
The Impact of Early-to-Moderate Stage Chronic Kidney Disease on Hospitalization Outcomes in Patients Undergoing Allogeneic Hematopoietic Stem Cell Transplant: A Nationwide Analysis Using the National Inpatient Sample Database (2002–2019)

 , and
, and
Abstract
1. Introduction
2. Methods and Materials
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wildes, T.M.; Stirewalt, D.L.; Medeiros, B.; Hurria, A. Hematopoietic stem cell transplantation for hematologic malignancies in older adults: Geriatric principles in the transplant clinic. J. Natl. Compr. Canc. Netw. 2014, 12, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Thakar, M.S.; Broglie, L.; Logan, B.; Artz, A.; Bunin, N.; Burroughs, L.M.; Fretham, C.; Jacobsohn, D.A.; Loren, A.W.; Kurtzberg, J.; et al. The Hematopoietic Cell Transplant Comorbidity Index predicts survival after allogeneic transplant for nonmalignant diseases. Blood 2019, 133, 754–762. [Google Scholar] [CrossRef] [PubMed]
- Sorror, M.L.; Maris, M.B.; Storb, R.; Baron, F.; Sandmaier, B.M.; Maloney, D.G.; Storer, B. Hematopoietic cell transplantation (HCT)-specific comorbidity index: A new tool for risk assessment before allogeneic HCT. Blood 2005, 106, 2912–2919. [Google Scholar] [CrossRef] [PubMed]
- HCUP-US NIS Overview. Available online: https://www.hcup-us.ahrq.gov/nisoverview.jsp (accessed on 16 June 2023).
- Trend Weights for HCUP NIS Data. Available online: https://www.hcup-us.ahrq.gov/db/nation/nis/trendwghts.jsp (accessed on 16 June 2023).
- Ammad Ud Din, M.; Saeed, H.; Shahzad, M.; Liaqat, H.; Sweet, K. The impact of mild-to-moderate chronic kidney disease on hospitalization outcomes in patients with acute myeloid leukemia. Leuk. Lymphoma 2023, 64, 1040–1044. [Google Scholar] [CrossRef] [PubMed]
- Ammad Ud Din, M.; Mahmud, A.; Mostafa, M.; Shahzad, M.; Liaqat, H.; Pinilla-Ibarz, J.; Jaglal, M. Risks and outcomes of hospitalizations in patients with chronic lymphocytic leukemia admitted with immune thrombocytopenia: An analysis of the National Inpatient Sample Database. Ann. Hematol. 2023, 102, 889–895. [Google Scholar] [CrossRef] [PubMed]
- Sahin, U.; Toprak, S.K.; Atilla, P.A.; Atilla, E.; Demirer, T. An overview of infectious complications after allogeneic hematopoietic stem cell transplantation. J. Infect Chemother. 2016, 22, 505–514. [Google Scholar] [CrossRef] [PubMed]
- Hirose, N.; Tachibana, T.; Izumi, A.; Sato, S.; Tadera, N.; Tamai, Y.; Kanamori, H.; Tanaka, M.; Nakajima, H. Bridging to transplant and post-transplant maintenance therapy with FLT3 inhibitors in patients with relapsed or refractory FLT3 mutated acute myeloid leukemia. Hematology 2023, 28, 2220518. [Google Scholar] [CrossRef] [PubMed]
- Farhadfar, N.; Dias, A.; Wang, T.; Fretham, C.; Chhabra, S.; Murthy, H.S.; Broglie, L.; D’Souza, A.; Gadalla, S.M.; Gale, R.P.; et al. Impact of pretransplantation renal dysfunction on outcomes after allogeneic hematopoietic cell transplantation. Transplant. Cell. Ther. 2021, 27, 410–422. [Google Scholar] [CrossRef] [PubMed]
- Shouval, R.; de Jong, C.N.; Fein, J.; Broers, A.E.; Danylesko, I.; Shimoni, A.; Reurs, M.R.; Baars, A.E.; van der Schaft, N.; Nagler, A.; et al. Baseline renal function and albumin are powerful predictors for allogeneic transplantation-related mortality. Biol. Blood Marrow Transplant. 2018, 24, 1685–1691. [Google Scholar] [CrossRef] [PubMed]
- Bodge, M.N.; Reddy, S.; Thompson, M.S.; Savani, B.N. Preparative regimen dosing for hematopoietic stem cell transplantation in patients with chronic kidney disease: Analysis of the literature and recommendations. Biol. Blood Marrow Transplant. 2014, 20, 908–919. [Google Scholar] [CrossRef] [PubMed]
- Lopes, J.A.; Jorge, S.; Neves, M. Acute kidney injury in HCT: An update. Bone Marrow Transplant. 2016, 51, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Renaghan, A.D.; Jaimes, E.A.; Malyszko, J.; Perazella, M.A.; Sprangers, B.; Rosner, M.H. Acute Kidney Injury and CKD Associated with Hematopoietic Stem Cell Transplantation. Clin. J. Am. Soc. Nephrol. 2020, 15, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Póvoa, P.; Coelho, L.; Dal-Pizzol, F.; Ferrer, R.; Huttner, A.; Conway Morris, A.; Nobre, V.; Ramirez, P.; Rouze, A.; Salluh, J.; et al. How to use biomarkers of infection or sepsis at the bedside: Guide to clinicians. Intensive Care Med. 2023, 49, 142–153. [Google Scholar] [CrossRef] [PubMed]
- Farha, N.; Munguti, C. A Dramatic Presentation of Pulmonary Edema Due to Renal Failure. Kans. J. Med. 2020, 13, 56–57. [Google Scholar] [CrossRef] [PubMed]
- Singh, J. Cardio-oncology and transplantation for acute myeloid leukemia. Best Pract. Res. Clin. Haematol. 2023, 36, 101465. [Google Scholar] [CrossRef] [PubMed]
- Turakhia, M.P.; Blankestijn, P.J.; Carrero, J.J.; Clase, C.M.; Deo, R.; Herzog, C.A.; Kasner, S.E.; Passman, R.S.; Pecoits-Filho, R.; Reinecke, H.; et al. Chronic kidney disease and arrhythmias: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Eur. Heart J. 2018, 39, 2314–2325. [Google Scholar] [CrossRef] [PubMed]
- Navaneethan, S.D.; Sankarasubbaiyan, S.; Gross, M.D.; Jeevanantham, V.; Monk, R.D. Tacrolimus-associated hypomagnesemia in renal transplant recipients. Transplant. Proc. 2006, 38, 1320–1322. [Google Scholar] [CrossRef] [PubMed]
- Benchimol, E.I.; Smeeth, L.; Guttmann, A.; Harron, K.; Moher, D.; Petersen, I.; Sørensen, H.T.; von Elm, E.; Langan, S.M.; The RECORD Working Committee. The Reporting of studies Conducted using Observational Routinely-collected health Data (RECORD) Statement. PLoS Med. 2015, 10, e0125620. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | With CKD N = 920 (1.1%) | Without CKD N = 83,706 (98.9%) | p Value |
|---|---|---|---|
| Age + SD (years) | 57.9 + 14.4 | 49.2 + 12.2 | <0.001 |
| Admission Type | |||
| Elective | 77.9 | 22.1 | <0.001 |
| Non-Elective | 82.2 | 17.8 | |
| Gender (%) | |||
| Male | 69.0 | 57.4 | <0.001 |
| Female | 31.0 | 42.6 | |
| Race (%) | |||
| White | 77.4 | 76.3 | <0.001 |
| Black | 11.0 | 6.1 | |
| Hispanic | 5.1 | 9.7 | |
| Other | 6.5 | 7.8 | |
| Comorbidities | |||
| CAD | 13.6 | 4.2 | <0.001 |
| Smoking | 3.8 | 4.0 | 0.72 |
| Alcohol Use | 0.0 | 0.2 | 0.18 |
| COPD | 14.1 | 7.0 | <0.001 |
| Diabetes | 23.7 | 11.0 | <0.001 |
| Drug Abuse | 1.5 | 2.9 | 0.02 |
| Hypertension | 66.4 | 34.8 | <0.001 |
| Hypothyroidism | 12.5 | 7.9 | <0.001 |
| Coagulopathy | 18.8 | 12.5 | <0.001 |
| Liver Disease | 7.5 | 4.9 | <0.001 |
| Depression | 14.7 | 13.4 | 0.27 |
| Obesity | 4.3 | 2.3 | <0.001 |
| Myocardial Infarction | 5.0 | 1.7 | <0.001 |
| Congestive Heart Disease | 14.1 | 4.9 | <0.001 |
| Peripheral Vascular Disease | 2.7 | 0.8 | <0.001 |
| Primary Insurance (%) | |||
| Medicare | 36.8 | 16.4 | <0.001 |
| Medicaid | 11.9 | 11.1 | |
| Private Insurance | 44.7 | 66.1 | |
| Self-Pay | 0.5 | 1.2 | |
| No charge | 0.0 | 0.2 | |
| Other | 6.1 | 5.0 | |
| Median Household Income (%) | |||
| 0–25th Percentile | 18.9 | 17.4 | 0.261 |
| 26th–50th Percentile | 23.2 | 22.2 | |
| 51st–75th Percentile | 24.3 | 27.0 | |
| 76Th–100th Percentile | 33.6 | 33.4 | |
| Hospital Size (%) | |||
| Small | 15.0 | 14.3 | <0.001 |
| Medium | 11.3 | 7.3 | |
| Large | 73.7 | 78.4 | |
| Hospital Region | |||
| Northeast | 13.0 | 22.8 | <0.001 |
| Midwest | 37.7 | 23.8 | |
| South | 26.4 | 30.2 | |
| West | 22.8 | 23.2 | |
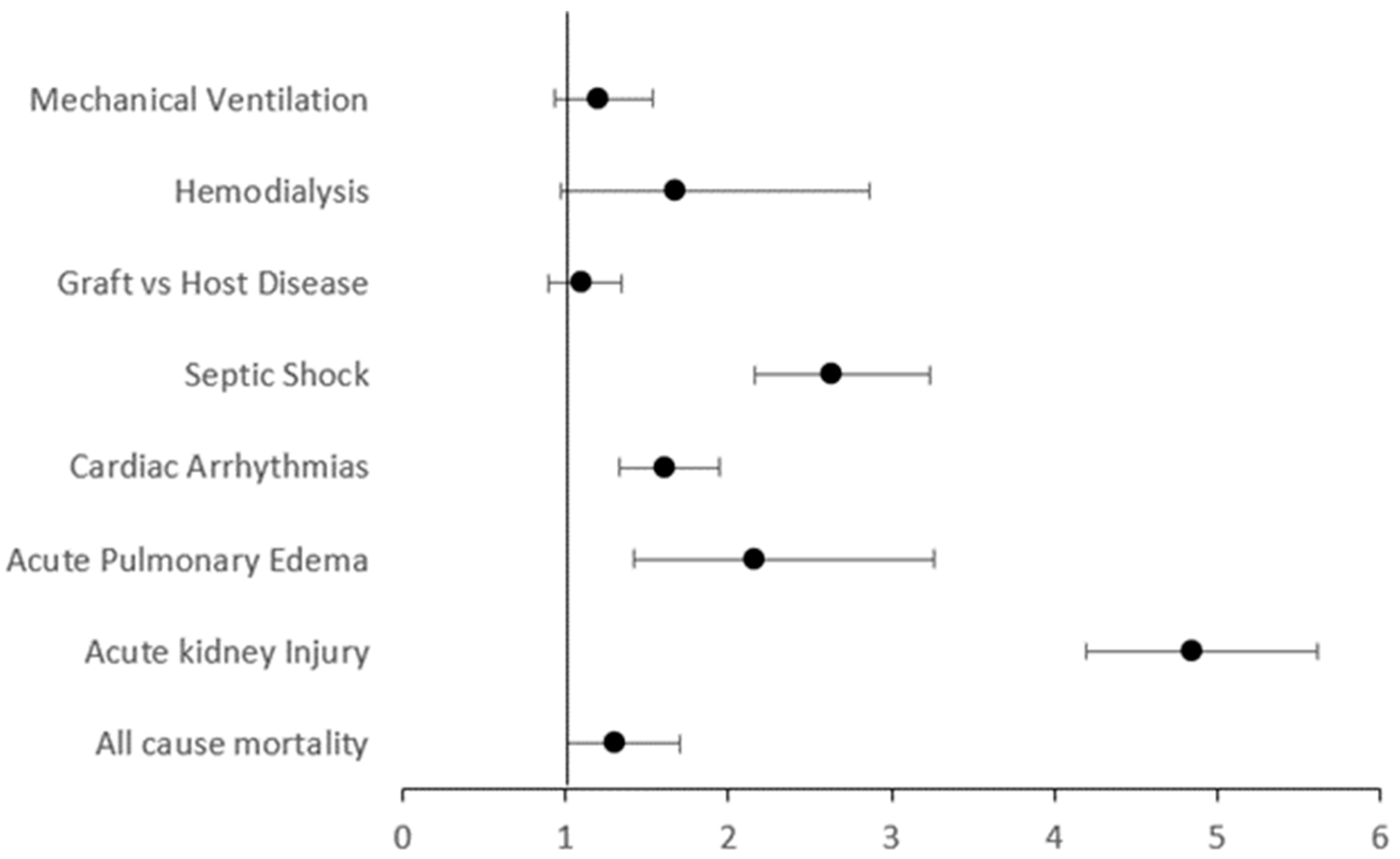
| Variable | CKD Group | Without CKD Group | Unadjusted Odds Ratio | p Value | Adjusted Odds Ratio | p Value |
|---|---|---|---|---|---|---|
| All-cause Mortality (%) | 9.6 | 6.4 | 1.56 95% CI (1.25–1.94) | <0.001 | 1.31 95% CI (1.01–1.70) | 0.04 |
| AKI (%) | 49.6 | 14.7 | 5.69 95% CI (5.00–6.48) | <0.001 | 4.85 95% CI (4.19–5.61) | <0.001 |
| Acute Pulmonary Edema (%) | 2.8 | 1.9 | 3.00 95% CI (2.02–4.46) | <0.001 | 2.16 95% CI (1.42–3.26) | <0.001 |
| Cardiac Arrhythmias (%) | 16.2 | 7.0 | 2.57 95% CI (2.15–3.07) | <0.001 | 1.61 (95% CI 1.33–1.95) | <0.001 |
| Cardiogenic Shock * (%) | 1.1 | 0.2 | 5.53 95% (2.91–10.5) | <0.001 | 2.93 95% CI (1.44–5.93) | 0.003 |
| Septic Shock (%) | 7.0 | 3.0 | 2.38 95% CI (1.84–3.08) | <0.001 | 2.64 95% CI (2.16–3.23) | <0.001 |
| GVHD (%) | 13.3 | 11.1 | 1.23 95% CI (1.02–1.49) | 0.03 | 1.10 95% CI (0.90–1.34) | 0.37 |
| Hemodialysis (%) | 1.6 | 0.4 | 3.68 95% CI (2.19–6.20) | <0.001 | 1.67 95% CI (0.97–2.87) | 0.07 |
| Mechanical Ventilation (%) | 9.8 | 5.9 | 1.74 95% CI (1.40–2.17) | <0.001 | 1.20 (95% 0.93–1.54) | 0.17 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ammad Ud Din, M.; Ain, Q.; Abedin, M.S.U.; Shahzad, M.; Mushtaq, M.U. The Impact of Early-to-Moderate Stage Chronic Kidney Disease on Hospitalization Outcomes in Patients Undergoing Allogeneic Hematopoietic Stem Cell Transplant: A Nationwide Analysis Using the National Inpatient Sample Database (2002–2019). Transplantology 2024, 5, 140-147. https://doi.org/10.3390/transplantology5030014
Ammad Ud Din M, Ain Q, Abedin MSU, Shahzad M, Mushtaq MU. The Impact of Early-to-Moderate Stage Chronic Kidney Disease on Hospitalization Outcomes in Patients Undergoing Allogeneic Hematopoietic Stem Cell Transplant: A Nationwide Analysis Using the National Inpatient Sample Database (2002–2019). Transplantology. 2024; 5(3):140-147. https://doi.org/10.3390/transplantology5030014
Chicago/Turabian StyleAmmad Ud Din, Mohammad, Qurratul Ain, Muhammad Shan Ul Abedin, Moazzam Shahzad, and Muhammad Umair Mushtaq. 2024. "The Impact of Early-to-Moderate Stage Chronic Kidney Disease on Hospitalization Outcomes in Patients Undergoing Allogeneic Hematopoietic Stem Cell Transplant: A Nationwide Analysis Using the National Inpatient Sample Database (2002–2019)" Transplantology 5, no. 3: 140-147. https://doi.org/10.3390/transplantology5030014
APA StyleAmmad Ud Din, M., Ain, Q., Abedin, M. S. U., Shahzad, M., & Mushtaq, M. U. (2024). The Impact of Early-to-Moderate Stage Chronic Kidney Disease on Hospitalization Outcomes in Patients Undergoing Allogeneic Hematopoietic Stem Cell Transplant: A Nationwide Analysis Using the National Inpatient Sample Database (2002–2019). Transplantology, 5(3), 140-147. https://doi.org/10.3390/transplantology5030014