
Impact of 1.0 mg/Day Dienogest Treatment on Bone Metabolism Markers in Young Women with Dysmenorrhea



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Klein, J.R.; Litt, I.F. Epidemiology of adolescent dysmenorrhea. Pediatrics 1981, 68, 661–664. [Google Scholar] [CrossRef]
- Derman, O.; Kanbur, N.O.; Tokur, T.E.; Kutluk, T. Premenstrual syndrome and associated symptoms in adolescent girls. Eur. J. Obstet. Gynecol. Reprod. Biol. 2004, 116, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Janssen, E.B.; Rijkers, A.C.M.; Hoppenbrouwers, K.M.C.; D’Hooghe, T.M. Prevalence of endometriosis diagnosed by laparoscopy in adolescents with dysmenorrhea or chronic pelvic pain: A systematic review. Hum. Reprod. Update 2017, 19, 570–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acién, P.; Velasco, I. Endometriosis: A Disease That Remains Enigmatic. ISRN Obstet. Gynecol. 2013, 2013, 242149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stratton, P.; Berkley, K.J. Chronic pelvic pain and endometriosis: Translational evidence of the relationship and implications. Hum. Reprod. Update 2010, 17, 327–346. [Google Scholar] [CrossRef] [Green Version]
- Jones, G.; Kennedy, S.; Barnard, A.; Wong, J.; Jenkinson, C. Development of an endometriosis quality-of-life instrument: The Endometriosis Health Profile-30. Obstet. Gynecol. 2001, 98, 258–264. [Google Scholar] [CrossRef]
- Laursen, B.S.; Bajaj, P.; Olesen, A.S.; Delmar, C.; Arendt-Nielsen, L. Health related quality of life and quantitative pain measurement in females with chronic non-malignant pain. Eur. J. Pain 2005, 9, 267–275. [Google Scholar] [CrossRef]
- Verkauf, B.S. Incidence, symptoms, and signs of endometriosis in fertile and infertile women. J. Fla. Med. Assoc. 1987, 74, 671–675. [Google Scholar]
- Brosens, I. Endometriosis and the outcome of in vitro fertilization. Fertil. Steril. 2004, 81, 1198–1200. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 760: Dysmenorrhea and Endometriosis in the Adolescent. Obstet. Gynecol. 2018, 132, e249–e258. [Google Scholar] [CrossRef]
- Osuga, Y.; Hayashi, K.; Kanda, S. Evaluation of the efficacy, safety, and clinically recommended dose of dienogest in the treatment of primary dysmenorrhea: A randomized, double-blind, multicenter, placebo-controlled study. Fertil. Steril. 2020, 113, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Casper, R.F. Progestin-only pills may be a better first-line treatment for endometriosis than combined estrogen-progestin contraceptive pills. Fertil. Steril. 2017, 107, 533–536. [Google Scholar] [CrossRef] [Green Version]
- Ebert, A.D. Daily Vaginal Application of Dienogest (Visanne©) for 3 Months in Symptomatic Deeply Infiltrating Rectovaginal Endometriosis: A Possible New Treatment Approach? Case Rep. Obstet. Gynecol. 2018, 2018, 8175870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strowitzki, T.; Marr, J.; Gerlinger, C.; Faustmann, T.; Seitz, C. Dienogest is as effective as leuprolide acetate in treating the painful symptoms of endometriosis: A 24-week, randomized, multicentre, open-label trial. Hum. Reprod. 2010, 25, 633–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chew, C.K.; Clarke, B.L. Causes of low peak bone mass in women. Maturitas 2018, 111, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Nishizawa, Y.; Miura, M.; Ichimura, S.; Inaba, M.; Imanishi, Y.; Shiraki, M.; Takada, J.; Chaki, O.; Hagino, H.; Fukunaga, M.; et al. Executive summary of the Japan Osteoporosis Society Guide for the Use of Bone Turnover Markers in the Diagnosis and Treatment of Osteoporosis (2018 Edition). Clin. Chim. Acta 2019, 498, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Halleen, J.M.; Tiitinen, S.L.; Ylipahkala, H.; Fagerlund, K.M.; Väänänen, H.K. Tartrate-resistant acid phosphatase 5b (TRACP 5b) as a marker of bone resorption. Clin. Lab. 2006, 52, 499–509. [Google Scholar] [CrossRef] [Green Version]
- Ueda, M.; Inaba, M.; Okuno, S.; Maeno, Y.; Ishimura, E.; Yamakawa, T.; Nishizawa, Y. Serum BAP as the clinically useful marker for predicting BMD reduction in diabetic hemodialysis patients with low PTH. Life Sci. 2005, 77, 1130–1139. [Google Scholar] [CrossRef]
- Agerbæk, M.; Eriksen, E.; Kragstrup, J.; Mosekilde, L.; Melsen, F. A reconstruction of the remodelling cycle in normal human cortical iliac bone. Bone Miner. 1991, 12, 101–112. [Google Scholar] [CrossRef]
- Cadogan, J.; Blumsohn, A.; Barker, M.E.; Eastell, R. A Longitudinal Study of Bone Gain in Pubertal Girls: Anthropometric and Biochemical Correlates. J. Bone Miner. Res. 2009, 13, 1602–1612. [Google Scholar] [CrossRef]
- Berger, C.; Goltzman, D.; Langsetmo, L.; Joseph, L.; Jackson, S.; Kreiger, N.; Tenenhouse, A.; Davison, K.S.; Josse, R.G.; Prior, J.C.; et al. Peak bone mass from longitudinal data: Implications for the prevalence, pathophysiology, and diagnosis of osteoporosis. J. Bone Miner. Res. 2010, 25, 1948–1957. [Google Scholar] [CrossRef]
- Klok, F.; Kruip, M.; van der Meer, N.; Arbous, M.; Gommers, D.; Kant, K.; Kaptein, F.; van Paassen, J.; Stals, M.; Huisman, M.; et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb. Res. 2020, 191, 145–147. [Google Scholar] [CrossRef]
- Terpos, E.; Ntanasis-Stathopoulos, I.; Elalamy, I.; Kastritis, E.; Sergentanis, T.N.; Politou, M.; Psaltopoulou, T.; Gerotziafas, G.; Dimopoulos, M.A. Hematological findings and complications of COVID-19. Am. J. Hematol. 2020, 95, 834–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thachil, J.; Tang, N.; Gando, S.; Falanga, A.; Cattaneo, M.; Levi, M.; Clark, C.; Iba, T. ISTH interim guidance on recognition and management of coagulopathy in COVID-19. J. Thromb. Haemost. 2020, 18, 1023–1026. [Google Scholar] [CrossRef] [PubMed]
- I Spratt, D.; Buchsbaum, R.J. COVID-19 and Hypercoagulability: Potential Impact on Management with Oral Contraceptives, Estrogen Therapy and Pregnancy. Endocrinology 2020, 161, bqaa121. [Google Scholar] [CrossRef]
- Lopez, L.M.; A Grimes, D.; Schulz, K.F.; Curtis, K.M.; Chen, M. Steroidal contraceptives: Effect on bone fractures in women. Cochrane Database Syst. Rev. 2014, 24, CD006033. [Google Scholar] [CrossRef]
- Hartard, M.; Kleinmond, C.; Wiseman, M.; Weissenbacher, E.R.; Felsenberg, D.; Erben, R.G. Detrimental effect of oral contraceptives on parameters of bone mass and geometry in a cohort of 248 young women. Bone 2007, 40, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Scholes, D.; Ichikawa, L.; Lacroix, A.Z.; Spangler, L.; Beasley, J.; Reed, S.; Ott, S.M. Oral contraceptive use and bone density in adolescent and young adult women. Contraception 2010, 81, 35–40. [Google Scholar] [CrossRef] [Green Version]
- Hadji, E.P.; Colli, P.-A. Regidor Bone health in estrogen-free contraception. Osteoporos Int. 2019, 30, 2391–2400. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients (n = 321) | Before | After 3 Months |
|---|---|---|
| Age (year) | 18.0 ± 3.7 (10–24) | |
| BMI (%) | 23.5 ± 1.8 (19–31) | |
| Epiphyseal line closure (n) | 289 | |
| VAS (mm) | 82.4 ± 9.2 (48–100) | 12.3 ± 6.7 (0–25) |
| 25 (OH) vitamin D (ng/mL) | 21.0 ± 5.0 (8–36) | 22.3 ± 4.3 (7–34) |
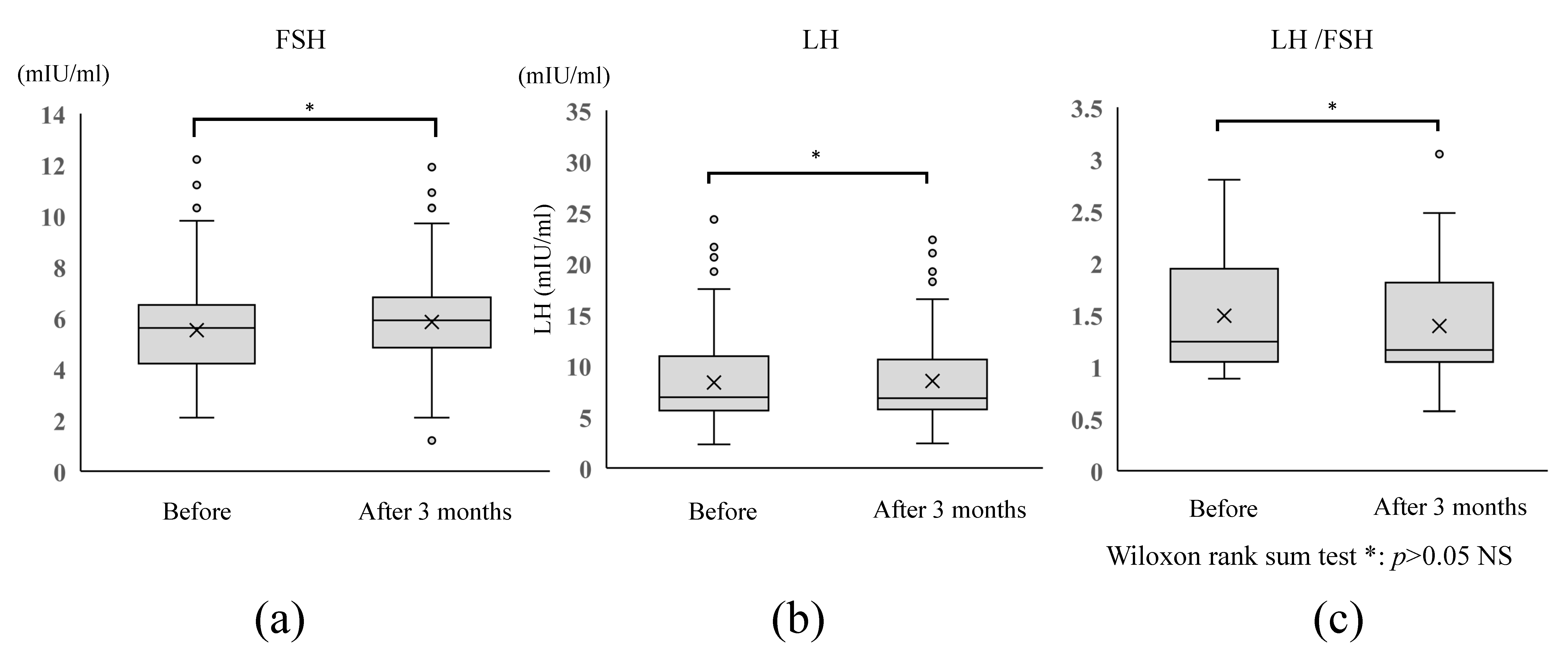
| LH (mIU/mL) | 7.6 ± 3.5 (3–24) | 7.3 ± 2.9 (3–23) |
| FSH (mIU/mL) | 5.5 ± 1.8 (2–12) | 6.1 ± 1.9 (1–12) |
| Estradiol (pg/mL) | 131.0 ± 92.5 (30–920) | 64.7 ± 8.9 (2–121) |
| Progesterone (ng/mL) | 1.2 ± 4.1 (0–56) | 0.12 ± 0.1 (0–1) |
| TRACP-5b (mU/dL) | 455.6 ± 323.6 (176–1452) | 462.1 ± 346.1 (121–1430) |
| BAP (μg/L) | 24.7 ± 19.0 (6–85) | 25.2 ± 22.3 (6–82) |
| T/B ratio | 22.1 ± 7.0 (6–45) | 21.5 ± 6.3 (7–42) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ota, I.; Ota, Y.; Taniguchi, F. Impact of 1.0 mg/Day Dienogest Treatment on Bone Metabolism Markers in Young Women with Dysmenorrhea. Endocrines 2021, 2, 293-300. https://doi.org/10.3390/endocrines2030027
Ota I, Ota Y, Taniguchi F. Impact of 1.0 mg/Day Dienogest Treatment on Bone Metabolism Markers in Young Women with Dysmenorrhea. Endocrines. 2021; 2(3):293-300. https://doi.org/10.3390/endocrines2030027
Chicago/Turabian StyleOta, Ikuko, Yoshiaki Ota, and Fuminori Taniguchi. 2021. "Impact of 1.0 mg/Day Dienogest Treatment on Bone Metabolism Markers in Young Women with Dysmenorrhea" Endocrines 2, no. 3: 293-300. https://doi.org/10.3390/endocrines2030027
APA StyleOta, I., Ota, Y., & Taniguchi, F. (2021). Impact of 1.0 mg/Day Dienogest Treatment on Bone Metabolism Markers in Young Women with Dysmenorrhea. Endocrines, 2(3), 293-300. https://doi.org/10.3390/endocrines2030027