1. Introduction
Prostate cancer (PCa) is the most common malignant tumor among men in the Western world [
1]. Men with a life expectancy of at least 10 years could benefit from radical prostatectomy (RP), where the robotic approach offers the benefits of minimally invasive surgery [
2].
Delayed postoperative bleeding is a serious complication of RP, although rare [
3]. Iatrogenic pelvic pseudo-aneurysms following open, robotic or laparoscopic procedures have been rarely reported in the past. The clinical presentation of a bleeding pseudoaneurysm can be diversified [
3] and the clinical management of hemorrhage after RP has not been well-described, despite wide institutional and anecdotal experiences. Several case series have described postoperative hemorrhage management through minimally invasive exploration as well as angioembolization, although decision-making criteria or decisional algorithms have not been well established [
4]. The following case shows a misleading presentation of delayed intermittent postoperative bleeding by a pseudoaneurysm after robotic radical prostatectomy. The clinical presentation was confusing and ambiguous, with a nuanced and intermittent course of symptoms. We hope this case could help the improvement in recognizing and assessing similar cases, which rarely occur but are easily susceptible to a dangerous complication.
In the second part of this work, we propose a narrative literature review on pseudoaneurysms consequent to radical prostatectomy, analyzing their clinical features, management, functional consequences and possible future perspectives.
2. Case Presentation
2.1. Patient Information
A 66-year-old patient underwent robotic-assisted-radical-prostatectomy (RARP) with a bilateral interfascial nerve-sparing approach and standard pelvic lymph node dissection (sPNLD) due to a GS 4 + 3 pT2 N0 R0 M0 prostate cancer (PCa). Preoperatory PSA was 9.250 ng/mL, and staging CT imaging and bone-scan were not suggestive for metastasis. Prostate volume at multiparametric Magnetic Resonance Imaging (mp-MRI) was 38 cc. Patient did not experience neither previous pelvic surgery nor radiotherapy nor androgen deprivation therapy treatment.
Concerning micturition and erectile status, the patient had an IPSS score of 10/25, QoL 4 [
5] and IIEF-5 score 13/25 [
6]. His clinical history included benign prostatic hyperplasia, hypertension, smoking (540 pack/year), grade-I obesity and a previous inferior ST-elevation myocardial infarction (STEMI) 14 years before RARP was successfully treated with thrombolysis. During the whole cardiological follow up, no heart symptoms were reported.
Four years before RARP, a coronary CT showed calcified plaques involving the anterior interventricular (IVA I) ca. 25% and circumflex artery (Cx) ca. 25%; contextual echocardiography evidenced ejection fraction 65% with a 42 mm aortic ectasia and low aortic insufficiency.
2.2. Clinical Findings and Diagnostic Assessment
In the immediate post-operative period after RARP, the patient experienced anemia, with a hemoglobin decrease from 10.2 to 8.3 mg/dL; subsequently, he was transfused two-pockets of red blood cells, leading to a restorage of preoperative hemoglobin levels, then he was discharged five days postoperatively. Convalescence period was free of complications.
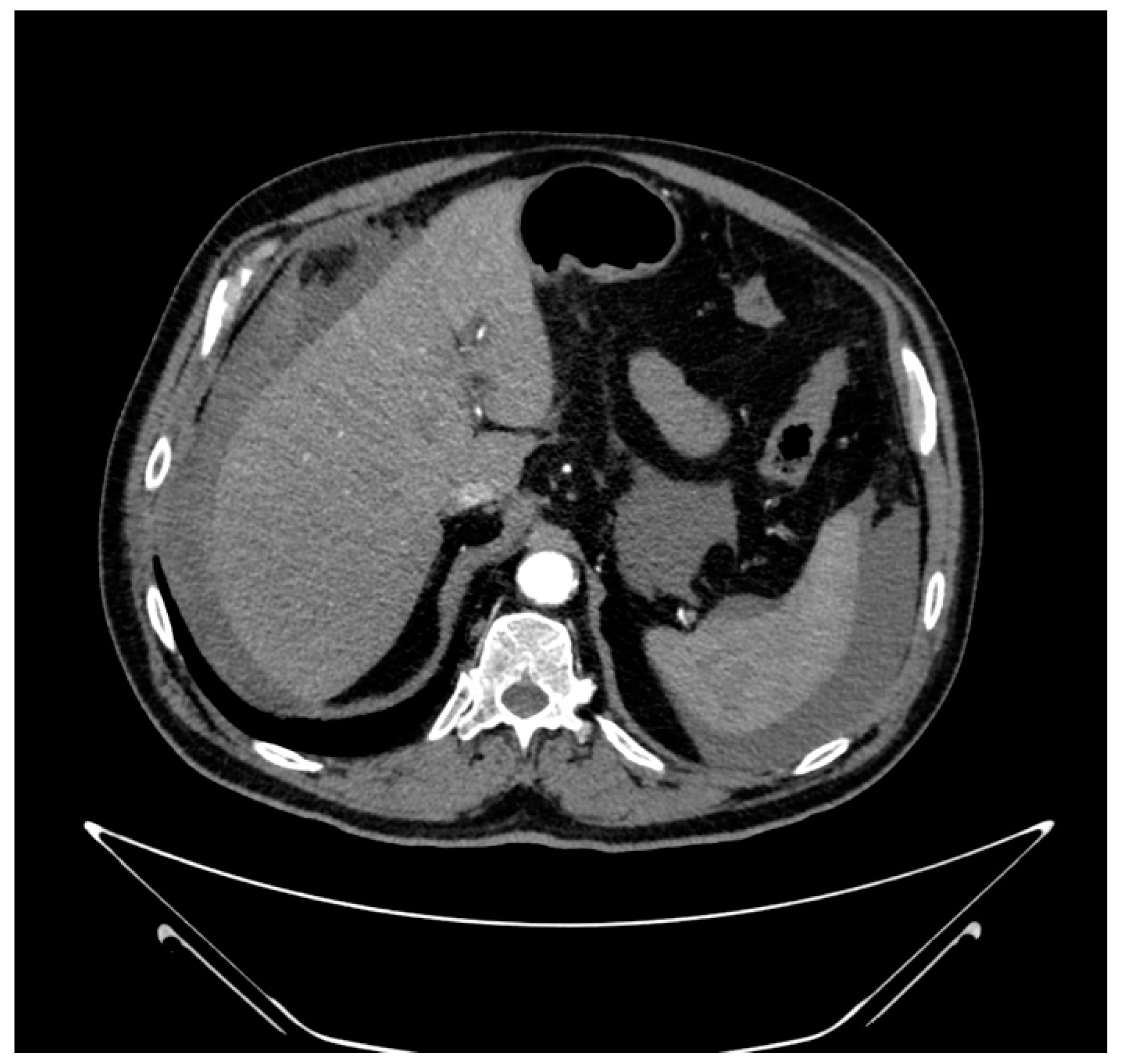
After 20 days, the patient came to our emergency department for chest pain and lypothimia—blood pressure 80/50 mmHg, Hb 9.2 mg/dL and Troponin 95.8 ng/L. An abdominal contrast-enhanced CT-Scan was performed, showing a moderate amount of perihepatic, perisplenic and free peritoneal effusion in the peritoneum with blood density in the pelvic cavity, without signs of extravasation blushing (
Figure 1).
Blood analysis revealed Hb 10.5 mg/dL, platelets 489,000 U/μL, international normalized ratio (INR) 1.13 and low troponin S increasing levels with a peak of 95.80 pg/mL. The patient underwent two red-cell unit transfusions. After two days, an abdominal ultrasound (US) showed stable abdominal effusion, approximately 65 mm in pelvis, 21 mm perihepatic and 32 mm perisplenic.
After one week, the patient woke up in the night for uneasiness, followed by cold sweating, nausea and hypotension (blood pressure 70/50 mmHg). The abdominal contrast-enhanced abdominal CT was performed immediately and confirmed the known effusion, reduced compared to the previous CT, but also displayed a pseudoaneurysm of an inferior-epigastric artery pubic-branch, in the anterior obturator area, of maximum 5 mm, without signs of active bleeding (
Figure 2).
2.3. Therapeutic Intervention
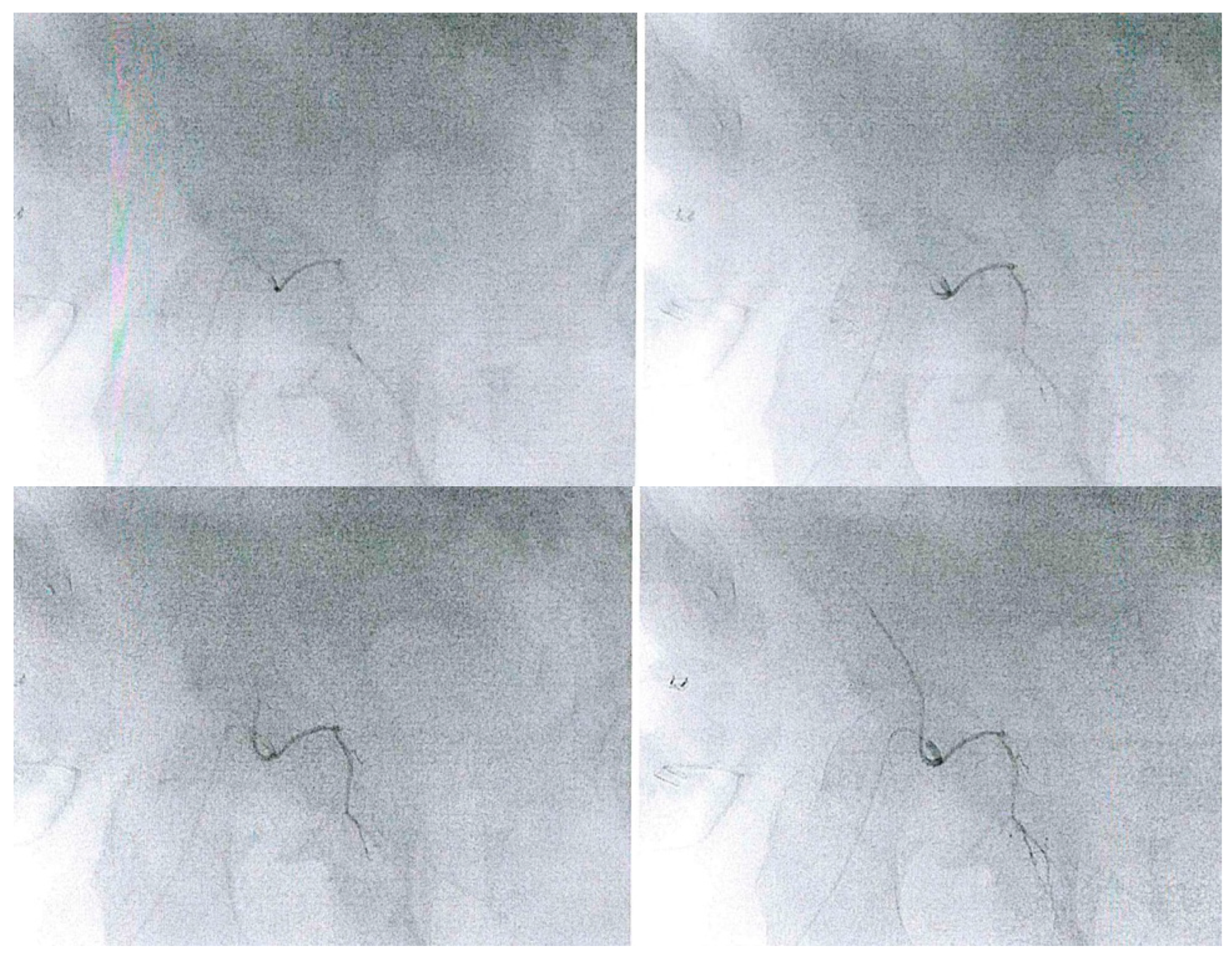
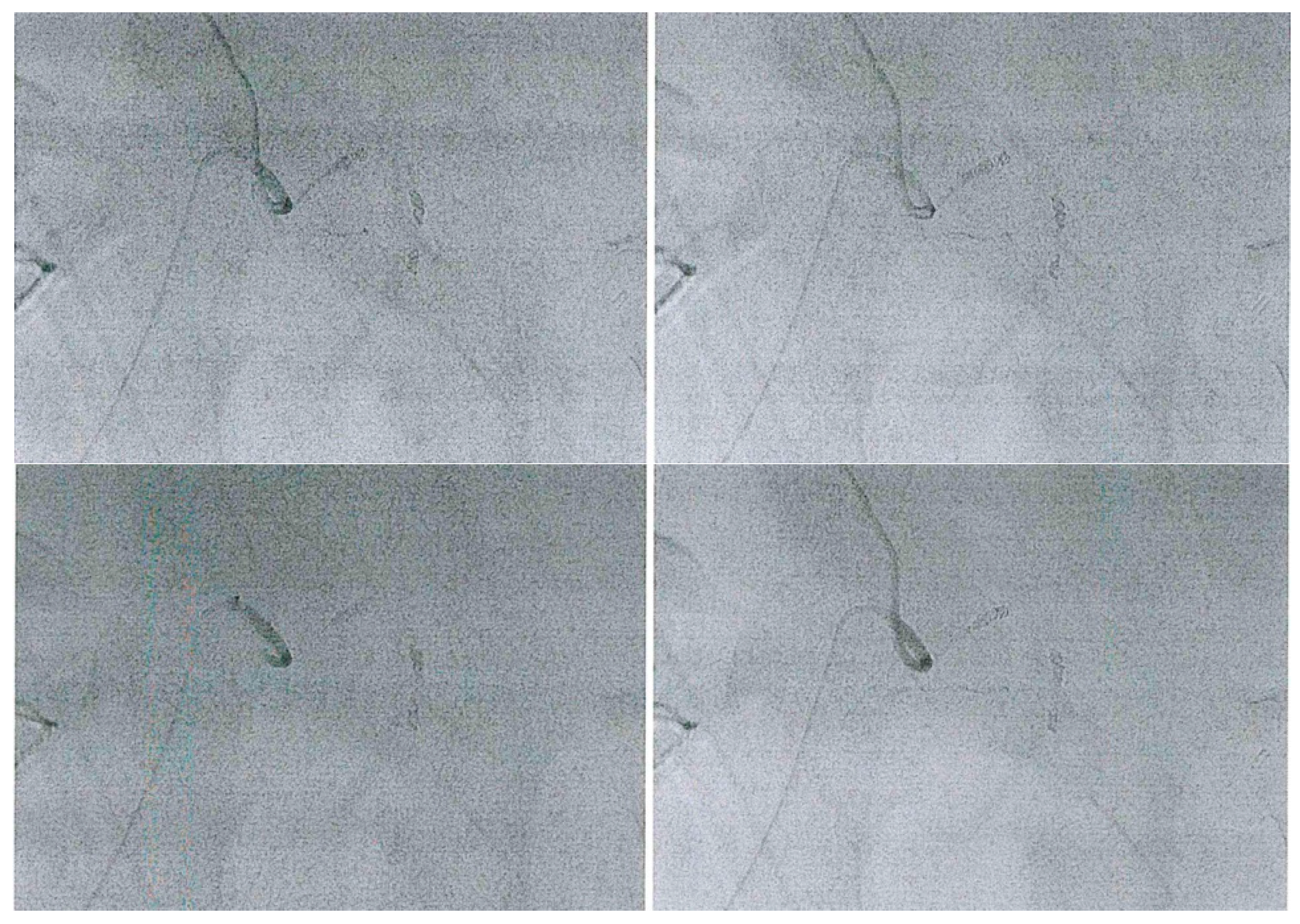
The patient underwent a superselective catheterization of the inferior right epigastric artery through right femoral access. The pseudoaneurysm was confirmed at angiographic study (
Figure 3) and embolized through four metallic microspirals Nester
® Cook 3 × 2 mm. Further complications were not observed (
Figure 4).
2.4. Follow-Up and Outcomes
After 6–12 months follow up, the patient experienced good continence, without requiring the use of safety pads. His erectile functions became worse: he started an intracavernosal injections therapy with complete satisfaction. Bleeding did not occur.
2.5. Discussion
A pseudoaneurysm consists of a single layer of fibrous tissue shaped like a sac creating a turbulent blood flow. It represents the result of a disruption in the vascular wall continuity. The main causes of a pseudoaneurysm are endovascular procedures, surgical procedures, biopsies and drainages [
7]. Monopolar electrocautery, if applied on an arterial wall, could lead to pseudoaneurysm formation [
3], as a consequence of arterial wall injury [
8], every time LND is performed during RARP; it does not require any other apparent risk factor to cause vascular damage [
9].
Every kind of arterial vessel could be involved in this type of injury, as first described in a case series by Bonne et al. [
10]. Pseudoaneurysms have a clinical relevance related to their risk of rupture, embolization of a thrombus, pain, infection or compression of adjacent structures [
11].
In the case presented, during the robotic extended pelvic lymph node dissection before RARP, the epigastric vascular structures were partially isolated and dissected to remove lymphatic tissue around iliac arteries. In particular, electrocautery with monopolar and/or bipolar energy was used: this might have caused vascular wall damage leading to pseudo-aneurysm development.
This case report presents some limitations. It offers an objective view on an atypical clinical presentation of a pseudoaneurysm, but all the findings presented cannot be generalized, as well as the presented management strategies. Any possible association between clinical data, diagnostic and follow-up findings, therapeutic path and patient anamnesis need to be considered only as an accidental relationship, avoiding any tendency to emphasize a cause-effect correlation. Case reports offer only the possibility to carry out hypotheses, they are free of epidemiological quantities, and they do not allow any generalization. The overinterpretation or misinterpretation of a case report may let the physician fall into “the anecdotal fallacy”.
3. Collecting Data
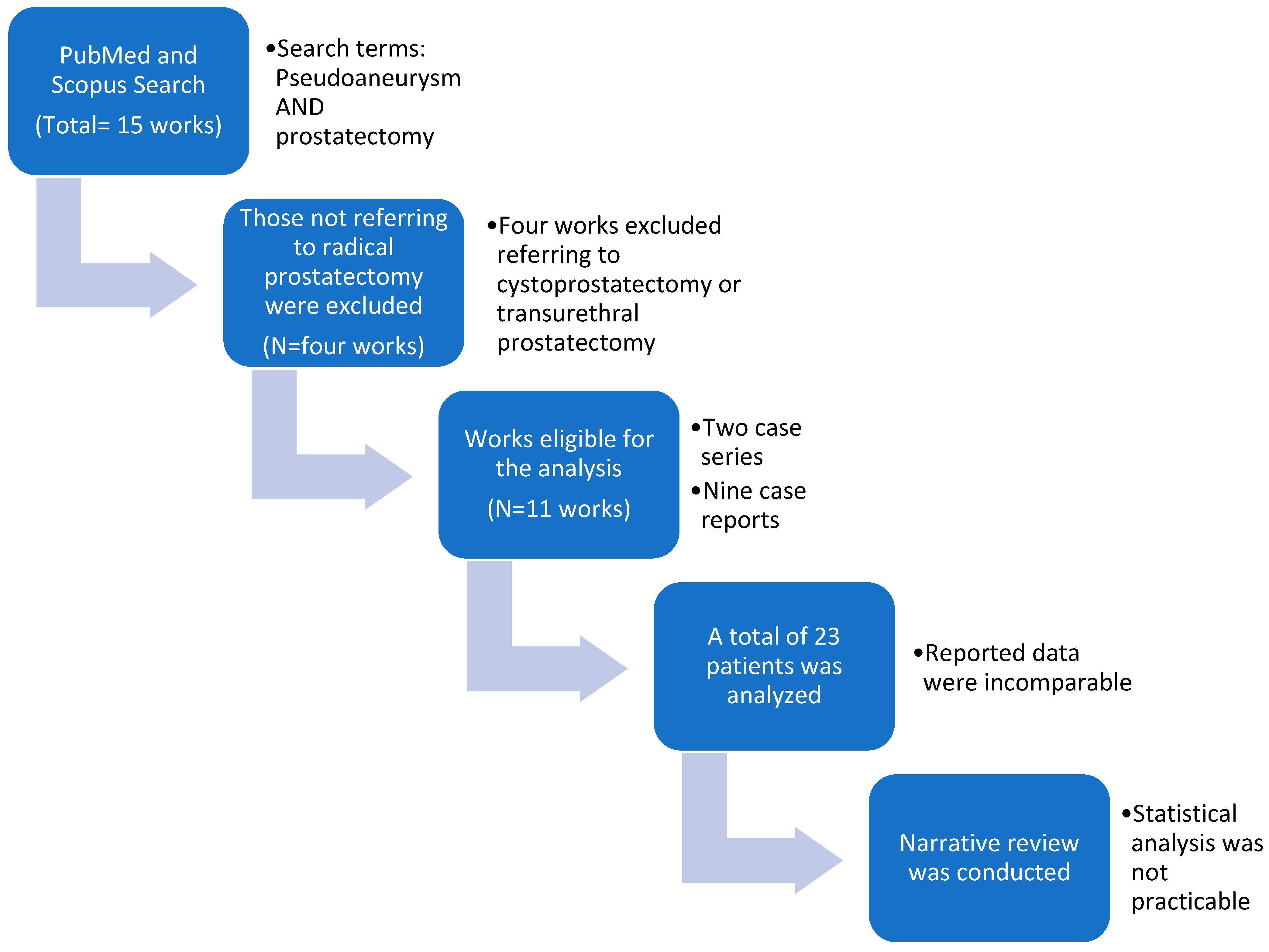
We searched PubMed and Scopus for pseudoaneurysms developing as complications of prostatectomy. The search terms used were “pseudoaneurysm” and “prostatectomy” using the Boolean Operator “AND” up to 1 June 2022. We used the default search strategy “all fields” and we did not select any additional filters. From the resulting 15 works, we excluded those referring to transurethral prostatectomy or cystoprostatectomy. Therefore 11 were included, distinguishable in two case series and nine case reports. We analyzed the reported data for a total of 23 patients who developed pseudoaneurysms after radical prostatectomy (
Figure 5).
The aim was to report a case series and case reports published to collect information according to the following parameters: (1) age, (2) type of surgical procedure (lymphoadenectomy and open, laparoscopic and robot assisted surgery), (3) time interval between operation and pseudoaneurysm evaluation, (4) clinical presentation, (5) imaging exams required to perform diagnosis, (6) artery involved, (7) treatment applied, (8) continence and (9) erectile function.
Due to the rareness of the presentation of pseudoaneurysms, the research found regarding the topic was limited. The data reported in each work were analyzed in different ways by their own authors, thus they lacked comparability and universality. Therefore, we propose a narrative review, as a statistical analysis could not be performed.
3.1. Diagnosis Assessment
There are only few published cases of postprostatectomy pseudoaneurysms (PPP), generally presenting as late hematuria [
12]. The clinical presentation was indeed faceted, but it presents bleeding as its main element. Injured vessels generally dwell in the prostatectomy area, nevertheless the tissue compression in the pelvic space avoids their risk of bleeding, except for large arterial damages or persistent hemorrhages that require intervention [
10]. The intraoperative diagnosis still remains a challenge, considering head-down position and pneumoperitoneum during laparoscopic or robotic procedures [
13].
The diagnosis of pseudoaneurysm is usually carried out through contrast-enhanced computed tomography (CT), a simple, effective and available exam, less invasive than angiography, that differently represents the best choice when a therapeutic intervention is required [
7,
12,
14]. In a previous report, authors suggested an algorithm based on performing CT as a first step and an immediate angiography if pseudoaneurysm was suspected by CT [
13].
Ultrasonography (US) is a valid alternative in consideration of its quick availability, cheapness, fastness, portability and it not requiring appropriate settings. However, its sensitivity is limited and it still remains a full operator-dependent image tool [
7]. In evaluating the prostatic lodge, US can take advantage of an endocavitary probe that allows the local percutaneous treatment, where possible [
12]. A challenging option is magnetic resonance angiography (MR) with three-dimensional gadolinium-enhanced angiography to evaluate pseudoaneurysms in every projection. Unfortunately, MR is expensive, time consuming and not easy to find everywhere. Furthermore, patients are often connected with medical equipment that are non-compatible with MR system, making their appropriate monitoring or vital function supply difficult [
7]. MR use has never been described in a diagnostic path related to pseudoaneurysm after RP.
3.2. Management
Pseudoaneurysm management can substantially vary, according to the requirements of quickness, invasiveness, tolerance of the different techniques and to the vessel involved. Our analysis revealed the following arteries involved, sometimes synchronously (number of cases-vessel or its branch): eight-pudendal, four-internal iliac or branch, three-corona mortis, two-superior vesical, two-inferior vesical, two-external iliac, one-internal iliac, one-gluteal, one-inferior epigastric, one-not identified. The patients were treated as follows (number of cases-type of treatment): sixteen-selective embolization, three-percutaneous embolization, one-transrectal ultrasound thrombin guided injection, one-surgical management. For two patients the pseudoaneurysm management was not described. The most preferred and described technique was endovascular management. A retrospective study analyzed 10 patients who received endovascular treatment for refractory bleeding after RARP showed the safety and efficacy of the procedure, without post-embolization ischemic events [
10]. The principal disadvantages of endovascular management are its invasiveness and the procedure-related risks (formation of hematomas, fistulas, secondary pseudoaneurysms, iodinated contrast material leakage, etc.) [
7].
Bazan et al. described a singular case of pseudoaneurysm visible via transrectal ultrasound, treated with image guided thrombin injection [
12]. Another alternative to endovascular treatment is the percutaneous embolization [
15], which has been described using coils, thrombin and n-butiyl cyanoacrylate glue. It still remains an interesting option when the catheterization of an artery can be challenging and was described by Gonzalez-Araiza et al. [
16]. When the presentation is a severe hemorrhagic shock with unstable hemodynamics, an immediate surgery is mandatory, following all the necessary circulation supports, such as transfusions [
3]. Surgical management must be considered also in case of embolization failure [
17]. The case we described in the present case report was treated through a selective embolization, that represents the most preferred technique [
10,
13,
14,
17,
18,
19], with complete success.
No technique has been shown to be superior or preferrable so far, since the choice depends on the factors mentioned above and the center experience.
3.3. Global Results
Pseudoaneurysms are extremely rare complications of RP. There are 23 reported pseudoaneurysms after RP in small case series and case reports. Two case series show an incidence between 0.16% [
17] and 0.71% [
10].
Patients mean age was 61.19 years, considering that for the 10 patients analyzed by Bonne et al., the mean age reported was 62 and for the two patients of Castelo et al., no age was available. Among the 23 reported patients who underwent prostatectomy, 12 of them received a robotic-assisted approach, eight a retropubic approach (RP) and three patients received a laparoscopic approach (LRP). Surgical approach was intraperitoneal in four cases, extraperitoneal in four cases and not defined in the remaining. Lymphadenectomy was performed in 11 of the 23 patients, was not performed in two of them, and was not specified for four case reports and the two patients by Castelo et al. [
17] (
Table 1).
The mean time from the operation until the clinical presentation was 26.7 days. For 10 patients, a mean time of 1.5 days between RP and endovascular procedure was reported [
10], while for two patients these data are not available [
17].
The symptom most frequently described was hematuria, that characterized 36% of cases (nine patients). Anastomotic dehiscence and anemia were equally found in 24% of patients. Lower back pain and peritoneal irritation had the same frequency (8%). More unfrequently reported symptoms were superficial wound infection, abdominal distension, near syncope, hemorrhagic shock, fever and hypogastric pain with a mean prevalence of 4%. For two patients, no clinical signs or symptoms have been described. For a group of 10 patients, authors describe a continuous drop in hemoglobin despite blood transfusion, hypovolemic shock and bloody discharge from an abdominal drainage catheter [
10].
The diagnostic tool used to confirm diagnosis was contrast enhanced CT-Scan in 18 patients, arteriography in two cases, not reported in two and surgical exploration in only one.
The most chosen management of pseudoaneurysms was embolization, performed in 22 patients (95.6%): 21 patients benefited from a percutaneous/endovascular approach, and one patient underwent transrectal echo-guided thrombin injection. Only one patient required surgical treatment. All the management strategies were one-shot successful (success rate 100%) and no further handling was required. No cases of death have been reported. One case of venous bleeding was described by Bonne et al. [
10] (
Table 2).
3.4. Functional Outcomes
Functional outcomes after pseudoaneurysm treatment are unclear, and are reported inconstantly, incompletely and only in some works. Incontinence and erectile disfunction still remain the most feared postoperative complications after radical prostatectomy [
21,
22]. We found out that erectile function (EF) has not been reported in about 10 patients. In the remaining it was described as good in two patients after two years follow up, seven patients with after 44.7 months mean time, and one patient after one year. EF was compromised in three patients with a mean time of 44.7 months. Similarly, data about continence complaints included: stress incontinence in five patients, in one of them at a follow up period of six months, and in four patients with a 44.7 months follow up mean time; follow up timing was not described for two patients portrayed as continent and for one described as incontinent; six patients were continent at 44.7 months of follow up, while for nine patients, no data were reported. (
Table 3).
This review identifies the internal pudendal artery system as the most frequently involved in pseudoaneurysm development. Since it plays a key role in the erection mechanism, providing high flow for penile tumescence and rigidity, its preservation is critical to ensure residual erectile function after radical prostatectomy [
14]. Suzuki et al. stated that excess embolization of the pudendal artery may be responsible for erectile dysfunction, suggesting to prefer selective minimal embolization in order to avoid erectile dysfunction [
13]. However, the largest case series here analyzed reports long-term impotence in 30% of patients (3/10 patients) and mild stress incontinence in 40% of them (4/10): therefore, authors assume that transarterial embolization or stent graft placement did not worsen potency and continence rates [
10]. Moreover, a singular review, based on 151/3749 patients who had a significant hemorrhage after radical prostatectomy, shows that 12 of them undergone a secondary procedure to control bleeding and experienced poorest erectile function at one year post-operatively [
4].
We can summarize as follows: first, our analysis shows that very poor data have been reported about pseudoaneurysm treatment after radical prostatectomy. Second, different managements are further poorly described to compare various approaches. Third, functional outcomes have been described in a different way by each research work making it difficult to set up a statistical analysis. Fourth, to compare functional data, patients also need to be stratified according to disease related risk, tumor grading (extracapsular extension, seminal vesicles involvement, etc.), prostate size, previous prostate or pelvic surgery, previous radiotherapy or androgen deprivation therapy treatment. Fifth, an analysis conducted in this way might also mitigate medico-legal issues. Since sexual disfunction is one of the most common disease processes managed in urology [
23], a better understanding of the functional effects of pseudoaneurysm treatment will allow the doctor to mention all the available alternatives and their complications or risks, to consent a patient conscious choice and to prevent all possible forensic litigations [
24].
3.5. Future Functional Assessment
The ideal approach should start with an evaluation of functional baseline status through self-administered and validated questionnaires: IIEF-5 for erectile function [
6], IPSS [
5], ICIQ-MLUTS [
25] and DAN-PSS [
26] for continence assessment. In this way, the comparison between baseline and postoperative functional condition can be carried out, and each procedural risk on functional impact might be corrected for all the factors that might affect both continence and the sexual sphere [
27]. A multivariate analysis thus constructed would allow a decisional algorithm definition. In this way, the management of this surgical complication can be seriously evaluated in relation to its possible long-term effects, when the patients with pseudoaneurysm do not need an immediate treatment or it is possible to offer them different management strategies. Obviously, treating it in an emergency setting would leave aside functional implications. This strategy would carry out a flowchart algorithm to perform different lines of treatment. The so-called “tailored management” might achieve pseudoaneurysm control, maximizing functional results and avoiding their compromise by a secondary or salvage treatment.
4. Conclusions
We believe that our case and its management are important and should be considered for the severity and misleading appearance any time a patient who has recently undergone minimally invasive surgery shows an acute clinical presentation.
Pseudoaneurysm is a rare surgical complication and may occur as a consequence of radical prostatectomy. The identification of accessory arteries is a critical phase during surgery, and it must be carried out carefully and avoid most indirect vessel injuries.
Clinical presentation can be multifaceted and often are not univocal. Imaging assessment is mandatory; a CT-scan can be defined as the best choice, followed by an angiography for doubtful cases or in anticipation of endovascular treatment. The management must reflect the severity of the clinical status: selective embolization is safe and effective for all the pseudoaneurysms; percutaneous embolization is minimally invasive and might be preferred when feasible; and surgical exploration is the imperative choice for emergency cases. The choice of the treatment actually depends on the patient’s clinical state or procedure tolerability and the medical center experience. Functional outcome is not predictable based on the few data reported so far. The data found are described qualitatively and bereft of countability, making it impossible to perform a statistical analysis. Future studies must also focus on functional aspects, standardizing both baseline and terminal evaluation and the follow up intervals. Quantifying the risk of functional alterations due to secondary procedures after radical prostatectomy might guide the choice of the most appropriate treatment.
Considering the prevalence of prostate cancer and the widespread surgical availability, the management of radical prostatectomy complications needs to be leveled and conformed exactly as the initial cure approach itself.
Author Contributions
Conceptualization, M.D.C. and D.A.; methodology, M.D.C.; validation, D.A., M.S. and C.F.; formal analysis, D.A.; investigation, M.D.C.; resources, F.P.; data curation, M.D.C. and D.M.; writing—original draft preparation, M.D.C.; writing—review and editing, M.D.C., E.C., D.A. and M.S.; visualization, D.A. and M.M.; supervision, D.A.; project administration, C.F. and F.P.; funding acquisition, M.D.C. and D.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
Not applicable.
Acknowledgments
The authors thank Erica Clemente for English revision.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Abramovic, I.; Vrhovec, B.; Skara, L.; Vrtaric, A.; Nikolac Gabaj, N.; Kulis, T.; Stimac, G.; Ljiljak, D.; Ruzic, B.; Kastelan, Z.; et al. MiR-182-5p and MiR-375-3p Have Higher Performance Than PSA in Discriminating Prostate Cancer from Benign Prostate Hyperplasia. Cancers 2021, 13, 2068. [Google Scholar] [CrossRef] [PubMed]
- Cochetti, G.; Del Zingaro, M.; Ciarletti, S.; Paladini, A.; Felici, G.; Stivalini, D.; Cellini, V.; Mearini, E. New Evolution of Robotic Radical Prostatectomy: A Single Center Experience with PERUSIA Technique. Appl. Sci. 2021, 11, 1513. [Google Scholar] [CrossRef]
- Fujisaki, A.; Takayama, T.; Yamazaki, M.; Komatsubara, M.; Kamei, J.; Sugihara, T.; Ando, S.; Fujimura, T. Postoperative Hemorrhagic Shock 7 Days After Robot-Assisted Radical Prostatectomy. J. Endourol. Case Rep. 2020, 6, 448–450. [Google Scholar] [CrossRef] [PubMed]
- Dean, L.W.; Tin, A.L.; Chesnut, G.T.; Assel, M.; LaDuke, E.; Fromkin, J.; Vargas, H.A.; Ehdaie, B.; Coleman, J.A.; Touijer, K.; et al. Contemporary Management of Hemorrhage After Minimally Invasive Radical Prostatectomy. Urology 2019, 130, 120–125. [Google Scholar] [CrossRef]
- Barry, M.J.; Fowler, F.J.; O’Leary, M.P.; Bruskewitz, R.C.; Holtgrewe, H.L.; Mebust, W.K.; Cockett, A.T. The American Urological Association Symptom Index for Benign Prostatic Hyperplasia. The Measurement Committee of the American Urological Association. J. Urol. 1992, 148, 1549–1557; discussion 1564. [Google Scholar] [CrossRef]
- Rosen, R.C.; Cappelleri, J.C.; Smith, M.D.; Lipsky, J.; Peña, B.M. Development and Evaluation of an Abridged, 5-Item Version of the International Index of Erectile Function (IIEF-5) as a Diagnostic Tool for Erectile Dysfunction. Int. J. Impot. Res. 1999, 11, 319–326. [Google Scholar] [CrossRef]
- Saad, N.E.A.; Saad, W.E.A.; Davies, M.G.; Waldman, D.L.; Fultz, P.J.; Rubens, D.J. Pseudoaneurysms and the Role of Minimally Invasive Techniques in Their Management. Radiographics 2005, 25 (Suppl. S1), S173–S189. [Google Scholar] [CrossRef]
- Postlaparoscopic Iatrogenic Pseudoaneurysms of the Arteries of the Peritoneal and Retroperitoneal Space: Case Report and Review of the Literature—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/19390271/ (accessed on 29 March 2022).
- Ricciardi, E.; Di Martino, G.; Maniglio, P.; Schimberni, M.; Frega, A.; Jakimovska, M.; Kobal, B.; Moscarini, M. Life-Threatening Bleeding after Pelvic Lymphadenectomy for Cervical Cancer: Endovascular Management of Ruptured False Aneurysm of the External Iliac Artery. World J. Surg. Oncol. 2012, 10, 149. [Google Scholar] [CrossRef]
- Bonne, L.; Gillardin, P.; De Wever, L.; Vanhoutte, E.; Joniau, S.; Oyen, R.; Maleux, G. Endovascular Management of Severe Arterial Haemorrhage After Radical Prostatectomy: A Case Series. Cardiovasc. Interv. Radiol. 2017, 40, 1698–1705. [Google Scholar] [CrossRef]
- Dell’Atti, L.; Galeotti, R. Pseudoaneurysm Secondary to Transvesical Prostatectomy. Indian J. Urol. 2016, 32, 164–165. [Google Scholar] [CrossRef]
- Bazan, F.; Sanchez Parrilla, J.; Radosevic, A.; Aguilar, G.; Frances, A.; del Riego, J.; Busto Barreda, M. Deep Pelvic Postprostatectomy Pseudoaneurysm Treated by Transrectal Ultrasound-Guided Thrombin Injection. Cardiovasc. Interv. Radiol. 2014, 37, 544–547. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, R.; Goto, T.; Kohno, S.; Kita, Y.; Shimizu, H.; Kobayashi, T.; Yamasaki, T.; Ogawa, O.; Inoue, T. Arteriovenous Fistula after Robot-Assisted Laparoscopic Prostatectomy: A Rare Case Report. IJU Case Rep. 2019, 2, 184–186. [Google Scholar] [CrossRef] [PubMed]
- Lopes, R.I.; Mitre, A.I.; Rocha, F.T.; Piovesan, A.C.; da Costa, O.F.; Karakhanian, W. Case Report: Late Recurrent Hematuria Following Laparoscopic Radical Prostatectomy May Predict Internal Pudendal Artery Pseudoaneurysm and Arteriovenous Fistula. J. Endourol. 2009, 23, 297–299. [Google Scholar] [CrossRef]
- Pisano, U.; Soon, V.-L.; Douglas, P. Corona Mortis Injury Causing Delayed Presentation of Pelvic Pseudoaneurysm. Radiol. Case Rep. 2021, 16, 1095–1098. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Araiza, G.; Haddad, L.; Patel, S.; Karageorgiou, J. Percutaneous Embolization of a Postsurgical Prostatic Artery Pseudoaneurysm and Arteriovenous Fistula. J. Vasc. Interv. Radiol. 2019, 30, 269–271. [Google Scholar] [CrossRef]
- Castelo, B.Q.L.; Mourao, T.C.; Santana, T.B.M.; Favaretto, R.d.L.; Oliveira, R.A.R.; Guimarães, G.C. Pelvic Pseudoaneurysm as a Cause of Severe Hematuria after Robotic-Assisted Radical Prostatectomy. Urology 2021, 148, e23–e24. [Google Scholar] [CrossRef] [PubMed]
- Beckley, I.; Patterson, B.; Hamaday, M.; Vale, J.; Hrouda, D. Case Report: Delayed Hemorrhage from an Accessory Internal Pudendal Artery Pseudoaneurysm after Robotic Radical Prostatectomy: Successful Management with Ct Angiography and Embolization. J. Endourol. 2007, 21, 923–925. [Google Scholar] [CrossRef]
- Feng, T.; Patel, H.D.; Allaf, M.E. Pudendal Artery Pseudoaneurysm after Robot-Assisted Laparoscopic Radical Prostatectomy. Urology 2013, 81, e5–e6. [Google Scholar] [CrossRef]
- Han, J.; Shah, M.; Djaladat, H.; Aron, M. Corona Mortis Artery Pseudoaneurysm Causing Delayed Intermittent Hemoperitoneum after Robotic Radical Prostatectomy. Urology 2020, 141, e24–e25. [Google Scholar] [CrossRef]
- Checcucci, E.; Pecoraro, A.; DE Cillis, S.; Manfredi, M.; Amparore, D.; Aimar, R.; Piramide, F.; Granato, S.; Volpi, G.; Autorino, R.; et al. The Importance of Anatomical Reconstruction for Continence Recovery after Robot Assisted Radical Prostatectomy: A Systematic Review and Pooled Analysis from Referral Centers. Minerva Urol. Nephrol. 2021, 73, 165–177. [Google Scholar] [CrossRef]
- Efficacy of Tadalafil in Penile Rehabilitation Started before Nerve-Sparing Robot-Assisted Radical Prostatectomy: A Double-Blind Pilot Study—Sexual Medicine. Available online: https://www.smoa.jsexmed.org/article/S2050-1161(22)00022-8/fulltext (accessed on 21 April 2022).
- Jesse, E.; Muncey, W.; Harris, D.; Tay, K.; Kim, T.; Omil-Lima, D.; Isali, I.; Loeb, A.; Thirumavalavan, N. Sexual Dysfunction Damages: A Legal Database Review. Can. Urol. Assoc. J. 2022, 16, E278–E286. [Google Scholar] [CrossRef] [PubMed]
- Raveesh, B.N.; Nayak, R.B.; Kumbar, S.F. Preventing Medico-Legal Issues in Clinical Practice. Ann. Indian Acad. Neurol. 2016, 19, S15–S20. [Google Scholar] [CrossRef] [PubMed]
- Donovan, J.L.; Peters, T.J.; Abrams, P.; Brookes, S.T.; de la Rosette, J.J.; Schäfer, W. Scoring the Short Form ICSmaleSF Questionnaire. International Continence Society. J. Urol. 2000, 164, 1948–1955. [Google Scholar] [CrossRef]
- Schou, J.; Poulsen, A.L.; Nordling, J. The Value of a New Symptom Score (DAN-PSS) in Diagnosing Uro-Dynamic Infravesical Obstruction in BPH. Scand. J. Urol. Nephrol. 1993, 27, 489–492. [Google Scholar] [CrossRef] [PubMed]
- EAU Guidelines on the Management of Non-Neurogenic Male LUTS—INTRODUCTION—Uroweb. Available online: https://uroweb.org/guidelines/management-of-non-neurogenic-male-luts/chapter/introduction (accessed on 21 April 2022).
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}