


Diabetic Ketoacidosis Management: Updates and Challenges for Specific Patient Population


Highlights
- Diabetic ketoacidosis (DKA) requires hospitalization for aggressive fluid replacement, electrolyte management, and insulin therapy.
- The major precipitating factors for DKA include a new diagnosis of diabetes, non-adherence to insulin therapy, and infections such as sepsis in patients with diabetes.
- Patient education and appropriate insulin dosing are key to preventing recurrence. Special patient populations, such as those with pregnancy, renal failure, acute pancreatitis, or insulin pump users, should be carefully considered.
- Our review demonstrates that the management of DKA remains standard, even in special patient populations such as those with pregnancy, acute pancreatitis, and, to a certain extent, patients on renal replacement therapy or with congestive heart failure.
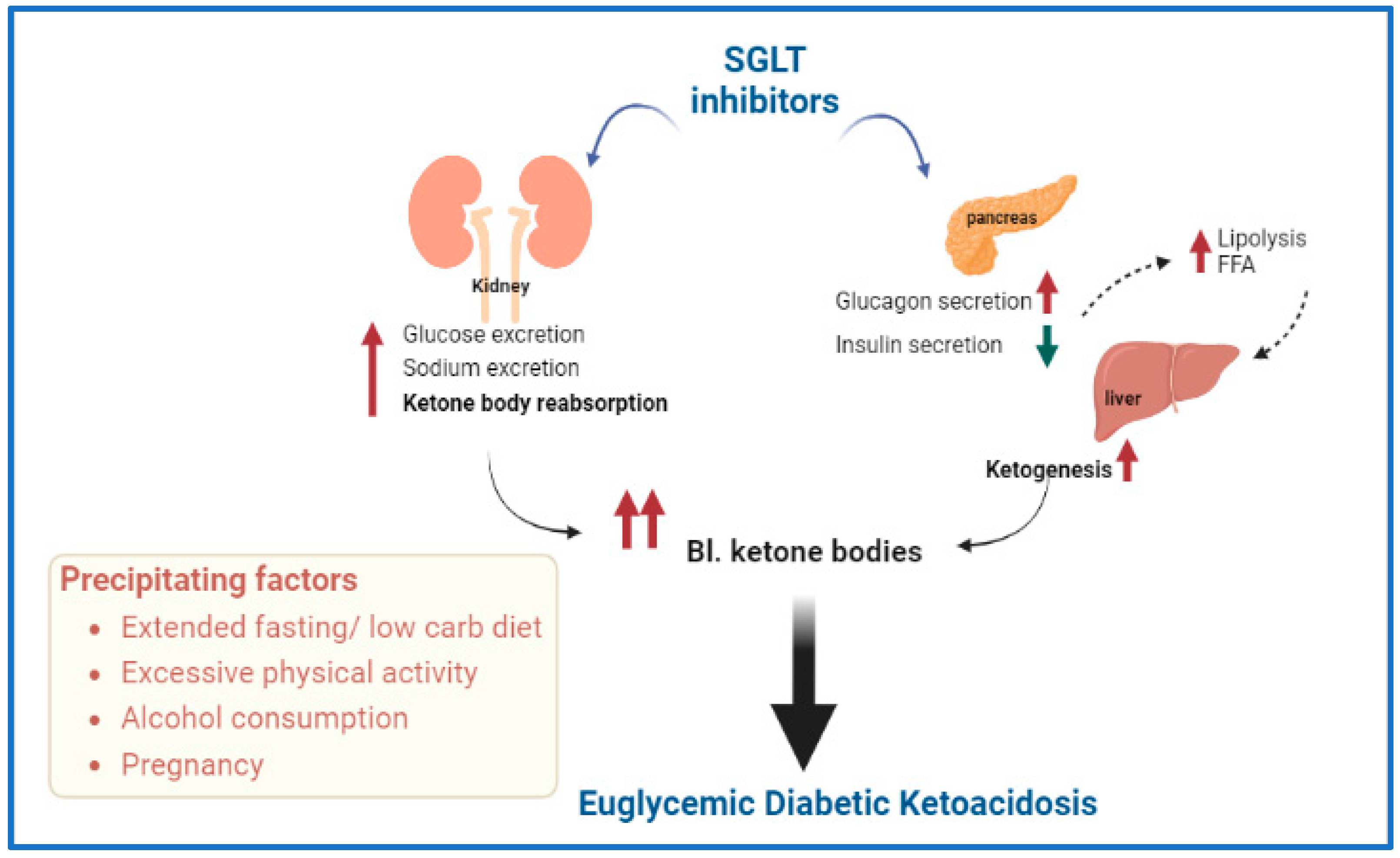
- Euglycemic DKA and ketonemia are on the rise with the increased use of Sodium–Glucose Cotransporter (SGLT) inhibitors. Patients are advised to follow the STICH protocol (STop SGLT inhibitor, Insulin administration, Carbohydrate consumption, Hydration).
- Patients with COVID-19 exhibit elevated levels of proinflammatory markers similar to those seen in DKA; however, no causal relationship has been established.
Abstract
1. Introduction
1.1. Diabetic Ketoacidosis (DKA)
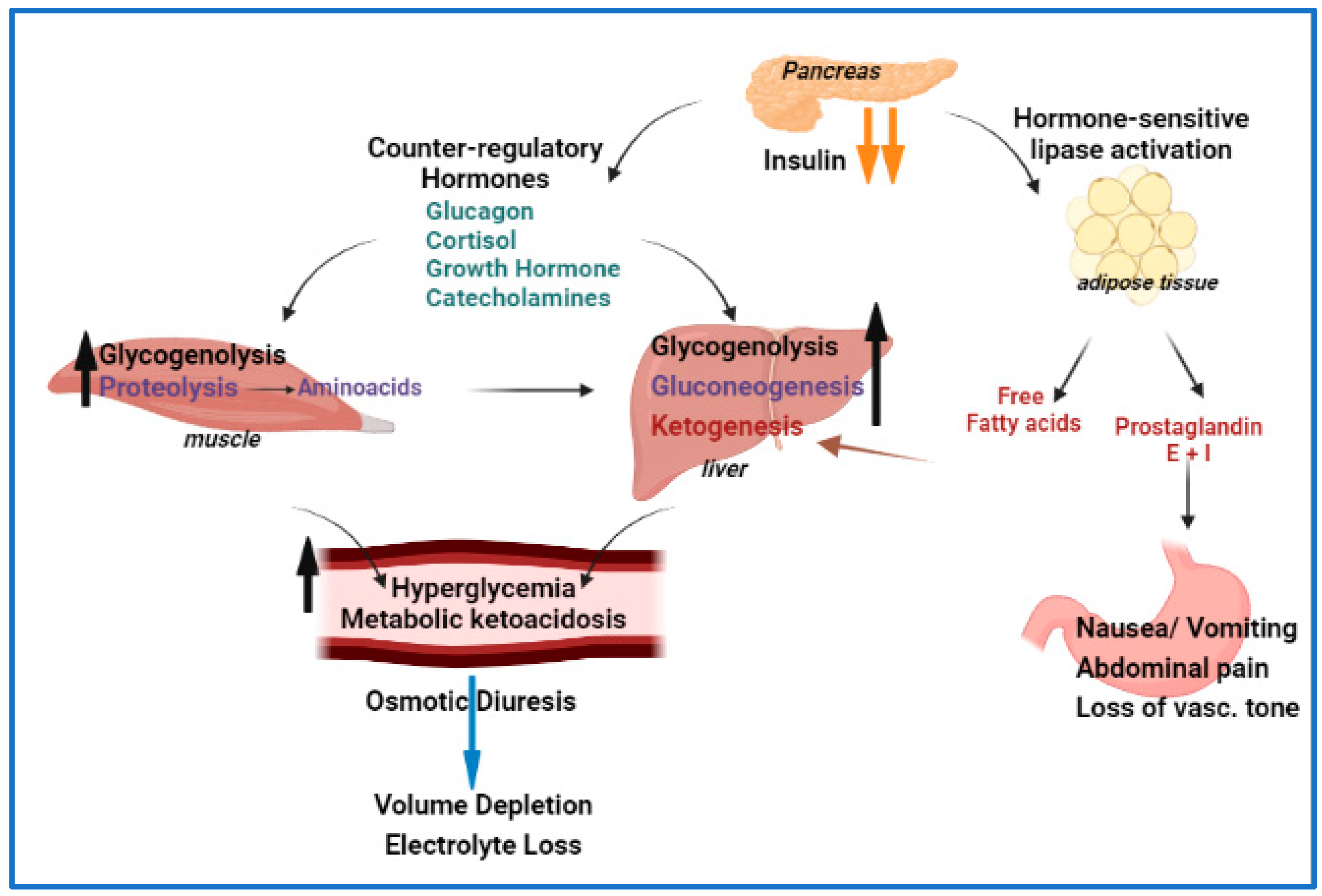
1.2. Pathophysiology of DKA
1.3. DKA Presentation and Diagnosis
2. Management of DKA
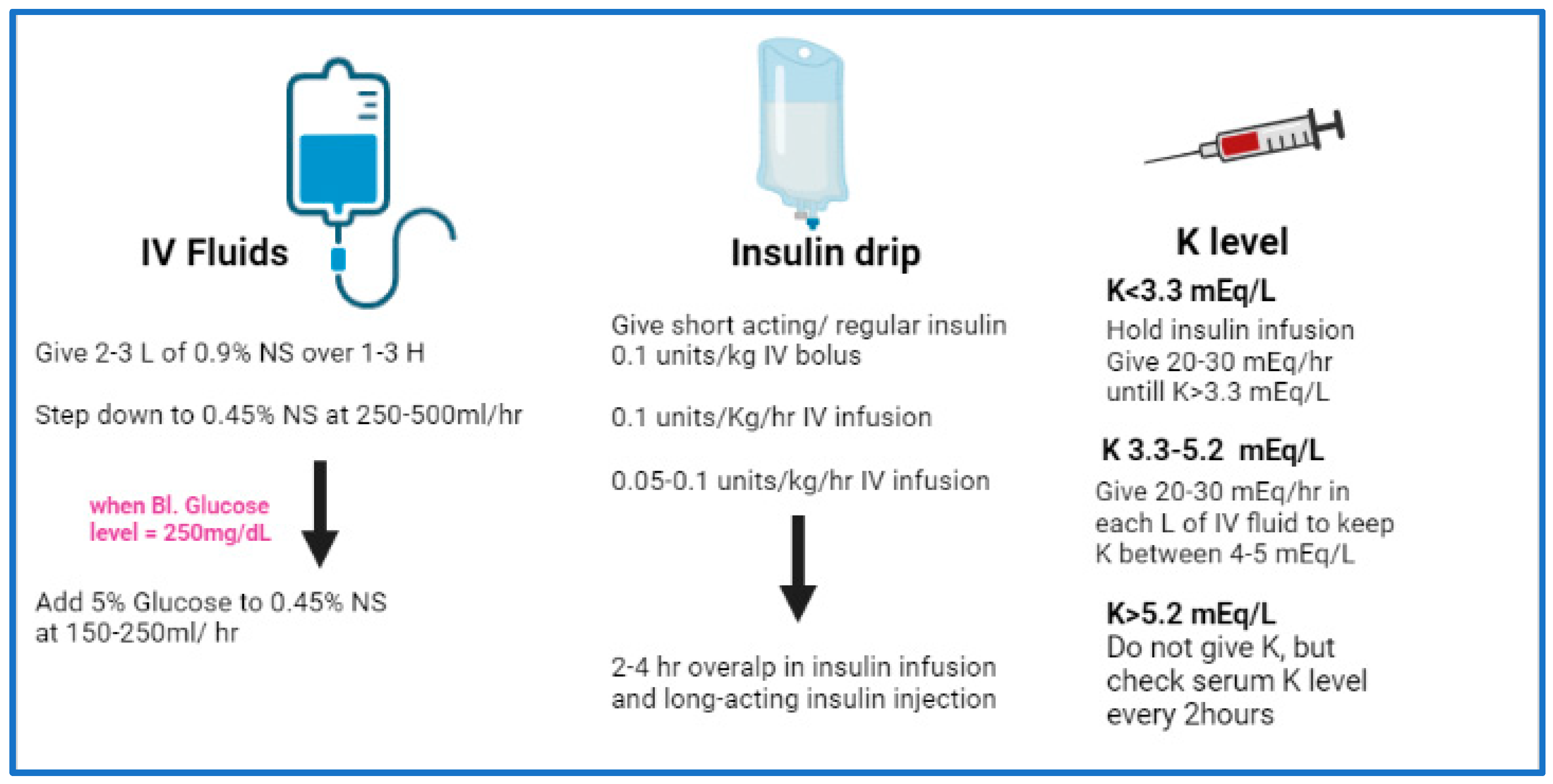
2.1. Standard Treatment of DKA
2.2. Treatment–Fluid Therapy
2.3. Treatment–Insulin Therapy
2.4. Treatment-Potassium
3. DKA in Special Population
3.1. DKA in Pregnancy
3.2. DKA in Renal Replacement
3.3. DKA in Acute Pancreatitis and Islets Transplants
3.4. DKA and Sodium–Glucose Cotransporter (SGLT) Inhibitors
3.5. DKA in Patients with Congestive Heart Failure (CHF)
3.6. DKA and Insulin Pump Users
3.7. DKA in Patients with COVID-19
4. Summary and Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kitabchi, A.E.; Umpierrez, G.E.; Miles, J.M.; Fisher, J.N. Hyperglycemic crises in adult patients with diabetes. Diabetes Care 2009, 32, 1335–1343. [Google Scholar] [CrossRef] [PubMed]
- Kichloo, A.; El-Amir, Z.; Wani, F.; Shaka, H. Hospitalizations for ketoacidosis in type 1 diabetes mellitus, 2008 to 2018. Bayl. Univ. Med. Cent. Proc. 2022, 35, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Benoit, S.R.; Zhang, Y.; Geiss, L.S.; Gregg, E.W.; Albright, A. Trends in Diabetic Ketoacidosis Hospitalizations and In-Hospital Mortality—United States, 2000–2014. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 362–365. [Google Scholar] [CrossRef] [PubMed]
- Sudhanshu, S.; Jevalikar, G.; Das, P.K.; Singh, P.K.; Bhatia, E.; Bhatia, V. Acute Respiratory Distress Syndrome: A Rare Complication in Pediatric Diabetic Ketoacidosis. Indian J. Pediatr. 2016, 83, 463–465. [Google Scholar] [CrossRef] [PubMed]
- Gosmanov, A.R.; Gosmanova, E.O.; Dillard-Cannon, E. Management of adult diabetic ketoacidosis. Diabetes Metab. Syndr. Obes. 2014, 7, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Chatzipanteli, K.; Head, C.; Megerman, J.; Axelrod, L. The relationship between plasma insulin level, prostaglandin production by adipose tissue, and blood pressure in normal rats and rats with diabetes mellitus and diabetic ketoacidosis. Metabolism 1996, 45, 691–698. [Google Scholar] [CrossRef]
- Tzamaloukas, A.H.; Rohrscheib, M.; Ing, T.S.; Siamopoulos, K.C.; Qualls, C.; Elisaf, M.S.; Vanderjagt, D.J.; Spalding, C.T. Serum potassium and acid-base parameters in severe dialysis-associated hyperglycemia treated with insulin therapy. Int. J. Artif. Organs 2005, 28, 229–236. [Google Scholar] [CrossRef]
- Nyenwe, E.A.; Kitabchi, A.E. Evidence-based management of hyperglycemic emergencies in diabetes mellitus. Diabetes Res. Clin. Pract. 2011, 94, 340–351. [Google Scholar] [CrossRef]
- Umpierrez, G.E.; Jones, S.; Smiley, D.; Mulligan, P.; Keyler, T.; Temponi, A.; Semakula, C.; Umpierrez, D.; Peng, L.; Ceron, M.; et al. Insulin analogs versus human insulin in the treatment of patients with diabetic ketoacidosis: A randomized controlled trial. Diabetes Care 2009, 32, 1164–1169. [Google Scholar] [CrossRef]
- Islam, T.; Sherani, K.; Surani, S.; Vakil, A. Guidelines and controversies in the management of diabetic ketoacidosis—A mini-review. World J. Diabetes 2018, 9, 226–229. [Google Scholar] [CrossRef]
- Munir, I.; Fargo, R.; Garrison, R.; Yang, A.; Cheng, A.; Kang, I.; Motabar, A.; Xu, K.; Loo, L.K.; Kim, D.I. Comparison of a ‘two-bag system’ versus conventional treatment protocol (‘one-bag system’) in the management of diabetic ketoacidosis. BMJ Open Diabetes Res. Care 2017, 5, e000395. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.N.; Shahshahani, M.N.; Kitabchi, A.E. Diabetic ketoacidosis: Low-dose insulin therapy by various routes. N. Engl. J. Med. 1977, 297, 238–241. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.; Hockaday, T.D.; Turner, R.C. Small doses of intramuscular insulin in the treatment of diabetic “coma”. Lancet 1973, 2, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Gupta, M.; Gunn, S. Use of Inhaled Insulin in a Patient with Subcutaneous Insulin Resistance Syndrome: A Rare Condition. AACE Clin. Case Rep. 2019, 5, e187–e191. [Google Scholar] [CrossRef] [PubMed]
- Kitabchi, A.E.; Umpierrez, G.E.; Fisher, J.N.; Murphy, M.B.; Stentz, F.B. Thirty years of personal experience in hyperglycemic crises: Diabetic ketoacidosis and hyperglycemic hyperosmolar state. J. Clin. Endocrinol. Metab. 2008, 93, 1541–1552. [Google Scholar] [CrossRef]
- Kitabchi, A.E.; Murphy, M.B.; Spencer, J.; Matteri, R.; Karas, J. Is a priming dose of insulin necessary in a low-dose insulin protocol for the treatment of diabetic ketoacidosis? Diabetes Care 2008, 31, 2081–2085. [Google Scholar] [CrossRef]
- Umpierrez, G.E.; Latif, K.; Stoever, J.; Cuervo, R.; Park, L.; Freire, A.X.; Kitabchi, A.E. Efficacy of subcutaneous insulin lispro versus continuous intravenous regular insulin for the treatment of patients with diabetic ketoacidosis. Am. J. Med. 2004, 117, 291–296. [Google Scholar] [CrossRef]
- Andrade-Castellanos, C.A.; Colunga-Lozano, L.E.; Delgado-Figueroa, N.; Gonzalez-Padilla, D.A. Subcutaneous rapid-acting insulin analogues for diabetic ketoacidosis. Cochrane Database Syst. Rev. 2016, 2016, CD011281. [Google Scholar] [CrossRef]
- Eledrisi, M.S.; Beshyah, S.A.; Malik, R.A. Management of diabetic ketoacidosis in special populations. Diabetes Res. Clin. Pract. 2021, 174, 108744. [Google Scholar] [CrossRef]
- Kitabchi, A.E.; Umpierrez, G.E.; Murphy, M.B.; Kreisberg, R.A. Hyperglycemic crises in adult patients with diabetes: A consensus statement from the American Diabetes Association. Diabetes Care 2006, 29, 2739–2748. [Google Scholar] [CrossRef]
- Sibai, B.M.; Viteri, O.A. Diabetic ketoacidosis in pregnancy. Obstet. Gynecol. 2014, 123, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Diguisto, C.; Strachan, M.W.J.; Churchill, D.; Ayman, G.; Knight, M. A study of diabetic ketoacidosis in the pregnant population in the United Kingdom: Investigating the incidence, aetiology, management and outcomes. Diabet. Med. 2022, 39, e14743. [Google Scholar] [CrossRef] [PubMed]
- ohan, M.; Baagar, K.A.M.; Lindow, S. Management of diabetic ketoacidosis in pregnancy. Obstet. Gynaecol. 2017, 19, 55–62. [Google Scholar] [CrossRef]
- Koye, D.N.; Magliano, D.J.; Nelson, R.G.; Pavkov, M.E. The Global Epidemiology of Diabetes and Kidney Disease. Adv. Chronic Kidney Dis. 2018, 25, 121–132. [Google Scholar] [CrossRef]
- Seddik, A.A.; Bashier, A.; Alhadari, A.K.; AlAlawi, F.; Alnour, H.H.; Bin Hussain, A.A.; Frankel, A.; Railey, M.J. Challenges in management of diabetic ketoacidosis in hemodialysis patients, case presentation and review of literature. Diabetes Metab. Syndr. 2019, 13, 2481–2487. [Google Scholar] [CrossRef]
- Tzamaloukas, A.H.; Ing, T.S.; Siamopoulos, K.C.; Rohrscheib, M.; Elisaf, M.S.; Raj, D.S.; Murata, G.H. Body fluid abnormalities in severe hyperglycemia in patients on chronic dialysis: Review of published reports. J. Diabetes Its Complicat. 2008, 22, 29–37. [Google Scholar] [CrossRef]
- Galindo, R.J.; Pasquel, F.J.; Fayfman, M.; Tsegka, K.; Dhruv, N.; Cardona, S.; Wang, H.; Vellanki, P.; Umpierrez, G.E. Clinical characteristics and outcomes of patients with end-stage renal disease hospitalized with diabetes ketoacidosis. BMJ Open Diabetes Res. Care 2020, 8, e000763. [Google Scholar] [CrossRef]
- Tzamaloukas, A.H.; Ing, T.S.; Siamopoulos, K.C.; Raj, D.S.; Elisaf, M.S.; Rohrscheib, M.; Murata, G.H. Pathophysiology and management of fluid and electrolyte disturbances in patients on chronic dialysis with severe hyperglycemia. Semin. Dial. 2008, 21, 431–439. [Google Scholar] [CrossRef]
- Mathuram Thiyagarajan, U.; Ponnuswamy, A.; Chung, A. An enigmatic triad of acute pancreatitis, diabetic ketoacidosis and hypertriglyceridaemia: Who is the culprit? BMJ Case Rep. 2019, 12, e217272. [Google Scholar] [CrossRef]
- Scherer, J.; Singh, V.P.; Pitchumoni, C.S.; Yadav, D. Issues in hypertriglyceridemic pancreatitis: An update. J. Clin. Gastroenterol. 2014, 48, 195–203. [Google Scholar] [CrossRef]
- Wang, Y.; Attar, B.M.; Hinami, K.; Jaiswal, P.; Yap, J.E.; Jaiswal, R.; Devani, K.; Simons-Linares, C.R.; Demetria, M.V. Concurrent Diabetic Ketoacidosis in Hypertriglyceridemia-Induced Pancreatitis: How Does It Affect the Clinical Course and Severity Scores? Pancreas 2017, 46, 1336–1340. [Google Scholar] [CrossRef]
- Nair, S.; Yadav, D.; Pitchumoni, C.S. Association of diabetic ketoacidosis and acute pancreatitis: Observations in 100 consecutive episodes of DKA. Am. J. Gastroenterol. 2000, 95, 2795–2800. [Google Scholar] [CrossRef] [PubMed]
- Singla, A.A.; Ting, F.; Singla, A. Acute pancreatitis secondary to diabetic ketoacidosis induced hypertriglyceridemia in a young adult with undiagnosed type 2 diabetes. JOP. J. Pancreas 2015, 16, 201–204. [Google Scholar] [CrossRef]
- Ravindran, D.; Mugunthan, R.S.R.; Shruthi, T.K.; Jayaraman, D. Severe diabetic ketoacidosis and autoimmune pancreatitis with SIRS in an adolescent with LRBA deficiency—A rare complication of a common primary immunodeficiency disease. J. Fam. Med. Prim. Care 2022, 11, 1552–1554. [Google Scholar] [CrossRef]
- Yilmaz-Yalcin, Y.; Bascil-Tutuncu, N.; Baysan-Cebi, H.P.; Verdi, H.; Erol, S.; Kaymaz, F.F.; Atac, F.B. A Lipotoxic Medium Decreases the Number of Lipid Droplets in beta Cells: One Possible Explanation of the beta-Cell Failure in Patients with Hyperlipidemia Receiving Tacrolimus. Exp. Clin. Transplant. epub before print. 2022. [Google Scholar] [CrossRef]
- Porrini, E.L.; Diaz, J.M.; Moreso, F.; Delgado Mallen, P.I.; Silva Torres, I.; Ibernon, M.; Bayes-Genis, B.; Benitez-Ruiz, R.; Lampreabe, I.; Lauzurrica, R.; et al. Clinical evolution of post-transplant diabetes mellitus. Nephrol. Dial. Transplant. 2016, 31, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Mazumder, M.A.; Gulati, S.; Narula, A.S.; Shehwar, D.; Mir, I.M. Tacrolimus-induced acute pancreatitis and diabetic ketoacidosis (DKA) in pediatric kidney transplant recipient. Pediatr. Transplant. 2022, 26, e14194. [Google Scholar] [CrossRef]
- Rickels, M.R.; Robertson, R.P. Pancreatic Islet Transplantation in Humans: Recent Progress and Future Directions. Endocr. Rev. 2019, 40, 631–668. [Google Scholar] [CrossRef]
- Rickels, M.R.; Stock, P.G.; de Koning, E.J.P.; Piemonti, L.; Pratschke, J.; Alejandro, R.; Bellin, M.D.; Berney, T.; Choudhary, P.; Johnson, P.R.; et al. Defining outcomes for beta-cell replacement therapy in the treatment of diabetes: A consensus report on the Igls criteria from the IPITA/EPITA opinion leaders workshop. Transpl. Int. 2018, 31, 343–352. [Google Scholar] [CrossRef]
- Hering, B.J.; Clarke, W.R.; Bridges, N.D.; Eggerman, T.L.; Alejandro, R.; Bellin, M.D.; Chaloner, K.; Czarniecki, C.W.; Goldstein, J.S.; Hunsicker, L.G.; et al. Phase 3 Trial of Transplantation of Human Islets in Type 1 Diabetes Complicated by Severe Hypoglycemia. Diabetes Care 2016, 39, 1230–1240. [Google Scholar] [CrossRef]
- Lyons, S.K.; Hermann, J.M.; Miller, K.M.; Hofer, S.E.; Foster, N.C.; Rami-Merhar, B.M.; Aleppo, G.; Seufert, J.; DiMeglio, L.A.; Danne, T.; et al. Use of Adjuvant Pharmacotherapy in Type 1 Diabetes: International Comparison of 49,996 Individuals in the Prospective Diabetes Follow-up and T1D Exchange Registries. Diabetes Care 2017, 40, e139–e140. [Google Scholar] [CrossRef]
- Sarafidis, P.; Loutradis, C.; Ferro, C.J.; Ortiz, A. SGLT-2 Inhibitors to Treat Hyponatremia Associated with SIADH: A Novel Indication? Am. J. Nephrol. 2020, 51, 553–555. [Google Scholar] [CrossRef] [PubMed]
- Loutradis, C.; Papadopoulou, E.; Angeloudi, E.; Karagiannis, A.; Sarafidis, P. The Beneficial Hemodynamic Actions of SGLT-2 Inhibitors beyond the Management of Hyperglycemia. Curr. Med. Chem. 2020, 27, 6682–6702. [Google Scholar] [CrossRef] [PubMed]
- Refardt, J.; Imber, C.; Sailer, C.O.; Jeanloz, N.; Potasso, L.; Kutz, A.; Widmer, A.; Urwyler, S.A.; Ebrahimi, F.; Vogt, D.R.; et al. A Randomized Trial of Empagliflozin to Increase Plasma Sodium Levels in Patients with the Syndrome of Inappropriate Antidiuresis. J. Am. Soc. Nephrol. 2020, 31, 615–624. [Google Scholar] [CrossRef]
- Yeoh, S.E.; Docherty, K.F.; Jhund, P.S.; Petrie, M.C.; Inzucchi, S.E.; Kober, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; et al. Relationship of Dapagliflozin with Serum Sodium: Findings From the DAPA-HF Trial. JACC Heart Fail. 2022, 10, 306–318. [Google Scholar] [CrossRef]
- Dhanasekaran, M.; Narayanan, S.; Mastoris, I.; Mehta, S. Canagliflozin-associated severe hyponatremia: A rare and potentially adverse effect? Endocrinol. Diabetes Metab. Case Rep. 2022, 2022, 21-0035. [Google Scholar] [CrossRef] [PubMed]
- Branco, A.; Fatima, R.; Liblik, K.; Jackson, R.; Payne, D.; El-Diasty, M. Euglycemic Diabetic Ketoacidosis Associated with Sodium-Glucose Cotransporter-2 Inhibitors After Cardiac Surgery: A Review of Current Literature. J. Cardiothorac. Vasc. Anesthesia 2022, 36, 3877–3886. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, W.; Sakaguchi, K. Euglycemic diabetic ketoacidosis induced by SGLT2 inhibitors: Possible mechanism and contributing factors. J. Diabetes Investig. 2016, 7, 135–138. [Google Scholar] [CrossRef]
- Teng, R.; Kurian, M.; Close, K.L.; Buse, J.B.; Peters, A.L.; Alexander, C.M. Comparison of Protocols to Reduce Diabetic Ketoacidosis in Patients with Type 1 Diabetes Prescribed a Sodium-Glucose Cotransporter 2 Inhibitor. Diabetes Spectr. 2021, 34, 42–51. [Google Scholar] [CrossRef]
- Goldenberg, R.M.; Gilbert, J.D.; Hramiak, I.M.; Woo, V.C.; Zinman, B. Sodium-glucose co-transporter inhibitors, their role in type 1 diabetes treatment and a risk mitigation strategy for preventing diabetic ketoacidosis: The STOP DKA Protocol. Diabetes Obes. Metab. 2019, 21, 2192–2202. [Google Scholar] [CrossRef]
- Klocker, A.A.; Phelan, H.; Twigg, S.M.; Craig, M.E. Blood beta-hydroxybutyrate vs. urine acetoacetate testing for the prevention and management of ketoacidosis in Type 1 diabetes: A systematic review. Diabet. Med. 2013, 30, 818–824. [Google Scholar] [CrossRef]
- Westcott, G.P.; Segal, A.R.; Mitri, J.; Brown, F.M. Prolonged glucosuria and relapse of diabetic ketoacidosis related to SGLT2-inhibitor therapy. Endocrinol. Diabetes Metab. 2020, 3, e00117. [Google Scholar] [CrossRef] [PubMed]
- Ekanayake, P.; Hupfeld, C.; Mudaliar, S. Sodium-Glucose Cotransporter Type 2 (SGLT-2) Inhibitors and Ketogenesis: The Good and the Bad. Curr. Diabetes Rep. 2020, 20, 74. [Google Scholar] [CrossRef] [PubMed]
- Blau, J.E.; Tella, S.H.; Taylor, S.I.; Rother, K.I. Ketoacidosis associated with SGLT2 inhibitor treatment: Analysis of FAERS data. Diabetes Res. Rev. 2017, 33, e2924. [Google Scholar] [CrossRef]
- Weissberg-Benchell, J.; Antisdel-Lomaglio, J.; Seshadri, R. Insulin pump therapy: A meta-analysis. Diabetes Care 2003, 26, 1079–1087. [Google Scholar] [CrossRef]
- Ramirez-Rincon, A.; Hincapie-Garcia, J.; Arango, C.M.; Aristizabal, N.; Castillo, E.; Hincapie, G.; Zapata, E.; Cuesta, D.P.; Delgado, M.; Abad, V.; et al. Clinical Outcomes after 1 Year of Augmented Insulin Pump Therapy in Patients with Diabetes in a Specialized Diabetes Center in Medellin, Colombia. Diabetes Technol. Ther. 2016, 18, 713–718. [Google Scholar] [CrossRef]
- Alshami, A.; Purewal, T.; Douedi, S.; Alazzawi, M.; Hossain, M.A.; Ong, R.; Sen, S.; Cheng, J.; Patel, S. Effect of Insulin Pump Use on Diabetic Ketoacidosis in Type 1 Diabetes Mellitus: A Matched Cohort Study. J. Clin. Med. 2021, 10, 898. [Google Scholar] [CrossRef] [PubMed]
- Evans, K. Diabetic ketoacidosis: Update on management. Clin. Med. 2019, 19, 396–398. [Google Scholar] [CrossRef]
- Chee, Y.J.; Ng, S.J.H.; Yeoh, E. Diabetic ketoacidosis precipitated by COVID-19 in a patient with newly diagnosed diabetes mellitus. Diabetes Res. Clin. Pract. 2020, 164, 108166. [Google Scholar] [CrossRef]
- Kazakou, P.; Paschou, S.A.; Psaltopoulou, T.; Gavriatopoulou, M.; Korompoki, E.; Stefanaki, K.; Kanouta, F.; Kassi, G.N.; Dimopoulos, M.A.; Mitrakou, A. Early and late endocrine complications of COVID-19. Endocr. Connect. 2021, 10, R229–R239. [Google Scholar] [CrossRef]
- Li, J.; Wang, X.; Chen, J.; Zuo, X.; Zhang, H.; Deng, A. COVID-19 infection may cause ketosis and ketoacidosis. Diabetes Obes. Metab. 2020, 22, 1935–1941. [Google Scholar] [CrossRef]
- Alhumaid, S.; Al Mutair, A.; Al Alawi, Z.; Rabaan, A.A.; Alomari, M.A.; Al Salman, S.A.; Al-Alawi, A.S.; Al Hassan, M.H.; Alhamad, H.; Al-Kamees, M.A.; et al. Diabetic ketoacidosis in patients with SARS-CoV-2: A systematic review and meta-analysis. Diabetol. Metab. Syndr. 2021, 13, 120. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Zhao, B.; Qu, Y.; Chen, Y.; Xiong, J.; Feng, Y.; Men, D.; Huang, Q.; Liu, Y.; Yang, B.; et al. Detectable Serum Severe Acute Respiratory Syndrome Coronavirus 2 Viral Load (RNAemia) Is Closely Correlated with Drastically Elevated Interleukin 6 Level in Critically Ill Patients with Coronavirus Disease 2019. Clin. Infect. Dis. 2020, 71, 1937–1942. [Google Scholar] [CrossRef] [PubMed]
- Stentz, F.B.; Umpierrez, G.E.; Cuervo, R.; Kitabchi, A.E. Proinflammatory cytokines, markers of cardiovascular risks, oxidative stress, and lipid peroxidation in patients with hyperglycemic crises. Diabetes 2004, 53, 2079–2086. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Mild DKA (glu > 250) | Moderate DKA (glu >250) | Severe DKA (glu > 250) | |
|---|---|---|---|
| Arterial pH | 7.25–7.30 | 7.00 to <7.24 | <7.00 |
| Serum bicarbonate | 15–18 | 10 to <15 | <10 |
| Urine ketone | Positive | Positive | Positive |
| Serum ketone | Positive | Positive | Positive |
| Serum osmolality | Variable | Variable | Variable |
| Anion gap | >10 | >12 | >12 |
| Mental status | Alert | Alert/drowsy | Stupor/coma |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El-Remessy, A.B. Diabetic Ketoacidosis Management: Updates and Challenges for Specific Patient Population. Endocrines 2022, 3, 801-812. https://doi.org/10.3390/endocrines3040066
El-Remessy AB. Diabetic Ketoacidosis Management: Updates and Challenges for Specific Patient Population. Endocrines. 2022; 3(4):801-812. https://doi.org/10.3390/endocrines3040066
Chicago/Turabian StyleEl-Remessy, Azza B. 2022. "Diabetic Ketoacidosis Management: Updates and Challenges for Specific Patient Population" Endocrines 3, no. 4: 801-812. https://doi.org/10.3390/endocrines3040066
APA StyleEl-Remessy, A. B. (2022). Diabetic Ketoacidosis Management: Updates and Challenges for Specific Patient Population. Endocrines, 3(4), 801-812. https://doi.org/10.3390/endocrines3040066