
Pulsed Radiofrequency as a Standalone Treatment for Adhesive Capsulitis


 , and
, and 
{kind=link}
{kind=link}
Abstract
1. Introduction
Adhesive Capsulitis
2. Case Report
2.1. Patient’s Characteristics
2.2. Pulsed Radiofrequency Treatment
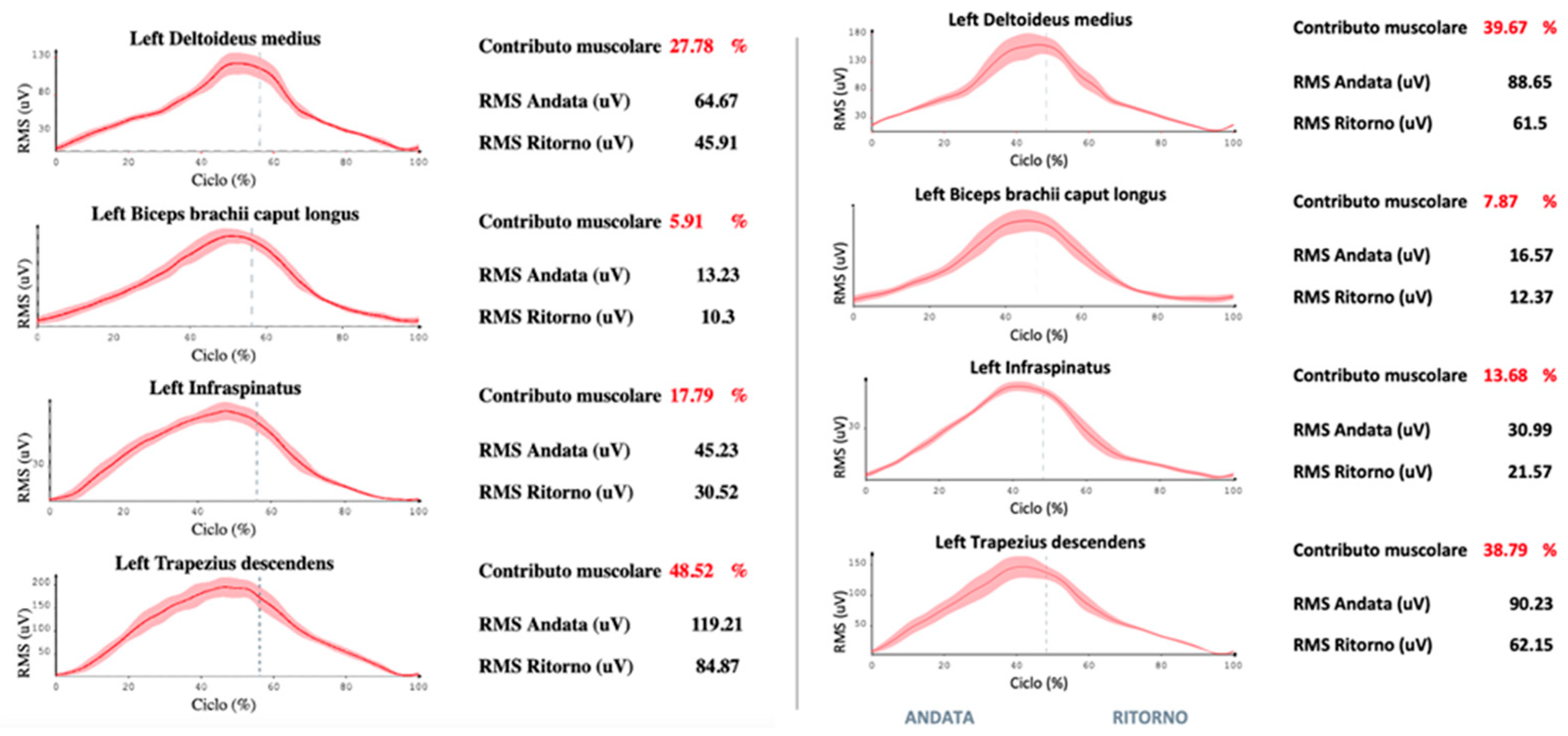
2.3. Kinematics Analysis
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Redler, L.H.; Dennis, E.R. Treatment of adhesive capsulitis of the shoulder. J. Am. Acad. Orthop. Surg. 2019, 27, e544. [Google Scholar] [CrossRef]
- Vittori, A.; Cascella, M.; Petrucci, E.; Cortegiani, A.; Bignami, E.G.; Innamorato, M.A.; Cuomo, A.; Torrano, V.; Petrini, F.; Giarratano, A.; et al. Strategies to Build and Maintain Competence in Pain Management: Insights from a SIAARTI Survey on Educational Needs among Italian Anesthesiologists. Pain Pract. 2023, 23, 501–510. [Google Scholar] [CrossRef] [PubMed]
- Thong, I.S.K.; Jensen, M.P.; Miró, J.; Tan, G. The Validity of Pain Intensity Measures: What Do the NRS, VAS, VRS, and FPS-R Measure? Scand. J. Pain 2018, 18, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Stucki, G.; Pollock, A.; Engkasan, J.P.; Selb, M. How to Use the International Classification of Functioning, Disability and Health as a Reference System for Comparative Evaluation and Standardized Reporting of Rehabilitation Interventions. Eur. J. Phys. Rehabil. Med. 2019, 55, 384–394. [Google Scholar] [CrossRef] [PubMed]
- Gigliuto, C.; De Gregori, M.; Malafoglia, V.; Raffaeli, W.; Compagnone, C.; Visai, L.; Petrini, P.; Avanzini, M.A.; Muscoli, C.; Viganò, J.; et al. Pain Assessment in Animal Models: Do We Need Further Studies? J. Pain Res. 2014, 7, 227–236. [Google Scholar] [CrossRef]
- Marchetti, G.; Vittori, A.; Mascilini, I.; Francia, E.; Picardo, S.G. Acupuncture for Pain Management in Pediatric Psoriatic Arthritis: A Case Report. Acupunct. Med. 2020, 38, 440–442. [Google Scholar] [CrossRef]
- Bongiorno, G.; Biancuzzi, H.; Dal Mas, F.; Bednarova, R.; Miceli, L. The Rehabilitation Tailor: Applying Personalized Medicine to Cancer Recovery. Front. Glob. Womens Health 2022, 3, 914302. [Google Scholar] [CrossRef]
- Taylor, A.M.; Phillips, K.; Patel, K.V.; Turk, D.C.; Dworkin, R.H.; Beaton, D.; Clauw, D.J.; Gignac, M.A.M.; Markman, J.D.; Williams, D.A.; et al. Assessment of Physical Function and Participation in Chronic Pain Clinical Trials: IMMPACT/OMERACT Recommendations. Pain 2016, 157, 1836–1850. [Google Scholar] [CrossRef]
- Gerdle, B.; Molander, P.; Stenberg, G.; Stålnacke, B.-M.; Enthoven, P. Weak Outcome Predictors of Multimodal Rehabilitation at One-Year Follow-up in Patients with Chronic Pain-a Practice Based Evidence Study from Two SQRP Centres. BMC Musculoskelet. Disord. 2016, 17, 490. [Google Scholar] [CrossRef]
- Naranjo-Hernández, D.; Reina-Tosina, J.; Roa, L.M. Sensor Technologies to Manage the Physiological Traits of Chronic Pain: A Review. Sensors 2020, 20, 365. [Google Scholar] [CrossRef]
- Bednarova, R.; Biancuzzi, H.; Rizzardo, A.; Dal Mas, F.; Massaro, M.; Cobianchi, L.; Barcellini, A.; Orlandi, E.; Miceli, L. Cancer Rehabilitation and Physical Activity: The “Oncology in Motion” Project. J. Cancer Educ. 2022, 37, 1066–1068. [Google Scholar] [CrossRef]
- Cobianchi, L.; Dal Mas, F.; Massaro, M.; Bednarova, R.; Biancuzzi, H.; Filisetti, C.; Barcellini, A.; Orlandi, E.; Miceli, L.; Angelos, P. Hand in hand: A multistakeholder approach for co-production of surgical care. Am. J. Surg. 2021, 223, 214–215. [Google Scholar] [CrossRef]
- Candela, V.; Giannicola, G.; Passaretti, D.; Venditto, T.; Gumina, S. Adhesive Capsulitis of the Shoulder: Pain Intensity and Distribution. Musculoskelet. Surg. 2017, 101, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Stout, A.; Friedly, J.; Standaert, C.J. Systemic Absorption and Side Effects of Locally Injected Glucocorticoids. PM&R 2019, 1, 409–419. [Google Scholar] [CrossRef]
- Wu, Y.-T.; Ho, C.-W.; Chen, Y.-L.; Li, T.-Y.; Lee, K.-C.; Chen, L.-C. Ultrasound-Guided Pulsed Radiofrequency Stimulation of the Suprascapular Nerve for Adhesive Capsulitis: A Prospective, Randomized, Controlled Trial. Anesth. Analg. 2014, 119, 686–692. [Google Scholar] [CrossRef] [PubMed]
- Beirens, B.J.H.; Bossuyt, F.M.; Arnet, U.; van der Woude, L.H.V.; de Vries, W.H.K. Shoulder Pain Is Associated with Rate of Rise and Jerk of the Applied Forces During Wheelchair Propulsion in Individuals with Paraplegic Spinal Cord Injury. Arch. Phys. Med. Rehabil. 2021, 102, 856–864. [Google Scholar] [CrossRef]
- Petrucci, E.; Vittori, A.; Cascella, M.; Vergallo, A.; Fiore, G.; Luciani, A.; Pizzi, B.; Degan, G.; Fineschi, V.; Marinangeli, F. Litigation in Anesthesia and Intensive Care Units: An Italian Retrospective Study. Healthcare 2021, 9, 1012. [Google Scholar] [CrossRef]
- Biancuzzi, H.; Dal Mas, F. La valutazione economica e delle performance nell’e-health: Una revisione della letteratura. Politiche Sanit. 2023, 24, 24–36. [Google Scholar] [CrossRef]
- Biancuzzi, H.; Dal Mas, F.; Bidoli, C.; Pegoraro, V.; Zantedeschi, M.; Negro, P.A.; Campostrini, S.; Cobianchi, L. Economic and Performance Evaluation of E-Health before and after the Pandemic Era: A Literature Review and Future Perspectives. Int. J. Environ. Res. Public Health 2023, 20, 4038. [Google Scholar] [CrossRef]
- Dal Mas, F.; Biancuzzi, H.; Bednarova, R.; Miceli, L. A Gender Perspective on Telemedicine—Early Results from the National Cancer Institute of Aviano Experience. In Organizational Resilience and Female Entrepreneurship During Crises: Emerging Evidence and Future Agenda; Springer: Cham, Switzerland, 2022; pp. 73–78. ISBN 978-3-030-89411-5. [Google Scholar]
- Miceli, L.; Dal Mas, F.; Biancuzzi, H.; Bednarova, R.; Rizzardo, A.; Cobianchi, L.; Holbmoe, E.S. Doctor@Home: Through a Telemedicine Co-production and Co-learning Journey. J. Cancer Educ. 2022, 37, 1236–1238. [Google Scholar] [CrossRef]
- Dal Mas, F.; Biancuzzi, H.; Massaro, M.; Miceli, L. Adopting a knowledge translation approach in healthcare co-production: A case study. Manag. Decis. 2020, 58, 1841–1862. [Google Scholar] [CrossRef]
- Dal Mas, F.; Biancuzzi, H.; Massaro, M.; Barcellini, A.; Cobianchi, L.; Miceli, L. Knowledge Translation in Oncology. A Case Study. Electron. J. Knowl. Manag. 2020, 18, 212–223. [Google Scholar] [CrossRef]
- Bhaskar, S.; Bradley, S.; Chattu, V.K.; Adisesh, A.; Nurtazina, A.; Kyrykbayeva, S.; Sakhamuri, S.; Yaya, S.; Sunil, T.; Thomas, P.; et al. Telemedicine Across the Globe-Position Paper From the COVID-19 Pandemic Health System Resilience PROGRAM (REPROGRAM) International Consortium (Part 1). Front. Public Health 2020, 8, 556720. [Google Scholar] [CrossRef] [PubMed]
- Cascella, M.; Marinangeli, F.; Vittori, A.; Scala, C.; Piccinini, M.; Braga, A.; Miceli, L.; Vellucci, R. Open Issues and Practical Suggestions for Telemedicine in Chronic Pain. Int. J. Environ. Res. Public Health 2021, 18, 12416. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bongiorno, G.; Bednarova, R.; Biancuzzi, H.; Dal Mas, F.; Rizzardo, A.; Tomasi, A.; Vigni, G.E.; Miceli, L. Pulsed Radiofrequency as a Standalone Treatment for Adhesive Capsulitis. Surgeries 2023, 4, 335-341. https://doi.org/10.3390/surgeries4030034
Bongiorno G, Bednarova R, Biancuzzi H, Dal Mas F, Rizzardo A, Tomasi A, Vigni GE, Miceli L. Pulsed Radiofrequency as a Standalone Treatment for Adhesive Capsulitis. Surgeries. 2023; 4(3):335-341. https://doi.org/10.3390/surgeries4030034
Chicago/Turabian StyleBongiorno, Giulia, Rym Bednarova, Helena Biancuzzi, Francesca Dal Mas, Alessandro Rizzardo, Andrea Tomasi, Giulio Edoardo Vigni, and Luca Miceli. 2023. "Pulsed Radiofrequency as a Standalone Treatment for Adhesive Capsulitis" Surgeries 4, no. 3: 335-341. https://doi.org/10.3390/surgeries4030034
APA StyleBongiorno, G., Bednarova, R., Biancuzzi, H., Dal Mas, F., Rizzardo, A., Tomasi, A., Vigni, G. E., & Miceli, L. (2023). Pulsed Radiofrequency as a Standalone Treatment for Adhesive Capsulitis. Surgeries, 4(3), 335-341. https://doi.org/10.3390/surgeries4030034