Yes | 14 | 6.80 | |
| Hypertension | 100.00 | ||
| No | 85 | 41.10 | |
| Yes | 122 | 58.90 | |
| Diabetes mellitus | 100.00 | ||
| No | 171 | 82.60 | |
| Yes | 36 | 17.40 | |
| Occurrence of falls | 98.10 | ||
| No | 173 | 85.20 | |
| Yes | 30 | 14.80 |
| Variable | Dynapenic Abdominal Obesity | |
|---|---|---|
| Prevalence (%) | Adjusted PR + (95% CI) | |
| LPA combined with SB # | ||
| ≥150 min/week and <342.85 min/day | 4.60 | 1 |
| ≥150 min/week and ≥342.85 min/day | 21.40 | 3.11 (0.54–8.30) |
| <150 min/week and <342.85 min/day | 8.40 | 1.60 (0.45–5.63) |
| <150 min/week and ≥342.85 min/day | 28.60 | 5.54 (1.91–16.03) & |
| Variable | Dynapenic Obesity | |
| Prevalence (%) | Adjusted PR * (95% CI) | |
| LPA combined with SB # | ||
| ≥150 min/week and <342.85 min/day | 3.40 | 1 |
| ≥150 min/week and ≥342.85 min/day | - | - |
| <150 min/week and <342.85 min/day | 4.20 | 1.04 (0.20–7.48) |
| <150 min/week and ≥342.85 min/day | 22.90 | 6.54 (1.68–36.66) & |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos, L.d.; Valença Neto, P.d.F.; de Almeida, C.B.; Coqueiro, R.d.S.; Santos, D.d.A.T.; Oliveira Carneiro, J.A.; Santana, P.d.S.; Costa, E.L.; Galvão, L.L.; Casotti, C.A. A Combination of Insufficient Physical Activity and Sedentary Behavior Associated with Dynapenic Abdominal Obesity and Dynapenic Obesity in Older Adults: A Cross-Sectional Analysis. Obesities 2025, 5, 57. https://doi.org/10.3390/obesities5030057
Santos Ld, Valença Neto PdF, de Almeida CB, Coqueiro RdS, Santos DdAT, Oliveira Carneiro JA, Santana PdS, Costa EL, Galvão LL, Casotti CA. A Combination of Insufficient Physical Activity and Sedentary Behavior Associated with Dynapenic Abdominal Obesity and Dynapenic Obesity in Older Adults: A Cross-Sectional Analysis. Obesities. 2025; 5(3):57. https://doi.org/10.3390/obesities5030057
Chicago/Turabian StyleSantos, Lucas dos, Paulo da Fonseca Valença Neto, Claudio Bispo de Almeida, Raildo da Silva Coqueiro, Douglas de Assis Teles Santos, José Ailton Oliveira Carneiro, Pabline dos Santos Santana, Elayny Lopes Costa, Lucas Lima Galvão, and Cezar Augusto Casotti. 2025. "A Combination of Insufficient Physical Activity and Sedentary Behavior Associated with Dynapenic Abdominal Obesity and Dynapenic Obesity in Older Adults: A Cross-Sectional Analysis" Obesities 5, no. 3: 57. https://doi.org/10.3390/obesities5030057
APA StyleSantos, L. d., Valença Neto, P. d. F., de Almeida, C. B., Coqueiro, R. d. S., Santos, D. d. A. T., Oliveira Carneiro, J. A., Santana, P. d. S., Costa, E. L., Galvão, L. L., & Casotti, C. A. (2025). A Combination of Insufficient Physical Activity and Sedentary Behavior Associated with Dynapenic Abdominal Obesity and Dynapenic Obesity in Older Adults: A Cross-Sectional Analysis. Obesities, 5(3), 57. https://doi.org/10.3390/obesities5030057