1. Introduction and Background
Trastuzumab, an innovative monoclonal antibody developed by Genentech, Inc. in San Francisco, California, is approved for the treatment of HER2-positive breast cancers and gastric cancer [
1]. While the role of HER2 overexpression in aggressive breast cancer is well established, the mechanisms by which trastuzumab exerts its effects are multifaceted. These mechanisms include antibody-dependent cell-mediated cytotoxicity, the inhibition of cleavage, and the disruption of oncogenic signaling. Moreover, trastuzumab enhances the interaction between the HER2 protein and the negative regulator Csk-homologous kinase through the phosphorylation of HER2 at Y1248. Clinical evidence suggests that inhibiting breast cancer cell growth by targeting HER2 phosphorylation at Y1248 is a critical factor in predicting the efficacy of trastuzumab in the neoadjuvant setting [
2]. Given the complexity of HER2-targeted therapies, understanding the mechanisms of trastuzumab action is of utmost importance.
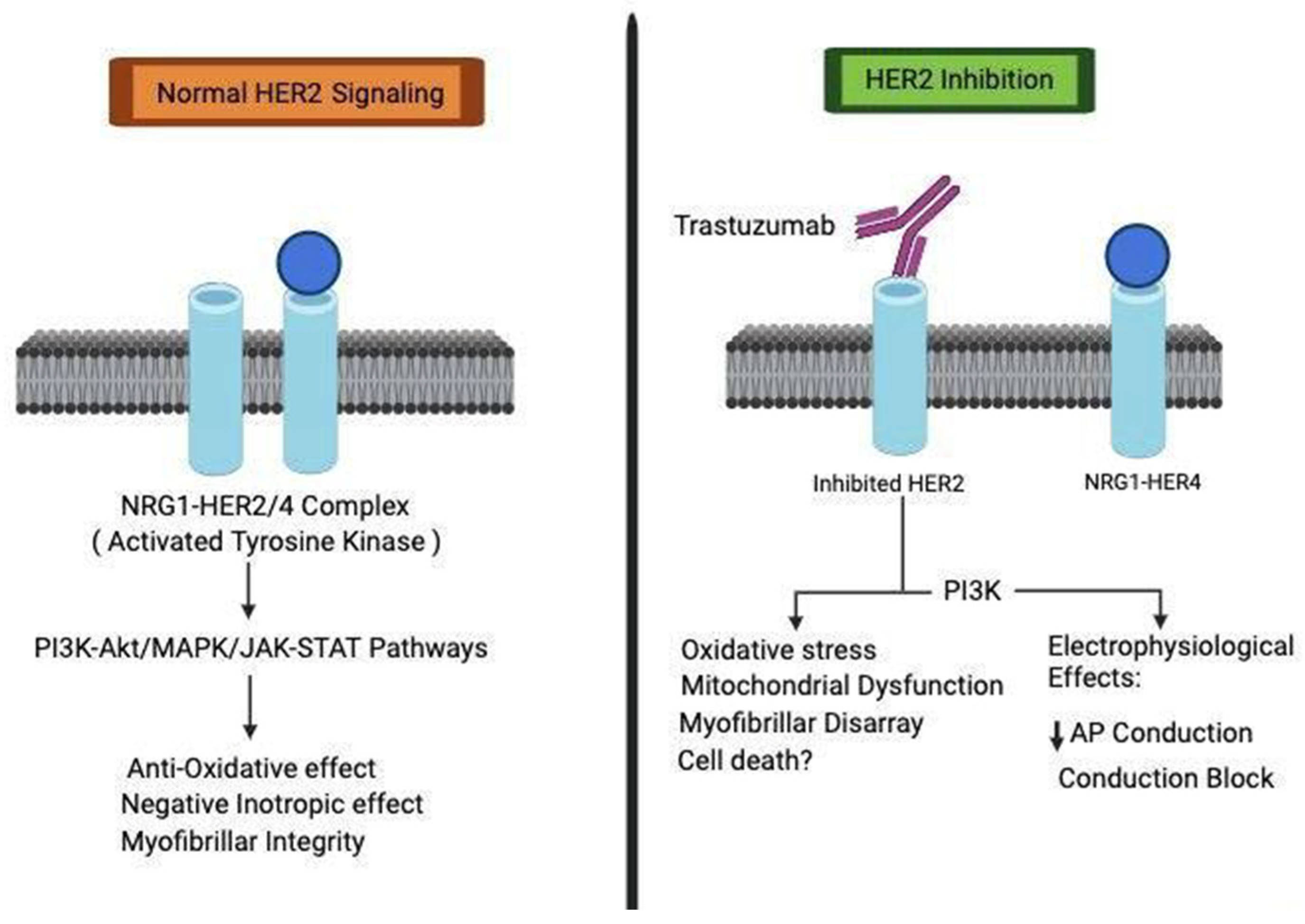
In addition, it is worth noting that HER2 signaling plays a significant role in cardiac development, as depicted in
Figure 1. Studies involving mice with heart-specific deletion of HER2 have demonstrated various signs of dilated cardiomyopathy. Recent investigations have further established a direct link between impaired HER2 signaling and trastuzumab-induced cardiotoxicity. Trastuzumab disrupts HER signaling by phosphorylating specific sites, namely 845 and 1248, on HER1 and HER2, respectively. This activation triggers the Erk/mTOR/Ulk 1 signaling pathway, inhibits autophagy, and accumulates reactive oxygen species in cardiomyocytes, ultimately contributing to cardiotoxicity. Notably, our research highlights that pertuzumab, an alternative monoclonal antibody targeting HER2 with a distinct binding site, does not interfere with HER2 signaling. This finding is consistent across both in vitro cardiomyocyte studies and clinical investigations [
3,
4,
5]. Unlike trastuzumab, pertuzumab does not disrupt Akt activity, a pathway that is downregulated by trastuzumab in HER2-positive breast cancer cells. The differential regulation of HER2 signaling in human cardiomyocytes and tumor cells subsequent to trastuzumab binding holds promise for elucidating the intricate mechanisms underlying trastuzumab-induced cardiotoxicity [
5].
Pertuzumab, commonly employed for the treatment of HER2 receptor-positive breast and gastrointestinal malignancies, can be administered either as a single agent or in combination with other chemotherapy medications. The recommended routes of administration include slow intravenous or subcutaneous infusion. Common adverse effects of pertuzumab comprise fever, headaches, and rash, while more severe side effects may involve heart failure or lung disease. Breast cancer is a complex disease that exhibits various characteristics and is a leading cause of death among women with cancer in the United States [
6]. Although metastatic breast cancer is generally not curable, the introduction of new systemic therapies has significantly improved survival rates. The choice of treatment depends on the presence of hormone receptor positivity or HER2 positivity in the tumor.
While trastuzumab has revolutionized the prognosis for individuals with HER2-positive breast cancer, it can often result in cardiac complications that hinder treatment [
7,
8].
Early studies involving trastuzumab, either alone or in combination with cisplatin, showed good tolerance. However, a subsequent study combining trastuzumab with anthracyclines revealed that 27% of HER2-positive breast cancer patients experienced cardiac issues, compared to less than 7% in the group treated with anthracyclines only. Retrospectively, it was suggested that 1 in 4 patients treated with trastuzumab in the adjuvant setting would develop left ventricular dysfunction. Larger subsequent studies confirmed the increased risk of cardiac problems associated with trastuzumab. As a result, subsequent trials adjusted their strategies by administering trastuzumab and chemotherapy separately, closely monitoring cardiac function, and excluding patients with pre-existing heart conditions. Initially, cardiac protective agents showed limited benefits; however, recent data suggest they may reduce the risk of cardiac problems. Despite these modifications, concerns about cardiotoxicity persist with trastuzumab-based regimens [
9,
10].
The standard treatment approach for breast cancer at various stages typically involves a combination of trastuzumab and anthracycline-based chemotherapy, such as doxorubicin. However, the precise mechanisms underlying cardiac complications associated with this combination therapy are not fully understood. Both doxorubicin and trastuzumab, whether administered individually or in combination, have been implicated in severe cardiac issues [
11]. Doxorubicin primarily affects DNA topoisomerase IIB (TOP2B) in the heart, leading to DNA damage and cell death in cardiomyocytes. It is hypothesized that in the absence of trastuzumab, the heart may be able to repair the damage caused by doxorubicin through mechanisms associated with normal HER2 function. However, trastuzumab, an anti-HER2 medication, may interfere with this function and potentially worsen cardiac injury. While the “repair-interfering model” seems plausible, there is insufficient experimental evidence to fully support it in the context of trastuzumab and anthracycline combination therapy-induced cardiac damage [
12,
13].
2. Review
Immune checkpoint molecules, such as CTLA-4 and PD-1, play pivotal roles in the modulation of T cell activity through their interactions with their respective ligands: CD80/CD86 and PD-L1. These interactions result in the suppression of T cell responses against tumors, thereby enabling tumor cells to evade immune-mediated destruction. Over the past years, the US Food and Drug Administration (FDA) has approved a number of monoclonal antibodies that specifically target these immune checkpoints, including ipilimumab and tremelimumab (anti-CTLA-4), nivolumab and pembrolizumab (anti-PD-1), and atezolizumab, avelumab, and durvalumab (anti-PD-L1). While these immune checkpoint inhibitors have revolutionized the management of advanced malignancies, they are also associated with a spectrum of potential adverse events, including myocarditis, cardiomyopathy, myocardial fibrosis, and heart failure. However, the precise underlying mechanisms responsible for these events remain largely elusive [
14].
In a study known as PANACEA, investigators examined the use of immune checkpoint antibodies alone or in combination with trastuzumab and anthracycline-based regimens. Among patients who received trastuzumab in conjunction with pembrolizumab, no initial cardiac disturbances were observed. However, immune-related adverse effects were encountered in 19% of these patients. Further investigations from this study and other relevant investigations are essential for evaluating the safety profile of combining trastuzumab with immune checkpoint inhibitors in terms of cardiac health [
15].
As an increasing number of cancer patients undergo HER2-targeted therapies that incorporate immune checkpoint inhibitors, the risk of cardiac complications elevates. Consequently, it is of utmost importance to comprehensively understand the underlying causes behind the potential cardiotoxicity induced by these medications, as well as to elucidate whether the concurrent use of these agents exacerbates the associated risk. Moreover, the identification of specific immunological characteristics that may render individuals more susceptible to cardiac complications arising from these therapeutic interventions is critical [
7,
16]. The urgency for developing time-sensitive and accurate bioassays, along with innovative non-invasive detection methods, cannot be overstated in the context of facilitating early identification of cardiotoxicity. These tools will play a vital role in supporting robust post-marketing surveillance programs for cancer drugs, ultimately leading to an enhanced quality of life for patients [
16].
Data from trials investigating adjuvant trastuzumab indicate that a significant percentage of patients experience declines in left ventricular ejection fraction (LVEF) without exhibiting symptoms, with rates ranging from 4.1% to 30.1%. Conversely, rates of symptomatic congestive heart failure (CHF) are relatively lower, varying from 0.6% to 3.8%. The HERA trial showcased higher rates of both CHF (0.8% and 0.8%) and LVEF decline (7.2% and 4.1%) in both the 2-year and 1-year trastuzumab arms compared to the observation group. However, no delayed cardiotoxicity was observed during the longer duration of follow-up (7–9 years). In NSABP B-31, CHF occurred in 2.6% of patients receiving trastuzumab, as opposed to 0.9% in the control group. Risk factors for CHF included an age of 60 or older, a baseline LVEF of 50–55%, and the usage of antihypertensive drugs. LVEF decline was observed in varying proportions (15.4%, 31.1%, and 27.1%) across different treatment groups. In the APT trial (trastuzumab and paclitaxel), lower rates of CHF (0.5%) and LVEF decline (3.2%) were observed. BCIRG 006 demonstrated higher rates of CHF in the AC-DH group (2.0%) compared to the AC-D group (0.7%) or TCH group (0.4%). A meta-analysis confirmed an elevated risk of grade 3 and 4 CHF with trastuzumab, albeit at low absolute rates. It is worth noting that most instances of LVEF decline resolve after discontinuation of treatment [
17]. The importance of evidence-based guidelines in the field of cardio-oncology is driven by substantial gaps in knowledge regarding screening for cardiotoxicity. It is vital to identify patients at high risk, although currently recognized risk factors such as age, baseline LVEF, hypertension, and exposure to anthracycline require further validation. The utilization of randomized trials and unbiased registries is critical in optimizing monitoring schedules and validating the effectiveness of interventions. For patients receiving trastuzumab regimens without cardiotoxicity risks, pivotal randomized trials comparing serial monitoring to reduced testing are necessary. Ongoing studies, such as SAFE-HEART, aim to investigate the safety of prolonged anti-HER2 therapy in patients with asymptomatic LVEF decline. The absence of well-designed studies impedes the establishment of precise screening and intervention guidelines, highlighting the necessity for collaboration among medical organizations. Informative studies are indispensable prior to the establishment of quality indicators, emphasizing the significance of robust research in guiding oncology and medical practices [
18,
19].
The utility of routine LVEF monitoring in early-stage breast cancer patients undergoing trastuzumab-based therapy remains a subject of debate. Despite almost a decade of follow-up data, the relationship between asymptomatic LVEF decline and heart failure in this patient population is not fully understood. Strong evidence demonstrating that early intervention in asymptomatic patients can prevent symptomatic heart failure is lacking [
20]. Routine LVEF monitoring has its limitations and can result in unnecessary diagnostic efforts due to error rates and false-positive results, potentially compromising treatment accuracy by wrongly identifying cardiotoxicity. The occurrence of both symptomatic and asymptomatic LVEF decline in these cases is very low. The connection between a low baseline LVEF and adverse cardiac outcomes suggests that a tailored monitoring approach may be more suitable. In conclusion, the value of routine LVEF monitoring for all early-stage breast cancer patients undergoing trastuzumab-based therapy is uncertain, particularly in cases without anthracycline treatment. Individualized risk assessment and monitoring strategies may offer a more appropriate approach to optimize patient care, minimize potential harm, and control costs [
20].
2.1. Clinical Utility of HER2 Testing
HER2 status plays a critical role in breast cancer and should be systematically evaluated in both newly diagnosed cases and cases that have metastasized. It serves as a predictive factor, indicating the potential for benefiting from treatment targeted at HER2. According to various guidelines, testing for HER2 expression is recommended for newly diagnosed, invasive, and metastatic breast cancers. Elevated levels of HER2 expression are associated with higher rates of disease recurrence and mortality, particularly when adjuvant systemic therapy is not utilized. However, the clinical significance of this prognostic information is uncertain, particularly in light of the earlier implementation of HER2-directed agents in the neoadjuvant and adjuvant settings. For individuals with hormone receptor-positive breast cancer, HER2 gene expression is an essential component of the 21-gene recurrence score assay [
21].
2.2. Recent Cardiotoxicity Surveillance
Contemporary guidelines propose the evaluation of left ventricular ejection fraction (LVEF) at the commencement and throughout breast cancer treatment to monitor cardiotoxicity. However, the existing data supporting these recommendations are limited. A case-control study involving 53 HER2-positive breast cancer patients with cardiotoxicity and 159 controls revealed that any reduction in LVEF to less than 55% at any point during treatment was associated with an increased risk of heart failure. The early identification of diminished LVEF during routine monitoring could facilitate the implementation of preventive strategies for heart failure [
22,
23,
24].
Emerging evidence suggests that assessing global longitudinal strain (GLS) can aid in the early detection of cardiac complications during cancer treatment. The SUCCOUR trial investigated whether utilizing GLS to guide early cardiac protection could prevent reductions in left ventricular ejection fraction (LVEF) in patients receiving chemotherapy that could be detrimental to the heart, compared to the standard LVEF-based approach. Although the trial did not identify a significant difference in the primary outcome (change in LVEF from baseline to one year between the groups), the GLS-guided approach exhibited fewer instances of cardiac complications over time (5.8% vs. 13.7%,
p = 0.02) [
24]. Further research is necessary to determine the long-term benefits of employing GLS in cancer or cardiac care.
Cardiotoxicity induced by anthracycline chemotherapy represents a significant and potentially life-threatening issue that diminishes the quality of life and compromises the efficacy of this treatment. Randomized controlled trials (RCTs) were identified for various interventions, including N-acetylcysteine, phenethylamines, coenzyme Q10, the combination of vitamin E, vitamin C, and N-acetylcysteine, L-carnitine, carvedilol, amifostine, and dexrazoxane. However, no RCTs were found for other potential cardioprotective measures, and non-randomized studies and case reports, which are prone to bias, were excluded [
4,
25]. Pooling the results of multiple interventions was not feasible due to the limited number of RCTs, variations in heart failure definitions, and methodological limitations. None of the included RCTs demonstrated a statistically significant difference in the incidence of heart failure, which may be attributed to small sample sizes and varying anthracycline doses. The efficacy of these cardioprotective interventions in preventing anthracycline-induced cardiac damage remains inconclusive. A more comprehensive and robust investigation is imperative to address this critical issue, particularly for dexrazoxane, which displayed promise in multiple RCTs involving adult breast cancer patients, although subgroup analyses for different patient populations posed challenges [
26,
27].
3. Conclusions
Trastuzumab-induced cardiomyopathy poses a significant challenge in the treatment of HER2-positive cancer. While trastuzumab is effective, its use often necessitates treatment discontinuation due to left ventricular systolic dysfunction. This review delves into the various aspects of trastuzumab-induced cardiomyopathy, including its mechanisms, diagnostic strategies, and potential interventions to protect cardiac health.
Understanding the complex mechanisms of trastuzumab, such as HER2 phosphorylation and signaling, underscores the need to balance cancer treatment efficacy with the prevention of cardiotoxicity. The concomitant use of trastuzumab with anthracycline-based chemotherapy further complicates the therapeutic landscape, necessitating investigation into the “repair-interfering model”. Moreover, the introduction of immune checkpoint inhibitors adds another layer of complexity, emphasizing the importance of assessing and monitoring cardiac risks as their combined use with trastuzumab becomes more prevalent.
Emerging surveillance methods for cardiotoxicity, such as global longitudinal strain (GLS), show promise for early intervention, especially as more patients are exposed to trastuzumab and immune checkpoint inhibitors. Collaboration among cardiologists, oncologists, and researchers is crucial for optimizing patient outcomes in the era of trastuzumab therapy. Evidence-based guidelines and personalized monitoring are essential to achieving a balance between effective cancer treatment and cardiovascular well-being. Addressing the complexities of trastuzumab-induced cardiomyopathy can significantly improve the quality of life for cancer patients and enhance the safety and efficacy of their treatment.



{kind=link}