
Customized versus Standard Epithelium Profiles in Transepithelial Photorefractive Keratectomy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Evaluation
2.2. Treatment Plan
2.3. Surgical Technique
2.4. Excimer Laser
2.5. Data Analysis
3. Results
3.1. Demographics
3.2. Epithelium Thickness
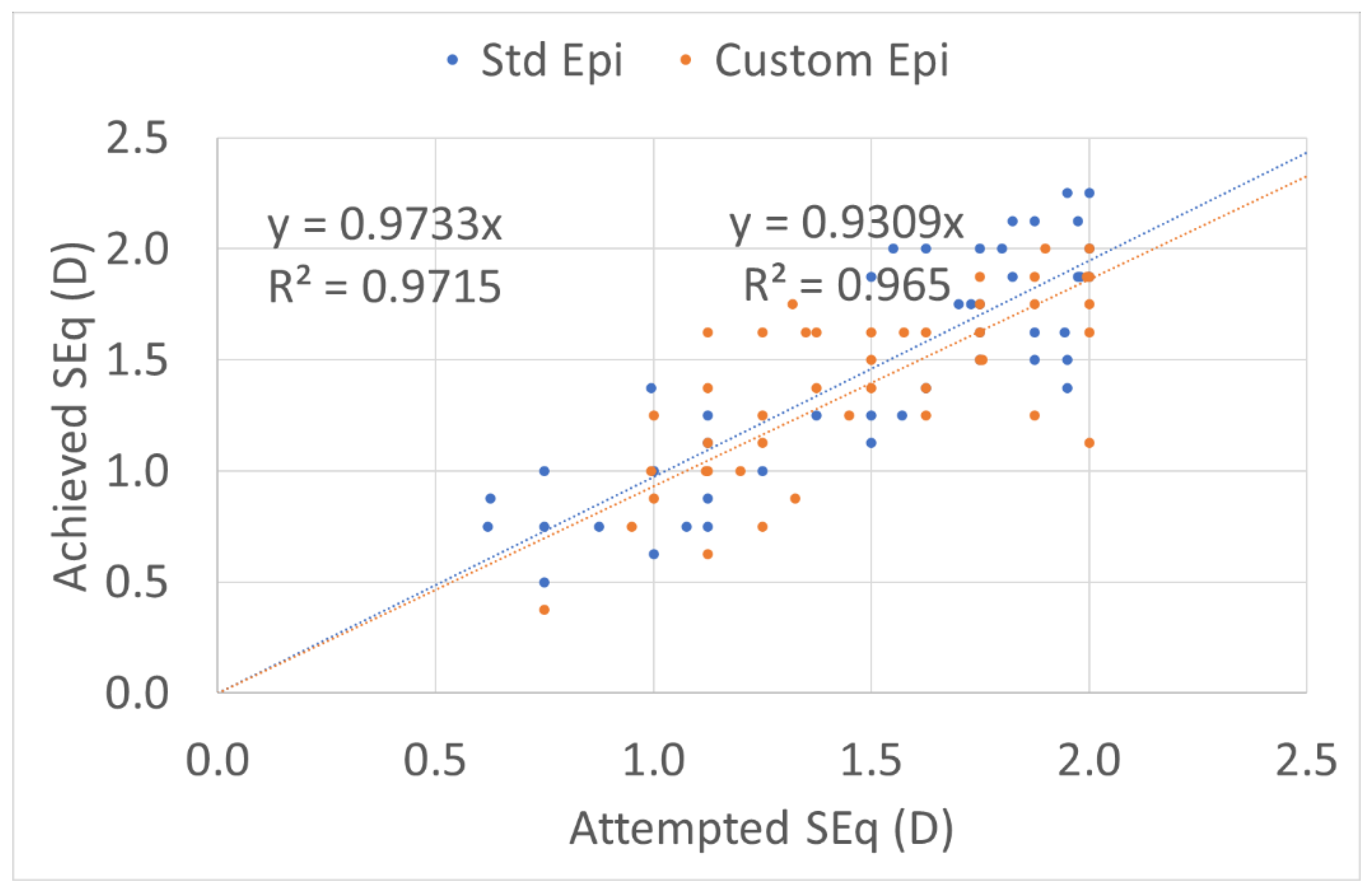
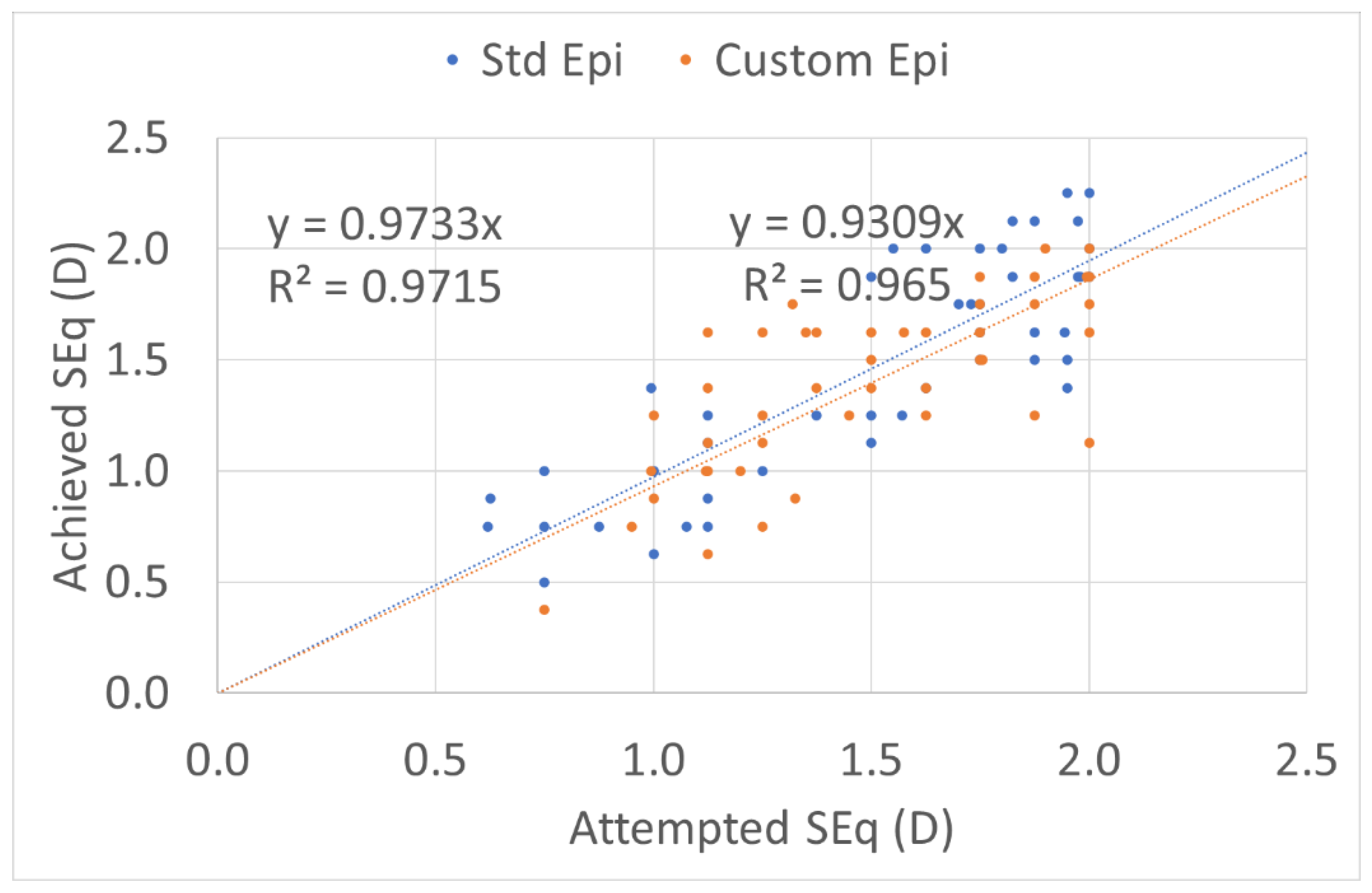
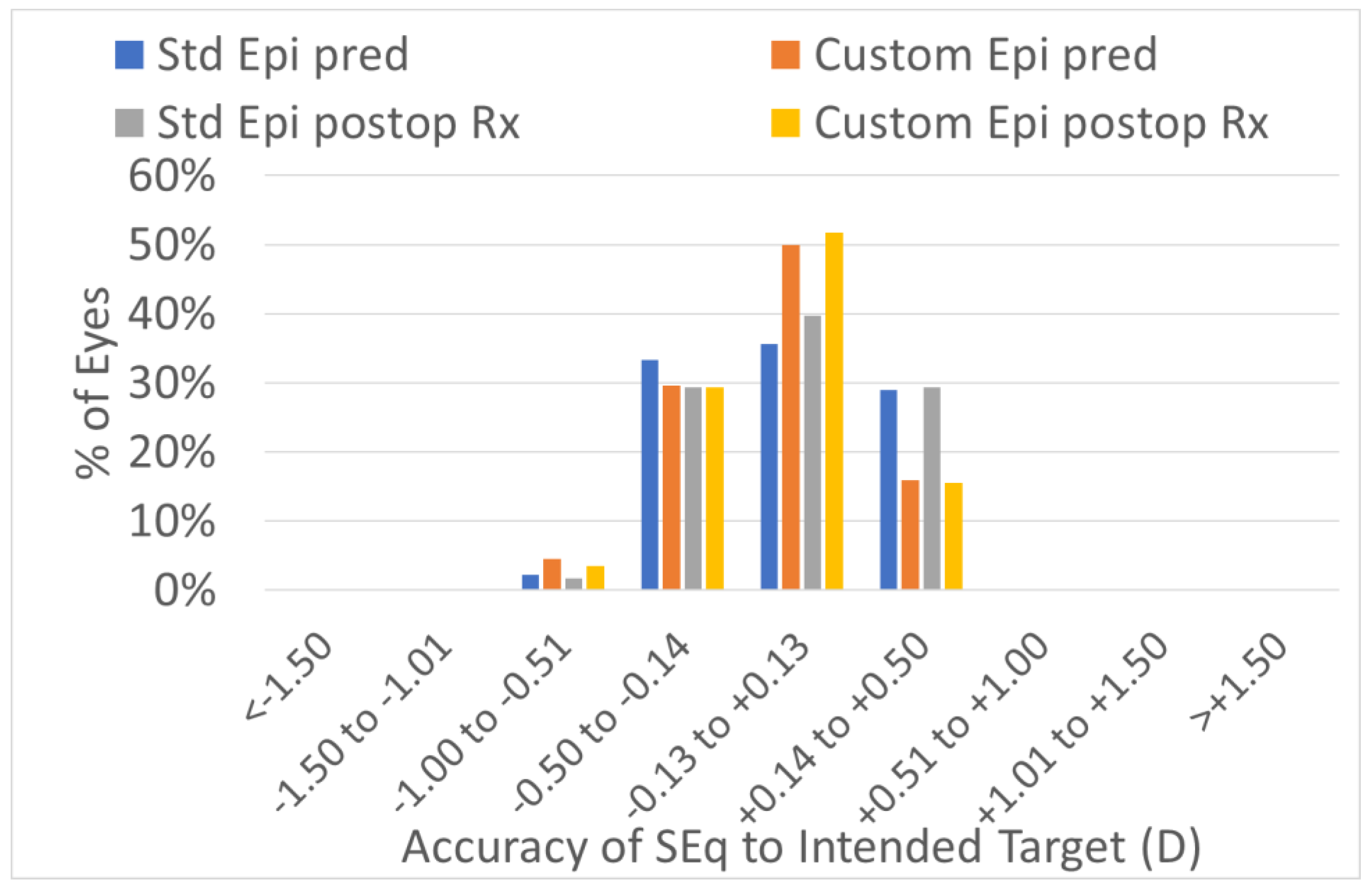
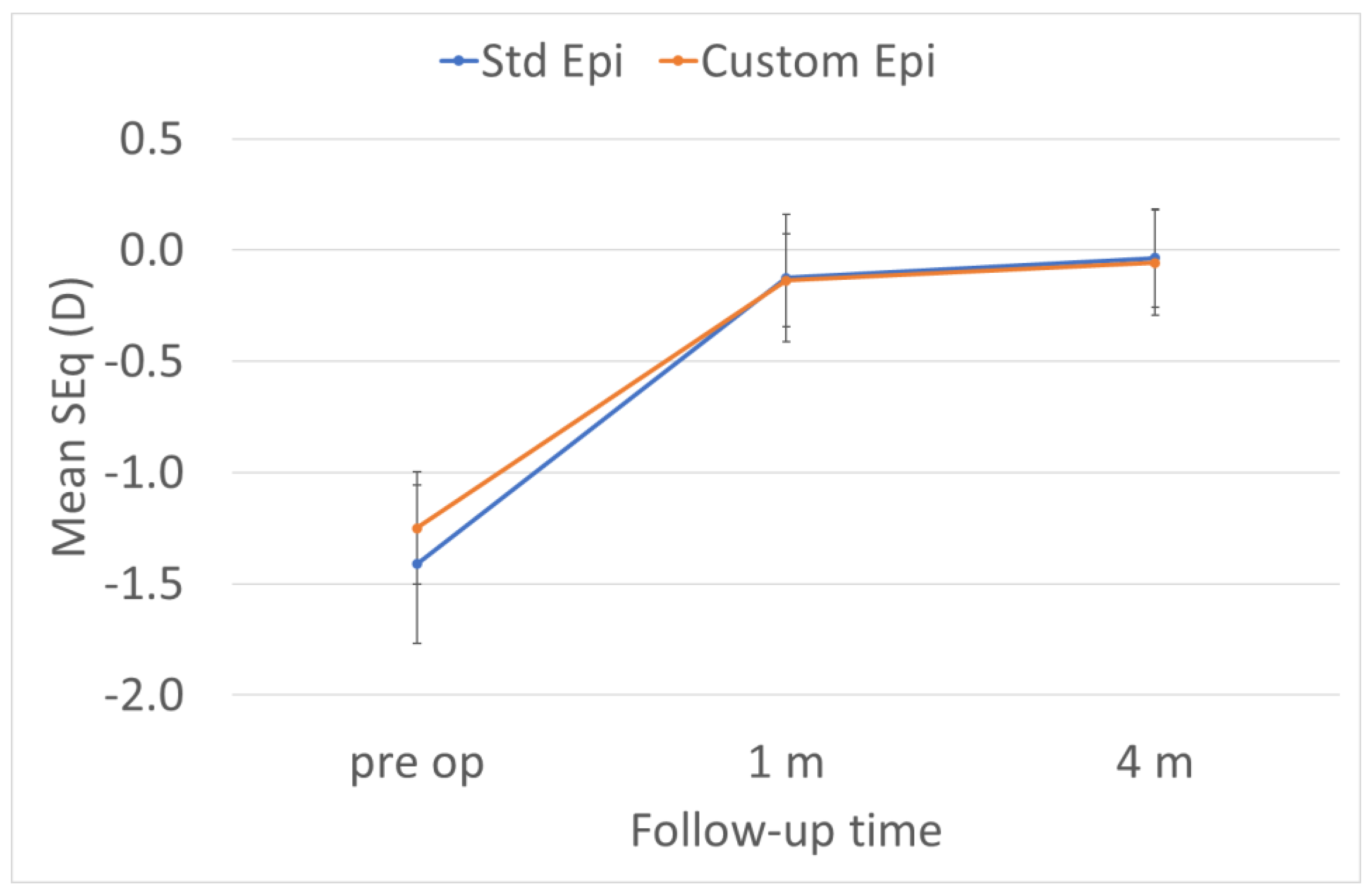
3.3. Predictability
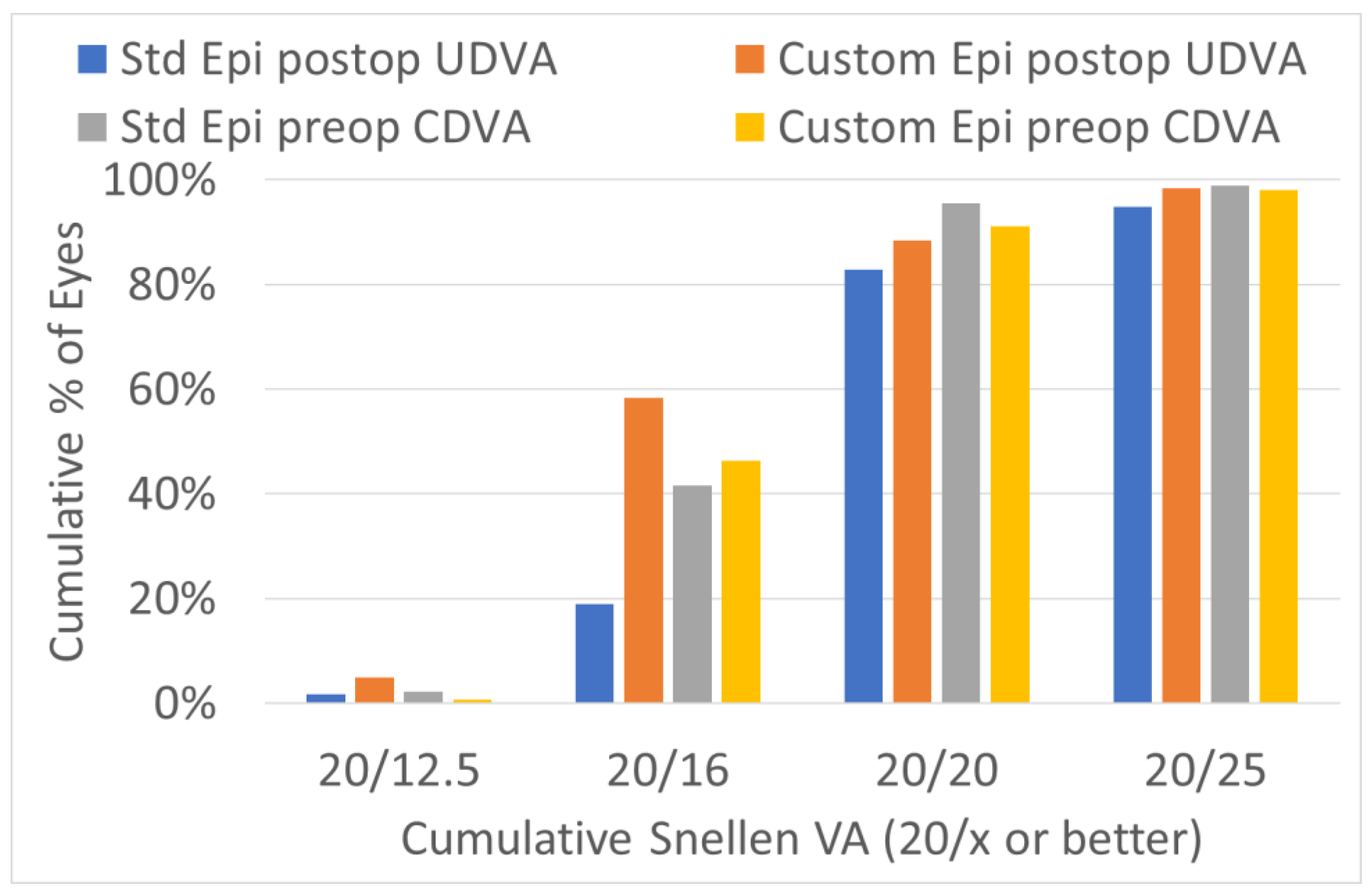
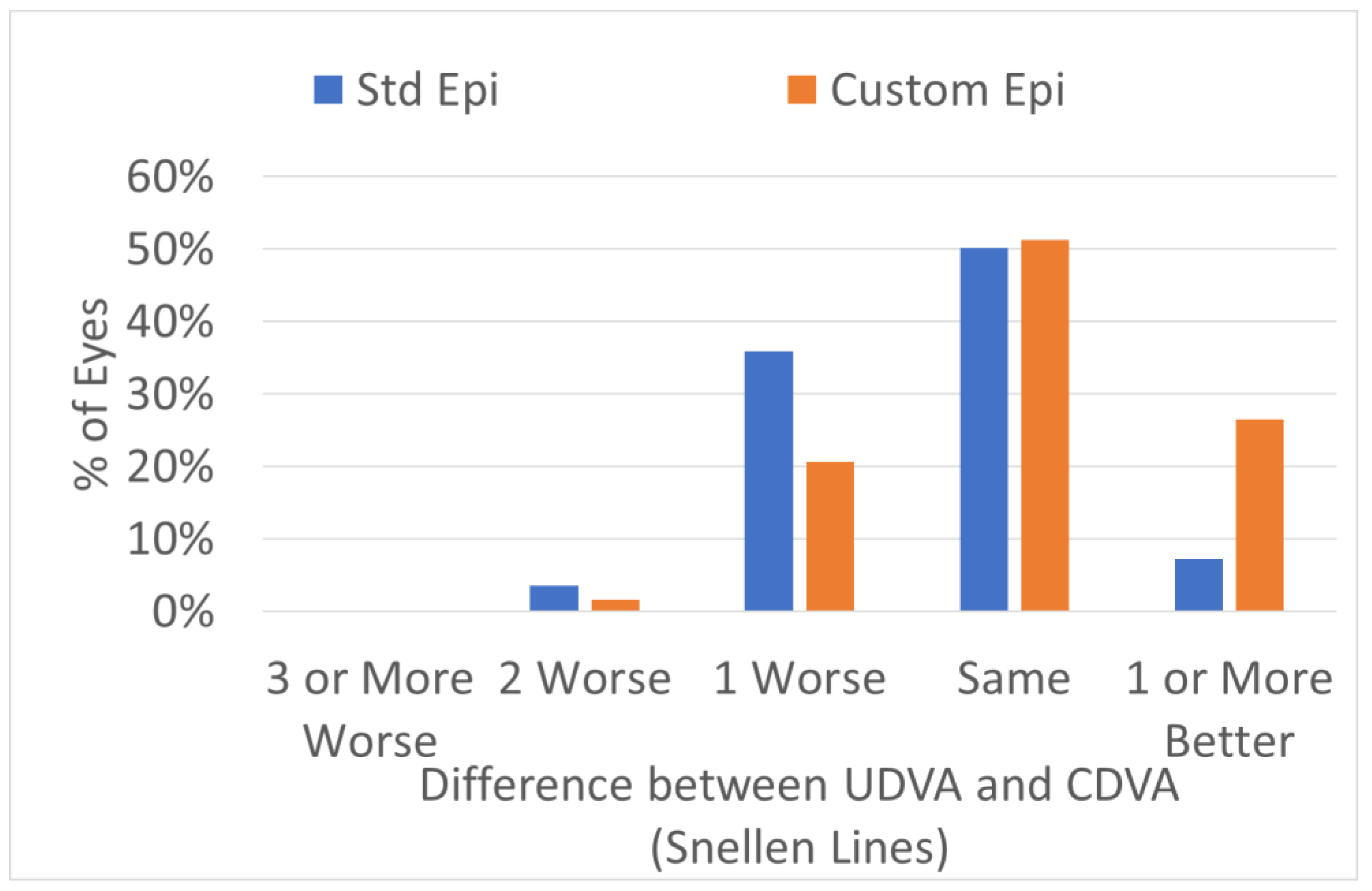
3.4. Efficacy
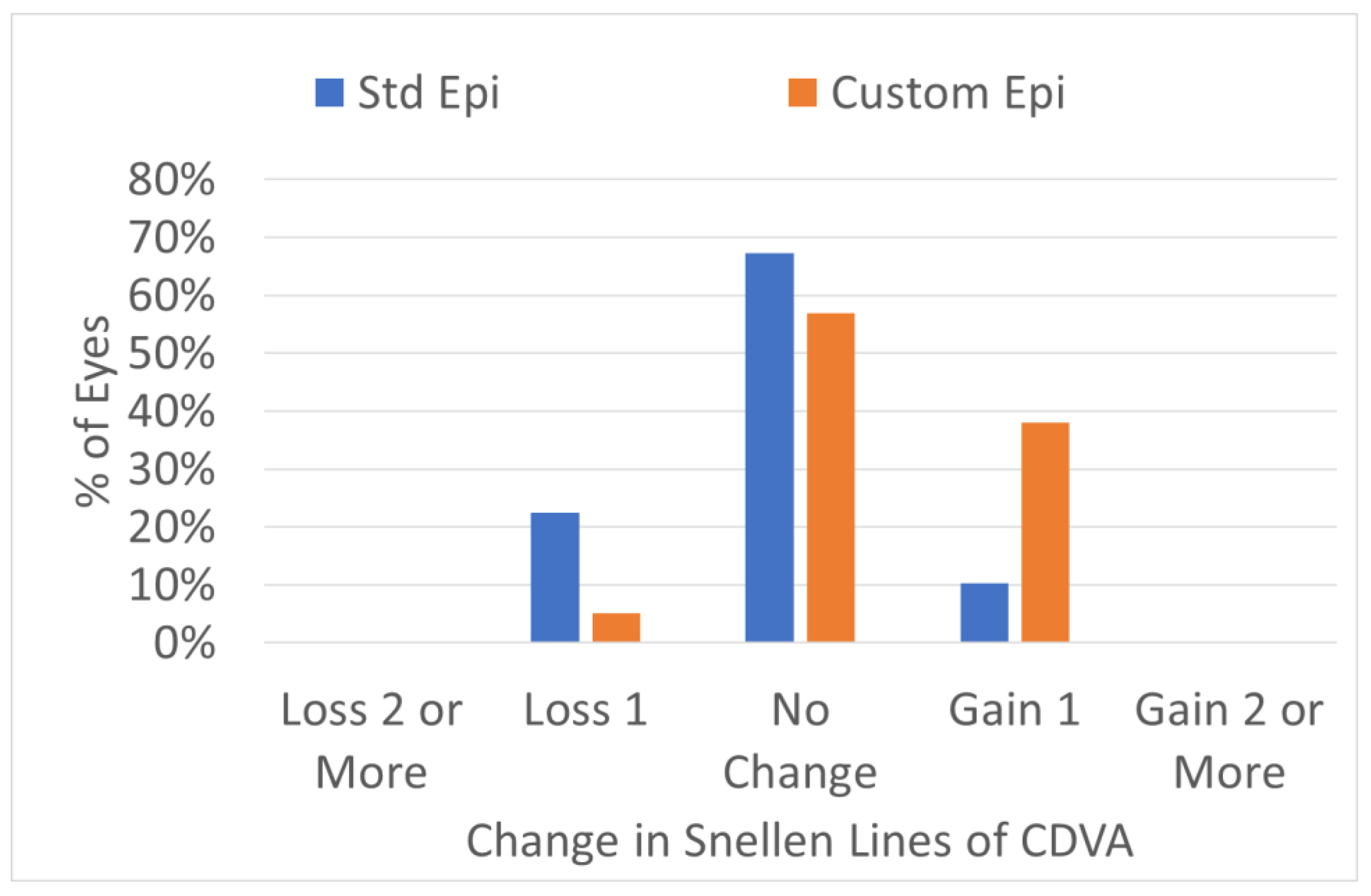
3.5. Safety
3.6. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aslanides, I.M.; Padroni, S.; Arba Mosquera, S.; Ioannides, A.; Mukherjee, A. Comparison of single-step reverse transepithelial all-surface laser ablation (ASLA) to alcohol-assisted photorefractive keratectomy. Clin. Ophthalmol. 2012, 6, 973–980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Ortueta, D.; von Rüden, D.; Arba-Mosquera, S. Comparison of Refractive and Visual Outcomes after Transepithelial Photorefractive Keratectomy (TransPRK) in Low versus Moderate Myopia. Photonics 2021, 8, 262. [Google Scholar] [CrossRef]
- Arba Mosquera, S.; Awwad, S.T. Theoretical analyses of the refractive implications of transepithelial PRK ablations. Br. J. Ophthalmol. 2013, 97, 905–911. [Google Scholar] [CrossRef] [PubMed]
- Hashmani, N.; Hashmani, S.; Saad, C.M. Wide Corneal Epithelial Mapping Using an Optical Coherence Tomography. Investig. Ophthalmol. Vis. Sci. 2018, 59, 1652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haque, S.; Jones, L.; Simpson, T. Thickness Mapping of the Cornea and Epithelium Using Optical Coherence Tomography. Optom. Vis. Sci. 2008, 85, E963–E976. [Google Scholar] [CrossRef] [PubMed]
- Mohammadpour, M.; Heidari, Z. MS-39®. In Diagnostics in Ocular Imaging; Mohammadpour, M., Ed.; Springer International Publishing: Cham, Switzerland, 2021; pp. 265–284. ISBN 978-3-030-54862-9. [Google Scholar]
- Vinciguerra, P.; Camesasca, F.I.; Vinciguerra, R.; Arba-Mosquera, S.; Torres, I.; Morenghi, E.; Randleman, J.B. Advanced Surface Ablation with a New Software for the Reduction of Ablation Irregularities. J. Refract. Surg. 2017, 33, 89–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arba-Mosquera, S.; de Ortueta, D. Geometrical analysis of the loss of ablation efficiency at non-normal incidence. Opt. Express 2021, 16, 3877–3895. [Google Scholar] [CrossRef] [PubMed]
- de Ortueta, D.; Schreyger, F.D. Centration on the cornea vertex normal during hyperopic refractive photoablation using videokeratoscopy. J. Refract. Surg. 2007, 23, 198–200. [Google Scholar] [CrossRef] [PubMed]
- Arbelaez, M.C.; Vidal, C.; Arba-Mosquera, S. Clinical outcomes of corneal vertex versus central pupil references with aberration-free ablation strategies and LASIK. Investig. Ophthalmol. Vis. Sci. 2008, 49, 5287–5294. [Google Scholar] [CrossRef] [PubMed]
- Arba-Mosquera, S.; Hollerbach, T. Ablation Resolution in Laser Corneal Refractive Surgery: The Dual Fluence Concept of the AMARIS Platform. Adv. Opt. Technol. 2010, 2010, 538541. [Google Scholar] [CrossRef] [Green Version]
- Seiler, T.; Kriegerowski, M.; Schnoy, N.; Bende, T. Ablation rate of human corneal epithelium and Bowman’s layer with the excimer laser (193 nm). Refract. Refract. Surg. 1990, 6, 99–102. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Swanson, E.; Lin, C.; Schuman, J.; Stinson, W.; Chang, W.; Hee, M.; Flotte, T.; Gregory, K.; Puliafito, C.; et al. Optical coherence tomography. Science 1991, 254, 1178–1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Meisler, D.M.; Tang, M.; Lu, A.T.H.; Thakrar, V.; Reiser, B.J.; Huang, D. Keratoconus Diagnosis with Optical Coherence Tomography Pachymetry Mapping. Ophthalmology 2008, 115, 2159–2166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savini, G.; Schiano-Lomoriello, D.; Hoffer, K.J. Repeatability of automatic measurements by a new anterior segment optical coherence tomographer combined with Placido topography and agreement with 2 Scheimpflug cameras. J. Cataract Refract. Surg. 2018, 44, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Khamar, P.; Rao, K.; Wadia, K.; Dalal, R.; Grover, T.; Versaci, F.; Gupta, K. Advanced epithelial mapping for refractive surgery. Indian J. Ophthalmol. 2020, 68, 2819. [Google Scholar] [CrossRef] [PubMed]
- Vega-Estrada, A.; Mimouni, M.; Espla, E.; Alió del Barrio, J.; Alio, J.L. Corneal Epithelial Thickness Intrasubject Repeatability and its Relation With Visual Limitation in Keratoconus. Am. J. Ophthalmol. 2019, 200, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Eckard, A.; Stave, J.; Guthoff, R.F. In vivo investigations of the corneal epithelium with the confocal Rostock Laser Scanning Microscope (RLSM). Cornea 2006, 25, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Reinstein, D.Z.; Archer, T.J.; Gobbe, M.; Silverman, R.H.; Coleman, D.J. Epithelial thickness in the normal cornea: Three-dimensional display with Artemis very high-frequency digital ultrasound. J. Refract. Surg. 2008, 24, 571–581. [Google Scholar] [PubMed]
- Jun, I.; Yong Kang, D.S.; Arba-Mosquera, S.; Jean, S.K.; Kim, E.K.; Seo, K.Y.; Kim, T.-I. Clinical outcomes of mechanical and transepithelial photorefractive keratectomy in low myopia with a large ablation zone. J. Cataract Refract. Surg. 2019, 45, 977–984. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Epithelial Profile | Central Thickness | Peripheral Thickness @4 mm Radial Distance | Remarks |
|---|---|---|---|
| Standard | 55 µm | 65 µm | Population based epithelium covering >75% of the normal population |
| Optimized (Standard + 5 µm) | 60 µm | 70 µm | Optimized population based epithelium covering >95% of the normal population |
| Customized (as measured by OCT) | 40–75 µm (as measured centrally using MS-39) | Central thickness + 10 µm | According to Impact of the Reference Point for Epithelial Thickness Measurements. Arba-Mosquera S, Awwad ST. J Refract Surg. 1 March 2020; 36(3):200–207 |
| Standard Epithelium X ± SD Range | Customized Epithelium X ± SD Range | p-Value between Groups | |||
|---|---|---|---|---|---|
| Number of eyes | 58 | 58 | --- | ||
| Age (years) | 35 ± 11 | 18 to 64 | 32 ± 9 | 18 to 56 | 0.1 |
| UDVA (Snellen) | 20/80 ± 11 | 20/20 to 20/400 | 20/80 ± 9 | 20/20 to 20/400 | 0.4 |
| CDVA (Snellen) | 20/18 ± 4 | 20/12 to 20/32 | 20/18 ± 3 | 20/12 to 20/32 | 0.5 |
| Spherical equivalent (D) | −1.41 ± 0.43 | −2.0 to −0.5 | −1.43 ± 0.36 | −2 to −0.75 | 0.4 |
| Astigmatism (D) | 0.8 ± 0.69 | 0 to 2.5 | 0.83 ± 0.70 | 0 to 3 | 0.4 |
| Central corneal thickness (µm) | 551 ± 35 | 442 to 666 | 553 ± 26 | 467 to 657 | 0.4 |
| Optical zone (mm) | 7.1 ± 0.2 | 6.7 to 7.7 | 6.8 ± 0.2 | 6.3 to 7.4 | <0.0001 |
| Total ablation zone (mm) | 8.2 ± 0.3 | 7.5 to 9.5 | 7.9 ± 0.3 | 7.4 to 9.0 | <0.0001 |
| Total ablation depth (µm) | 90 ± 9 | 67 to 142 | 86 ± 9 | 88 to 175 | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Ortueta, D.; von Rüden, D.; Arba-Mosquera, S. Customized versus Standard Epithelium Profiles in Transepithelial Photorefractive Keratectomy. Optics 2021, 2, 266-275. https://doi.org/10.3390/opt2040025
de Ortueta D, von Rüden D, Arba-Mosquera S. Customized versus Standard Epithelium Profiles in Transepithelial Photorefractive Keratectomy. Optics. 2021; 2(4):266-275. https://doi.org/10.3390/opt2040025
Chicago/Turabian Stylede Ortueta, Diego, Dennis von Rüden, and Samuel Arba-Mosquera. 2021. "Customized versus Standard Epithelium Profiles in Transepithelial Photorefractive Keratectomy" Optics 2, no. 4: 266-275. https://doi.org/10.3390/opt2040025
APA Stylede Ortueta, D., von Rüden, D., & Arba-Mosquera, S. (2021). Customized versus Standard Epithelium Profiles in Transepithelial Photorefractive Keratectomy. Optics, 2(4), 266-275. https://doi.org/10.3390/opt2040025