Abstract
Background and Objectives: Effective pain management is essential for optimizing recovery after laparoscopic cholecystectomy (LC). Ultrasound-guided erector spinae plane (ESP) and transversus abdominis plane (TAP) blocks are validated techniques, but may be limited by equipment requirements and technical complexity. This study aimed to evaluate whether surgeon-delivered local anesthetic infiltration provides comparable analgesic efficacy. Materials and Methods: This prospective, randomized, controlled, single-center trial enrolled 172 patients undergoing elective LC between November 2020 and June 2022. Patients were randomized into four groups: Group A—surgeon-delivered port-site and intraperitoneal bupivacaine infiltration; Group B—ESP block; Group C—TAP block; and Group D—control. Primary outcomes were postoperative pain assessed by Visual Analog Scale (VAS) scores at 1, 3, 6, 12, and 24 h, and Behavioral Pain Scale (BPS) scores at 1 and 3 h. Secondary outcomes included 24 h tramadol consumption, patient satisfaction, additional rescue analgesia requirement, and procedure duration. Results: All intervention groups (A–C) demonstrated significantly lower VAS and BPS scores compared to controls (VAS at 24 h: 1.8 ± 0.9 vs. 2.8 ± 1.3, p < 0.001). Tramadol use was also reduced (≈82 mg vs. 97 mg, p < 0.001), with fewer opioid-related adverse effects. No significant differences were observed among Groups A–C. Patient satisfaction was higher in the intervention groups, and no major complications were reported. Conclusions: Surgeon-delivered local infiltration achieved analgesic efficacy equivalent to ESP and TAP blocks. Considering its simplicity, safety, and minimal resource demands, this method may represent a practical alternative for enhanced recovery pathways following LC.
1. Introduction
Although laparoscopic cholecystectomy (LC) is minimally invasive, patients frequently experience significant postoperative pain in the first 24 h, arising from trocar-site incisions, peritoneal insufflation, and gallbladder bed inflammation [1,2]. This pain can delay recovery and reduce patient satisfaction.
Systemic analgesics such as opioids and NSAIDs are commonly used, but their side effects and limited efficacy for visceral pain have encouraged multimodal strategies [3]. Surgeon-administered local anesthetic infiltration is one of the earliest and most practical methods, and previous studies have shown its efficacy in reducing both incisional and referred shoulder pain [4,5].
In recent years, ultrasound-guided regional techniques—particularly the transversus abdominis plane (TAP) and erector spinae plane (ESP) blocks—have gained attention. These blocks provide effective somatic and partial visceral analgesia [6,7], and meta-analyses confirm that TAP blocks significantly reduce pain scores and opioid consumption compared with systemic analgesia alone [8]. However, several randomized trials have reported comparable outcomes between TAP block and local infiltration [9].
ESP block has also emerged as a promising modality, with trials showing reduced pain, opioid use, and postoperative nausea [10,11]. Nevertheless, its widespread application is limited by the need for ultrasound equipment, expertise, and additional operative time.
Therefore, optimizing surgeon-delivered techniques—such as combined port-site and intraperitoneal infiltration with bupivacaine—may offer analgesic efficacy comparable to ESP and TAP blocks while being simpler and more accessible [12]. This question is particularly relevant in enhanced recovery after surgery (ERAS) protocols, where safe, reproducible, and opioid-sparing strategies are prioritized.
Accordingly, we conducted a randomized controlled trial to evaluate whether surgeon-delivered infiltration provides analgesia equivalent to ultrasound-guided ESP and TAP blocks in patients undergoing LC. We hypothesized that infiltration would be non-inferior regarding pain scores, opioid consumption, and patient satisfaction.
2. Materials and Methods
2.1. Study Design and Ethical Approval
This randomized, controlled, single-center trial was prospectively conducted between November 2020 and June 2022. In accordance with local regulatory processes, the study was conducted prospectively; however, ethical approval from the Clinical Research Ethics Committee of Afyonkarahisar Health Sciences University was formally obtained later (Meeting No: 2022/8, Approval Date: 1 July 2022). Prior to surgery, all patients were thoroughly informed about laparoscopic cholecystectomy, general anesthesia, and the regional block techniques, and written informed consent was obtained for each of these procedures. The analgesic techniques evaluated (local infiltration, ESP, and TAP blocks) are established components of perioperative practice and posed no additional risk beyond routine care.
2.2. Patient Selection and Inclusion Criteria
A total of 190 consecutive patients scheduled for elective LC at two public hospitals were screened. Eighteen were excluded: ten for not meeting inclusion criteria [acute cholecystitis (n = 2), previous upper abdominal surgery (n = 2), gallstone pancreatitis (n = 1), coagulopathy (n = 1), previous ERCP (n = 1), elevated preoperative inflammatory markers (n = 3)], five declined participation, and three were excluded for non-compliance. Ultimately, 172 patients aged 18–75 years with ASA I–III and normal preoperative CRP/WBC values were enrolled and randomized into four groups: Group A (infiltration, n = 45), Group B (ESP block, n = 42), Group C (TAP block, n = 41), and Group D (control, n = 44). The patient selection and allocation process is illustrated in Figure 1.
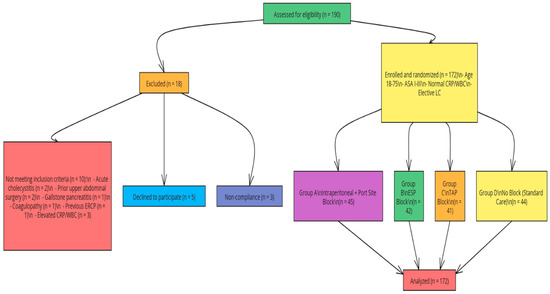
Figure 1.
Patient enrollment and allocation. A total of 190 patients were assessed for eligibility; 172 were randomized into four groups and included in the final analysis.
2.3. Randomization and Blinding
Randomization was performed using a computer-generated sequence stratified by ASA score. Allocation concealment was maintained with sealed, opaque envelopes prepared by an independent researcher not involved in patient care. The study was conducted in a single-blind fashion: patients and outcome assessors were blinded to group assignment, while the clinicians performing anesthesia or infiltration were necessarily aware of the interventions. Postoperative data collection was conducted by an independent anesthesiologist blinded to group allocation.
2.4. Anesthesia and Surgical Protocol
Standard ASA monitoring (electrocardiogram, noninvasive blood pressure, pulse oximetry, and temperature) was applied to all patients. General anesthesia was induced with intravenous fentanyl (Fentanyl®, Janssen, Beerse, Belgium; 1–2 μg/kg), propofol (Propofol®, Fresenius Kabi, Bad Homburg, Germany; 2 mg/kg), and rocuronium bromide (Esmeron®, Merck Sharp & Dohme, Haarlem, The Netherlands; 0.6 mg/kg). Maintenance was achieved with sevoflurane (Sevorane®, AbbVie, Chicago, IL, USA; 0.8–1 MAC) in a 50% O2–air mixture, supplemented with remifentanil infusion (Ultiva®, GlaxoSmithKline, Brentford, UK; 0.05–0.2 μg/kg/min), titrated according to hemodynamic responses. Pneumoperitoneum was established at 12 mmHg, and all laparoscopic cholecystectomies were performed in a standardized four-port technique. To prevent postoperative nausea and vomiting (PONV), 4 mg ondansetron (Zofran®, GlaxoSmithKline, Brentford, UK) was administered intravenously near the end of surgery. All procedures were performed by the same surgeon and the same anesthesiologist to minimize variability. All blocks were performed under general anesthesia after induction, prior to skin incision.
2.5. Interventions
Group A (Infiltration): Surgeon-delivered intraperitoneal and port-site infiltration with 40 mL of 0.25% bupivacaine (Marcaine®, AstraZeneca, Södertälje, Sweden; 20 mL intraperitoneal, 20 mL distributed across trocar sites). For trocar infiltration, 6 mL was injected into each 10 mm port and 4 mL into each 5 mm port, ensuring infiltration into skin, fascia, and peritoneal layers.
Group B (ESP block): Bilateral ESP blocks were performed with the patient in the lateral decubitus position at the T8 level with a high-frequency linear ultrasound probe (DC-60, Mindray, Shenzhen, China; 6–13 MHz). Using an in-plane technique, a 22-gauge needle (Braun, Melsungen, Germany) was advanced to the erector spinae plane on the transverse process. Twenty milliliters of 0.25% bupivacaine (Marcaine®, AstraZeneca, Södertälje, Sweden) was injected per side, with spread confirmed sonographically in cranio-caudal directions.
Group C (TAP block): Bilateral oblique subcostal TAP blocks were performed with the patient in the supine position under ultrasound guidance (DC-60, Mindray, Shenzhen, China). With the probe placed parallel to the costal margin, the space between the rectus abdominis and transversus abdominis muscle fascia was targeted using an in-plane needle approach (22-gauge, Braun, Melsungen, Germany). Twenty milliliters of 0.25% bupivacaine (Marcaine®, AstraZeneca, Södertälje, Sweden) was administered per side, and adequate distribution was confirmed.
Group D (Control): Standard LC without additional local or regional analgesia.2.6.
2.6. Postoperative Analgesia and Data Collection
All patients received standardized postoperative analgesia consisting of intravenous paracetamol (1 g every 8 h). Rescue analgesia was provided with intravenous tramadol (1 mg/kg). Pain was assessed using the VAS at 1, 3, 6, 12, and 24 h, and the BPS at 1 and 3 h. Other adverse effects (e.g., pruritus) were likewise assessed both by Likert score (0–3) and by incidence (present/absent). Patient satisfaction was measured on a 0–10 numeric rating scale.
2.7. Outcome Measures
2.7.1. Primary Outcomes
- VAS scores at 1, 3, 6, 12, and 24 h
- BPS scores at 1 and 3 h
- 24 h tramadol consumption (mg)
2.7.2. Secondary Outcomes
- Time to first analgesic request (h)
- Patient satisfaction (0–10)
- Pruritus (Likert score 0–3 and incidence %)
- Length of hospital stay (h, maximum 24 h)
- Additional rescue analgesia requirement
- Duration of ESP/TAP procedures (min)
- Block-related complications (hematoma, local toxicity, failure)
2.8. Sample Size and Power Analysis
Sample size was calculated using G*Power 3.1 based on Altiparmak et al. [1], which reported an 8 mg difference in 24 h opioid consumption (SD = 12 mg). To achieve 80% power at α = 0.05, a minimum of 72 patients (at least 18 per group) was required. Enrollment of 172 patients across four groups exceeded this requirement.
2.9. Statistical Analysis
Data were analyzed using SPSS v26.0. Distribution normality was assessed with the Shapiro–Wilk test, and homogeneity of variance with the Levene test. Parametric variables were compared using one-way ANOVA with Bonferroni correction; non-parametric variables with Kruskal–Wallis and Dunn–Bonferroni post hoc tests. Repeated measures ANOVA evaluated time-dependent changes in VAS and BPS scores. Categorical variables were analyzed with chi-square or Fisher’s exact test, applying continuity correction where appropriate. A p-value < 0.05 was considered statistically significant.
3. Results
A total of 172 patients were randomized and completed the study: Group A (n = 45), Group B (n = 42), Group C (n = 41), and Group D (n = 44). Baseline demographic and clinical characteristics are presented in Table 1. No significant intergroup differences were observed in age, sex, BMI, ASA status, prior abdominal surgery, CRP, WBC, comorbidities (diabetes, hypertension, hyperlipidemia), or lifestyle factors (smoking, alcohol use) (all p > 0.05). The only significant variation was anesthesia duration, which was longer in Groups B and C compared with Groups A and D (p < 0.001), reflecting the additional time required for block procedures.

Table 1.
Demographic, clinical, and comorbidity characteristics.
Postoperative pain scores are summarized in Table 2. VAS and BPS values were significantly lower in Groups A–C compared with Group D at all assessed time points (p < 0.001), with no significant differences among Groups A–C (p > 0.05). Repeated-measures ANOVA demonstrated a significant time effect for both VAS (F(4, 316) = 41.70, p < 0.001, η2 = 0.35) and BPS (F(1, 79) = 6.25, p = 0.015, η2 = 0.07). The temporal trajectory of VAS across groups is shown in Figure 2, and early BPS changes are depicted in Figure 3.
Table 2.
Postoperative pain scores and analgesic outcomes.
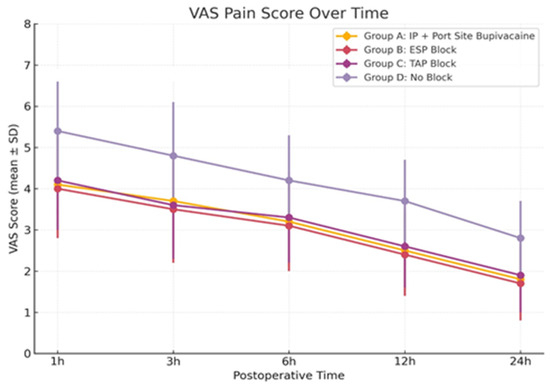
Figure 2.
VAS Pain Score Over Time. Postoperative Visual Analog Scale (VAS) scores at 1, 3, 6, 12, and 24 h. Data presented as mean ± SD. p values indicate comparisons between intervention and control groups using ANOVA with Bonferroni correction.
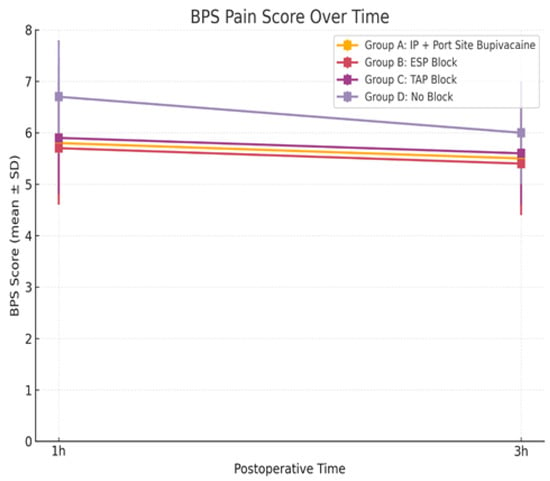
Figure 3.
BPS Pain Score Over Time. Behavioral Pain Scale (BPS) scores at 1 and 3 hours postoperatively. Data presented as mean ± SD. p values indicate comparisons between intervention and control groups using ANOVA with Bonferroni correction.
Total 24 h tramadol consumption was significantly lower in Groups A–C compared with Group D (p < 0.001). The mean reduction of ~15 mg was observed, with fewer opioid-related adverse effects and a longer time to first rescue analgesia. In addition to mean tramadol consumption, 15–17% of patients in Groups A–C required rescue analgesia compared with 34.1% in Group D (Table 3). Furthermore, the mean time to first analgesic request was significantly prolonged in Groups A–C (~5 h) compared with Group D (3.4 ± 1.0 h, p < 0.001; Table 2). Patient satisfaction scores were also significantly higher in the intervention groups (p < 0.001).
Table 3.
Secondary outcomes and complications.
Secondary outcomes are summarized in Table 3. Pruritus showed a non-significant trend favoring the intervention groups.
The mean block duration was 6.2 ± 1.0 min in Group B and 6.5 ± 1.1 min in Group C, with no significant difference between groups (p = 0.31). Minor block-related adverse events occurred in only 2.4% of patients in Groups B and C and resolved spontaneously. No major complications were observed. Hospital stay did not differ significantly across groups (p = 0.28); all patients were discharged within 24 h. Patient satisfaction distributions by group are presented in Figure 4.
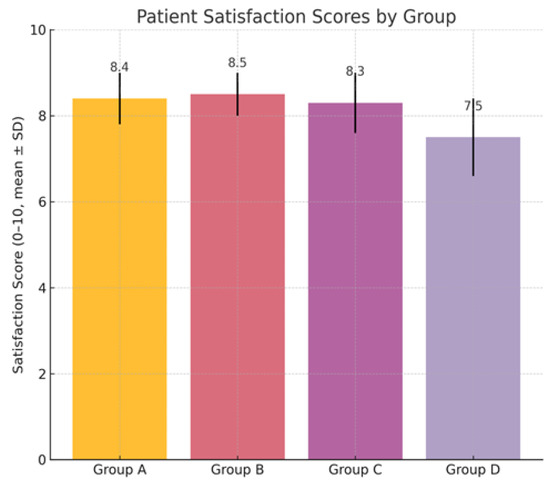
Figure 4.
Patient satisfaction scores (0–10 scale) within 24 h postoperatively. Data presented as mean ± SD. p values indicate comparisons between intervention and control groups using ANOVA with Bonferroni correction.
4. Discussion
This study demonstrated that surgeon-delivered bupivacaine infiltration provided analgesic efficacy comparable to ultrasound-guided ESP and TAP blocks in patients undergoing laparoscopic cholecystectomy (LC). All three active interventions significantly reduced postoperative pain scores, opioid consumption, and opioid-related side effects compared with standard systemic analgesia, while patient satisfaction remained equally high across groups. No major complications were observed in either the block or infiltration groups, supporting the overall safety of these strategies.
Previous studies have established that regional anesthesia techniques such as TAP and ESP blocks can provide effective postoperative analgesia in LC. Randomized trials and meta-analyses have consistently shown that TAP blocks reduce postoperative VAS scores and opioid requirements compared to systemic analgesia alone [13,14]. In addition, recent systematic reviews and meta-analyses have confirmed that both TAP and ESP blocks provide significant analgesic benefits compared with no intervention, while showing no major differences when compared directly with local infiltration techniques [14,15,16,17,18,19]. Similarly, ESP blocks have emerged as an effective modality with favorable recovery profiles [9,10]. In agreement with these findings, our results confirmed that both ESP and TAP blocks significantly lowered pain scores and tramadol use relative to controls. A recent multicenter randomized trial by Nalbant et al. also demonstrated that ESP, TAP, and trocar-site infiltration provided comparable analgesic outcomes in LC, supporting our observation that surgeon-delivered infiltration can match block efficacy [20].
Importantly, our findings extend the existing literature by demonstrating that surgeon-delivered infiltration can achieve equivalent outcomes to these block techniques. Ortiz et al. reported no difference between TAP block and trocar-site infiltration regarding postoperative pain and opioid use [21], and later trials confirmed similar observations [22]. These findings are consistent with the multicenter randomized trial of Nalbant et al., which demonstrated comparable outcomes among ESP, TAP, and trocar-site infiltration [20]. Our study extends these observations by including combined intraperitoneal and trocar-site infiltration, thereby demonstrating equivalence not only with TAP, but also with ESP blocks. Similarly, Stasiowski et al. demonstrated that infiltration anaesthesia significantly improved perioperative outcomes following lumbar discectomy under general anaesthesia, further underscoring the versatility and clinical relevance of infiltration techniques across different surgical fields [23]. By contrast, some randomized studies suggested a transient early advantage of TAP block over infiltration, particularly in the first 2 h postoperatively, with prolonged time to rescue analgesia [24]. However, those studies typically employed port-site infiltration alone. In our protocol, infiltration combined both port-site and intraperitoneal administration, targeting both somatic and visceral pain. This broader approach likely explains why our infiltration group achieved outcomes comparable to ESP and TAP blocks across the full 24 h period. A recent meta-analysis also concluded that TAP blocks were superior to no intervention but not significantly different from infiltration techniques, which aligns closely with our results [14].
The analgesic mechanisms of ESP block have been investigated in cadaveric and radiological studies. It has been shown that an injection at thoracic levels can spread to the paravertebral, intercostal, and occasionally prevertebral spaces, potentially explaining its efficacy on both visceral and somatic pain [25,26,27]. Rahimzadeh et al. even reported bilateral sensory effects after unilateral ESP block, supporting its wide mediastinal and paravertebral diffusion [28].
The equivalence observed between ESP and TAP blocks in our series is consistent with previous meta-analyses, which showed similar reductions in pain intensity and opioid consumption [16,18,29]. Our data support the interpretation that the choice between TAP and ESP may depend more on practitioner expertise, patient anatomy, and resource availability than on major efficacy differences. Notably, in our cohort, infiltration with intraperitoneal bupivacaine produced a ~15% reduction in tramadol use (mean 82–83 mg/24 h), comparable to both ESP and TAP groups, underscoring the clinical relevance of adequately treating visceral pain [28,29,30]. Although the absolute opioid-sparing effect corresponds to approximately 1.5 mg of morphine equivalent over 24 h, which may appear modest, its clinical relevance is supported by the lower need for rescue analgesia and the higher patient satisfaction observed in the intervention groups.
Another relevant point is the different absorption characteristics of local anesthetics depending on the tissue. TAP blocks, performed in a relatively less vascularized fascial plane, may prolong the duration of analgesia compared with infiltration at trocar sites, which have denser vascularity and potentially faster systemic absorption [7,12,31]. This pharmacokinetic difference may partially explain why some studies observed longer-lasting analgesia with TAP despite using the same agents. In our study, however, the addition of intraperitoneal bupivacaine to trocar-site infiltration likely compensated for this limitation, providing balanced somatic and visceral pain relief across the first 24 h.
Beyond analgesic efficacy, this study highlights practical advantages of surgeon-delivered infiltration. Performing bilateral ESP or TAP blocks required 15–20 additional minutes and ultrasound guidance, whereas infiltration was completed rapidly during wound closure without delaying surgery [21,32]. The logistical simplicity of infiltration, combined with equivalent analgesic outcomes, makes it an attractive option for routine LC within enhanced recovery protocols. In addition, TAP blocks are increasingly performed by surgeons, including laparoscopic-guided approaches, which broadens their applicability in clinical practice [22,24]. Consistent with prior studies, our intervention groups also demonstrated improved postoperative outcomes compared to controls [33,34,35]. The need for additional rescue analgesia was markedly reduced in Groups A–C, reflecting improved pain control in the first postoperative day. Importantly, no infiltration-related complications were observed, while only minor, self-limiting adverse events occurred in the block groups, confirming the safety of both approaches [36].
Finally, although our trial involved bilateral TAP and ESP blocks, several studies suggest unilateral applications may also provide sufficient analgesia due to contralateral spread of ESP and the efficacy of subcostal TAP when performed correctly [28,37]. Similarly, Chen et al. recently compared ESP and TAP blocks directly in LC and found no significant differences in pain scores or opioid consumption, reinforcing our conclusion that both blocks offer equivalent efficacy [38]. Future comparative studies are warranted to clarify whether unilateral versus bilateral administration influences clinical outcomes in LC.
In summary, our findings confirm that ESP and TAP blocks provide effective analgesia after LC, but also demonstrate that a properly executed surgeon-delivered infiltration can achieve equivalent efficacy. By consolidating evidence from previous RCTs [20,21,22] and meta-analyses [14,15,16,17,18,19], our trial adds novel confirmation that infiltration may serve as a pragmatic and equally effective alternative, especially in contexts with limited access to ultrasound or regional anesthesia expertise. By minimizing resource demands and procedural time without compromising outcomes, infiltration represents a practical, safe, and widely applicable alternative. Broader integration of this approach may facilitate enhanced recovery after LC, particularly in settings where access to ultrasound-guided regional anesthesia is limited [19].
This single-center design with a moderate sample size may limit the generalizability of the findings. Although patients and outcome assessors were blinded, complete blinding of surgeons was not feasible, potentially introducing a degree of performance bias. The infiltration technique combined both port-site and intraperitoneal administration; thus, results may not be directly applicable to other methods. Moreover, all procedures were performed by experienced clinicians, which may not reflect outcomes in lower-resource or learning-curve environments. Pain scores were recorded only at rest, and movement-related scores were not assessed, which represents an additional limitation of this study. The 24 h follow-up period does not capture long-term analgesic outcomes or recovery metrics. While extended follow-up (e.g., 48-h or chronic pain outcomes) would be valuable, it is generally impractical since patients undergoing elective laparoscopic cholecystectomy are typically discharged within 24 h worldwide. Notably, two patients in the control group required an additional hospital day for pain palliation. This highlights the clinical relevance of effective analgesia but introduces a minor limitation in the uniformity of 24 h outcome assessment. Another limitation is that bupivacaine was used instead of ropivacaine, as the latter was not routinely available in our setting; therefore, our findings may not be fully generalizable to centers where ropivacaine is the standard agent. PONV-related outcomes were excluded from the final analysis because group homogeneity for PONV risk factors could not be assured within this dataset. In addition, due to regulatory requirements for drug-related clinical trials in our country, formal ethics approval was granted after patient enrollment, and therefore the prospectively collected data were retrospectively registered under the ethics committee framework. Furthermore, study-specific informed consent was not obtained beyond routine surgical consent, which represents an additional limitation.
5. Conclusions
Surgeon-delivered bupivacaine infiltration achieved analgesic efficacy equivalent to ESP and TAP blocks in laparoscopic cholecystectomy. By reducing pain, opioid use, and related adverse effects while maintaining high patient satisfaction, this simple and cost-effective technique represents a practical alternative to regional blocks, particularly within ERAS pathways and day-case surgery.
Author Contributions
Conceptualization, M.C.G. and R.K.A.; methodology, M.C.G. and R.K.A.; software, M.C.G. and R.K.A.; validation, M.C.G. and R.K.A.; formal analysis, M.C.G. and R.K.A.; investigation, M.C.G. and R.K.A.; resources M.C.G. and R.K.A.; data curation, M.C.G. and R.K.A.; writing—original draft preparation, M.C.G. and R.K.A.; writing—review and editing, M.C.G. and R.K.A.; visualization, M.C.G. and R.K.A.; supervision, M.C.G. and R.K.A.; project administration, M.C.G. and R.K.A.; funding acquisition, M.C.G. and R.K.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Clinical Research Ethics Committee of Afyonkarahisar Health Sciences University (Approval No: 2022/8; Date: 1 July 2022) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to institutional and ethical restrictions.
Acknowledgments
The authors sincerely thank the operating room staff of Emirdağ State Hospital for their assistance during block procedures and for ensuring accurate perioperative data recording, as well as the nursing staff of the General Surgery Clinic for their support in the systematic collection of postoperative patient data. The authors also gratefully acknowledge Assoc. Fatih Akkuş for his valuable contributions to the statistical analysis.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| LC | Laparoscopic Cholecystectomy |
| ESP | Erector Spinae Plane |
| TAP | Transversus Abdominis Plane |
| VAS | Visual Analog Scale |
| BPS | Behavioral Pain Scale |
| PONV | Postoperative Nausea and Vomiting |
| ASA | American Society of Anesthesiologists |
| BMI | Body Mass Index |
| CRP | C-reactive Protein |
| WBC | White Blood Cell Count |
| SD | Standard Deviation |
| ANOVA | Analysis of Variance |
| ERAS | Enhanced Recovery After Surgery |
| MAC | Minimum Alveolar Concentration |
| SPSS | Statistical Package for the Social Sciences |
References
- Altıparmak, B.; Korkmaz Toker, M.; Uysal, A.I.; Kuşçu, Y.; Gümüş Demirbilek, S. Ultrasound-guided erector spinae plane block versus oblique subcostal transversus abdominis plane block for postoperative analgesia of adult patients undergoing laparoscopic cholecystectomy: Randomized, controlled trial. J. Clin. Anesth. 2019, 57, 31–36. [Google Scholar] [CrossRef]
- Macías, A.A.; Finneran, J.J. Regional Anesthesia Techniques for Pain Management for Laparoscopic Surgery: A Review of the Current Literature. Curr. Pain. Headache Rep. 2022, 26, 33–42. [Google Scholar] [CrossRef]
- Bayoumi, H.M.; Abdelaziz, D.H.; El Said, N.O.; Boraii, S.; Bendas, E.R. Postoperative pain management following laparoscopic cholecystectomy-non-opioid approaches: A review. Futur. J. Pharm. Sci. 2024, 10, 125. [Google Scholar] [CrossRef]
- Nikoubakht, N.; Faiz, S.H.R.; Mousavie, S.H.; Shafeinia, A.; Zonoz, L.B.N. Effect of Bupivacaine Intraperitoneal and Intra-Abdominal Bicarbonate in Reducing Postoperative Pain in Laparoscopic Cholecystectomy: A Double-Blind Randomized Clinical Trial Study. BMC Res. Notes 2022, 15, 103. [Google Scholar] [CrossRef]
- Bourgeois, C.; Oyaert, L.; Van de Velde, M.; Pogatzki-Zahn, E.; Freys, S.M.; Sauter, A.R.; Dewinter, G. Pain management after laparoscopic cholecystectomy: A systematic review and procedure-specific postoperative pain management (PROSPECT) recommendations. Eur. J. Anaesthesiol. EJA 2024, 41, 841–855. [Google Scholar] [CrossRef]
- Chin, K.J.; Versyck, B.; Pawa, A. Ultrasound-guided fascial plane blocks of the chest wall: A state-of-the-art review. Anaesthesia 2021, 76 (Suppl. 1), 110–126. [Google Scholar] [CrossRef] [PubMed]
- Davey, M.G.; Daly, G.R.; Donlon, N.E.; Healy, N.A.; Hill, A.D.K. Ultrasound-guided versus laparoscopic-guided transversus abdominus plane block for laparoscopic cholecystectomy—A systematic review and meta-analysis of randomised clinical trials. Surgeon 2025, 6, 3. [Google Scholar] [CrossRef]
- Irvine, D.; Rennie, C.; Coughlin, E.; Thornton, I.; Mhaskar, R.; Huang, J. The Efficacy of Transversus Abdominis Plane (TAP) Blocks When Completed by Anesthesiologists Versus by Surgeons: A Systematic Review and Meta-Analysis. Healthcare 2024, 12, 2586. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.J.; Chu, S.; Yu, E.; Joo, J.D. Comparison of the efficacy of erector spinae plane block according to the difference in bupivacaine concentrations for analgesia after laparoscopic cholecystectomy: A retrospective study. J. Yeungnam Med. Sci. 2023, 40, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Xie, Q.; Ye, W.; Zhou, Z.; Lei, Z. Ultrasound-guided erector spinae plane block for postoperative analgesia in Chinese patients undergoing laparoscopic cholecystectomy: A double-blind randomized controlled trial. Langenbecks Arch. Surg. 2023, 408, 111. [Google Scholar] [CrossRef]
- Jeong, H.-W.; Kim, C.S.; Choi, K.T.; Jeong, S.-M.; Kim, D.-H.; Lee, J.-H. Preoperative versus Postoperative Rectus Sheath Block for Acute Postoperative Pain Relief after Laparoscopic Cholecystectomy: A Randomized Controlled Study. J. Clin. Med. 2019, 8, 1018. [Google Scholar] [CrossRef]
- Chen, Q.; Chen, E.; Qian, X. A Narrative Review on Perioperative Pain Management Strategies in Enhanced Recovery Pathways—The Past, Present and Future. J. Clin. Med. 2021, 10, 2568. [Google Scholar] [CrossRef] [PubMed]
- Fayez, M.; Metias, Y.; Khalil, M.; Salah, M.; Abd, A.; Bedewy, E.; Ismail, T. Comparing Ultrasound-Guided Erector Spinae Plane Block vs Oblique Subcostal TAP Block Analgesia After Laparoscopic Cholecystectomy: A Randomized Clinical Study. Egypt. J. Hosp. Med. 2025, 100, 2985–2993. [Google Scholar] [CrossRef]
- Wang, W.; Wang, L.; Gao, Y. A Meta-Analysis of Randomized Controlled Trials Concerning the Efficacy of Transversus Abdominis Plane Block for Pain Control After Laparoscopic Cholecystectomy. Front. Surg. 2021, 8, 700318. [Google Scholar] [CrossRef]
- Zewdu, D.; Tantu, T.; Eanga, S.; Tilahun, T. Analgesic efficacy of erector spinae plane block versus transversus abdominis plane block for laparoscopic cholecystectomy: A systematic review and meta-analysis of randomized controlled trial. Front. Med. 2024, 11, 1399253. [Google Scholar] [CrossRef]
- Kamel, A.A.F.; Amin, O.A.I.; Ibrahem, M.A.M. Bilateral Ultrasound-Guided Erector Spinae Plane Block Versus Transversus Abdominis Plane Block on Postoperative Analgesia after Total Abdominal Hysterectomy. Pain. Physician 2020, 23, 375–382. [Google Scholar] [CrossRef]
- Qian, L.; Hu, N.Q.; Shen, Q.H.; Ni, K. Comparison of the efficiency of ultrasound-guided ESPB and TAPB on postoperative analgesia: A system review and meta-analysis. Front. Med. 2025, 12, 1595778. [Google Scholar] [CrossRef] [PubMed]
- Mehmet Selim, Ç.; Halide, S.; Erkan Cem, Ç.; Onur, K.; Sedat, H.; Senem, U. Efficacy of Unilateral External Oblique Intercostal Fascial Plane Block Versus Subcostal TAP Block in Laparoscopic Cholecystectomy: Randomized, Prospective Study. Surg. Innov. 2024, 31, 381–388. [Google Scholar] [CrossRef]
- Gökduman, H.C.; Abdullah, T.; Enişte, İ.A.; Canbaz, M.; Gümüş-Özcan, F. Erector spinae plane block as a rescue therapy in following cholecystectomy: A historical cohort study. Cir. Cir. 2024, 92, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Nalbant, B.; Donmez, A.; Altinsoy, S.; Akelma, F.K. Efficacy of subcostal TAP block, ESP block, and trocar site local anesthetic infiltration in elective LC: A randomized trial. Medicine 2025, 104, e43607. [Google Scholar] [CrossRef]
- Ortiz, J.; Suliburk, J.W.; Wu, K.; Bailard, N.S.; Mason, C.; Minard, C.G.; Palvadi, R.R. Bilateral transversus abdominis plane block does not decrease postoperative pain after laparoscopic cholecystectomy when compared with local anesthetic infiltration of trocar insertion sites. Reg. Anesth. Pain. Med. 2012, 37, 188–192. [Google Scholar] [CrossRef]
- Uzunay, N.T.; Mingir, T.; Erginoz, E.; Karakas, D.O.; Kose, E. Comparison of laparoscopic-guided versus ultrasound-guided TAP block in laparoscopic cholecystectomy. Cir. Cir. 2024, 92, 174–180. [Google Scholar] [CrossRef]
- Stasiowski, M.; Missir, A.; Pluta, A.; Szumera, I.; Stasiak, M.; Szopa, W.; Błaszczyk, B.; Możdżyński, B.; Majchrzak, K.; Tymowski, M.; et al. Influence of infiltration anaesthesia on perioperative outcomes following lumbar discectomy under surgical pleth index-guided general anaesthesia: A preliminary report from a randomised controlled prospective trial. Adv. Med. Sci. 2020, 65, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Baral, B.; Poudel, P.R. Comparison of analgesic efficacy of ultrasound-guided subcostal TAP block with port-site infiltration following laparoscopic cholecystectomy. J. Nepal. Health Res. Counc. 2019, 16, 457–461. [Google Scholar] [CrossRef]
- Yang, H.M.; Choi, Y.J.; Kwon, H.J.; O, J.; Cho, T.H.; Kim, S.H. Comparison of injectate spread and nerve involvement between retrolaminar and erector spinae plane blocks in the thoracic region: A cadaveric study. Anaesthesia 2018, 73, 1244–1250. [Google Scholar] [CrossRef] [PubMed]
- Vidal, E.; Gimenez, H.; Forero, M.; Fajardo, M. Erector spinae plane block: A cadaver study to determine its mechanism of action. Rev. Esp. Anestesiol. Reanim. 2018, 65, 514–519. [Google Scholar] [CrossRef]
- Schwartzmann, A.; Peng, P.; Maciel, M.A.; Forero, M. Mechanism of the erector spinae plane block: Insights from a magnetic resonance imaging study. Can. J. Anaesth. 2018, 65, 1165–1166. [Google Scholar] [CrossRef]
- Rahimzadeh, P.; Faiz, S.H.R.; Salehi, S.; Imani, F.; Mueller, A.L.; Sabouri, A.S. Unilateral right-sided ultrasound-guided erector spinae plane block for post-laparoscopic cholecystectomy analgesia: A randomized control trial. Anesth. Pain. Med. 2022, 12, e132152. [Google Scholar] [CrossRef]
- Herrador-Benito, J.; Páramo-Zunzunegui, J.; Rodríguez-Caravaca, G.; Durán-Poveda, M. Pre-incisional local infiltration with levobupivacaine in laparoscopic cholecystectomy: A randomized and clinical trial. Cir. Cir. 2024, 92, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Rahimzadeh, P.; Faiz, S.H.R.; Latifi-Naibin, K.; Alimian, M. A Comparison of effect of preemptive versus postoperative use of ultrasound-guided bilateral transversus abdominis plane (TAP) block on pain relief after laparoscopic cholecystectomy. Sci. Rep. 2022, 12, 623. [Google Scholar] [CrossRef]
- Suseela, I.; Anandan, K.; Aravind, A.; Kaniyil, S. Comparison of ultrasound-guided bilateral subcostal transversus abdominis plane block and port-site infiltration with bupivacaine in laparoscopic cholecystectomy. Indian. J. Anaesth. 2018, 62, 497–501. [Google Scholar] [CrossRef]
- Balan, C.; Bubenek-Turconi, S.-I.; Tomescu, D.R.; Valeanu, L. Ultrasound-Guided Regional Anesthesia–Current Strategies for Enhanced Recovery after Cardiac Surgery. Medicina 2021, 57, 312. [Google Scholar] [CrossRef]
- Koo, C.H.; Hwang, J.Y.; Shin, H.J.; Ryu, J.H. The Effects of Erector Spinae Plane Block in Terms of Postoperative Analgesia in Patients Undergoing Laparoscopic Cholecystectomy: A Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2020, 9, 2928. [Google Scholar] [CrossRef] [PubMed]
- Saleem, S.Z.; Akhtar, S.M.M.; Fareed, A.; Shaik, A.A.; Asghar, M.S. Redefining pain management: Investigating the efficacy and safety of erector spinae plane block and oblique subcostal transversus abdominis plane block in laparoscopic cholecystectomy—A meta analysis of randomized controlled trials. BMC Anesthesiol. 2025, 25, 182. [Google Scholar] [CrossRef]
- Yang, X.; Zhang, Y.; Chen, Y.; Xu, M.; Lei, X.; Fu, Q. Analgesic effect of erector spinae plane block in adults undergoing laparoscopic cholecystectomy: A systematic review and meta-analysis of randomized controlled trials. BMC Anesthesiol. 2023, 23, 7. [Google Scholar] [CrossRef] [PubMed]
- Kahveci, M.; Abut, F.Y.Ç.; Erdem, G. Impact of Ultrasonography-Guided Transversus Abdominis Plane Block and Local Anesthetic Infiltration in the Surgical Field on Postoperative Analgesic Requirements for Laparoscopic Cholecystectomy Procedures. Istanbul Med. J. 2024, 25, 269–273. [Google Scholar] [CrossRef]
- Vrsajkov, V.; Mančić, N.; Mihajlović, D.; Milićević, S.T.; Uvelin, A.; Vrsajkov, J.P. Subcostal transversus abdominis plane block can improve analgesia after laparoscopic cholecystectomy. Braz. J. Anesthesiol. 2018, 68, 149–153. [Google Scholar] [CrossRef]
- Chen, H.; Li, J.; Zuo, J.; Zhang, X. Comparison of analgesic effects between erector spinae and transversus abdominis plane blocks in patients undergoing laparoscopic cholecystectomy. Pak. J. Med. Sci. 2024, 40 Pt 2, 415–420. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).