
A Feasible Technique in Laparoscopic Excision for Juvenile Cystic Adenomyosis: A Case Report, Literature Review, and Surgical Video


 ,
,
Abstract
:1. Introduction
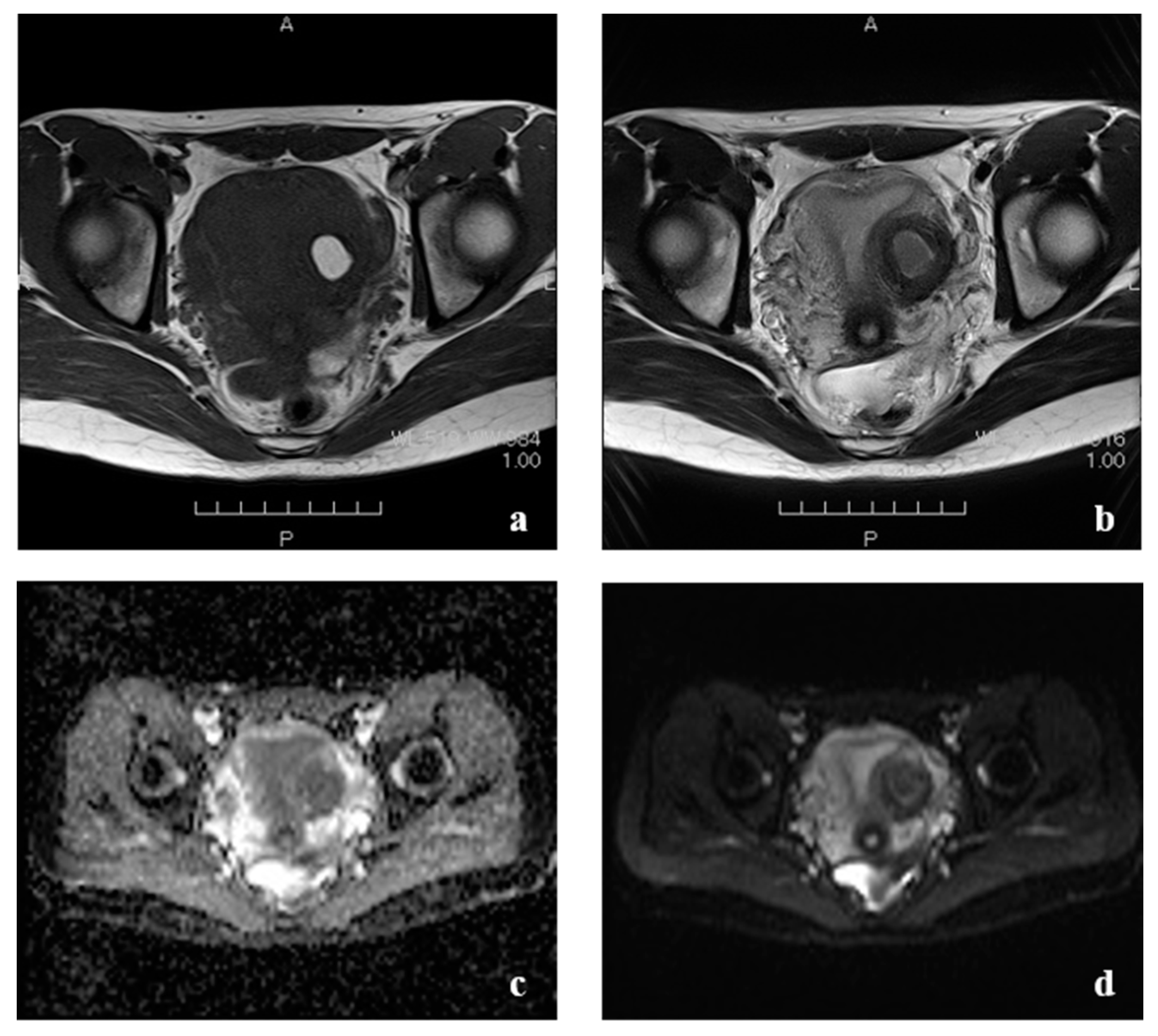
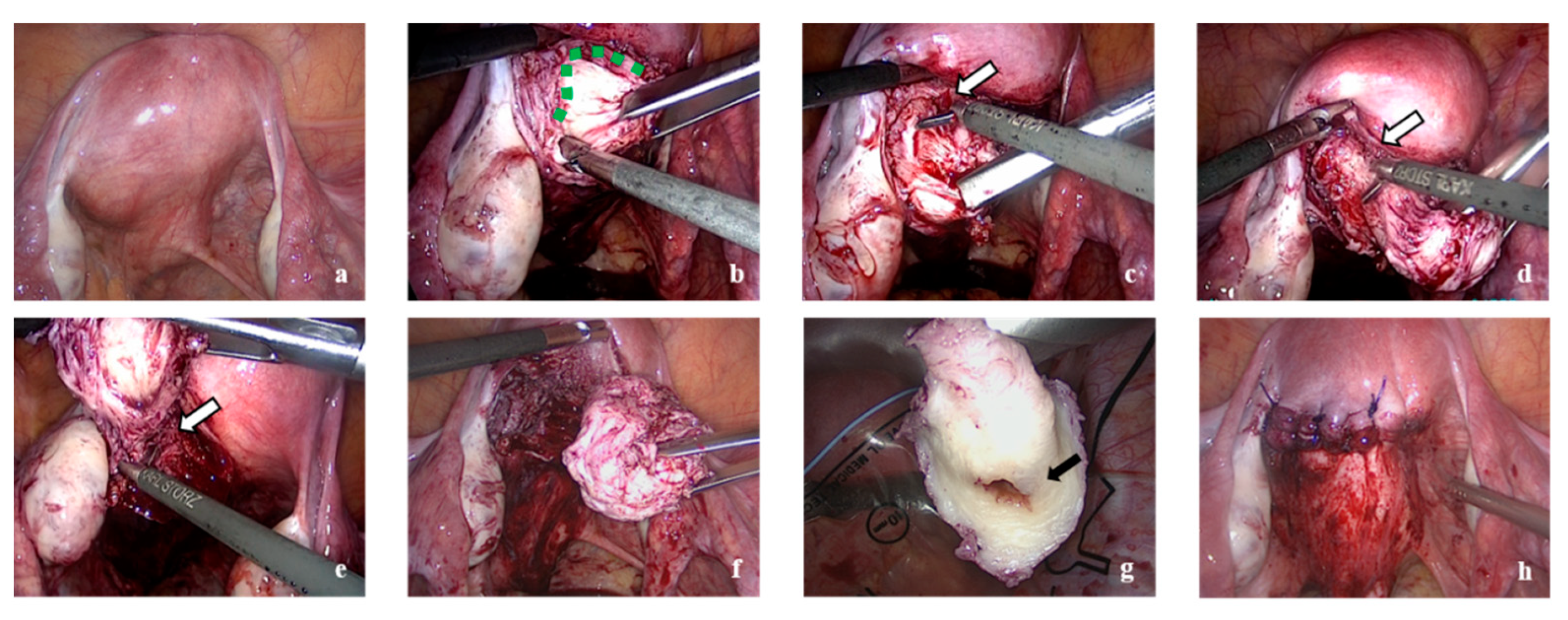
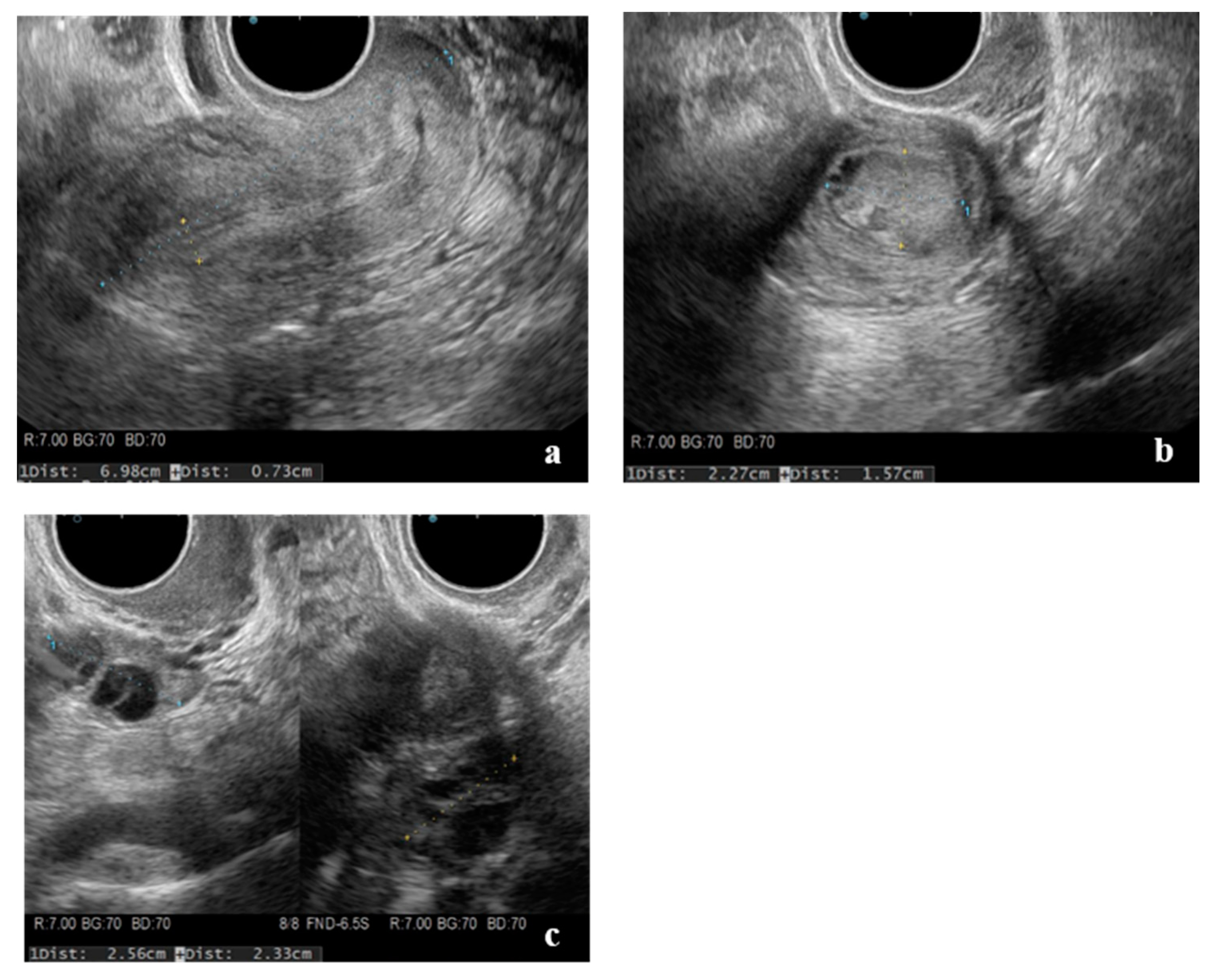
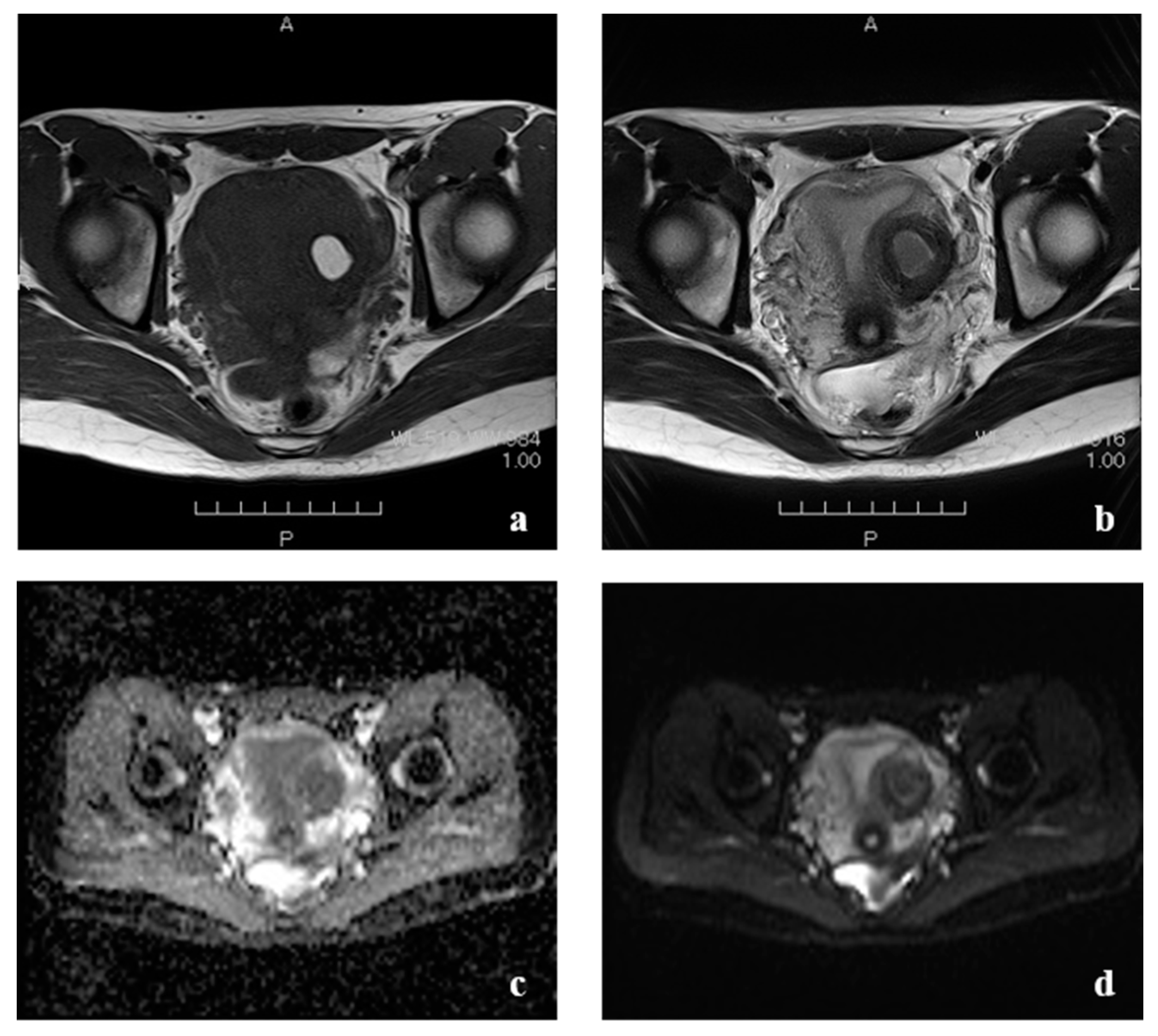
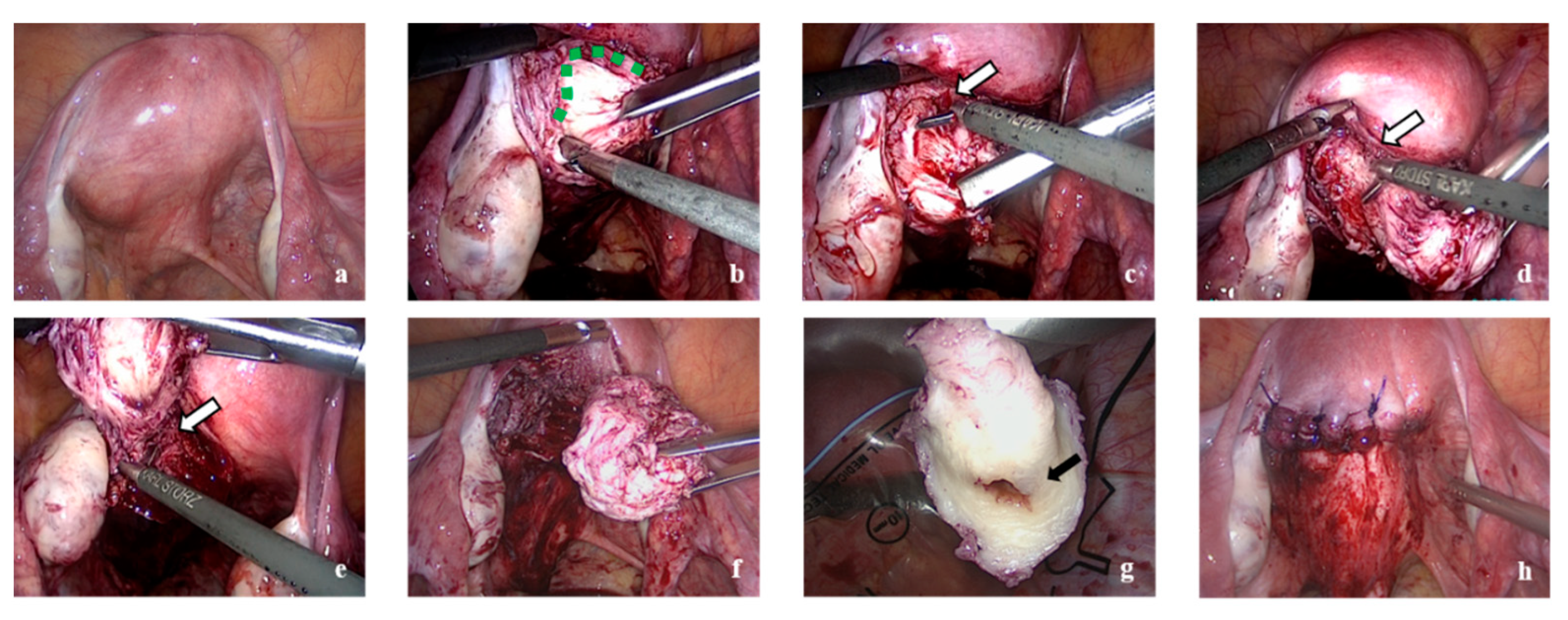
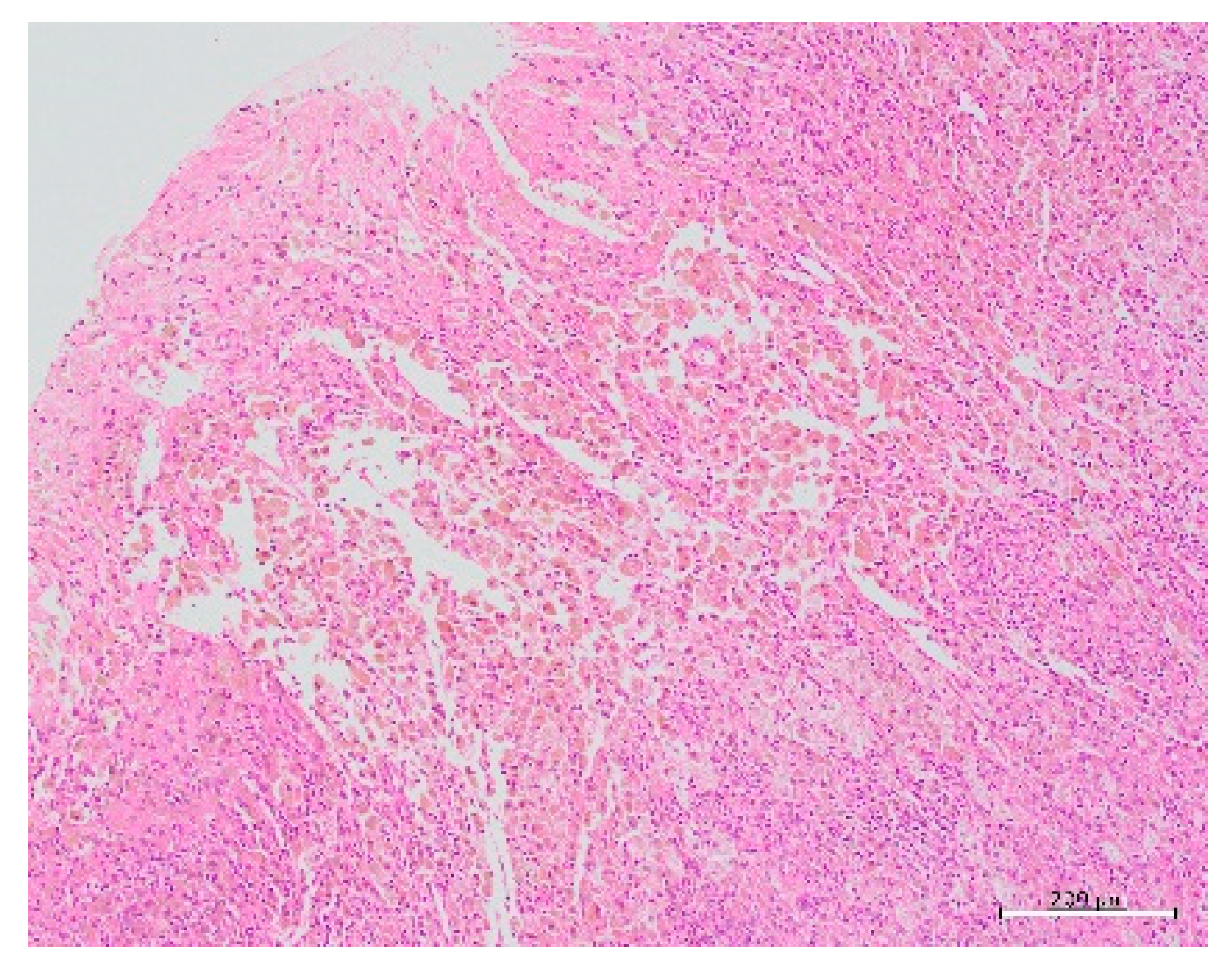
2. Case Presentation
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Dubransky, V. Submuckose uterus cyste. Zbl. Gynak 1936, 60, 564. [Google Scholar]
- Takeuchi, H.; Kitade, M.; Kikuchi, I.; Kumakiri, J.; Kuroda, K.; Jinushi, M. Diagnosis, laparoscopic management, and histopathologic findings of juvenile cystic adenomyoma: A review of nine cases. Fertil. Steril. 2010, 94, 862–868. [Google Scholar] [CrossRef] [PubMed]
- Nabeshima, H.; Murakami, T.; Terada, Y.; Noda, T.; Yaegashi, N.; Okamura, K. Total Laparoscopic Surgery of Cystic Adenomyoma under Hydroultrasonographic Monitoring. J. Am. Assoc. Gynecol. Laparosc. 2003, 10, 195–199. [Google Scholar] [CrossRef]
- Kamio, M.; Taguchi, S.; Oki, T.; Tsuji, T.; Iwamoto, I.; Yoshinaga, M.; Douchi, T. Isolated adenomyotic cyst associated with severe dysmenorrhea. J. Obstet. Gynaecol. Res. 2007, 33, 388–391. [Google Scholar] [CrossRef] [PubMed]
- Kriplani, A.; Mahey, R.; Agarwal, N.; Bhatla, N.; Yadav, R.; Singh, M.K. Laparoscopic Management of Juvenile Cystic Adenomyoma: Four Cases. J. Minim. Invasive Gynecol. 2011, 18, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Takeda, A.; Sakai, K.; Mitsui, T.; Nakamura, H. Laparoscopic management of juvenile cystic adenomyoma of the uterus: Report of two cases and review of the literature. J. Minim. Invasive Gynecol. 2007, 14, 370–374. [Google Scholar] [CrossRef]
- Nishida, M.; Takano, K.; Arai, Y.; Ozone, H.; Ichikawa, R. Conservative surgical management for diffuse uterine adenomyosis. Fertil. Steril. 2010, 94, 715–719. [Google Scholar] [CrossRef]
- Osada, H. Uterine adenomyosis and adenomyoma: The surgical approach. Fertil. Steril. 2018, 109, 406–417. [Google Scholar] [CrossRef] [Green Version]
- Arya, S.; Burks, H.R. Juvenile cystic adenomyoma, a rare diagnostic challenge: Case Reports and literature review. F S Rep. 2021, 2, 166–171. [Google Scholar] [CrossRef]
- Cucinella, G.; Billone, V.; Pitruzzella, I.; Monte, A.I.L.; Palumbo, V.D.; Perino, A. Adenomyotic Cyst in a 25-Year-Old Woman: Case Report. J. Minim. Invasive Gynecol. 2013, 20, 894–898. [Google Scholar] [CrossRef] [Green Version]
- Agha, R.A.; Borrelli, M.R.; Farwana, R.; Koshy, K.; Fowler, A.J.; Orgill, D.P.; Zhu, H.; Alsawadi, A.; Noureldin, A.; Rao, A.; et al. The SCARE 2018 statement: Updating consensus Surgical CAse REport (SCARE) guidelines. Int. J. Surg. 2018, 60, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Tahlan, A.; Nanda, A.; Mohan, H. Uterine adenomyoma: A clinicopathologic review of 26 cases and a review of the literature. Int. J. Gynecol. Pathol. 2006, 25, 361–365. [Google Scholar] [CrossRef]
- Branquinho, M.M.; Marques, A.L.; Leite, H.B.; Silva, I.S. Juvenile cystic adenomyoma. BMJ Case Rep. 2012, 2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molitor, J.J. Adenomyosis: A clinical and pathologic appraisal. Am. J. Obstet. Gynecol. 1971, 110, 275–282. [Google Scholar] [CrossRef]
- Tamura, M.; Fukaya, T.; Takaya, R.; Ip, C.W.; Yajima, A. Juvenile Adenomyotic Cyst of the Corpus Uteri with Dysmenorrhea. Tohoku J. Exp. Med. 1996, 178, 339–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levgur, M. Therapeutic options for adenomyosis: A review. Arch. Gynecol. Obstet. 2007, 276, 1–15. [Google Scholar] [CrossRef]
- Wada, S.-I.; Kudo, M.; Minakami, H. Spontaneous uterine rupture of a twin pregnancy after a laparoscopic adenomyomectomy: A case report. J. Minim. Invasive Gynecol. 2006, 13, 166–168. [Google Scholar] [CrossRef] [PubMed]
- Dogan, E.; Gode, F.; Saatli, B.; Seçil, M. Juvenile cystic adenomyosis mimicking uterine malformation: A case report. Arch. Gynecol. Obstet. 2008, 278, 593–595. [Google Scholar] [CrossRef]
- Nabeshima, H.; Murakami, T.; Nishimoto, M.; Sugawara, N.; Sato, N. Successful Total Laparoscopic Cystic Adenomyomectomy after Unsuccessful Open Surgery Using Transtrocar Ultrasonographic Guiding. J. Minim. Invasive Gynecol. 2008, 15, 227–230. [Google Scholar] [CrossRef]
- Ota, Y.; Ota, K.; Takahashi, T.; Suzuki, S.; Sano, R.; Shiota, M. New surgical technique of laparoscopic resection of adenomyosis under real-time intraoperative ultrasound elastography guidance: A case report. Heliyon 2020, 6, e04628. [Google Scholar] [CrossRef]
- Ho, M.-L.; Raptis, C.; Hulett, R.; McAlister, W.-H.; Moran, K.; Bhalla, S. Adenomyotic cyst of the uterus in an adolescent. Pediatric Radiol. 2008, 38, 1239–1242. [Google Scholar] [CrossRef]
- Potter, D.-A.; Schenken, R.-S. Noncommunicating accessory uterine cavity. Fertil. Steril. 1998, 70, 1165–1166. [Google Scholar] [CrossRef]
- Fisseha, S.; Smith, Y.-R.; Kumetz, L.-M.; Mueller, G.-C.; Hussain, H.; Quint, E.-H. Cystic myometrial lesion in the uterus of an adolescent girl. Fertil. Steril. 2006, 86, 716–718. [Google Scholar] [CrossRef] [PubMed]
- Ball, E.; Ganji, M.; Janik, G.; Koh, C. Laparoscopic resection of cystic adenomyosis in a teenager with arcurate uterus. Gynecol. Surg. 2009, 6, 367–370. [Google Scholar] [CrossRef] [Green Version]
- Akar, M.-E.; Leezer, K.-H.; Yalcinkaya, T.-M. Robot-assisted laparoscopic management of a case with juvenile cystic adenomyoma. Fertil. Steril. 2010, 94, 55–56. [Google Scholar] [CrossRef] [PubMed]
- Kumakiri, J.; Kikuchi, I.; Sogawa, Y.; Jinushi, M.; Aoki, Y.; Kitade, M.; Takeda, S. Single-incision laparoscopic surgery using an articulating monopolar for juvenile cystic adenomyoma. Minim. Invasive Ther. Allied Technol. 2013, 22, 312–315. [Google Scholar] [CrossRef] [PubMed]
- Pontrelli, G.; Bounous, V.-E.; Scarperi, S.; Minelli., L.; Di, S.-S.-A.; Florio, P. Rare case of giant cystic adenomyoma mimicking a uterine malformation, diagnosed and treated by hysteroscopy. J. Obstet. Gynaecol. Res. 2015, 41, 1300–1304. [Google Scholar] [CrossRef]
- Dadhwal, V.; Sharma, A.; Khoiwal, K. Juvenile Cystic Adenomyoma Mimicking a Uterine Anomaly: A Report of Two Cases. Eurasian J. Med. 2017, 49, 59–61. [Google Scholar] [CrossRef] [PubMed]
- Peters, A.; Rindos, N.-B.; Guido, R.-S.; Donnellan, N.-M. Uterine-sparing Laparoscopic Resection of Accessory Cavitated Uterine Masses. J. Minim. Invasive Gynecol. 2018, 25, 24–25. [Google Scholar] [CrossRef]
- Protopapas, A.; Kypriotis, K.; Chatzipapas, I.; Kathopoulis, N.; Sotiropoulou, M.; Michala, L. Juvenile Cystic Adenomyoma vs Blind Uterine Horn: Challenges in the Diagnosis and Surgical Management. J. Pediatric Adolesc. Gynecol. 2020, 33, 735–738. [Google Scholar] [CrossRef]
- Wilcox, A.; Schmidt, M.; Luciano, D. Identification of Juvenile Cystic Adenomyoma Using High-Resolution Imaging. Obstet. Gynecol. 2020, 136, 1021–1024. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age, Years | G | P | Menarche, Years | Cyst Size, mm | Cyst Location | CA125, U/mL | Previous Medical Management | Mullerian Anomalies | Surgery | Intraoperative Findings | Device | Suture | Specimen Weight, g | Ope Duration, min | Bood Loss, mL | Postope VAS (0–100) | Reference |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 16 | 0 | 0 | 12 | 30 | Left | N/A | None | DIP: normal | Open | 3 cm, left | N/A | N/A | N/A | N/A | N/A | N/A | Tamura, 1996 [15] |
| 2 | 27 | 0 | 0 | N/A | 20 | Right | N/A | NSAIDs, GnRH agonist, OC | N/A | Laparoscopy | 2 cm, right | Harmonic scalpel, a special tension device | myometrium: 1 polyglactin Z suture, serosal: continuous 4-0 polypropylene suture | N/A | 190 | few | 0 | Nabeshima, 2007 [19] |
| 3 | 19 | 0 | 0 | N/A | 30 | Right | 40.9 | GnRH agonist | HSG: normal | Laparoscopy | posterior, right | Harmonic scalpel, a special tension device | myometrium: 0 polyglactin suture, serosal: continuous 4-0 polypropylene suture | 234 | <100 | 0 | Nabeshima, 2003 [3] | |
| 4 | 23 | 0 | 0 | 12 | 30 | Left | 2.5 | Danazol, GnRH agonist, OC | HSG: normal | Open | 3 cm, anterior, left | N/A | N/A | N/A | 80 | 86 | 0 | Kamio, 2007 [4] |
| 5 | 16 | 0 | 0 | N/A | N/A | Right | N/A | None | HSG: normal | N/A | right | N/A | N/A | N/A | N/A | N/A | N/A | Ho, 2008 [21] |
| 6 | 15 | 0 | 0 | N/A | 40 | Left | N/A | NSAIDs, OC | HSG: normal | Open | 3 cm, anterior, left, near the round ligament | N/A | N/A | N/A | N/A | N/A | N/A | Potter, 1998 [22] |
| 7 | 13 | 0 | 0 | N/A | 21 | Left | N/A | OC | N/A | Not attempted | - | - | - | - | - | - | - | Fisseha, 2006 [23] |
| 8 | 20 | 0 | 0 | 13 | 30 | Right | 25 | NSAIDs, GnRH agonist | HSG, DIP: normal | Laparoscopy | anterior, right, near the round ligament | Harmonic scalpel, claw forceps | single-layer closure | N/A | N/A | N/A | N/A | Takeda, 2007 [6] |
| 9 | 20 | 0 | 0 | 14 | 26 | Left | 40.5 | NSAIDs | HSG, DIP: normal | Laparoscopy | the uterine surface appeared unchanged | Harmonic scalpel | single-layer closure | N/A | 67 | <50 | 0 | Takeda, 2007 [6] |
| 10 | 30 | 0 | 0 | N/A | 35 | L: 3, R: 6 | 43 | None | HSG, DIP: normal | Laparoscopy | N/A | N/A | N/A | 10 | 70 | 20 | 20 | Takeuchi, 2010 [2] |
| 11 | 29 | 0 | 0 | N/A | 30 | 141 | None | HSG, DIP: normal | Laparoscopy | N/A | N/A | N/A | 10 | 120 | 100 | 30 | Takeuchi, 2010 [2] | |
| 12 | 27 | 2 | 2 | N/A | 42 | 36 | None | HSG, DIP: normal | Laparoscopy | N/A | N/A | N/A | 10 | 70 | 50 | 20 | Takeuchi, 2010 [2] | |
| 13 | 20 | 0 | 0 | N/A | 28 | 551 | OC | HSG, DIP: normal | Laparoscopy | N/A | N/A | N/A | 11 | 96 | 52 | 20 | Takeuchi, 2010 [2] | |
| 14 | 30 | 2 | 2 | N/A | 30 | 34 | None | HSG, DIP: normal | Laparoscopy | N/A | N/A | N/A | 7 | 76 | 5 | 10 | Takeuchi, 2010 [2] | |
| 15 | 28 | 0 | 0 | N/A | 25 | 12 | GnRH agonist, OC | HSG, DIP: normal | Laparoscopy | N/A | N/A | N/A | 7 | 70 | 10 | 2 | Takeuchi, 2010 [2] | |
| 16 | 23 | 0 | 0 | N/A | 28 | 157 | OC | HSG, DIP: normal | Laparoscopy | N/A | N/A | N/A | 3.5 | 75 | 50 | 30 | Takeuchi, 2010 [2] | |
| 17 | 20 | 0 | 0 | N/A | 34 | 34 | GnRH agonist | HSG, DIP: normal | Laparoscopy | N/A | N/A | N/A | 111.5 | 76 | 50 | 20 | Takeuchi, 2010 [2] | |
| 18 | 20 | 0 | 0 | N/A | 34 | 14 | GnRH agonist | HSG, DIP: normal | Laparoscopy | N/A | N/A | N/A | 4.1 | 49 | 10 | 10 | Takeuchi, 2010 [2] | |
| 19 | 16 | 0 | 0 | 38 | Right | N/A | NSAIDs, OC | HYS: normal | Laparoscopy | 4 cm, posterior, right | unipolar and bipolar electrosurgery | 2-0 polyglactin | 20 | 50 | N/A | 0 | Kriplani, 2011 [5] | |
| 20 | 18 | 0 | 0 | N/A | 42 | Right | N/A | NSAIDs, OC | HYS: normal | Laparoscopy | 5 cm, right | unipolar and bipolar electrosurgery | 2-0 polyglactin | 25 | 80 | N/A | 10 | Kriplani, 2011 [5] |
| 21 | 16 | 0 | 0 | N/A | 31 | N/A | N/A | NSAIDs | HYS: normal | Laparoscopy | 5 cm, anterior | unipolar and bipolar electrosurgery | 2-0 polyglactin | 18 | 60 | N/A | 0 | Kriplani, 2011 [5] |
| 22 | 24 | 0 | 0 | N/A | 30 | Right | N/A | NSAIDs, OC | HYS: normal | Laparoscopy | 4 cm, anterior, right, entering broad ligament | unipolar and bipolar electrosurgery | 2-0 polyglactin | 27 | 75 | N/A | 0 | Kriplani, 2011 [5] |
| 23 | 19 | 0 | 0 | N/A | 40 | Left | WNL | NSAIDs, OC | HSG: normal | Open | anterior, left | scalpel | double layer closure | N/A | N/A | N/A | 0 | Dogan, 2008 [18] |
| 24 | 19 | 0 | 0 | 13 | 20 | Left | NSAIDs, OC | HYS: normal | Laparoscopy | 2 cm, anterior, left | Harmonic scalpel | 2/0 PDS myometrium, 3/0 PDS serosa | N/A | 90 | <20 | 0 | Ball, 2009 [24] | |
| 25 | 15 | 0 | 0 | N/A | 47 | Right | N/A | OC, GnRH agonist | Robotic-assisted Lap | 4 cm, anterior fundal, right | N/A | four layers | N/A | N/A | N/A | N/A | Akar, 2010 [25] | |
| 26 | 18 | 0 | 0 | 14 | 30 | Left | N/A | hormonal therapy | MRI: normal | Laparoscopy | 3 cm, lateral, left | monopolar scissors | 2 layers, 2-0 vicryl | N/A | 120 | few | Relieved | Ayra, 2021 [9] |
| 27 | 16 | 0 | 0 | 14 | 51 | Right | N/A | OC | N/A | Laparoscopy | 5 cm, right, near the cornu | monopolar scissors | 2 layers, 2-0 vicryl | N/A | N/A | N/A | Relieved | Ayra, 2021 [9] |
| 28 | 17 | 0 | 0 | 13 | 33 | Right | NSAIDs, OC | N/A | Not attempted | - | - | - | - | - | - | - | Branquinho, 2012 [13] | |
| 29 | 25 | 0 | 0 | 12 | 50 | N/A | 38 | NSAIDs | N/A | Laparoscopy | N/A | monopolar hook | N/A | N/A | 70 | <20 | Relieved | Cucinella, 2013 [10] |
| 30 | 20 | 0 | 0 | N/A | 30 | N/A | N/A | N/A | N/A | Laparoscopy | N/A | monopolar hook | barbed string | Relieved | Kumakiri, 2013 [26] | |||
| 31 | 27 | 0 | 0 | N/A | 75 | Right | 96 | OC | N/A | Hysteroscopy | bilocular cyst of 8 cm, posterior | monopolar loop | None | N/A | N/A | N/A | Relieved | Pontrelli, 2015 [27] |
| 32 | 23 | 0 | 0 | 17 | 39 | Right | N/A | None | HYS: normal | Open | anterior, right side | N/A | 1-0 vicryl | N/A | N/A | N/A | Relieved | Dadhwal, 2017 [28] |
| 33 | 16 | 0 | 0 | 13 | 40 | Left | N/A | None | HYS: normal | Laparoscopy | 4 cm, left | N/A | 1-0 V-lock | N/A | N/A | N/A | Relieved | Dadhwal, 2017 [28] |
| 34 | 19 | 0 | 0 | N/A | 30 | Left | N/A | OC | N/A | Not attempted | - | - | - | - | - | - | - | Peters, 2018 [29] |
| 35 | 14 | 0 | 0 | N/A | 38 | Left | N/A | progestins | MRI: normal | Laparoscopy | left side, near the cornu | monopolar needle | 2 layers using figure of 8 absorbable sutures | N/A | N/A | N/A | 40 | Protopapas, 2020 [30] |
| 36 | 18 | 0 | 0 | 13 | 23 | Left | N/A | OC, LNG-IUD | HYS: normal | Laparoscopy | anterior, left, near the round ligament | monopolar scissors | 2 layers, 0-Vicryl, serosa: 2-0 Monocryl | N/A | N/A | N/A | N/A | Wilcox, 2020 [31] |
| 37 | 18 | 0 | 0 | N/A | 36 | Left | N/A | OC | HYS: normal | Laparoscopy | anterior, left, near the round ligament | monopolar scissors | myometrium: 0 Vicryl, serosa: running stitch of 2–0 Vicryl | N/A | N/A | N/A | N/A | Wilcox, 2020 [31] |
| Median | 19 | 0 | 0 | 13 | 30.5 | R: 18, L: 16 | 38 | 10 | 75.5 | 50 | 6 | |||||||
| This case | 22 | 0 | 0 | 15 | 36 | L | 51.9 | None | CT, MRI: None | Laparoscopy | 3 cm, lateral, left side | Harmonic Scalpel, scissors forceps | 2 layers using 0 PDS | 14 | 69 | few | 2 | Present study |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katakura, M.; Katagiri, Y.; Ota, K.; Mukai, T.; Nakaoka, K.; Maemura, T.; Morita, M. A Feasible Technique in Laparoscopic Excision for Juvenile Cystic Adenomyosis: A Case Report, Literature Review, and Surgical Video. Endocrines 2021, 2, 284-292. https://doi.org/10.3390/endocrines2030026
Katakura M, Katagiri Y, Ota K, Mukai T, Nakaoka K, Maemura T, Morita M. A Feasible Technique in Laparoscopic Excision for Juvenile Cystic Adenomyosis: A Case Report, Literature Review, and Surgical Video. Endocrines. 2021; 2(3):284-292. https://doi.org/10.3390/endocrines2030026
Chicago/Turabian StyleKatakura, Masafumi, Yukiko Katagiri, Kuniaki Ota, Takafumi Mukai, Kentaro Nakaoka, Toshimitsu Maemura, and Mineto Morita. 2021. "A Feasible Technique in Laparoscopic Excision for Juvenile Cystic Adenomyosis: A Case Report, Literature Review, and Surgical Video" Endocrines 2, no. 3: 284-292. https://doi.org/10.3390/endocrines2030026
APA StyleKatakura, M., Katagiri, Y., Ota, K., Mukai, T., Nakaoka, K., Maemura, T., & Morita, M. (2021). A Feasible Technique in Laparoscopic Excision for Juvenile Cystic Adenomyosis: A Case Report, Literature Review, and Surgical Video. Endocrines, 2(3), 284-292. https://doi.org/10.3390/endocrines2030026