Abstract
Background/Objectives: Congenital clubfoot (CC) is one of the most common congenital deformities of the lower limbs, typically presenting as a complex skeletal malformation. It is frequently associated with other congenital anomalies, although the co-occurrence with agenesis of the toes is rare. This case report describes a unique presentation of congenital clubfoot associated with agenesis of the 4th and 5th toes, focusing on clinical management and reviewing the literature on skeletal malformations linked to CC. Methods: A comprehensive literature review was conducted, focusing on studies published in the last decade regarding congenital clubfoot and its association with other skeletal malformations. A clinical analysis of a patient with congenital clubfoot and digital agenesis was performed, including diagnostic methods, treatment approach, and follow-up results. The patient was treated with the Ponseti method, followed by percutaneous Achilles tendon tenotomy due to insufficient correction. Due to persistent equinus deformity, a second intervention involving Achilles tendon lengthening and syndesmotic capsulotomy was performed. Results: The patient presented with unilateral congenital clubfoot and agenesis of the 4th and 5th toes, a rare combination. Initial correction was achieved with the Ponseti method, but further surgical intervention was needed. Follow-up at 2 years showed excellent results, with the patient able to walk without difficulty. The literature review revealed limited cases involving digital agenesis associated with clubfoot. Conclusions: This case report highlights the rare association between congenital clubfoot and agenesis of the 4th and 5th toes. While satisfactory outcomes were achieved, further studies are needed to explore potential worse outcomes in cases with associated malformations and the genetic factors involved.
1. Introduction
Congenital clubfoot (CC) is one of the most common congenital deformities of the lower limbs, with an estimated incidence of approximately 1 in 1000 live births [1]. The deformity is characterized by a combination of foot inversion, equinus, adduction, cavus, and varus, and can affect one or both feet. The etiology of CC remains largely unknown, though genetic, environmental, and intrauterine factors have been suggested as contributing causes [2]. While the condition itself is well recognized, its association with other skeletal malformations, particularly agenesis of the toes, is extremely rare.
Agenesis of the toes, particularly the 4th and 5th digits, has been documented in a limited number of cases and is often considered a separate congenital anomaly. The occurrence of both congenital clubfoot and agenesis of multiple digits presents a unique challenge in diagnosis and treatment, as the management approach must account for both the deformity and the absence of toes. Current treatment strategies for CC primarily include conservative methods, such as the Ponseti technique, which has shown favorable outcomes in most cases. However, in some instances, surgical interventions, including Achilles tendon tenotomy, are required to achieve optimal correction [3].
The literature on the association between CC and agenesis of the toes is sparse, with few cases described in the medical literature. Some authors have speculated that these anomalies might share a common developmental origin, while others suggest that their co-occurrence is purely coincidental. This paper presents a rare case of congenital clubfoot characterized by the agenesis of the fourth and fifth toes. Furthermore, it reviews the extant literature on this skeletal malformation in clubfoot.
The objective of this study is to describe the clinical presentation, management, and outcome of a rare association between congenital clubfoot and digital agenesis, and to explore whether such anatomical variations influence the standard Ponseti treatment protocol.
2. Materials and Methods
This study presents a rare case of congenital clubfoot (CC) associated with agenesis of the 4th and 5th toes. The patient involved in this study is a 1-month-old (male), diagnosed with unilateral (left side) congenital clubfoot, treated according to the Ponseti method.
- Patient Information
The patient was initially evaluated at the Annunziata Hospital, Cosenza (Italy), with informed consent obtained for both treatment and publication of the case. The patient’s medical history, including prenatal, perinatal, and postnatal factors, was reviewed to ensure the case’s uniqueness and to rule out other potential causes of the malformation. No genetic testing was conducted for this patient; however, clinical and radiographic evaluations revealed no systemic anomalies suggestive of syndromic associations.
- Diagnostic Evaluation
Diagnosis of congenital clubfoot was made based on physical examination, which showed typical features of the deformity. Agenesis of the 4th and 5th toes was diagnosed through X-ray and clinical examination.
- Treatment Protocol
The treatment of congenital clubfoot was carried out using the Ponseti method, which involved the application of a femoro-pedal plaster cast, replaced weekly for six weeks at the age of two months. Once the clubfoot deformity was adequately corrected, an Achilles tendon tenotomy was performed under general anesthesia at the age of three months. However, due to the persistence of the equinus deformity, a second surgical procedure was required at eight months, consisting of Achilles tendon lengthening and sindesmo-capsulotomy. A new femoro-pedal plaster cast was then applied for one month, followed by the use of the Mitchell-Ponseti brace for 23 h per day for three months, and subsequently only during nap time.
- Follow-Up and Outcome Measures
Post-treatment follow-up was conducted weekly to monitor the patient’s progress and ensure proper foot alignment. The patient’s clinical outcomes were assessed using the Pirani Score alongside radiological imaging to evaluate the alignment of the foot and the position of the toes.
- Literature Review Methodology
A systematic review of the literature was conducted to examine the current state of knowledge regarding congenital clubfoot and associated skeletal malformations, with a particular focus on agenesis of the toes. We searched PubMed and Google Scholar databases for articles published in the last ten years, using the following key terms: “congenital clubfoot,” “agenesis of toes,” “congenital foot deformities,” and “skeletal malformations”. Studies were included if they addressed congenital clubfoot associated with skeletal anomalies, excluding syndromic or genetically confirmed cases.
- Data Availability
All data associated with this study are available upon request. The patient’s anonymized medical records, images, and relevant data have been submitted and can be accessed.
3. Results
3.1. Clinical Outcomes
- The initial patient’s foot deformity was classified as 5 Pirani Score indicating a severe deformity (Figure 1).
- Follow-up assessments were carried out at 30 and 60 days and demonstrated persistent equinus of the foot (as noted in Figure 2, incomplete descent of calcaneus).
- Due to persistent of equinus deformity, the patient underwent Achilles tendon tenotomy and sindesmocapsulotomy (Figure 3a).
- The final clinical outcome showed corrected alignment, mobility, and function (Figure 3b,c).
- At the two-year follow-up, the foot demonstrated good alignment, mobility, and function. Gait was normal, with no signs of limping. Physical and X-ray examination revealed a 2 cm limb length discrepancy on the left side (Figure 4).
3.2. Radiological Findings
- Pre-treatment imaging showed typical congenital clubfoot features, such as equinus, adductus, and varus.
- Agenesis of the 4th and 5th toes was confirmed via X-ray, showing the absence of the 4th and 5th toes.
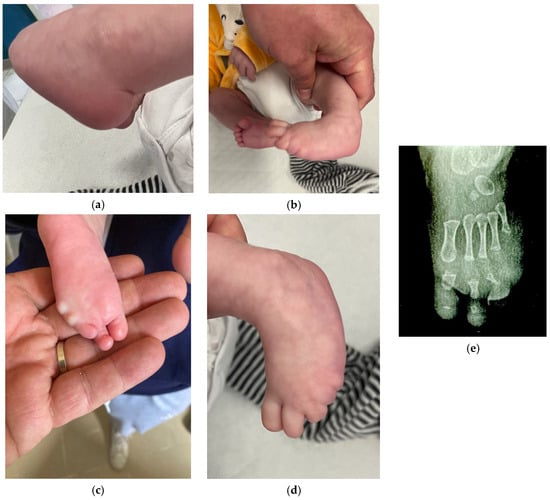
Figure 1.
This is the foot before the treatment. (a): equinus deformity; (b): varus and supination of the foot; (c,d): absence of 4th and 5th finger; (e): x-ray of the foot before treatment.
Figure 1.
This is the foot before the treatment. (a): equinus deformity; (b): varus and supination of the foot; (c,d): absence of 4th and 5th finger; (e): x-ray of the foot before treatment.
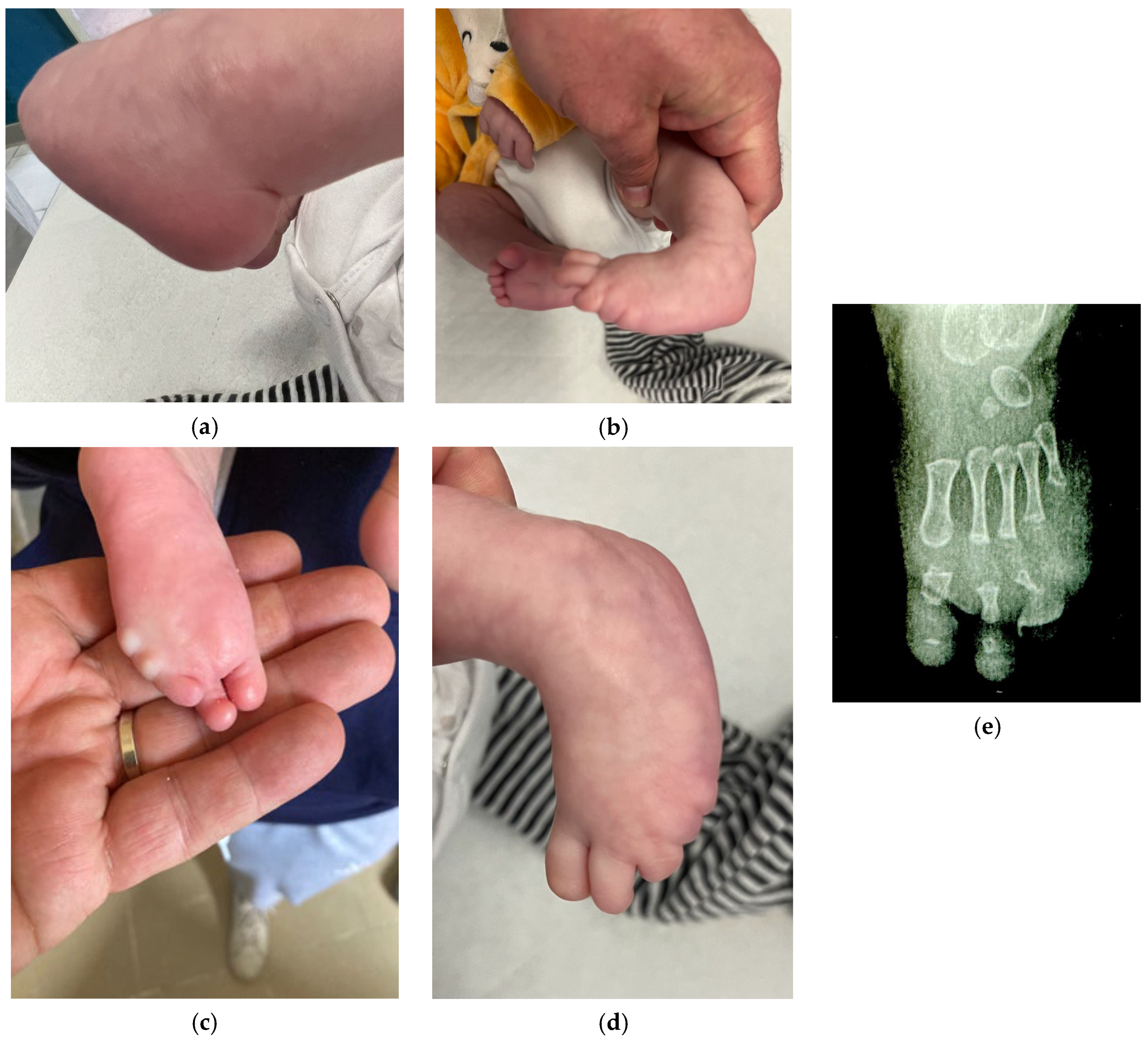

Figure 2.
This is the foot at the end of first treatment. We achieved a good reduction (a), but the heel remained unreduced (b,c) (X-ray at 6 months).
Figure 2.
This is the foot at the end of first treatment. We achieved a good reduction (a), but the heel remained unreduced (b,c) (X-ray at 6 months).

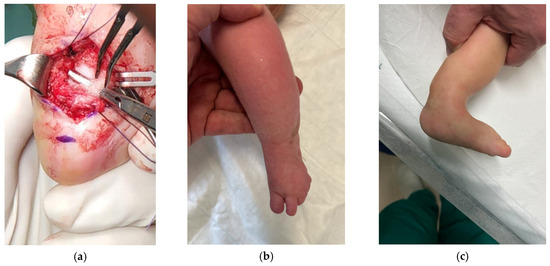
Figure 3.
Due to persistent equinus deformity, a second intervention involving Achilles tendon lengthening and capsular release (syndesmotic capsulotomy) (a) was performed, achieving corrected alignment, mobility, and function (b,c).
Figure 3.
Due to persistent equinus deformity, a second intervention involving Achilles tendon lengthening and capsular release (syndesmotic capsulotomy) (a) was performed, achieving corrected alignment, mobility, and function (b,c).
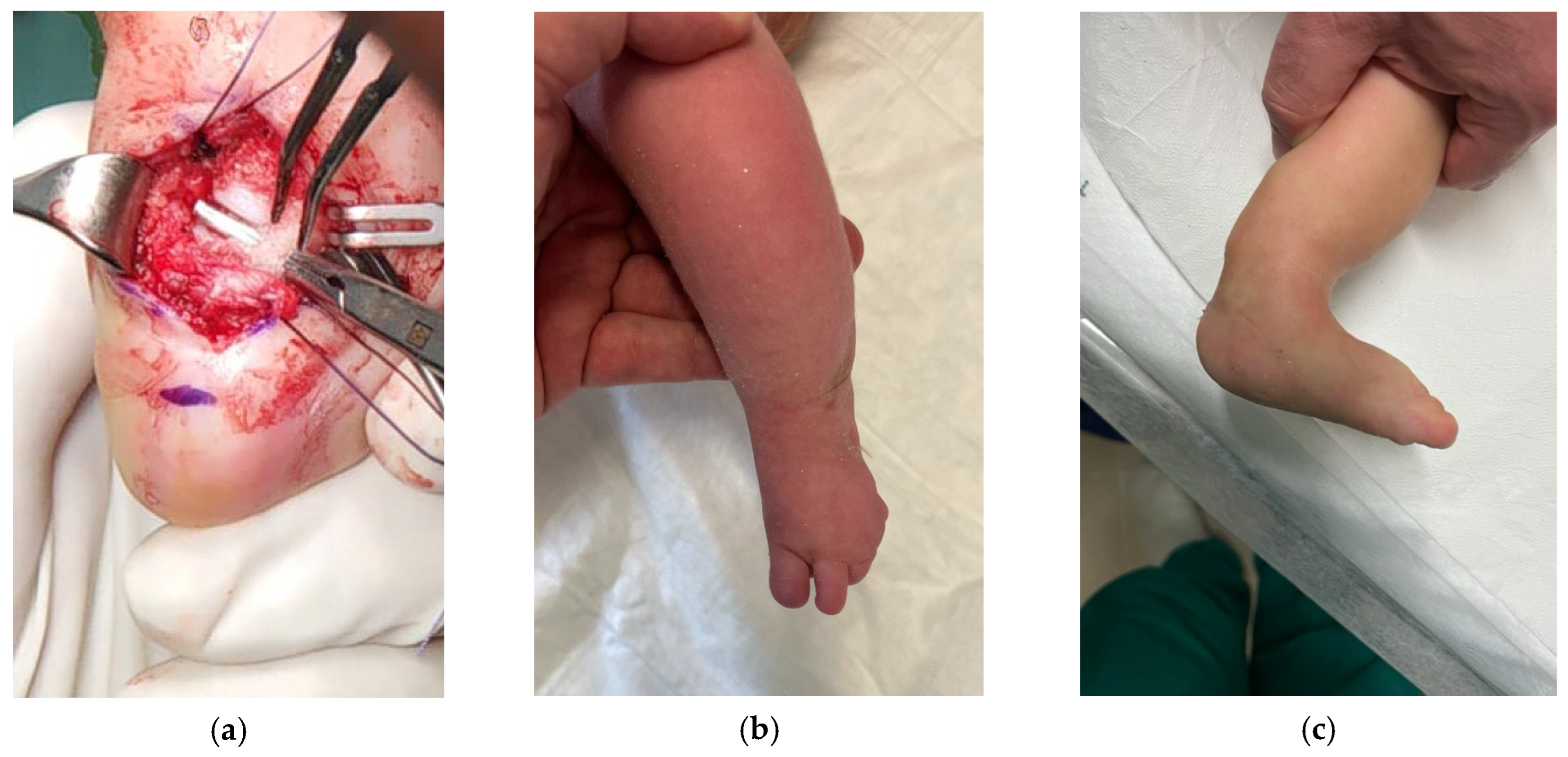

Figure 4.
Follow-up at two years showed good alignment and mobility. An X-ray revealed a 2 cm limb length discrepancy on the left side.
Figure 4.
Follow-up at two years showed good alignment and mobility. An X-ray revealed a 2 cm limb length discrepancy on the left side.

4. Discussion
4.1. Interpretation of Findings
The case presented highlights a rare association of congenital clubfoot with agenesis of the 4th and 5th toes. The patient’s clinical outcomes following Ponseti treatment, supplemented with Achilles tendon tenotomy, were favorable, showing significant improvement in foot alignment and function. This outcome is consistent with the extensive body of literature supporting the Ponseti method as the gold standard for managing congenital clubfoot. Studies have demonstrated high success rates with this approach, particularly in terms of achieving initial correction and long-term functional outcomes [3].
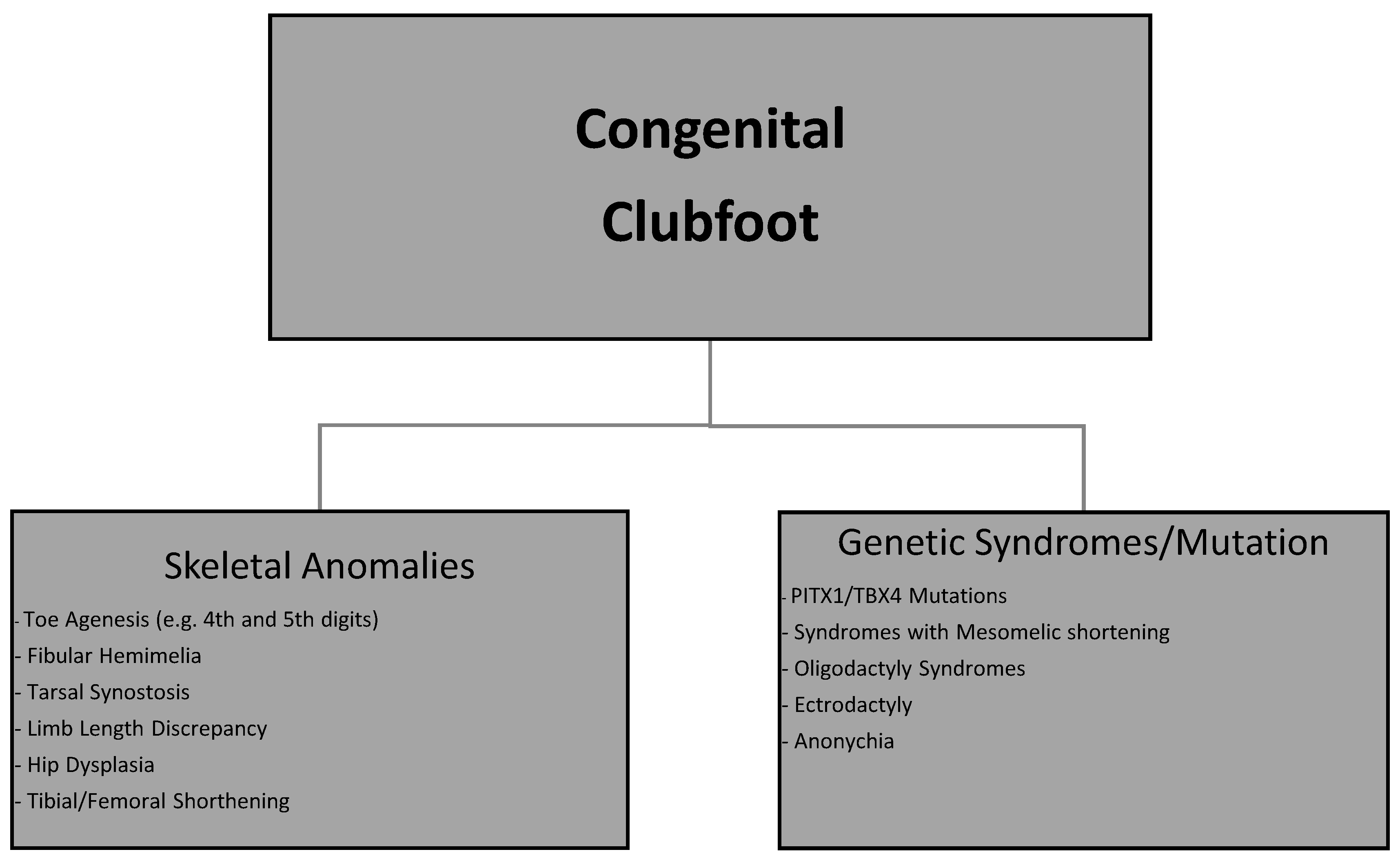
In the differential diagnosis (Figure 5), fibular hemimelia should be considered, particularly in light of the associated toe agenesis and the presence of ankle varus. Paley’s classification of fibular hemimelia includes presentations with foot deformities mimicking clubfoot, often accompanied by hypoplasia or absence of lateral rays. However, in our case, radiological and clinical findings confirmed the presence of all leg bones and a typical pattern of equinovarus deformity consistent with congenital clubfoot. Nevertheless, the hypoplasia of the lateral foot and missing toes may contribute to a complex biomechanical imbalance and should prompt clinicians to consider a broader spectrum of congenital limb deficiencies in such presentations.
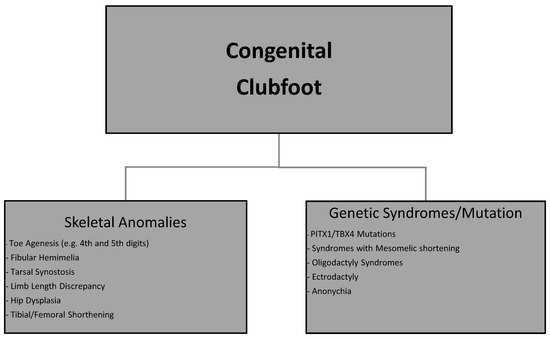
Figure 5.
Association of congenital clubfoot.
However, the unique presence of agenesis of the 4th and 5th toes adds a new layer of complexity to this case. Toe agenesis, a rare malformation, is often linked to other skeletal anomalies or syndromes. While some studies have explored the associations between congenital clubfoot and other skeletal malformations, such as hip dysplasia and limb-length discrepancies [4], the relationship between clubfoot and toe agenesis remains under-researched. Prenatal diagnosis is therefore essential to rule out other malformations from birth and to initiate appropriate treatment that also takes into account any other associated conditions [5]. This case contributes to the limited knowledge available, offering a deeper understanding of how isolated toe agenesis may coexist with congenital foot deformities.
4.2. Comparing with Existing Literature
A review of recent studies confirms that congenital clubfoot is frequently associated with other skeletal malformations, though most studies focus on conditions such as hip dysplasia, tibial anomalies, and fibular hemimelia. However, the occurrence of toe agenesis in association with clubfoot is rarely reported. Some studies have highlighted the genetic and developmental factors that contribute to both conditions [6,7]. For instance, mutations in genes involved in limb development, such as those related to HoxC-gene cluster, have been implicated in cases of both clubfoot and vertical talus, and hip dysplasia [8].
We found only one study in the literature that investigates the anatomy of a congenitally short lower limb associated with rigid clubfoot and ectrodactyly [9]. The authors dissected and performed arteriography on an amputated limb to examine the relationship between abnormal arterial patterns and bony anomalies. The limb presented a short femur, tibia, and fibula, clubfoot with tarsal synostosis (fusion of tarsal bones), absence of some metatarsals, ectrodactyly, and a bifid hallux (split big toe). The authors hypothesize that the abnormal arterial pattern reduced the collateral blood supply, making the limb more susceptible to teratogenic damage. They suggest that a vascular event (e.g., hemorrhage or embolism) compromised blood flow, leading to both general limb shortening and specific defects in the foot.
4.3. Implications for Future Research
From the literature analysis, few studies highlight the association between congenital clubfoot and agenesis of the toes. The absence of the last rays has not caused modifications to the Ponseti method. This case underscores the need for further research into the relationship between congenital clubfoot and associated skeletal malformations, including toe agenesis. Given the rarity of such associations, large multicenter studies and genetic investigations are warranted to explore potential genetic links and identify predictors of such co-occurring malformations. Furthermore, future research could focus on long-term outcomes for patients with both congenital clubfoot and toe agenesis, examining whether standard treatment protocols, like the Ponseti method, provide adequate functional results in such cases.
In terms of treatment, the Ponseti method remains the gold standard for clubfoot correction, with multiple studies supporting its efficacy in achieving foot correction and minimizing the need for extensive surgeries. However, the presence of toe agenesis may necessitate modifications in the treatment protocol, particularly in terms of assessing functional outcomes. While the literature generally focuses on the correction of foot deformities, less attention is given to the long-term implications of associated malformations such as toe agenesis.
Furthermore, the causes of limb formation defects are often linked to a vascular etiology [10]. It is therefore logical that in cases of congenital clubfoot associated with limb formation defects, the vascularization must be given serious consideration.
Additionally, the role of genetic counseling in managing patients with complex congenital malformations should be explored. Understanding the genetic factors contributing to both clubfoot and toe agenesis could help guide therapeutic decisions and inform prognosis.
4.4. Limitations of the Current Study
While this case provides valuable insights into a rare association, it is important to acknowledge the limitations of a single case report. Larger cohort studies are needed to confirm the generalizability of the findings and further elucidate the full spectrum of congenital clubfoot associations. Moreover, the long-term follow-up data for this patient is limited, and further assessment will be needed to determine the durability of the treatment outcomes over time.
5. Conclusions
In conclusion, this case report highlights a rare association between congenital clubfoot and agenesis of the 4th and 5th toes, contributing to the limited body of literature on this topic. The successful management of the patient using the Ponseti method, complemented by Achilles tendon tenotomy, supports the efficacy of this approach in correcting congenital clubfoot deformities, even in the presence of associated skeletal malformations. However, the presence of toe agenesis adds complexity to clinical management and requires further research to understand the long-term implications on foot function and overall mobility. It is evident that the association between clubfoot and skeletal anomalies often suggests an underlying chromosomal pathology, which can lead to treatment resistance and significantly influence the outcome.
This case emphasizes the need for more studies exploring the co-occurrence of clubfoot with other skeletal malformations, particularly in cases involving toe agenesis, as well as the role of genetic factors in such associations.
Author Contributions
Conceptualization, G.V. and G.C.; methodology, G.V.; formal analysis, G.V.; investigation, G.V.; resources, G.V.; data curation, G.V.; writing—original draft preparation, G.V.; writing—review and editing, G.C.; visualization, G.V.; supervision, G.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Case reports typically do not require approval from an Ethics Committee. This is because case reports are not considered clinical trials or research studies involving experimental procedures. In Italy, the Code of Medical Ethics (Article 36) and the General Data Protection Regulation (GDPR)-Regulation (EU) 2016/679 govern the publication of case reports. These regulations allow for the publication of such reports provided that informed consent from the patient (or legal guardian in the case of minors) is obtained, and confidentiality regarding sensitive patient information is maintained.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed at the corresponding authors.
Acknowledgments
During the preparation of this manuscript, ChatGPT-version Versione 1.2025.168, an AI language model developed by OpenAI, was used to improve the writing style and enhance the clarity of the text. However, no generative AI tools were used in the research process or for sourcing bibliographic data. The content, data analysis, and all scientific interpretations are solely the result of the authors’ work and expertise.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CC | congenital clubfoot |
References
- Panza, R.; Albano, F.; Casto, A.; Del Vecchio, C.; Laforgia, N.; Dibello, D. Incidence and prevalence of congenital clubfoot in Apulia: A regional model for future prospective national studies. Ital. J. Pediatr. 2023, 49, 151. [Google Scholar] [CrossRef] [PubMed]
- Dobbs, M.B.; Gurnett, C.A. Genetics of clubfoot. J. Pediatr. Orthop. B 2012, 21, 7–9. [Google Scholar] [CrossRef] [PubMed]
- Ganesan, B.; Luximon, A.; Al-Jumaily, A.; Balasankar, S.K.; Naik, G.R. Ponseti method in the management of clubfoot under 2 years of age: A systematic review. PLoS ONE 2017, 12, e0178299. [Google Scholar] [CrossRef] [PubMed]
- Håberg, Ø.; Foss, O.A.; Lian, Ø.B.; Holen, K.J. Is foot deformity associated with developmental dysplasia of the hip? Bone Joint J. 2020, 102-B, 1582–1586. [Google Scholar] [CrossRef] [PubMed]
- Ruzzini, L.; De Salvatore, S.; Longo, U.G.; Marino, M.; Greco, A.; Piergentili, I.; Costici, P.F.; Denaro, V. Prenatal Diagnosis of Clubfoot: Where Are We Now? Systematic Review and Meta-Analysis. Diagnostics 2021, 11, 2235. [Google Scholar] [CrossRef] [PubMed]
- Hedley, P.L.; Lausten-Thomsen, U.; Conway, K.M.; Hinds, K.; Romitti, P.A.; Christiansen, M. Trends in congenital clubfoot prevalence and co-occurring anomalies during 1994–2021 in Denmark: A nationwide register-based study. BMC Musculoskelet. Disord. 2023, 24, 784. [Google Scholar] [CrossRef] [PubMed]
- Bianco, A.M.; Ragusa, G.; Di Carlo, V.; Faletra, F.; Di Stazio, M.; Racano, C.G.; Cappellani, S.; De Pellegrin, M.; d’Addetta, I.; Carluccio, G.; et al. What Is the Exact Contribution of PITX1 and TBX4 Genes in Clubfoot Development? An Italian Study. Genes 2022, 13, 1958. [Google Scholar] [CrossRef] [PubMed]
- Alvarado, D.M.; McCall, K.; Hecht, J.T.; Dobbs, M.B.; Gurnett, C.A. Deletions of 5′ HOXC genes are associated with lower extremity malformations, including clubfoot and vertical talus. J. Med. Genet. 2016, 53, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Hootnick, D.R.; Packard, D.S., Jr.; Levinsohn, E.M.; Lebowitz, M.R.; Lubicky, J.P. The anatomy of a congenitally short limb with clubfoot and ectrodactyly. Teratology 1984, 29, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Ordal, L.; Keunen, J.; Martin, N.; Shehata, N.; Borschel, G.H.; Clarke, H.M.; Toi, A.; Shuman, C.; Chitayat, D. Congenital limb deficiencies with vascular etiology: Possible association with maternal thrombophilia. Am. J. Med. Genet. A 2016, 170, 3083–3089. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).