
Molecular Hydrogen as Medicine: An Assessment of Administration Methods




Abstract
1. Introduction
2. H2—A Novel Medical Molecule?
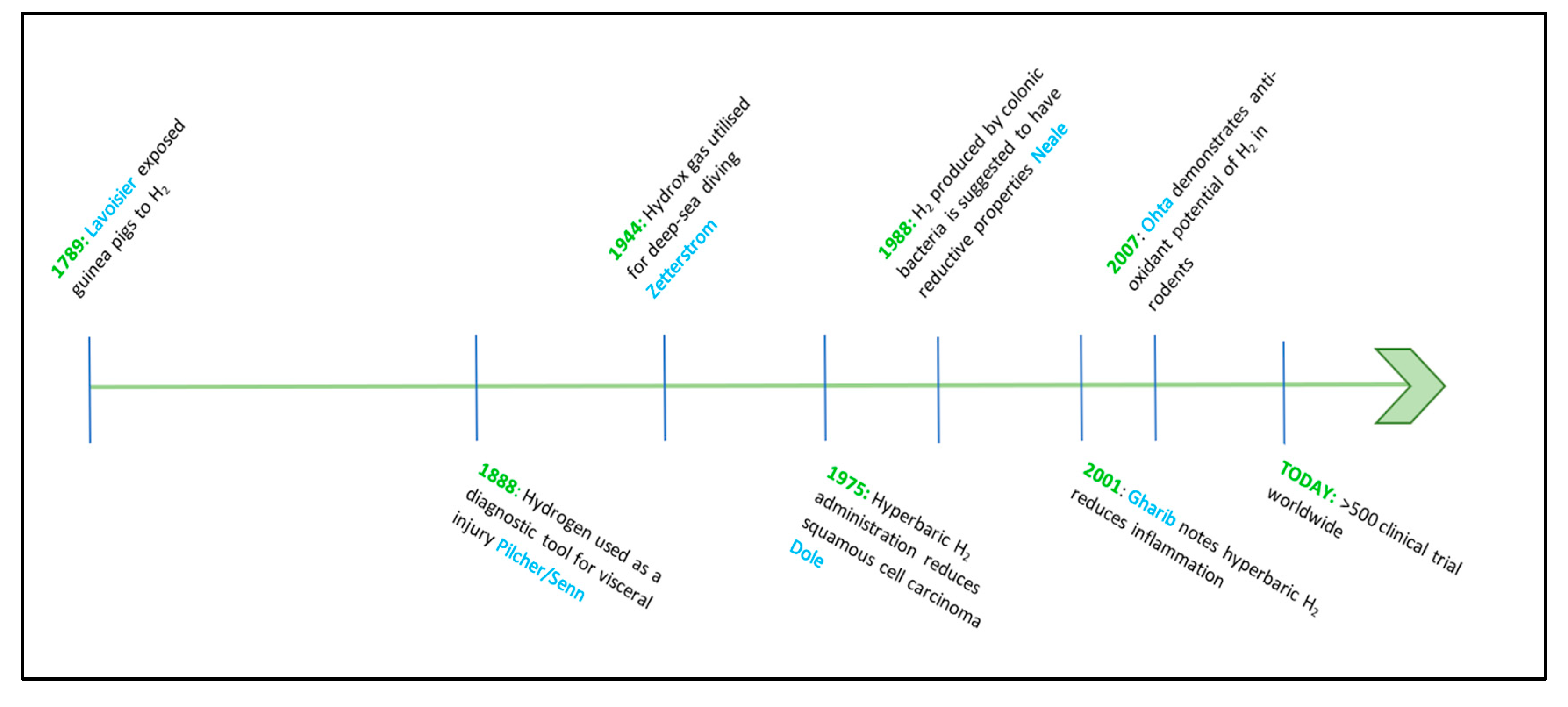
A Brief History of H2 as a Medical Gas
3. The H2 Hypothesis
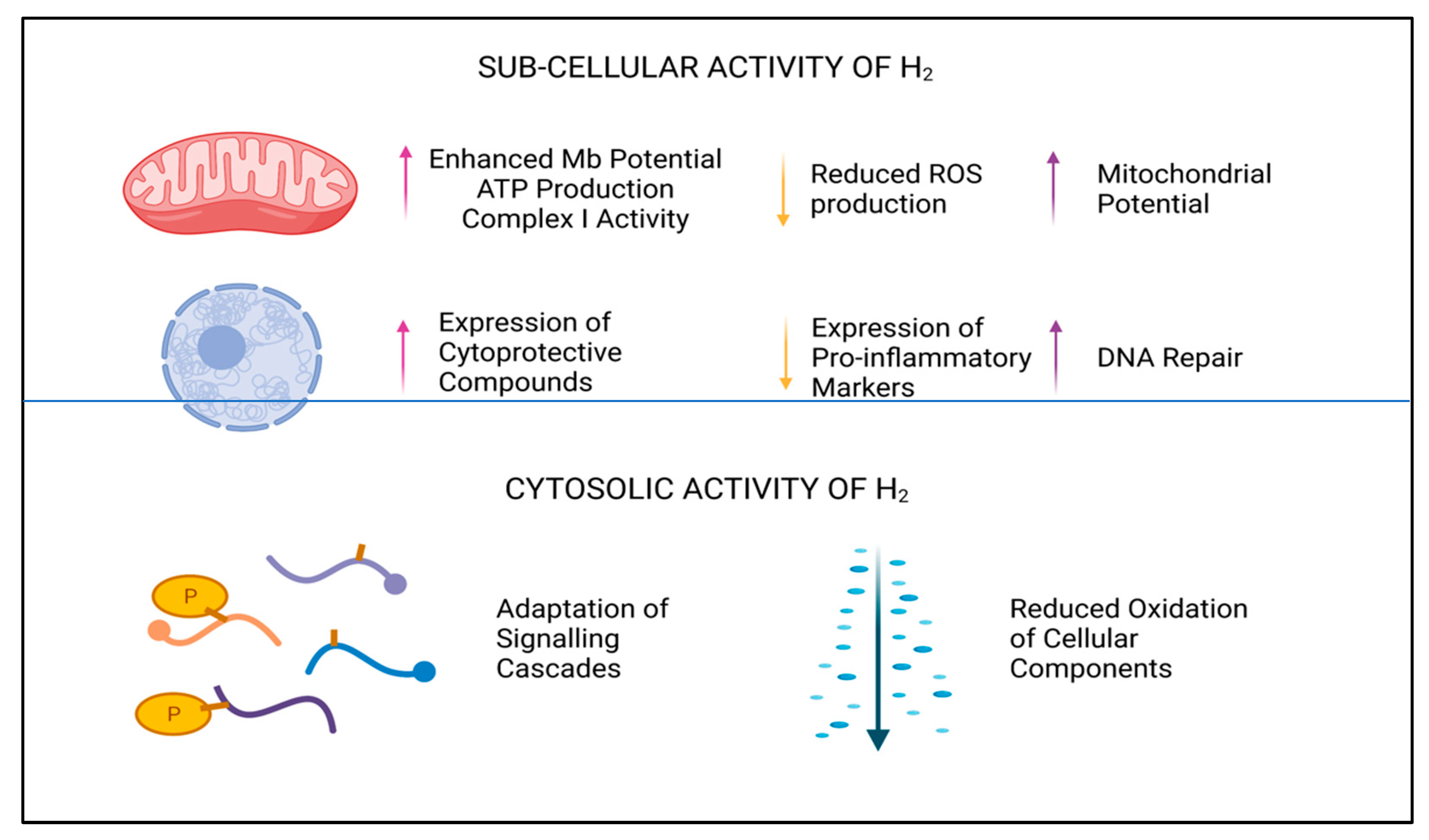
3.1. Mechanisms of Action
3.2. Effects on Human Physiology
4. H2—Methods of Administration
4.1. Ingestion
4.1.1. Dietary Supplements
4.1.2. Hydrogen-Rich Water (HRW)
4.2. Inhalation—H2 and HHO
4.3. Infusion
Hydrogen-Rich Saline
4.4. Nanotechnology
4.4.1. Nanodevices—Mg/Hyaluronic Acid
4.4.2. Nanoparticles—Palladium Hydride (PdH)
4.5. Topical Administration—Bath, Gels, and Patches
5. Future Perspectives
5.1. Mitigating the Risks
5.2. Research Requirements
5.2.1. Clinical
5.2.2. Empirical
5.2.3. Financial
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| Alanine transaminase | ALT |
| Aspartate Transaminase | AST |
| Catalase | CAT |
| Chronic Obstructive Pulmonary Disease | COPD |
| Coronavirus Infectious Disease | COVID-19 |
| Gastroesophageal Reflux Disease | GERD |
| Glutathione Peroxidase | GPx |
| Hydrogen-Rich Saline | HRS |
| Hydrogen-Rich Water | HRW |
| Insulin-like growth factor-1 | IGF-1 |
| Irritable Bowel Disease | IBD |
| Lactate Dehydrogenase | LDH |
| Lipopolysaccharide | LPS |
| Malondialdehyde | (MDA) |
| Nuclear factor erythroid 2-related factor 2 | NRF2 |
| Nuclear factor kappa-light-chain-enhancer of activated B cells | NF-kB |
| Oxy–hydrogen | HHO |
| Palladium-hydride | PdH |
| Polymeric poly (lactic-co-glycolic acid) | PLGA |
| Reactive Oxygen Species | ROS |
| Superoxide Dismutase | (SOD) |
References
- Russell, G.; Zulfiqar, F.; Hancock, J.T. Hydrogenases and the role of molecular hydrogen in plants. Plants 2020, 9, 1136. [Google Scholar] [CrossRef]
- Iida, A.; Nosaka, N.; Yumoto, T.; Knaup, E.; Naito, H.; Nishiyama, C.; Yamakawa, Y.; Tsukahara, K.; Terado, M.; Sato, K.; et al. The clinical application of hydrogen as a medical treatment. Acta Med. Okayama 2016, 70, 331–337. [Google Scholar] [PubMed]
- Ge, L.; Yang, M.; Yang, N.N.; Yin, X.X.; Song, W.G. Molecular hydrogen: A preventive and therapeutic medical gas for various diseases. Oncotarget 2017, 8, 102653. [Google Scholar] [CrossRef] [PubMed]
- Safety of Inhaled Hydrogen Gas Mixtures in Healthy Volunteers. Available online: https://clinicaltrials.gov/ct2/results?cond=&term=molecular+hydrogen&cntry=&state=&city=&dist (accessed on 5 July 2021).
- Russell, G.; Nenov, A.; Hancock, J.T. Oxy-hydrogen Gas: The Rationale behind Its Use as a Novel and Sustainable Treatment for COVID-19 and Other Respiratory Diseases. Eur. Med. J. 2021, 21-00027. [Google Scholar] [CrossRef]
- Ostojic, S.M.; Vukomanovic, B.; Calleja-Gonzalez, J.; Hoffman, J.R. Effectiveness of oral and topical hydrogen for sports-related soft tissue injuries. Postgrad. Med. 2014, 126, 188–196. [Google Scholar] [CrossRef]
- Abraini, J.H.; Ansseau, M.; Bisson, T.; de Mendoza, J.L.J.; Therme, P. Personality patterns of anxiety during occupational deep dives with long-term confinement in hyperbaric chamber. J. Clin. Psychol. 1998, 54, 825–830. [Google Scholar] [CrossRef]
- Dole, M.; Wilson, F.R.; Fife, W.P. Hyperbaric hydrogen therapy: A possible treatment for cancer. Science 1975, 190, 152–154. [Google Scholar] [CrossRef]
- Ostojic, S.M. Hydrogen-rich water as a modulator of gut microbiota? J. Funct. Foods 2021, 78, 104360. [Google Scholar] [CrossRef]
- Xia, C.; Liu, W.; Zeng, D.; Zhu, L.; Sun, X.; Sun, X. Effect of hydrogen-rich water on oxidative stress, liver function, and viral load in patients with chronic Hepatitis B. Clin. Transl. Sci. 2013, 6, 372–375. [Google Scholar] [CrossRef] [PubMed]
- Korovljev, D.; Stajer, V.; Ostojic, J.; LeBaron, T.W.; Ostojic, S.M. Hydrogen-rich water reduces liver fat accumulation and improves liver enzyme profiles in patients with non-alcoholic fatty liver disease: A randomized controlled pilot trial. Clin. Res. Hepatol. Gastroenterol. 2019, 43, 688–693. [Google Scholar] [CrossRef]
- Mizuno, K.; Sasaki, A.T.; Ebisu, K.; Tajima, K.; Kajimoto, O.; Nojima, J.; Kuratsune, H.; Hori, H.; Watanabe, Y. Hydrogen-rich water for improvements of mood, anxiety, and autonomic nerve function in daily life. Med. Gas Res. 2017, 7, 247. [Google Scholar] [PubMed]
- Todorovic, N.; Zanini, D.; Stajer, V.; Korovljev, D.; Ostojic, J.; Ostojic, S.M. Hydrogen-rich water and caffeine for alertness and brain metabolism in sleep-deprived habitual coffee drinkers. Food Sci. Nutr. 2021, 9, 5139–5145. [Google Scholar] [CrossRef] [PubMed]
- Ostojic, S.M. Inadequate production of H2 by gut microbiota and Parkinson disease. Trends Endocrinol. Metab. 2018, 29, 286–288. [Google Scholar] [CrossRef]
- Wang, S.T.; Bao, C.; He, Y.; Tian, X.; Yang, Y.; Zhang, T.; Xu, K.F. Hydrogen gas (XEN) inhalation ameliorates airway inflammation in asthma and COPD patients. QJM Int. J. Med. 2020, 113, 870–875. [Google Scholar] [CrossRef]
- Xu, C.; Wang, S.; Wang, H.; Liu, K.; Zhang, S.; Chen, B.; Liu, H.; Tong, F.; Peng, F.; Tu, Y.; et al. Magnesium-based micromotors as hydrogen generators for precise rheumatoid arthritis therapy. Nano Lett. 2021, 21, 1982–1991. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Han, W.; Nakao, A. Biological Safety of Hydrogen. In Hydrogen Molecular Biology and Medicine; Springer: Dordrecht, The Netherlands, 2015; pp. 35–48. [Google Scholar]
- Senn, N. Rectal insufflation of hydrogen gas an infallible test in the diagnosis of visceral injury of the gastro-intestinal tract in penetrating wounds of the abdomen. J. Am. Med. Assoc. 1888, 10, 767–777. [Google Scholar] [CrossRef][Green Version]
- Pilcher, J.E. Senn on the diagnosis of gastro-intestinal perforation by the rectal insufflation of hydrogen gas. Ann. Surg. 1888, 8, 190. [Google Scholar] [CrossRef] [PubMed]
- Meisenbach, A. A rectal plug for Senn’s method of insufflation of hydrogen gas. J. Am. Med. Assoc. 1888, 11, 908–909. [Google Scholar] [CrossRef][Green Version]
- Hillmantel, J. Two cases of gunshot-wound of the abdomen in which hydrogen-gas test was applied. J. Am. Med. Assoc. 1888, 11, 83–85. [Google Scholar] [CrossRef][Green Version]
- ZetterstrÖm, A. Deep-sea diving with synthetic gas mixtures. Mil. Surg. 1948, 103, 104–106. [Google Scholar] [CrossRef]
- Bjurstedt, H.; Severin, G. The prevention of decompression sickness and nitrogen narcosis by the use of hydrogen as a substitute for nitrogen (The Arne ZetterstrÖm Method for deep-sea diving). Mil. Surg. 1948, 103, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Fife, W.; Texas A & M University; National Sea Grant Program (U.S.); United States, Office of Naval Research. The Use of Non-Explosive Mixtures of Hydrogen and Oxygen for Diving; Texas A& M University: College Station, TX, USA, 1979. [Google Scholar]
- Neale, R.J. Dietary fibre and health: The role of hydrogen production. Med. Hypotheses 1988, 27, 85–87. [Google Scholar] [CrossRef]
- Shirahata, S.; Kabayama, S.; Nakano, M.; Miura, T.; Kusumoto, K.; Gotoh, M.; Hayashi, H.; Otsubo, K.; Morisawa, S.; Katakura, Y. Electrolyzed–reduced water scavenges active oxygen species and protects DNA from oxidative damage. Biochem. Biophys. Res. Commun. 1997, 234, 269–274. [Google Scholar] [CrossRef]
- Gharib, B.; Hanna, S.; Abdallahi, O.M.; Lepidi, H.; Gardette, B.; De Reggi, M. Anti-inflammatory properties of molecular hydrogen: Investigation on parasite-induced liver inflammation. Comptes Rendus l’Académie des Sci.-Ser. III-Sci. Vie 2001, 324, 719–724. [Google Scholar] [CrossRef]
- Ohsawa, I.; Ishikawa, M.; Takahashi, K.; Watanabe, M.; Nishimaki, K.; Yamagata, K.; Katsura, K.I.; Katayama, Y.; Asoh, S.; Ohta, S. Hydrogen acts as a therapeutic anti-oxidant by selectively reducing cytotoxic oxygen radicals. Nat. Med. 2007, 13, 688–694. [Google Scholar] [CrossRef]
- Fukuda, K.I.; Asoh, S.; Ishikawa, M.; Yamamoto, Y.; Ohsawa, I.; Ohta, S. Inhalation of hydrogen gas suppresses hepatic injury caused by ischemia/reperfusion through reducing oxidative stress. Biochem. Biophys. Res. Commun. 2007, 361, 670–674. [Google Scholar] [CrossRef]
- Nogueira, J.E.; Branco, L.G. Recent advances in molecular hydrogen research reducing exercise-induced oxidative stress and inflammation. Curr. Pharm. Des. 2021, 27, 731–736. [Google Scholar] [CrossRef]
- Li, Q.; Xie, F.; Yi, Y.; Zhao, P.; Zhang, X.; Zhang, X.; Zhang, X.; Ma, X. Hydroxyl-radical scavenging activity of hydrogen does not significantly contribute to its biological function. bioRxiv 2021. [Google Scholar] [CrossRef]
- Penders, J.; Kissner, R.; Koppenol, W.H. ONOOH does not react with H2: Potential beneficial effects of H2 as an antioxidant by selective reaction with hydroxyl radicals and peroxynitrite. Free Radic. Biol. Med. 2014, 75, 191–194. [Google Scholar] [CrossRef]
- Hancock, J.T.; Russell, G. Downstream Signalling from Molecular Hydrogen. Plants 2021, 10, 367. [Google Scholar] [CrossRef]
- Ghosh, N.; Das, A.; Chaffee, S.; Roy, S.; Sen, C.K. Immunity and Inflammation in Health and Disease: Emerging Roles of Nutraceuticals and Functional Foods in Immune Support; Academic Press: Cambridge, MA, USA, 2018. [Google Scholar]
- Raghunath, A.; Sundarraj, K.; Nagarajan, R.; Arfuso, F.; Bian, J.; Kumar, A.P.; Sethi, G.; Perumal, E. Antioxidant response elements: Discovery, classes, regulation and potential applications. Redox Biol. 2018, 17, 297–314. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.P. How mitochondria produce reactive oxygen species. Biochem. J. 2009, 417, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Ishihara, G.; Kawamoto, K.; Komori, N.; Ishibashi, T. Molecular hydrogen suppresses superoxide generation in the mitochondrial complex I and reduced mitochondrial membrane potential. Biochem. Biophys. Res. Commun. 2020, 522, 965–970. [Google Scholar] [CrossRef] [PubMed]
- Xie, K.; Wang, Y.; Yin, L.; Wang, Y.; Chen, H.; Mao, X.; Wang, G. Hydrogen gas alleviates sepsis-induced brain injury by improving mitochondrial biogenesis through the activation of PGC-α in mice. Shock 2021, 55, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, J.E.; Amorim, M.R.; Pinto, A.P.; da Rocha, A.L.; da Silva, A.S.; Branco, L.G. Molecular hydrogen downregulates acute exhaustive exercise-induced skeletal muscle damage. Can. J. Physiol. Pharmacol. 2021, 99, 812–820. [Google Scholar] [CrossRef] [PubMed]
- Wilson, H.R.; Veal, D.; Whiteman, M.; Hancock, J.T. Hydrogen gas and its role in cell signalling. CAB Rev. Perspect. Agric. Vet. Sci. Nutr. Nat. Resour. 2017, 12, 1–3. [Google Scholar] [CrossRef]
- Slezak, J.; Kura, B.; LeBaron, T.W.; Singal, P.K.; Buday, J.; Barancik, M. Oxidative stress and pathways of molecular hydrogen effects in medicine. Curr. Pharm. Des. 2021, 27, 610–625. [Google Scholar] [CrossRef]
- Sha, J.B.; Zhang, S.S.; Lu, Y.M.; Gong, W.J.; Jiang, X.P.; Wang, J.J.; Qiao, T.L.; Zhang, H.H.; Zhao, M.Q.; Wang, D.P.; et al. Effects of the long-term consumption of hydrogen-rich water on the anti-oxidant activity and the gut flora in female juvenile soccer players from Suzhou, China. Med Gas Res. 2018, 8, 135. [Google Scholar]
- Ji, X.; Zheng, W.; Yao, W. Protective role of hydrogen gas on oxidative damage and apoptosis in intestinal porcine epithelial cells (IPEC-J2) induced by deoxynivalenol: A preliminary study. Toxins 2020, 12, 5. [Google Scholar] [CrossRef]
- Murakami, Y.; Ito, M.; Ohsawa, I. Molecular hydrogen protects against oxidative stress-induced SH-SY5Y neuroblastoma cell death through the process of mitohormesis. PLoS ONE 2017, 12, 0176992. [Google Scholar] [CrossRef]
- LeBaron, T.W.; Kura, B.; Kalocayova, B.; Tribulova, N.; Slezak, J. A new approach for the prevention and treatment of cardiovascular disorders. Molecular hydrogen significantly reduces the effects of oxidative stress. Molecules 2019, 24, 2076. [Google Scholar] [CrossRef]
- Yu, X.; Gurry, T.; Nguyen, L.T.T.; Richardson, H.S.; Alm, E.J. Prebiotics and community composition influence gas production of the human gut microbiota. MBio 2020, 11, 00217–00220. [Google Scholar] [CrossRef] [PubMed]
- Hylemon, P.B.; Harris, S.C.; Ridlon, J.M. Metabolism of hydrogen gases and bile acids in the gut microbiome. FEBS Lett. 2018, 592, 2070–2082. [Google Scholar] [CrossRef] [PubMed]
- Soleimani, V.; Sahebkar, A.; Hosseinzadeh, H. Turmeric (Curcuma longa) and its major constituent (curcumin) as nontoxic and safe substances. Phytother. Res. 2018, 32, 985–995. [Google Scholar] [CrossRef] [PubMed]
- Zam, W. Gut microbiota as a prospective therapeutic target for curcumin: A review of mutual influence. J. Nutr. Metab. 2018, 2018, 1367984. [Google Scholar] [CrossRef]
- Shimouchi, A.; Nose, K.; Takaoka, M.; Hayashi, H.; Kondo, T. Effect of dietary turmeric on breath hydrogen. Dig. Dis. Sci. 2009, 54, 1725–1729. [Google Scholar] [CrossRef] [PubMed]
- Alharbi, A.A.D.; Ebine, N.; Nakae, S.; Hojo, T.; Fukuoka, Y. Application of molecular hydrogen as an anti-oxidant in responses to ventilatory and ergogenic adjustments during incremental exercise in humans. Nutrients 2021, 13, 459. [Google Scholar] [CrossRef] [PubMed]
- Settineri, R.; Ji, J.; Luo, C.; Ellithorpe, R.R.; de Mattos, G.F.; Rosenblatt, S.; LaValle, J.; Jinenez, A.; Ohta, S.; Nicolson, G.L. Effects of hydrogenized water on intracellular biomarkers for anti-oxidants, glucose uptake, insulin signaling and SIRT 1 and telomerase activity. Am. J. Food Nutr. 2016, 4, 161–168. [Google Scholar] [CrossRef]
- Ostojic, S.M. Molecular hydrogen in sports medicine: New therapeutic perspectives. Int. J. Sports Med. 2015, 36, 273–279. [Google Scholar] [CrossRef]
- Kawamura, T.; Higashida, K.; Muraoka, I. Application of molecular hydrogen as a novel anti-oxidant in sports science. Oxidative Med. Cell. Longev. 2020, 2020, 2328768. [Google Scholar] [CrossRef]
- LeBaron, T.W.; Larson, A.J.; Ohta, S.; Mikami, T.; Barlow, J.; Bulloch, J.; DeBeliso, M. Acute supplementation with molecular hydrogen benefits submaximal exercise indices. Randomized, double-blinded, placebo-controlled crossover pilot study. J. Lifestyle Med. 2019, 9, 36. [Google Scholar] [CrossRef] [PubMed]
- Kishimoto, Y.; Kato, T.; Ito, M.; Azuma, Y.; Fukasawa, Y.; Ohno, K.; Kojima, S. Hydrogen ameliorates pulmonary hypertension in rats by anti-inflammatory and anti-oxidant effects. J. Thorac. Cardiovasc. Surg. 2015, 150, 645–654. [Google Scholar] [CrossRef] [PubMed]
- Ohsawa, I. Biological Responses to Hydrogen molecule and its preventive effects on inflammatory diseases. Curr. Pharm. Des. 2021, 27, 659–666. [Google Scholar] [CrossRef] [PubMed]
- Yoritaka, A.; Takanashi, M.; Hirayama, M.; Nakahara, T.; Ohta, S.; Hattori, N. Pilot study of H2 therapy in Parkinson’s disease: A randomized double-blind placebo-controlled trial. Mov. Disord. 2013, 28, 836–839. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, M.; Kabayama, S.; Ito, S. The hydrogen molecule as anti-oxidant therapy: Clinical application in hemodialysis and perspectives. Ren. Replace. Ther. 2016, 2, 23. [Google Scholar] [CrossRef]
- Franceschelli, S.; Gatta, D.M.P.; Pesce, M.; Ferrone, A.; Di Martino, G.; Di Nicola, M.; De Lutiis, M.A.; Vitacolonna, E.; Patruno, A.; Grilli, A.; et al. Modulation of the oxidative plasmatic state in gastroesophageal reflux disease with the addition of rich water molecular hydrogen: A new biological vision. J. Cell. Mol. Med. 2018, 22, 2750–2759. [Google Scholar] [CrossRef]
- Chen, X.; Zhai, X.; Shi, J.; Liu, W.W.; Tao, H.; Sun, X.; Kang, Z. Lactulose mediates suppression of dextran sodium sulfate-induced colon inflammation by increasing hydrogen production. Dig. Dis. Sci. 2013, 58, 1560–1568. [Google Scholar] [CrossRef]
- Nakao, A.; Toyoda, Y.; Sharma, P.; Evans, M.; Guthrie, N. Effectiveness of hydrogen rich water on anti-oxidant status of subjects with potential metabolic syndrome—An open label pilot study. J. Clin. Biochem. Nutr. 2010, 46, 140–149. [Google Scholar] [CrossRef]
- Ierardi, E.; Rosania, R.; Zotti, M.; Principe, S.; Laonigro, G.; Giorgio, F.; de Francesco, V.; Panella, C. Metabolic syndrome and gastro-esophageal reflux: A link towards a growing interest in developed countries. World J. Gastrointest. Pathophysiol. 2010, 1, 91. [Google Scholar] [CrossRef]
- Chen, H.; Sun, Y.P.; Hu, P.F.; Liu, W.W.; Xiang, H.G.; Li, Y.; Yan, R.L.; Su, N.; Ruan, C.P.; Sun, X.J.; et al. The effects of hydrogen-rich saline on the contractile and structural changes of intestine induced by ischemia-reperfusion in rats. J. Surg. Res. 2011, 167, 316–322. [Google Scholar] [CrossRef]
- Shen, N.Y.; Bi, J.B.; Zhang, J.Y.; Zhang, S.M.; Gu, J.X.; Qu, K.; Liu, C. Hydrogen-rich water protects against inflammatory bowel disease in mice by inhibiting endoplasmic reticulum stress and promoting heme oxygenase-1 expression. World J. Gastroenterol. 2017, 23, 1375. [Google Scholar] [CrossRef]
- Aoki, K.; Nakao, A.; Adachi, T.; Matsui, Y.; Miyakawa, S. Pilot study: Effects of drinking hydrogen-rich water on muscle fatigue caused by acute exercise in elite athletes. Med. Gas Res. 2012, 2, 12. [Google Scholar] [CrossRef]
- Russell, G.; Rehman, M.; TW, L.; Veal, D.; Adukwu, E.; Hancock, J. An overview of SARS-CoV-2 (COVID-19) infection and the importance of molecular hydrogen as an adjunctive therapy. React. Oxyg. Species 2020, 10, 150–165. [Google Scholar] [CrossRef]
- Barancik, M.; Kura, B.; LeBaron, T.W.; Bolli, R.; Buday, J.; Slezak, J. Molecular and cellular mechanisms associated with effects of molecular hydrogen in cardiovascular and central nervous systems. Antioxidants 2020, 9, 1281. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Wei, C.H.; Chen, A.L.; Sun, X.C.; Guo, G.Y.; Zou, X.; Shi, J.D.; Lai, P.Z.; Zheng, Z.G.; Zhong, N.S. Hydrogen/oxygen mixed gas inhalation improves disease severity and dyspnea in patients with Coronavirus disease 2019 in a recent multicenter, open-label clinical trial. J. Thorac. Dis. 2020, 12, 3448. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Feng, X.; Fan, Y.; Zhu, G.; Bai, C. Molecular hydrogen alleviates asthma through inhibiting IL-33/ILC2 axis. Inflamm. Res. 2021, 70, 569–579. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.; Li, D.; Hu, J.; Mei, H.; Shu, J.; Long, Z.; Yuan, L.; Li, D.; Guan, R.; Li, Y.; et al. Hydrogen gas inhalation protects against cigarette smoke-induced COPD development in mice. J. Thorac. Dis. 2018, 10, 3232. [Google Scholar] [CrossRef]
- Yamamoto, R.; Homma, K.; Suzuki, S.; Sano, M.; Sasaki, J. Hydrogen gas distribution in organs after inhalation: Real-time monitoring of tissue hydrogen concentration in rat. Sci. Rep. 2019, 9, 1–7. [Google Scholar]
- Sano, M.; Ichihara, G.; Katsumata, Y.; Hiraide, T.; Hirai, A.; Momoi, M.; Tamura, T.; Ohata, S.; Kobayashi, E. Pharmacokinetics of a single inhalation of hydrogen gas in pigs. PLoS ONE 2020, 15, e0234626. [Google Scholar] [CrossRef]
- Zhang, Y.; Xu, J.; Yang, H. Hydrogen: An endogenous regulator of liver homeostasis. Front. Pharmacol. 2020, 11, 877. [Google Scholar] [CrossRef]
- Kamimura, N.; Nishimaki, K.; Ohsawa, I.; Ohta, S. Molecular hydrogen improves obesity and diabetes by inducing hepatic FGF21 and stimulating energy metabolism in db/db mice. Obesity 2011, 19, 1396–1403. [Google Scholar] [CrossRef]
- Liu, B.; Xue, J.; Zhang, M.; Wang, M.; Ma, T.; Zhao, M.; Gu, Q.; Qin, S. Hydrogen inhalation alleviates non-alcoholic fatty liver disease in metabolic syndrome rats. Mol. Med. Rep. 2020, 22, 2860–2868. [Google Scholar] [PubMed]
- Xie, K.; Liu, L.; Yu, Y.; Wang, G. Hydrogen gas presents a promising therapeutic strategy for sepsis. BioMed Res. Int. 2014, 2014, 807635. [Google Scholar] [CrossRef] [PubMed]
- Qiu, P.; Liu, Y.; Zhang, J. Recent advances in studies of molecular hydrogen against sepsis. Int. J. Biol. Sci. 2019, 15, 1261. [Google Scholar] [CrossRef] [PubMed]
- Qi, B.; Yu, Y.; Wang, Y.; Wang, Y.; Yu, Y.; Xie, K. Perspective of molecular hydrogen in the treatment of sepsis. Curr. Pharm. Des. 2021, 27, 667–678. [Google Scholar] [CrossRef]
- Tamura, T.; Hayashida, K.; Sano, M.; Suzuki, M.; Shibusawa, T.; Yoshizawa, J.; Kobayashi, Y.; Suzuki, T.; Ohta, S.; Morisaki, H.; et al. Feasibility and safety of hydrogen gas inhalation for post-cardiac arrest syndrome–first-in-human pilot study. Circ. J. 2016, 80, 1870–1873. [Google Scholar] [CrossRef]
- Chi, J.; Li, Z.; Hong, X.; Zhao, T.; Bie, Y.; Zhang, W.; Yang, J.; Feng, Z.; Yu, Z.; Xu, Q.; et al. Inhalation of hydrogen attenuates progression of chronic heart failure via suppression of oxidative stress and P53 related to apoptosis pathway in rats. Front. Physiol. 2018, 9, 1026. [Google Scholar] [CrossRef]
- Zhang, Y.; Tan, S.; Xu, J.; Wang, T. Hydrogen therapy in cardiovascular and metabolic diseases: From bench to bedside. Cell. Physiol. Biochem. 2018, 47, 1–10. [Google Scholar] [CrossRef]
- Katsumata, Y.; Sano, F.; Abe, T.; Tamura, T.; Fujisawa, T.; Shiraishi, Y.; Kohsaka, S.; Ueda, I.; Homma, K.; Suzuki, M.; et al. The effects of hydrogen gas inhalation on adverse left ventricular remodeling after percutaneous coronary intervention for ST-elevated myocardial infarction—First pilot study in humans. Circ. J. 2017, CJ-17-0105. [Google Scholar] [CrossRef]
- Данилoва, Д.А.; Бричкин, Ю.Д.; Медведев, А.П.; Пичугин, В.В.; Федoрoв, С.А.; Таранoв, Е.В.; Назарoв, Е.И.; Рязанoв, М.В.; Бoльшухин, Г.В.; Дерюгина, А.В. Application of molecular hydrogen in heart surgery under cardiopulmonary bypass. Сoвременные Технoлoгии Медицине 2021, 13, 71–77. [Google Scholar]
- Song, G.; Tian, H.; Qin, S.; Sun, X.; Yao, S.; Zong, C.; Luo, Y.; Liu, J.; Yu, Y.; Sang, H.; et al. Hydrogen decreases athero-susceptibility in apolipoprotein B-containing lipoproteins and aorta of apolipoprotein E knockout mice. Atherosclerosis 2012, 221, 55–65. [Google Scholar] [CrossRef]
- Hori, A.; Ichihara, M.; Kimura, H.; Ogata, H.; Kondo, T.; Hotta, N. Inhalation of molecular hydrogen increases breath acetone excretion during submaximal exercise: A randomized, single-blinded, placebo-controlled study. Med. Gas Res. 2020, 10, 96. [Google Scholar] [CrossRef]
- Javorac, D.; Stajer, V.; Ratgeber, L.; Betlehem, J.; Ostojic, S. Short-term H2 inhalation improves running performance and torso strength in healthy adults. Biol. Sport 2019, 36, 333. [Google Scholar] [CrossRef] [PubMed]
- Alleman, R.J.; Katunga, L.A.; Nelson, M.A.; Brown, D.A.; Anderson, E.J. The “Goldilocks Zone” from a redox perspective—Adaptive vs. deleterious responses to oxidative stress in striated muscle. Front. Physiol. 2014, 5, 358. [Google Scholar] [CrossRef]
- Fu, Z.; Zhang, Z.; Wu, X.; Zhang, J. Hydrogen-rich saline inhibits lipopolysaccharide-induced acute lung injury and endothelial dysfunction by regulating autophagy through mTOR/TFEB signaling pathway. BioMed Res. Int. 2020, 9121894. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Zhou, C.; Xie, K.; Meng, X.; Wang, Y.; Yu, Y. Hydrogen-rich saline alleviated the hyperpathia and microglia activation via autophagy mediated inflammasome inactivation in neuropathic pain rats. Neuroscience 2019, 421, 17–30. [Google Scholar] [CrossRef]
- Ishibashi, T.; Sato, B.; Shibata, S.; Sakai, T.; Hara, Y.; Naritomi, Y.; Koyanagi, S.; Hara, H.; Nagao, T. Therapeutic efficacy of infused molecular hydrogen in saline on rheumatoid arthritis: A randomized, double-blind, placebo-controlled pilot study. Int. Immunopharmacol. 2014, 21, 468–473. [Google Scholar] [CrossRef] [PubMed]
- Uto, K.; Sakamoto, S.; Que, W.; Shimata, K.; Hashimoto, S.; Sakisaka, M.; Narita, Y.; Yoshii, D.; Zhong, L.; Komohara, Y.; et al. Hydrogen-rich solution attenuates cold ischemia-reperfusion injury in rat liver transplantation. BMC Gastroenterol. 2019, 8, 25. [Google Scholar] [CrossRef]
- Okamoto, A.; Kohama, K.; Aoyama-Ishikawa, M.; Yamashita, H.; Fujisaki, N.; Yamada, T.; Yumoto, T.; Nosaka, N.; Naito, H.; Tsukahara, K.; et al. Intraperitoneally administered, hydrogen-rich physiologic solution protects against postoperative ileus and is associated with reduced nitric oxide production. Surgery 2016, 160, 623–631. [Google Scholar] [CrossRef]
- Sada, H.; Egi, H.; Ide, K.; Sawada, H.; Sumi, Y.; Hattori, M.; Sentani, K.; Oue, N.; Yasui, W.; Ohdan, H. Peritoneal lavage with hydrogen-rich saline can be an effective and practical procedure for acute peritonitis. Surg. Today 2021, 51, 1860–1871. [Google Scholar] [CrossRef]
- Guo, K.W. Green nanotechnology of trends in future energy: A review. Int. J. Energy Res. 2012, 36, 1–17. [Google Scholar] [CrossRef]
- Sutariya, V.B.; Pathak, Y. (Eds.) Biointeractions of Nanomaterials; CRC Press: Boca Raton, FL, USA, 2014. [Google Scholar]
- Liu, Y.; Li, J.; Chen, M.; Chen, X.; Zheng, N. Palladium-based nanomaterials for cancer imaging and therapy. Theranostics 2014, 10, 10057. [Google Scholar] [CrossRef] [PubMed]
- Bilal, M.; Barani, M.; Sabir, F.; Rahdar, A.; Kyzas, G.Z. Nanomaterials for the treatment and diagnosis of Alzheimer’s disease: An overview. NanoImpact 2020, 20, 100251. [Google Scholar] [CrossRef]
- Murthy, S.K. Nanoparticles in modern medicine: State of the art and future challenges. Int. J. Nanomed. 2007, 2, 129. [Google Scholar]
- Zhang, L.; Zhao, P.; Yue, C.; Jin, Z.; Liu, Q.; Du, X.; He, Q. Sustained release of bioactive hydrogen by Pd hydride nanoparticles overcomes Alzheimer’s disease. Biomaterials 2019, 197, 393–404. [Google Scholar] [CrossRef]
- Zhan, C.; Li, H.; Li, X.; Jiang, Y.; Xie, Z. Synthesis of PdH 0.43 nanocrystals with different surface structures and their catalytic activities towards formic acid electro-oxidation. Sci. China Mater. 2020, 63, 375–382. [Google Scholar] [CrossRef]
- Zhao, P.; Jin, Z.; Chen, Q.; Yang, T.; Chen, D.; Meng, J.; Lu, X.; Gu, Z.; He, Q. Local generation of hydrogen for enhanced photothermal therapy. Nat. Commun. 2018, 9, 4241. [Google Scholar] [CrossRef]
- Perricone, N.V.; Perricone Hydrogen Water Company LLC. Medication Enhancement Using Hydrogen. U.S. Patent 10,076,540, 18 September 2018. [Google Scholar]
- Safonov, V.L.; H2 Universe LLC. Systems and Methods for Topical Application of Molecular Hydrogen. U.S. Patent Application No. 16/376,894, 2019. pending. [Google Scholar]
- Satoh, F.; Sasaki, H.; Kurokawa, R.; Hirano, S.; Ichikawa, Y.; Miz Co Ltd. Method and Molecular Hydrogen-Containing Composition for Promotion of Postoperative Recovery. U.S. Patent Application 17/147,692, 2021. pending. [Google Scholar]
- Yoon, K.S.; Huang, X.Z.; Yoon, Y.S.; Kim, S.K.; Song, S.B.; Chang, B.S.; Kim, D.H.; Lee, K.J. Histological study on the effect of electrolyzed reduced water-bathing on UVB radiation-induced skin injury in hairless mice. Biol. Pharm. Bull. 2011, 34, 1671–1677. [Google Scholar] [CrossRef]
- Zhu, Q.; Wu, Y.; Li, Y.; Chen, Z.; Wang, L.; Xiong, H.; Dai, E.; Wu, J.; Fan, B.; Ping, L.; et al. Positive effects of hydrogen-water bathing in patients of psoriasis and parapsoriasis en plaques. Sci. Rep. 2018, 8, 8051. [Google Scholar] [CrossRef]
- Tarnava, A. Supersaturated Hydrogen-Rich Water Hydrotherapy for Recovery of Acute Injury to the Proximal Phalanges on the 5th Toe: A Case Report. J. Sci. Med. 2021, 3. [Google Scholar] [CrossRef]
- Lebwohl, M. A clinician’s paradigm in the treatment of psoriasis. J. Am. Acad. Dermatol. 2005, 53, S59–S69. [Google Scholar] [CrossRef] [PubMed]
- Ohta, S. Molecular hydrogen as a preventive and therapeutic medical gas: Initiation, development and potential of hydrogen medicine. Pharmacol. Ther. 2014, 144, 1–11. [Google Scholar] [CrossRef]
- Huang, C.S.; Kawamura, T.; Toyoda, Y.; Nakao, A. Recent advances in hydrogen research as a therapeutic medical gas. Free Radic. Res. 2010, 44, 971–982. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Zhang, H.T.; Qin, S.C. Neuroprotective effects of molecular hydrogen: A critical review. Neurosci. Bull. 2021, 37, 389–404. [Google Scholar] [CrossRef] [PubMed]
- Shin, W. Medical applications of breath hydrogen measurements. Anal. Bioanal. Chem. 2014, 406, 3931–3939. [Google Scholar] [CrossRef]
- Hancock, J.T.; LeBaron, T.W.; Russell, G. Molecular Hydrogen: Redox Reactions and Possible Biological Interactions. React. Oxyg. Species 2021, 11, 17–25. [Google Scholar] [CrossRef]
- Dincer, I. Green methods for hydrogen production. Int. J. Hydrog. Energy 2012, 37, 1954–1971. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Organ | H2 Concentration-µmol/L | Comments |
|---|---|---|
| Brain | 26 | H2 can traverse the blood–brain barrier |
| Kidney | 18 | Lowest tested tissue concentration of H2 |
| Liver | 29 | Glycogen has a high capacity for storing H2 |
| Mesentery Fat | 23 | Improved lipid profiling |
| Thigh Muscle | 18 | Retained H2 significantly longer than other tissues |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Russell, G.; Nenov, A.; Kisher, H.; Hancock, J.T. Molecular Hydrogen as Medicine: An Assessment of Administration Methods. Hydrogen 2021, 2, 444-460. https://doi.org/10.3390/hydrogen2040025
Russell G, Nenov A, Kisher H, Hancock JT. Molecular Hydrogen as Medicine: An Assessment of Administration Methods. Hydrogen. 2021; 2(4):444-460. https://doi.org/10.3390/hydrogen2040025
Chicago/Turabian StyleRussell, Grace, Alexander Nenov, Hesham Kisher, and John T. Hancock. 2021. "Molecular Hydrogen as Medicine: An Assessment of Administration Methods" Hydrogen 2, no. 4: 444-460. https://doi.org/10.3390/hydrogen2040025
APA StyleRussell, G., Nenov, A., Kisher, H., & Hancock, J. T. (2021). Molecular Hydrogen as Medicine: An Assessment of Administration Methods. Hydrogen, 2(4), 444-460. https://doi.org/10.3390/hydrogen2040025