

The Impact of COVID-19 Regulations on Adherence to Recombinant Human Growth Hormone Therapy: Evidence from Real-World Data

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
- (i).
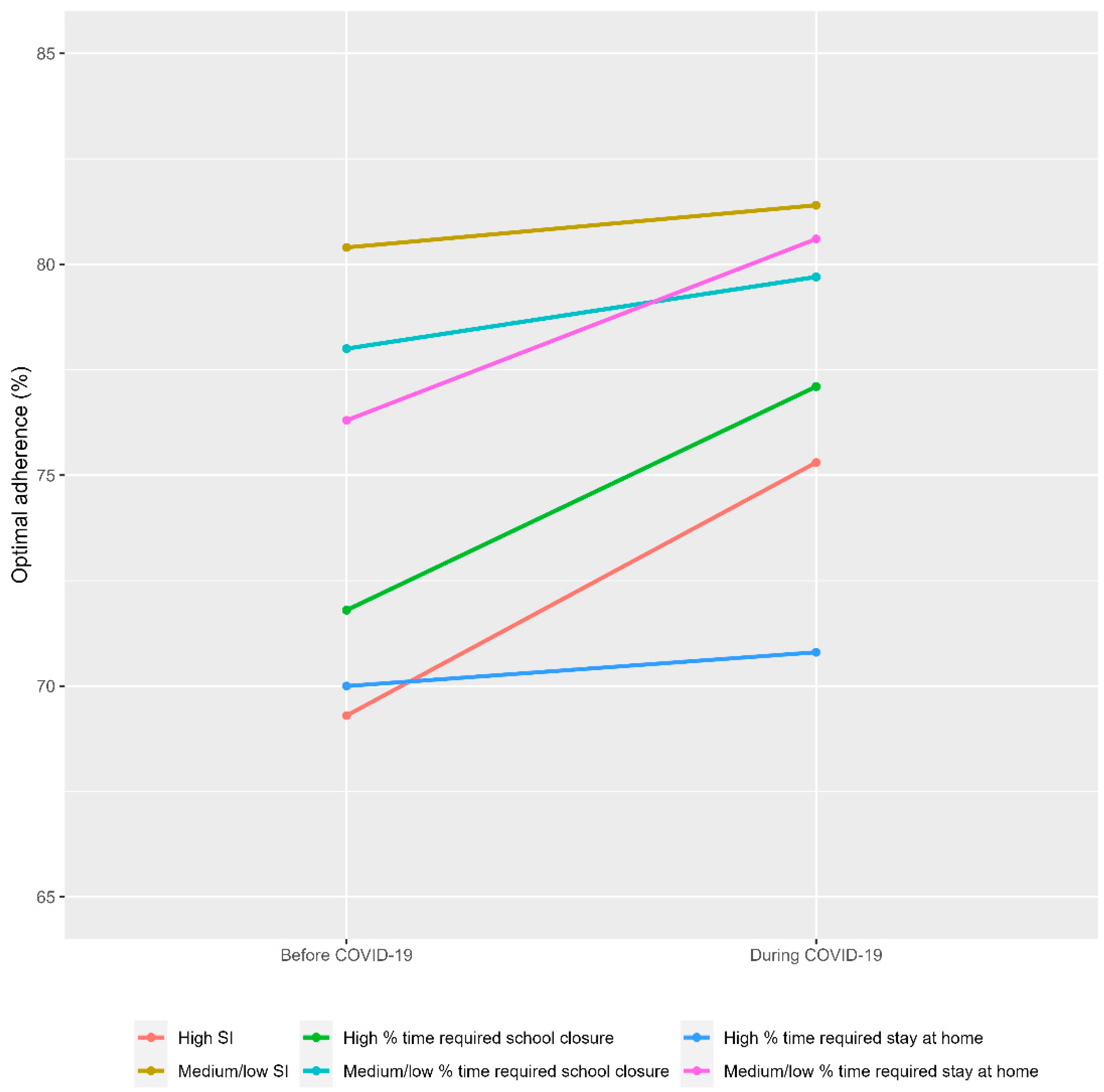
- The stringency index (SI) [21]: school closures; workplace closures; cancellation of public events; restrictions on public gatherings; closures of public transport; stay-at-home requirements; public information campaigns; restrictions on internal movements; and international travel controls. The index on any given day was calculated as the mean score of the nine indicators, each taking a value between 0 and 100 (100 = strictest). The mean SI (across all daily values) during the COVID-19 period was calculated and categorised as high (mean SI ≥ 68 (75th percentile (P75)) of SI of all countries with available data) versus medium/low (mean SI < 68).
- (ii).
- School closure (four categories: 0—No measures, 1—Recommend closing, 2—Require closing [only at some levels or categories, e.g., just high schools, or just public schools], 3—Require closing all levels) [22]. In our study, we calculated the proportion of days during the COVID-19 period with school closure requirements at all levels (Category 3), or only at certain levels or categories, e.g., secondary or public schools only (Category 2) versus recommend closing (Category 1) or no measures (Category 0). This proportion (i.e., 100 x number of days in Category 3 or 2 divided by the total number of days during COVID-19) was then calculated and categorised as high (≥88% [P75 of all countries with available data]) versus medium/low (<88%).
- (iii).
- Stay-at-home requirements (four categories: 0—No measures, 1—Recommend not leaving house, 2—Require not leaving house with exceptions for daily exercise, grocery shopping, and ‘essential’ trips, 3—Require not leaving house with minimal exceptions [e.g., allowed to leave only once every few days, or only one person can leave at a time, etc.]) [23]. In our study, we calculated the proportion of days with stay-at-home requirements including not leaving the house with minimal exceptions such as allowed to leave only once every few days, or only one person can leave at a time (Category 3), or not leaving the house with exceptions for daily exercise, grocery shopping and ‘essential’ trips (Category 2) versus recommend not leaving the house (Category 1) or no measures (Category 0). This proportion (i.e., 100 × number of days in Category 3 or 2 divided by the total number of days during COVID-19) was then calculated and categorised as high (≥65% (P75 of all countries with available data)) versus medium/low (<65%).
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pak, A.; Adegboye, O.A.; Adekunle, A.I.; Rahman, K.M.; McBryde, E.S.; Eisen, D.P. Economic Consequences of the COVID-19 Outbreak: The Need for Epidemic Preparedness. Front. Public Health 2020, 8, 241. [Google Scholar] [CrossRef]
- Hale, T.; Angrist, N.; Goldszmidt, R.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S.; Cameron-Blake, E.; Hallas, L.; Majumdar, S.; et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat. Hum. Behav. 2021, 5, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Miller, F.A.; Young, S.B.; Dobrow, M.; Shojania, K.G. Vulnerability of the medical product supply chain: The wake-up call of COVID-19. BMJ Qual. Saf. 2021, 30, 331–335. [Google Scholar] [CrossRef]
- Shukar, S.; Zahoor, F.; Hayat, K.; Saeed, A.; Gillani, A.H.; Omer, S.; Hu, S.; Babar, Z.U.; Fang, Y.; Yang, C. Drug Shortage: Causes, Impact, and Mitigation Strategies. Front. Pharm. 2021, 12, 693426. [Google Scholar] [CrossRef] [PubMed]
- Kretchy, I.A.; Asiedu-Danso, M.; Kretchy, J.P. Medication management and adherence during the COVID-19 pandemic: Perspectives and experiences from low-and middle-income countries. Res. Soc. Adm. Pharm. 2021, 17, 2023–2026. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.T.; Bussell, J.K. Medication adherence: WHO cares? Mayo. Clin. Proc. 2011, 86, 304–314. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez Arnao, M.D.; Rodriguez Sanchez, A.; Diez Lopez, I.; Ramirez Fernandez, J.; Bermudez de la Vega, J.A.; Yeste Fernandez, D.; Chueca Guindulain, M.; Corripio Collado, R.; Perez Sanchez, J.; Fernandez Gonzalez, A. Adherence and long-term outcomes of growth hormone therapy with easypod in pediatric subjects: Spanish ECOS study. Endocr. Connect 2019, 8, 1240–1249. [Google Scholar] [CrossRef]
- van Dommelen, P.; Koledova, E.; Wit, J.M. Effect of adherence to growth hormone treatment on 0–2 year catch-up growth in children with growth hormone deficiency. PLoS ONE 2018, 13, e0206009. [Google Scholar] [CrossRef]
- Giavoli, C.; Profka, E.; Giancola, N.; Rodari, G.; Giacchetti, F.; Ferrante, E.; Arosio, M.; Mantovani, G. Growth hormone therapy at the time of COVID-19 pandemic: Adherence and drug supply issues. Eur. J. Endocrinol. 2020, 183, L13–L15. [Google Scholar] [CrossRef]
- Mohseni, S.; Heydari, Z.; Qorbani, M.; Radfar, M. Adherence to growth hormone therapy in children and its potential barriers. J. Pediatr. Endocrinol. Metab. 2018, 31, 13–20. [Google Scholar] [CrossRef]
- Plevinsky, J.M.; Young, M.A.; Carmody, J.K.; Durkin, L.K.; Gamwell, K.L.; Klages, K.L.; Ghosh, S.; Hommel, K.A. The impact of COVID-19 on pediatric adherence and self-management. J. Pediatr. Psychol. 2020, 45, 977–982. [Google Scholar] [CrossRef]
- Bokolo Anthony, J. Use of telemedicine and virtual care for remote treatment in response to COVID-19 pandemic. J. Med. Syst. 2020, 44, 132. [Google Scholar] [CrossRef] [PubMed]
- van Heuckelum, M.; van den Ende, C.H.M.; Houterman, A.E.J.; Heemskerk, C.P.M.; van Dulmen, S.; van den Bemt, B.J.F. The effect of electronic monitoring feedback on medication adherence and clinical outcomes: A systematic review. PLoS ONE 2017, 12, e0185453. [Google Scholar] [CrossRef] [PubMed]
- Boman, N.; Fernandez-Luque, L.; Koledova, E.; Kause, M.; Lapatto, R. Connected health for growth hormone treatment research and clinical practice: Learnings from different sources of real-world evidence (RWE)-large electronically collected datasets, surveillance studies and individual patients’ cases. BMC Med. Inf. Decis. Mak. 2021, 21, 136. [Google Scholar] [CrossRef]
- Koledova, E.; Stoyanov, G.; Ovbude, L.; Davies, P.S.W. Adherence and long-term growth outcomes: Results from the easypod() connect observational study (ECOS) in paediatric patients with growth disorders. Endocr. Connect 2018, 7, 914–923. [Google Scholar] [CrossRef]
- Koledova, E.; Tornincasa, V.; van Dommelen, P. Analysis of real-world data on growth hormone therapy adherence using a connected injection device. BMC Med. Inf. Decis. Mak. 2020, 20, 176. [Google Scholar] [CrossRef]
- Omoloja, A.; Vundavalli, S. Patient generated health data: Benefits and challenges. Curr. Probl. Pediatr. Adolesc. Health Care 2021, 51, 101103. [Google Scholar] [CrossRef] [PubMed]
- Budd, J.; Miller, B.S.; Manning, E.M.; Lampos, V.; Zhuang, M.; Edelstein, M.; Rees, G.; Emery, V.C.; Stevens, M.M.; Keegan, N.; et al. Digital technologies in the public-health response to COVID-19. Nat. Med. 2020, 26, 1183–1192. [Google Scholar] [CrossRef]
- Norozi, S.A.; Moen, T. Childhood as a social construction. J. Educ. Soc. Res. 2016, 6, 75–80. [Google Scholar] [CrossRef]
- Our World in Data. Available online: https://ourworldindata.org/ (accessed on 7 March 2023).
- Our World in Data. COVID-19: Stringency Index. Available online: https://ourworldindata.org/covid-stringency-index (accessed on 7 March 2023).
- Our World in Data. School Closures during the COVID-19 Pandemic. Available online: https://ourworldindata.org/grapher/school-closures-covid (accessed on 7 March 2023).
- Our World in Data. COVID-19: Stay-at-Home Restrictions. Available online: https://ourworldindata.org/covid-stay-home-restrictions (accessed on 7 March 2023).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: http://www.r-project.org/index.html (accessed on 7 March 2023).
- Aston, J.; Wilson, K.A.; Terry, D.R.P. The treatment-related experiences of parents, children and young people with regular prescribed medication. Int. J. Clin. Pharm. 2019, 41, 113–121. [Google Scholar] [CrossRef]
- Brod, M.; Hojbjerre, L.; Alolga, S.L.; Beck, J.F.; Wilkinson, L.; Rasmussen, M.H. Understanding Treatment Burden for Children Treated for Growth Hormone Deficiency. Patient 2017, 10, 653–666. [Google Scholar] [CrossRef] [PubMed]
- Leggett, C.; Giles, L.; Anderson, J.J.A.; Doogue, M.; Couper, J.; Pena, A.S. Adherence to metformin is reduced during school holidays and weekends in children with type 1 diabetes participating in a randomised controlled trial. Arch Dis. Child 2019, 104, 890–894. [Google Scholar] [CrossRef]
- McQuaid, E.L.; Landier, W. Cultural issues in medication adherence: Disparities and directions. J. Gen. Intern Med. 2018, 33, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Eyawo, O.; Viens, A.M.; Ugoji, U.C. Lockdowns and low- and middle-income countries: Building a feasible, effective, and ethical COVID-19 response strategy. Glob. Health 2021, 17, 13. [Google Scholar] [CrossRef]
- Petherick, A.; Goldszmidt, R.; Andrade, E.B.; Furst, R.; Hale, T.; Pott, A.; Wood, A. A worldwide assessment of changes in adherence to COVID-19 protective behaviours and hypothesized pandemic fatigue. Nat. Hum. Behav. 2021, 5, 1145–1160. [Google Scholar] [CrossRef]
- The World Bank. List of Countries by GNI (Nominal) Per Capita. Available online: https://data.worldbank.org/indicator/ny.gnp.pcap.cd?year_high_desc=true (accessed on 7 March 2023).
- Sheikh, A.; Sheikh, Z.; Sheikh, A. Novel approaches to estimate compliance with lockdown measures in the COVID-19 pandemic. J. Glob. Health 2020, 10, 010348. [Google Scholar] [CrossRef] [PubMed]
- Google: COVID-19 Community Mobility Reports. Available online: https://www.google.com/covid19/mobility/ (accessed on 7 March 2023).
- Malik, S.; Moloney, C.; Koledova, E.; Reston, J.; Weinman, J. Designing a Personalized Digital Patient Support Program for Patients Treated with Growth Hormone: Key Design Considerations. J. Med. Internet. Res. 2020, 22, e18157. [Google Scholar] [CrossRef] [PubMed]
- Cuddy, A.J.; Wolf, E.B.; Glick, P.; Crotty, S.; Chong, J.; Norton, M.I. Men as cultural ideals: Cultural values moderate gender stereotype content. J. Pers. Soc. Psychol. 2015, 109, 622–635. [Google Scholar] [CrossRef]
- Donker, M.H.; Mastrotheodoros, S.; Branje, S. Development of parent-adolescent relationships during the COVID-19 pandemic: The role of stress and coping. Dev. Psychol. 2021, 57, 1611–1622. [Google Scholar] [CrossRef]
- Kapetanovic, S.; Gurdal, S.; Ander, B.; Sorbring, E. Reported Changes in Adolescent Psychosocial Functioning during the COVID-19 Outbreak. Adolescents 2021, 1, 10–20. [Google Scholar] [CrossRef]
- Czeisler, M.É.; Marynak, K.; Clarke, K.E.N.; Salah, Z.; Shakya, I.; Thierry, J.M.; Ali, N.; McMillan, H.; Wiley, J.F.; Weaver, M.D.; et al. Delay or Avoidance of Medical Care Because of COVID-19-Related Concerns—United States, June 2020. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 1250–1257. [Google Scholar] [CrossRef] [PubMed]
- Mehrotra, A.; Chernew, M.; Linetsky, D.; Hatch, H.; Cutler, D.; Schneider, E.C. The Impact of the COVID-19 Pandemic on Outpatient Care: Visits Return to Prepandemic Levels, but not for all Providers and Patients. 2020. Available online: https://www.commonwealthfund.org/publications/2020/oct/impact-covid-19-pandemic-outpatient-care-visits-return-prepandemic-levels (accessed on 7 March 2023).
- Gomez, R.; Ahmed, S.F.; Maghnie, M.; Li, D.; Tanaka, T.; Miller, B.S. Treatment Adherence to Injectable Treatments in Pediatric Growth Hormone Deficiency Compared with Injectable Treatments in Other Chronic Pediatric Conditions: A Systematic Literature Review. Front. Endocrinol. 2021, 13, 795224. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Country | Before COVID-19 a | During COVID-19 b | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Boys (%) | Girls (%) | Age (Years) Mean (SD) | Time on Treatment Halfway through This Period (Years) Mean | N | Boys (%) | Girls (%) | Age (Years) Mean (SD) | Time on Treatment Halfway through This Period (Years) Mean | |
| Czech Republic | 341 | 66 | 34 | 11.6 (3.1) | 3.1 | 351 | 67 | 33 | 11.7 (3.0) | 3.4 |
| Finland | 104 | 73 | 27 | 11.1 (3.1) | 2.8 | 108 | 69 | 31 | 11.2 (3.3) | 3.2 |
| France | 390 | 64 | 36 | 12.2 (2.7) | 2.3 | 375 | 64 | 36 | 12.1 (2.8) | 2.3 |
| Germany | 798 | 60 | 40 | 11.6 (3.1) | 3.0 | 734 | 62 | 38 | 11.5 (3.1) | 3.2 |
| Ireland | 74 | 70 | 30 | 12.1 (3.0) | 1.5 | 76 | 68 | 32 | 12.5 (3.0) | 2.2 |
| Italy | 281 | 56 | 44 | 12.2 (2.7) | 1.9 | 282 | 56 | 44 | 12.3 (2.7) | 2.0 |
| Spain | 2528 | 55 | 45 | 11.4 (2.8) | 1.8 | 2665 | 54 | 46 | 11.5 (2.8) | 2.0 |
| Sweden | 122 | 65 | 35 | 12.1 (2.9) | 4.7 | 99 | 64 | 36 | 12.1 (3.1) | 4.8 |
| Switzerland | 132 | 72 | 28 | 12.4 (3.1) | 2.5 | 139 | 69 | 31 | 12.7 (3.1) | 2.8 |
| United Kingdom | 540 | 61 | 39 | 11.6 (3.0) | 2.8 | 513 | 61 | 39 | 11.8 (3.1) | 3.1 |
| Argentina | 847 | 65 | 36 | 11.4 (2.9) | 1.3 | 991 | 64 | 36 | 11.6 (2.9) | 1.8 |
| Brazil | 189 | 60 | 40 | 11.1 (2.6) | 1.4 | 93 | 60 | 40 | 11.0 (2.5) | 1.8 |
| Chile | 689 | 57 | 43 | 11.9 (2.6) | 1.5 | 130 | 52 | 48 | 12.2 (2.4) | 2.2 |
| Colombia | 858 | 55 | 45 | 11.9 (2.6) | 1.4 | 293 | 55 | 45 | 11.9 (2.7) | 1.7 |
| Guatemala | 190 | 49 | 51 | 12.0 (2.6) | 1.2 | 111 | 50 | 50 | 12.3 (2.7) | 1.6 |
| Peru | 263 | 49 | 51 | 11.4 (2.7) | 1.0 | 76 | 54 | 46 | 11.4 (2.9) | 1.8 |
| Taiwan | 467 | 58 | 42 | 12.5 (2.3) | 1.0 | 445 | 58 | 42 | 12.6 (2.2) | 1.3 |
| Canada | 102 | 59 | 41 | 11.7 (2.9) | 1.1 | 125 | 58 | 42 | 11.9 (2.8) | 1.1 |
| Before COVID-19 a | During COVID-19 b | Difference during-before | ||||
|---|---|---|---|---|---|---|
| Country | Optimal (≥85%) Adherence (%) | Optimal (≥85%) Adherence (%) | Stringency Index (Mean [SD]) | Proportion of Time with Required School Closure (%) | Proportion of Time with Required Stay at Home (%) | Change in Optimal (≥85%) Adherence (%) |
| Czech Republic | 88 | 91 | 56 (18) | 68 | 36 | 3 |
| Finland | 77 | 74 | 46 (14) | 40 | 0 | −3 |
| France | 83 | 88 | 64 (15) | 60 | 52 | 5 |
| Germany | 80 | 85 | 64 (14) | 63 | 36 | 5 |
| Ireland | 70 | 76 | 70 (20) | 88 | 48 | 6 |
| Italy | 82 | 90 | 70 (15) | 94 | 53 | 8 |
| Spain | 83 | 80 | 67 (13) | 66 | 62 | −3 |
| Sweden | 81 | 86 | 60 (10) | 65 | 0 | 5 |
| Switzerland | 75 | 74 | 52 (13) | 48 | 0 | −1 |
| United Kingdom | 66 | 73 | 70 (16) | 73 | 38 | 7 |
| Argentina | 62 | 65 | 83 (16) | 96 | 95 | 2 |
| Brazil | 83 | 78 | 68 (13) | 97 | 82 | −4 |
| Chile | 68 | 74 | 76 (16) | 96 | 93 | 6 |
| Colombia | 54 | 71 | 75 (16) | 96 | 58 | 18 |
| Guatemala | 72 | 85 | 71 (23) | 96 | 53 | 13 |
| Peru | 67 | 66 | 80 (16) | 97 | 96 | −1 |
| Taiwan | 69 | 66 | 25 (3) | 0 | 0 | −3 |
| Canada | 88 | 89 | 67 (13) | 96 | 14 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Dommelen, P.; Baños, R.M.; Arnaud, L.; Le Masne, Q.; Koledova, E. The Impact of COVID-19 Regulations on Adherence to Recombinant Human Growth Hormone Therapy: Evidence from Real-World Data. Endocrines 2023, 4, 194-204. https://doi.org/10.3390/endocrines4010017
van Dommelen P, Baños RM, Arnaud L, Le Masne Q, Koledova E. The Impact of COVID-19 Regulations on Adherence to Recombinant Human Growth Hormone Therapy: Evidence from Real-World Data. Endocrines. 2023; 4(1):194-204. https://doi.org/10.3390/endocrines4010017
Chicago/Turabian Stylevan Dommelen, Paula, Rosa Maria Baños, Lilian Arnaud, Quentin Le Masne, and Ekaterina Koledova. 2023. "The Impact of COVID-19 Regulations on Adherence to Recombinant Human Growth Hormone Therapy: Evidence from Real-World Data" Endocrines 4, no. 1: 194-204. https://doi.org/10.3390/endocrines4010017
APA Stylevan Dommelen, P., Baños, R. M., Arnaud, L., Le Masne, Q., & Koledova, E. (2023). The Impact of COVID-19 Regulations on Adherence to Recombinant Human Growth Hormone Therapy: Evidence from Real-World Data. Endocrines, 4(1), 194-204. https://doi.org/10.3390/endocrines4010017