
A Review on Tactile Displays for Conventional Laparoscopic Surgery



Abstract
1. Introduction
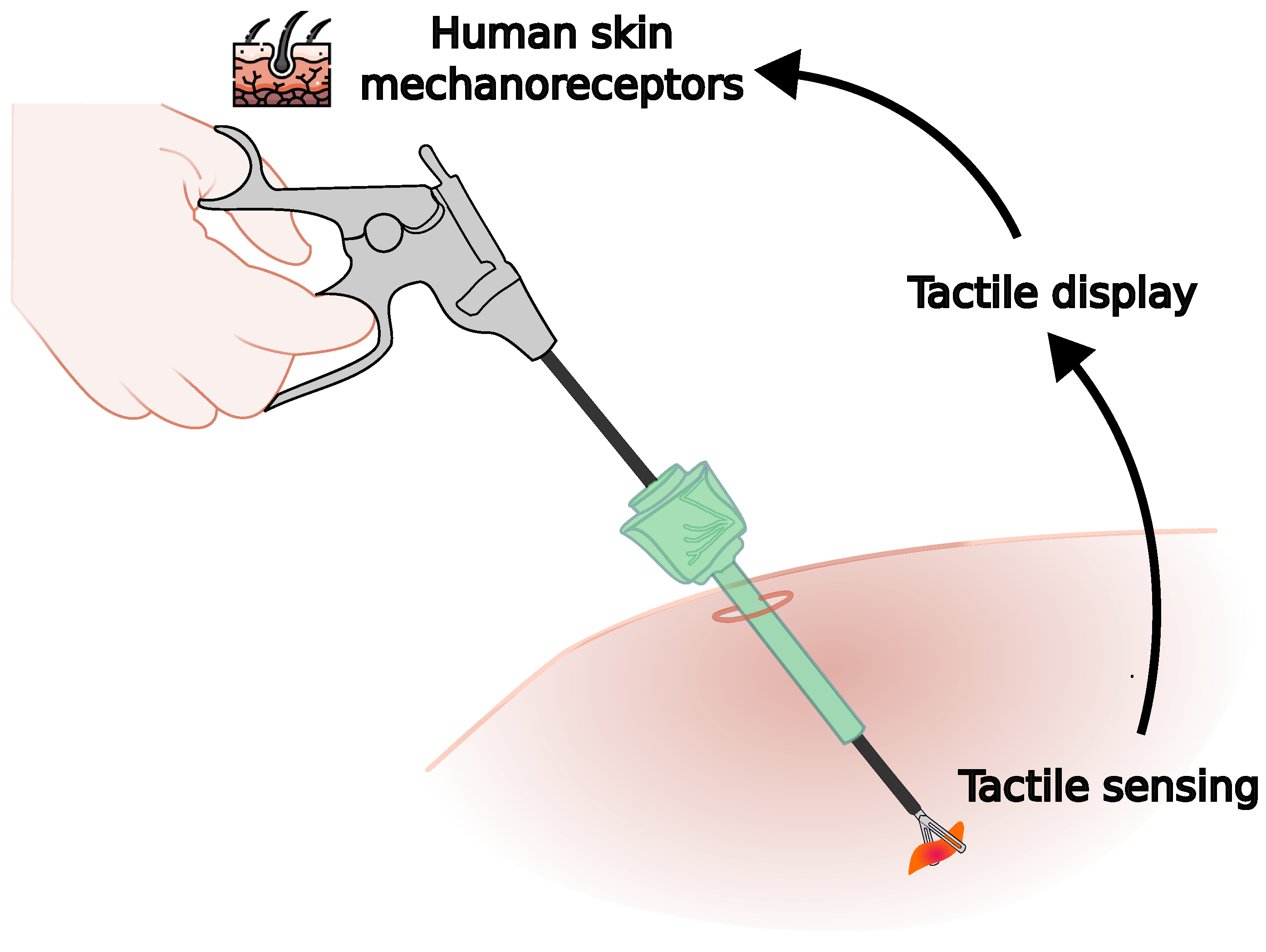
1.1. Haptic Feedback in Minimally Invasive Surgery
1.2. Related Surveys
2. Materials and Methods
2.1. Research Question
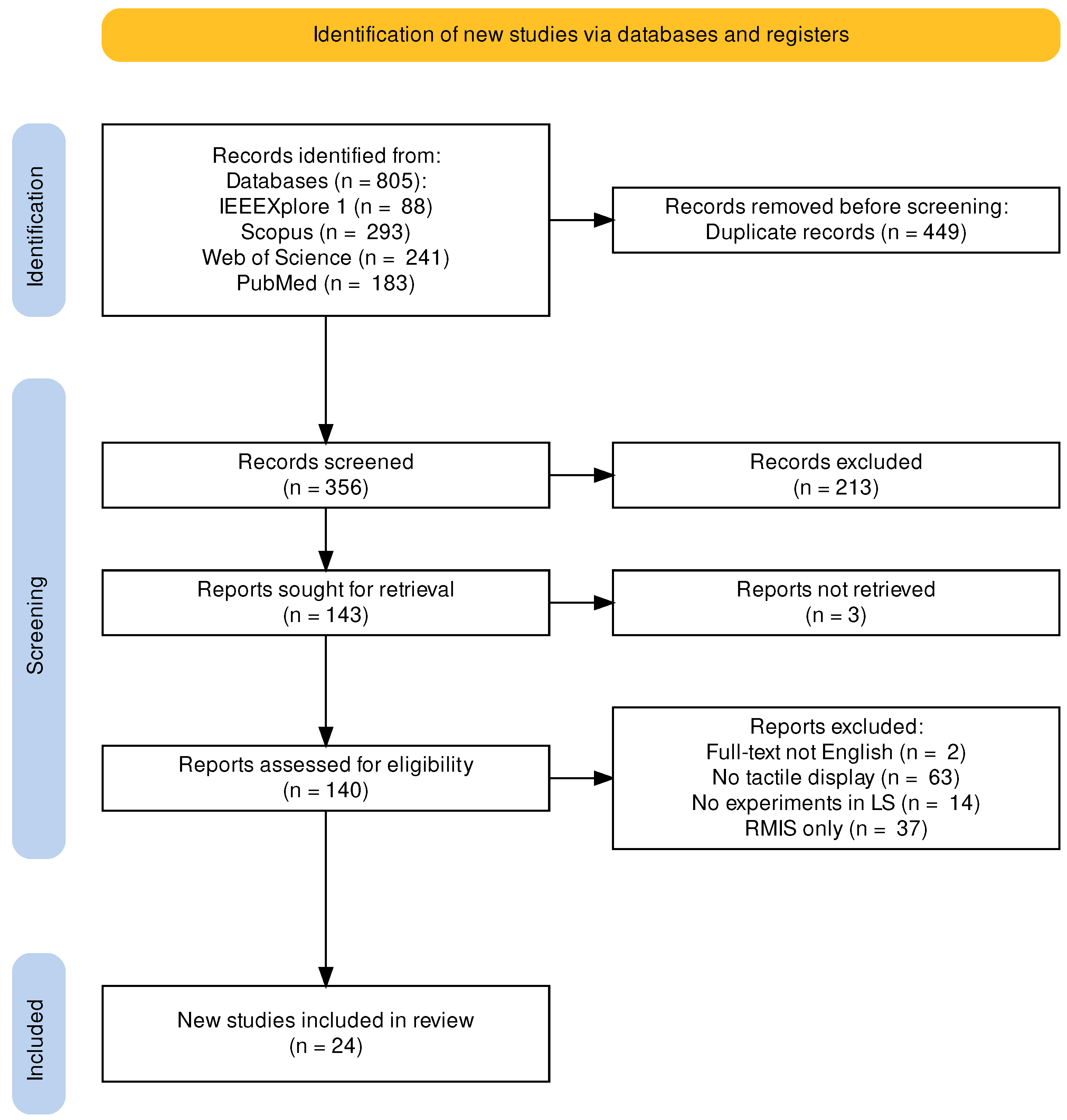
2.2. Search Methodology and Systematic Review
2.3. Study Selection and Inclusion Criteria
3. Results
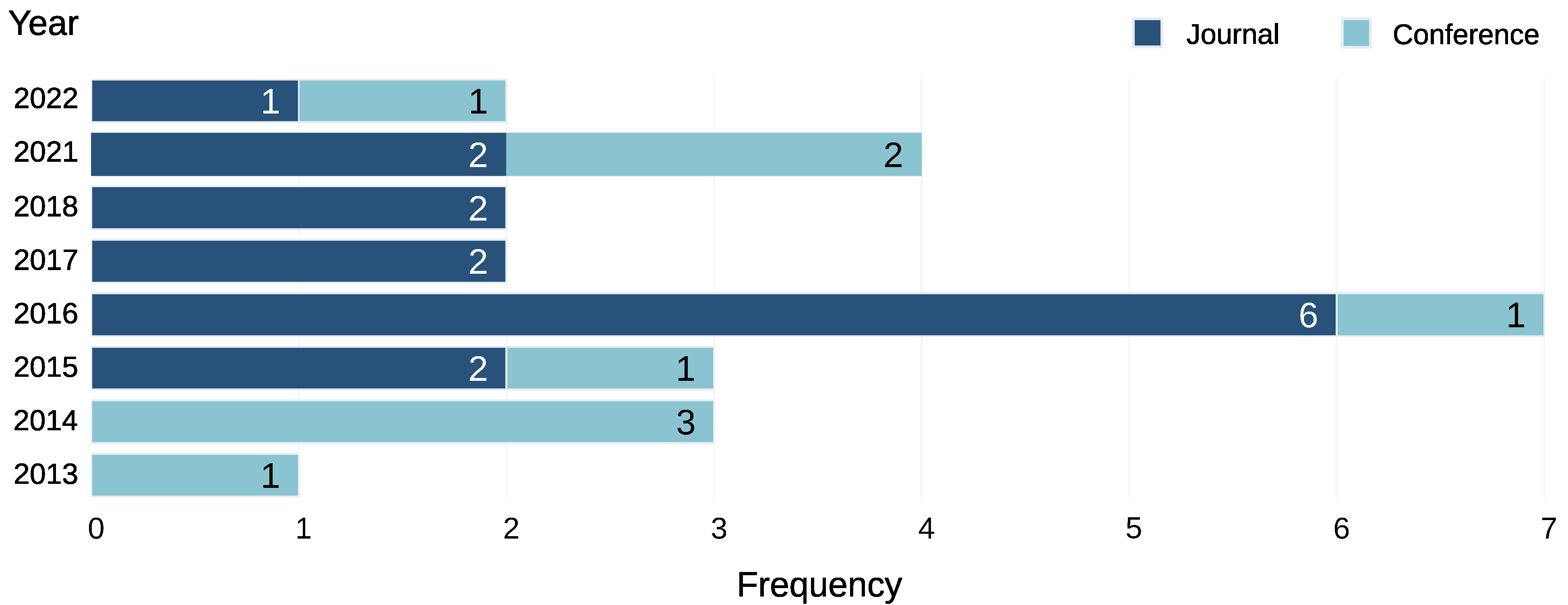
3.1. Descriptive Analysis of the Reviewed Studies
3.2. Tactile Display Modalities
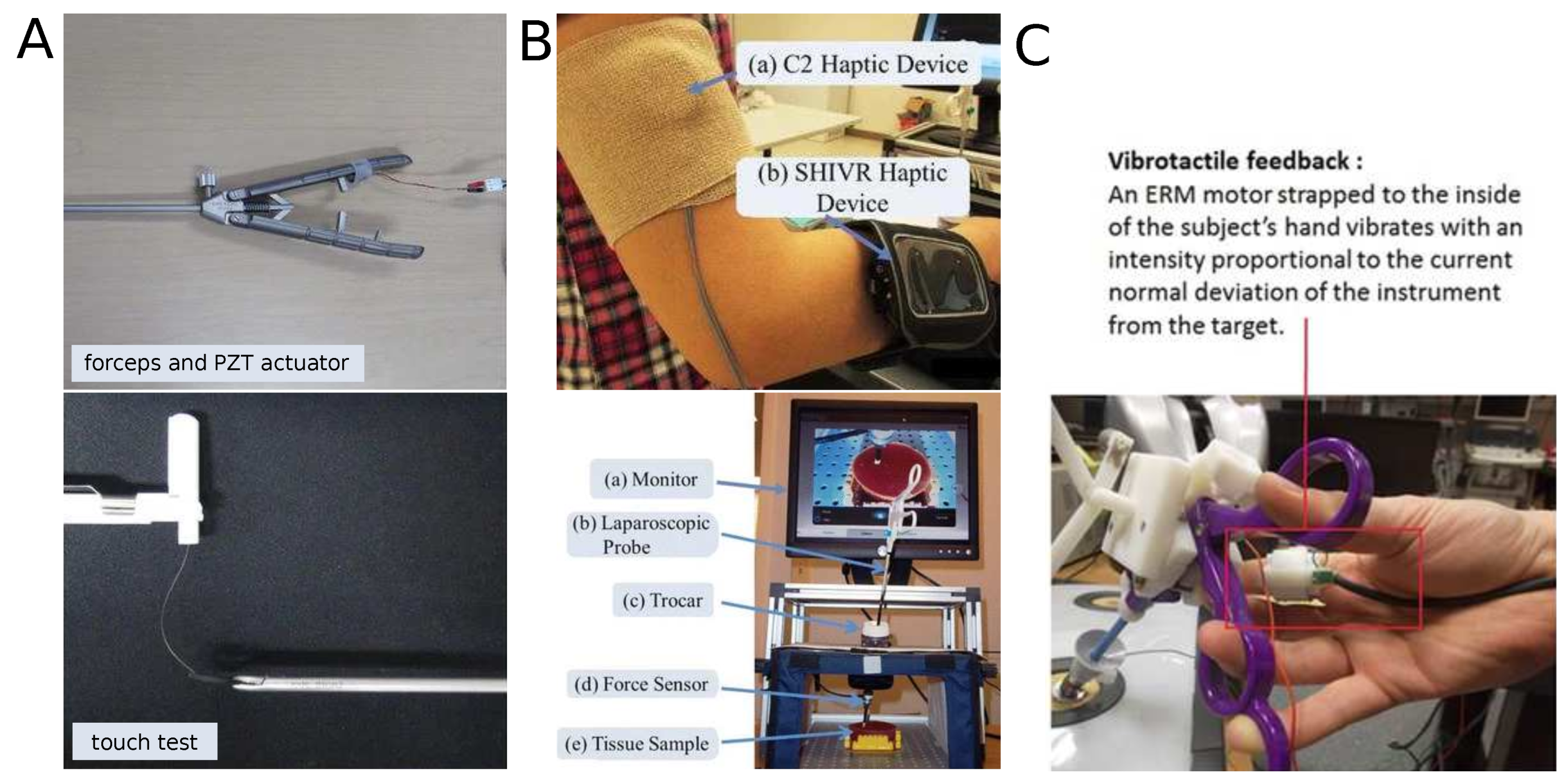
- Skin tactile displays: Skin deformation is used. Three modalities for tactile feedback display are considered: vibrotactile devices, skin indentation devices, and grip feedback devices,
- Non-contact tactile displays: Propose the use of visualizations of tactile information (e.g., pressure maps). Some also include a visual representation of the interaction forces.
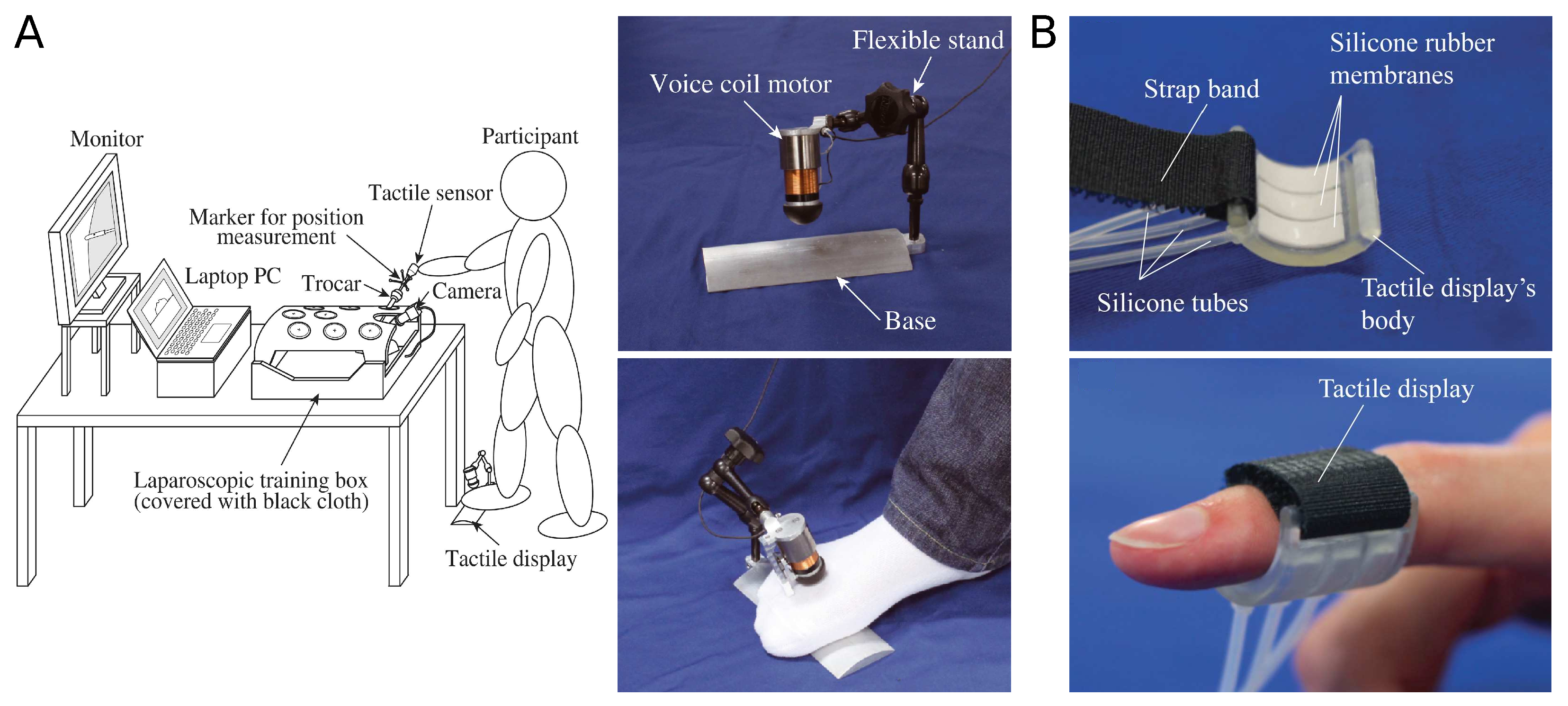
3.3. Skin Tactile Displays
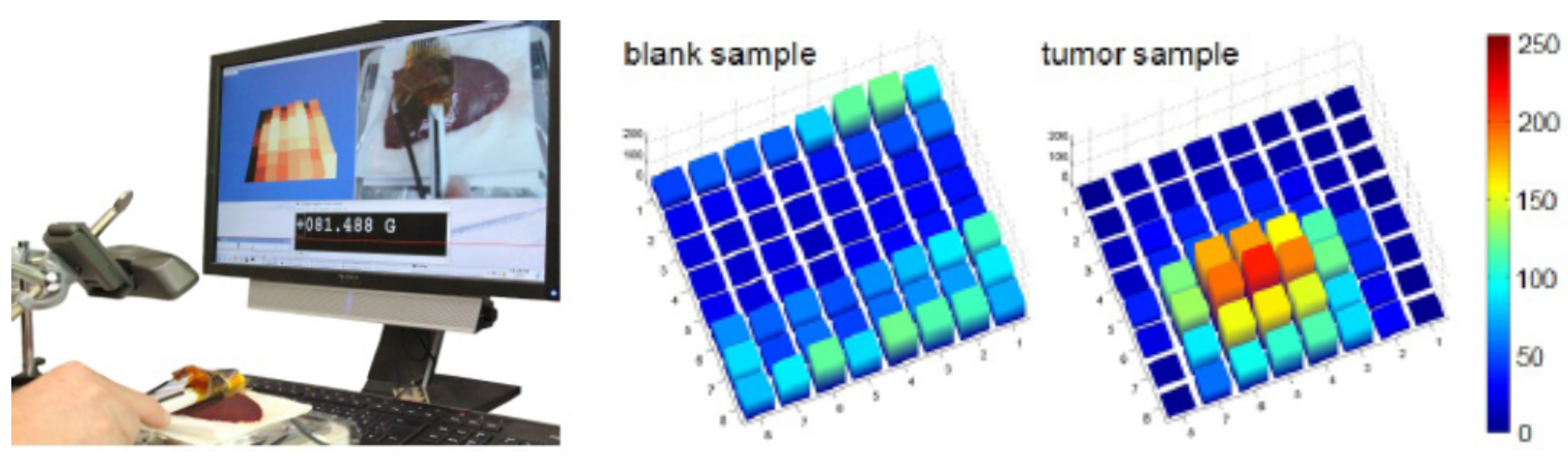
3.4. Non-Contact Tactile Displays
4. Discussion
4.1. Applications in Laparoscopic Surgery
4.1.1. Palpation
4.1.2. Tissue manipulation
4.1.3. Suturing
4.1.4. Guidance
4.2. Challenges in the Development of Tactile Displays
- Transparency: The tactile display should provide tactile information to the surgeon in a natural and seamless way to avoid increasing the surgeon’s cognitive workload.
- Compactability: Size of the tactile display must be able to be included in the surgical workspace without constraining the surgeon’s movement.
- Weight: The weight of the display should not affect the manipulation of the surgical tool and should not increase the surgeon’s effort. The selection of external actuators and its location are critical to reduce the overall weight of the device.
- Time delay: The time delay between tactile sensing and tactile feedback rendering reduces its effectiveness.
- Safety: Forces generated must be kept within a safe range to avoid injuring the surgeon.
- Adjustable: Each user requires different levels of stimulation, and adjustable perception is desirable.
- Sterilizable: Tactile displays mounted close to the surgical workspace (e.g., surgical tool or surgeon’s hands) must be sterilized.
- Reusability: To reduce costs, surgical instruments are commonly reused multiple times before being discarded. In the same way, tactile displays should be designed to last for many uses. Single-use devices could eliminate the need for cleaning or sterilization but increase costs and have a high environmental impact.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sieber, A.; Houston, K.; Woegerer, C.; Enoksson, P.; Menciassi, A.; Dario, P. Sensorized Tools for Haptic Force Feedback in Computer Assisted Surgery. In Haptics Rendering and Applications; Saddik, A.E., Ed.; IntechOpen: Rijeka, Croatia, 2012; Chapter 7. [Google Scholar] [CrossRef][Green Version]
- Xin, H.; Zelek, J.; Carnahan, H. Laparoscopic surgery, perceptual limitations and force: A review. In Proceedings of the First Canadian Student Conference on Biomedical Computing, Waterloo, ON, Canada, 2006; Volume 144. [Google Scholar]
- Freschi, C.; Ferrari, V.; Melfi, F.; Ferrari, M.; Mosca, F.; Cuschieri, A. Technical review of the da Vinci surgical telemanipulator. Int. J. Med. Robot. Comput. Assist. Surg. 2013, 9, 396–406. [Google Scholar] [CrossRef] [PubMed]
- DiMaio, S.; Hanuschik, M.; Kreaden, U. The da Vinci surgical system. In Surgical Robotics; Springer: Berlin/Heidelberg, Germany, 2011; pp. 199–217. [Google Scholar]
- Colan, J.; Nakanishi, J.; Aoyama, T.; Hasegawa, Y. A Cooperative Human-Robot Interface for Constrained Manipulation in Robot-Assisted Endonasal Surgery. Appl. Sci. 2020, 10, 4809. [Google Scholar] [CrossRef]
- Colan, J.; Nakanishi, J.; Aoyama, T.; Hasegawa, Y. Optimization-Based Constrained Trajectory Generation for Robot-Assisted Stitching in Endonasal Surgery. Robotics 2021, 10, 27. [Google Scholar] [CrossRef]
- Koyama, Y.; Marinho, M.M.; Mitsuishi, M.; Harada, K. Autonomous Coordinated Control of the Light Guide for Positioning in Vitreoretinal Surgery. IEEE Trans. Med. Robot. Bionics 2022, 4, 156–171. [Google Scholar] [CrossRef]
- Okamura, A.M. Haptics in robot-assisted minimally invasive surgery. In The Encyclopedia of Medical Robotics; Chapter 11; World Scientific: Singapore, 2019; pp. 317–339. [Google Scholar] [CrossRef]
- See, A.R.; Choco, J.A.G.; Chandramohan, K. Touch, Texture and Haptic Feedback: A Review on How We Feel the World around Us. Appl. Sci. 2022, 12, 4686. [Google Scholar] [CrossRef]
- Schostek, S.; Schurr, M.O.; Buess, G.F. Review on aspects of artificial tactile feedback in laparoscopic surgery. Med. Eng. Phys. 2009, 31, 887–898. [Google Scholar] [CrossRef]
- Amirabdollahian, F.; Livatino, S.; Vahedi, B.; Gudipati, R.; Sheen, P.; Gawrie-Mohan, S.; Vasdev, N. Prevalence of haptic feedback in robot-mediated surgery: A systematic review of literature. J. Robot. Surg. 2018, 12, 11–25. [Google Scholar] [CrossRef] [PubMed]
- Westebring-van der Putten, E.P.; Goossens, R.H.; Jakimowicz, J.J.; Dankelman, J. Haptics in minimally invasive surgery—A review. Minim. Invasive Ther. Allied Technol. 2008, 17, 3–16. [Google Scholar] [CrossRef]
- Hadi Hosseinabadi, A.H.; Salcudean, S.E. Force sensing in robot-assisted keyhole endoscopy: A systematic survey. Int. J. Robot. Res. 2022, 41, 136–162. [Google Scholar] [CrossRef]
- Eltaib, M.; Hewit, J. Tactile sensing technology for minimal access surgery—A review. Mechatronics 2003, 13, 1163–1177. [Google Scholar] [CrossRef]
- Eriksen, M.B.; Frandsen, T.F. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: A systematic review. J. Med. Libr. Assoc. 2018, 106, 420. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Othman, W.; Lai, Z.H.A.; Abril, C.; Barajas-Gamboa, J.S.; Corcelles, R.; Kroh, M.; Qasaimeh, M.A. Tactile Sensing for Minimally Invasive Surgery: Conventional Methods and Potential Emerging Tactile Technologies. Front. Robot. AI 2022, 8, 376. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Nagai, T.; Sakaguchi, M.; Fujiwara, M.; Sano, A. Tactile sensing system including bidirectionality and enhancement of haptic perception by tactile feedback to distant part. In Proceedings of the 2013 World Haptics Conference (WHC), Daejeon, Republic of Korea, 14–17 April 2013; pp. 145–150. [Google Scholar]
- Tanaka, Y.; Nagai, T.; Fujiwara, M.; Sano, A. Lump detection with tactile sensing system including haptic bidirectionality. In Proceedings of the 2014 World Automation Congress (WAC), Waikoloa, HI, USA, 3–7 August 2014; pp. 77–82. [Google Scholar]
- Kurita, Y.; Sueda, Y.; Ishikawa, T.; Hattori, M.; Sawada, H.; Egi, H.; Ohdan, H.; Ueda, J.; Tsuji, T. Surgical grasping forceps with enhanced sensorimotor capability via the stochastic resonance effect. IEEE ASME Trans. Mechatron. 2016, 21, 2624–2634. [Google Scholar] [CrossRef]
- Sawada, H.; Egi, H.; Hattori, M.; Suzuki, T.; Mukai, S.; Kurita, Y.; Yasui, W.; Ohdan, H. Stochastic resonance enhanced tactile feedback in laparoscopic surgery. Surg. Endosc. 2015, 29, 3811–3818. [Google Scholar] [CrossRef] [PubMed]
- Hoskins, R.; Wang, J.; Cao, C.G.L. Use of stochastic resonance methods for improving laparoscopic surgery performance. Surg. Endosc. 2016, 30, 4214–4219. [Google Scholar] [CrossRef] [PubMed]
- Howard, T.; Szewczyk, J. Visuo-haptic feedback for 1D Guidance in laparoscopic surgery. In Proceedings of the 5th IEEE RAS/EMBS International Conference on Biomedical Robotics and Biomechatronics, Sao Paulo, Brazil, 12–15 August 2014; pp. 58–65. [Google Scholar]
- Howard, T.; Szewczyk, J. Assisting control of forces in laparoscopy using tactile and visual sensory substitution. In New Trends in Medical and Service Robots; Springer: Berlin/Heidelberg, Germany, 2016; pp. 151–164. [Google Scholar]
- Howard, T.; Szewczyk, J. Improving precision in navigating laparoscopic surgery instruments toward a planar target using haptic and visual feedback. Front. Robot. AI 2016, 3, 37. [Google Scholar] [CrossRef]
- Tanaka, Y.; Aragaki, S.; Fukuda, T.; Fujiwara, M.; Sano, A. A study on tactile display for haptic sensing system with sensory feedback for laparoscopic surgery. In Proceedings of the 2014 International Symposium on Micro-NanoMechatronics and Human Science (MHS), Nagoya, Japan, 10–12 November 2014; p. 1. [Google Scholar]
- Tanaka, Y.; Sano, A. Pervasive Haptics: Simple Tactile Technologies Utilizing Human Tactile and Haptic Characteristics; Springer: Tokyo, Japan, 2016; pp. 231–246. [Google Scholar]
- Fukuda, T.; Tanaka, Y.; Kappers, A.M.L.; Fujiwara, M.; Sano, A. Visual and tactile feedback for a direct-manipulating tactile sensor in laparoscopic palpation. Int. J. Med. Robot. Comput. Assist. Surg. 2018, 14, e1879. [Google Scholar] [CrossRef]
- Fukuda, T.; Tanaka, Y.; Kappers, A.M.L.; Fujiwara, M.; Sano, A. A Pneumatic Tactile Ring for Instantaneous Sensory Feedback in Laparoscopic Tumor Localization. IEEE Trans. Haptics 2018, 11, 485–497. [Google Scholar] [CrossRef]
- Ly, H.H.; Tanaka, Y.; Fujiwara, M. SuP-Ring: A pneumatic tactile display with substitutional representation of contact force components using normal indentation. Int. J. Med. Robot. 2021, 17, e2325. [Google Scholar] [CrossRef]
- Ly, H.H.; Tanaka, Y.; Fujiwara, M. Tumor Depth and Size Perception Using a Pneumatic Tactile Display in Laparoscopic Surgery. IEEE Access 2021, 9, 167795–167811. [Google Scholar] [CrossRef]
- Udo, T.; Ukai, T.; Tanaka, Y.; Miura, H.; Terada, Y. A sensory feedback system with pneumatic dual-structure tactile display for softness assessment during laparoscopic surgery. In Proceedings of the 2021 IEEE World Haptics Conference (WHC), Montreal, QC, Canada, 6–9 July 2021; pp. 685–690. [Google Scholar]
- Aguirre, M.E.; Kommuri, K.D.; Isbister, D.J.; Gallego, J.A. Multi-Modal Mechanism for Enhancing Haptics and Safety in Handheld Surgical Grasping. In Proceedings of the 2022 IEEE Haptics Symposium (HAPTICS), Santa Barbara, CA, USA, 21–24 March 2022; pp. 1–6. [Google Scholar]
- Wiederer, C.; Fröhlich, M.; Strohmayr, M.W. Improving tactile sensation in laparoscopic surgery by overcoming size restrictions. Curr. Dir. Biomed. Eng. 2015, 1, 135–139. [Google Scholar] [CrossRef]
- Beccani, M.; Natali, C.D.; Valdastri, P.; Obstein, K.L. Restoring Haptic Feedback in NOTES Procedures with a Novel Wireless Tissue Stiffness Probe. J. Med. Robot. Res. 2016, 1, 1650002. [Google Scholar] [CrossRef]
- Afshari, E.; Sarkhosh, H.; Najarian, S. A novel tactile probe with medical and surgical applications. Sens. Rev. 2017, 37, 404–409. [Google Scholar] [CrossRef]
- Naidu, A.S.; Escoto, A.; Fahmy, O.; Patel, R.V.; Naish, M.D. An autoclavable wireless palpation instrument for minimally invasive surgery. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 6489–6492. [Google Scholar]
- Naidu, A.S.; Patel, R.V.; Naish, M.D. Low-cost disposable tactile sensors for palpation in minimally invasive surgery. IEEE ASME Trans. Mechatron. 2017, 22, 127–137. [Google Scholar] [CrossRef]
- Escoto, A.; Bhattad, S.; Shamsil, A.; Sanches, A.; Trejos, A.L.; Naish, M.D.; Malthaner, R.A.; Patel, R.V. A multi-sensory mechatronic device for localizing tumors in minimally invasive interventions. In Proceedings of the 2015 IEEE International Conference on Robotics and Automation (ICRA), Seattle, WA, USA, 26–30 May 2015; pp. 4742–4747. [Google Scholar]
- Wang, P.; Liu, Z.; Huang, J.; Huang, X.; Chen, J.; Peng, D. Novel optical fiber tactile sensor in laparoscope for force feedback. In Proceedings of the 26th Optoelectronics and Communications Conference, Hong Kong, China, 3–7 July 2021; p. W1D.4. [Google Scholar]
- Wang, P.; Zhang, S.; Liu, Z.; Huang, Y.; Huang, J.; Huang, X.; Chen, J.; Fang, B.; Peng, D. Smart laparoscopic grasper integrated with fiber Bragg grating based tactile sensor for real-time force feedback. J. Biophotonics 2022, 15, e202100331. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Population | Conventional laparoscopic surgery | Other types of LS (e.g., robot-assisted surgery) |
| Intervention | All forms of tactile displays | - |
| Comparators | Not applicable | - |
| Outcomes | Tactile information rendering from LS tasks in ex vivo or phantom setups | Study does not include LS tasks in ex vivo or phantom setups |
| Search Strategy |
|---|
| TITLE-ABS ( (“minimally invasive” OR “laparoscop*” OR “endoscop*” OR “MIS”) AND “surg*” AND (“somatosensory” OR “tactile” OR “cutaneous” ) AND (“display” OR “feedback” OR “augmentation” OR “interface” OR “device”) ) AND PUBYEAR > 2012 |
| Authors | Date | Modality | Application | Sensor | Actuator | Feedback Location | Phantom | Ex-Vivo |
|---|---|---|---|---|---|---|---|---|
| Tanaka et al. [18,19] | 2014 | Vibrotactile | Tissue stiffness discrimination | Acoustic | Voice coil actuator | Handpalm | X | - |
| Kurita et al. [20] and Sawada et al. [21] | 2016 | Vibrotactile | Tissue stiffness discrimination and suturing | Piezoelectric | PZT actuator | Handpalm | X | X |
| Hoskings et al. [22] | 2016 | Vibrotactile | Tissue stiffness discrimination | 6-axis Force/Torque | Voice coil actuator and piezoelectric | Upperarm and forearm | X | - |
| Howard et al. [23,24,25] | 2016 | Vibrotactile | Guidance | 6-axis Force/Torque | ERM vibration motor | Handpalm | X | - |
| Tanaka et al. [26,27] | 2016 | Skin indentation | Tissue stiffness discrimination | Acoustic | Rigid tactor | Forearm | X | - |
| Fukuda et al. [28] | 2018 | Skin indentation | Tissue stiffness discrimination | Acoustic | Voice coil motor | Foot | X | - |
| Ly et al. [29,30,31] | 2021 | Skin indentation | Tissue stiffness discrimination | Acoustic | Pneumatic actuator | Fingertip | X | - |
| Udo et al. [30,31,32] | 2021 | Skin indentation | Tissue stiffness discrimination | three-axis force | Pneumatic actuator | Fingertips | X | - |
| Aguirre et al. [33] | 2022 | Grip feedback | Tissue manipulation | Sensorless | Compliant mechanism | Fingertips | X | - |
| Authors | Date | Application | Sensor Type | Visualization Parameters | Phantom | Ex-Vivo |
|---|---|---|---|---|---|---|
| Wiederer et al. [34] | 2015 | Tissue stiffness discrimination | PBCTs based sensor | 3D color-coded bar graphs indicating palpation force | - | X |
| Beccani et al. [35] | 2016 | Tissue stiffness discrimination | Pressure sensor | Endoscope position and pressure exerted over tissues | - | X |
| Afshari et al. [36] | 2017 | Tissue stiffness discrimination | Force and magnetic sensors | Interaction forces and displacements | X | X |
| Naidu et al. [37,38] and Escoto et al. [39] | 2016 | Tissue stiffness discrimination | Piezoresistive sensor | 2D pressure map and average pressure level | X | X |
| Wang et al. [40,41] | 2022 | Tissue stiffness discrimination | fiber Bragg gratings (FBG) based sensor | Gripping force from the tactile sensor | X | X |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colan, J.; Davila, A.; Hasegawa, Y. A Review on Tactile Displays for Conventional Laparoscopic Surgery. Surgeries 2022, 3, 334-346. https://doi.org/10.3390/surgeries3040036
Colan J, Davila A, Hasegawa Y. A Review on Tactile Displays for Conventional Laparoscopic Surgery. Surgeries. 2022; 3(4):334-346. https://doi.org/10.3390/surgeries3040036
Chicago/Turabian StyleColan, Jacinto, Ana Davila, and Yasuhisa Hasegawa. 2022. "A Review on Tactile Displays for Conventional Laparoscopic Surgery" Surgeries 3, no. 4: 334-346. https://doi.org/10.3390/surgeries3040036
APA StyleColan, J., Davila, A., & Hasegawa, Y. (2022). A Review on Tactile Displays for Conventional Laparoscopic Surgery. Surgeries, 3(4), 334-346. https://doi.org/10.3390/surgeries3040036