
Preliminary Study on the Development of a Real-Time Pressure-Monitoring Facial Mask for Burn Rehabilitation

 , ,
, ,
Abstract
1. Introduction
2. Methods
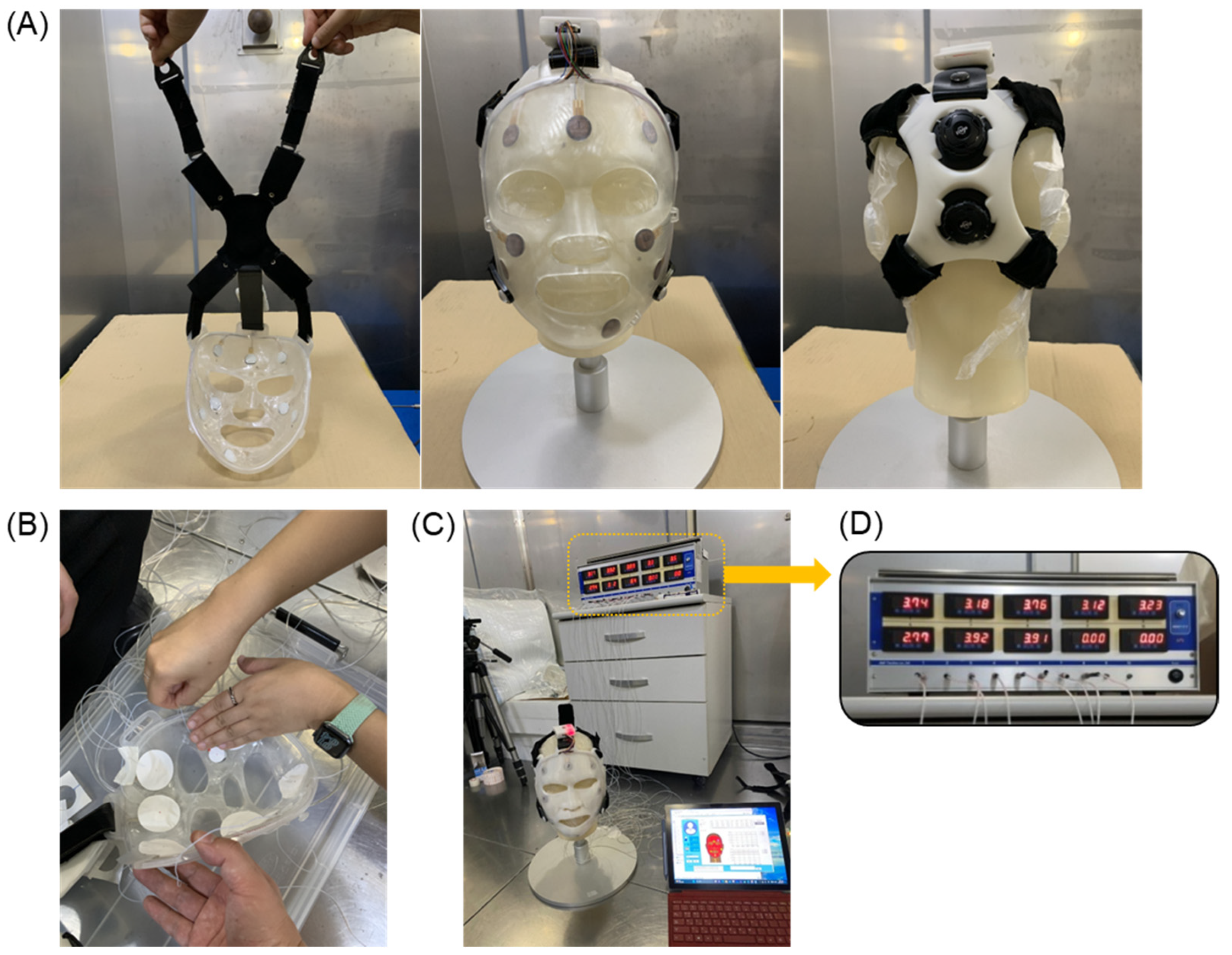
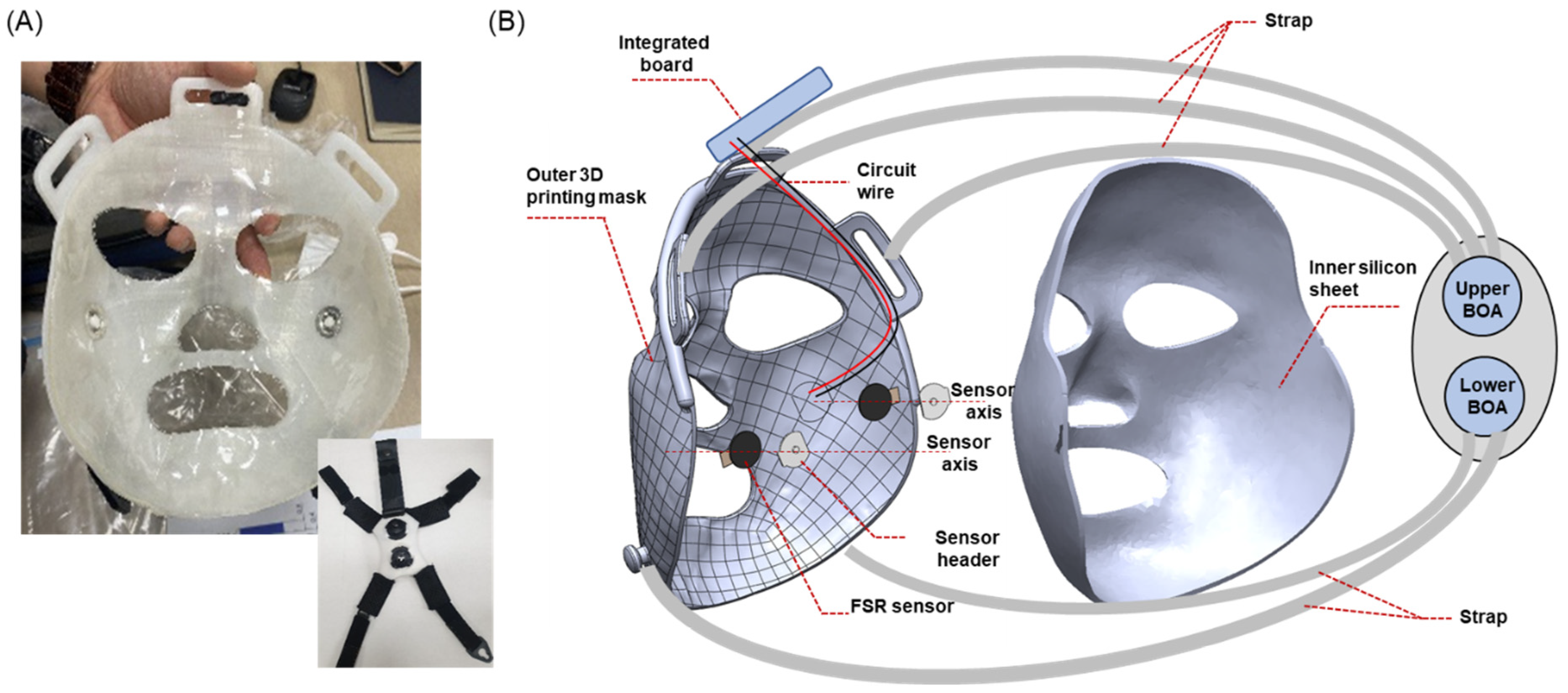
2.1. Burn Mask Design and Manufacturing of Facial Masks
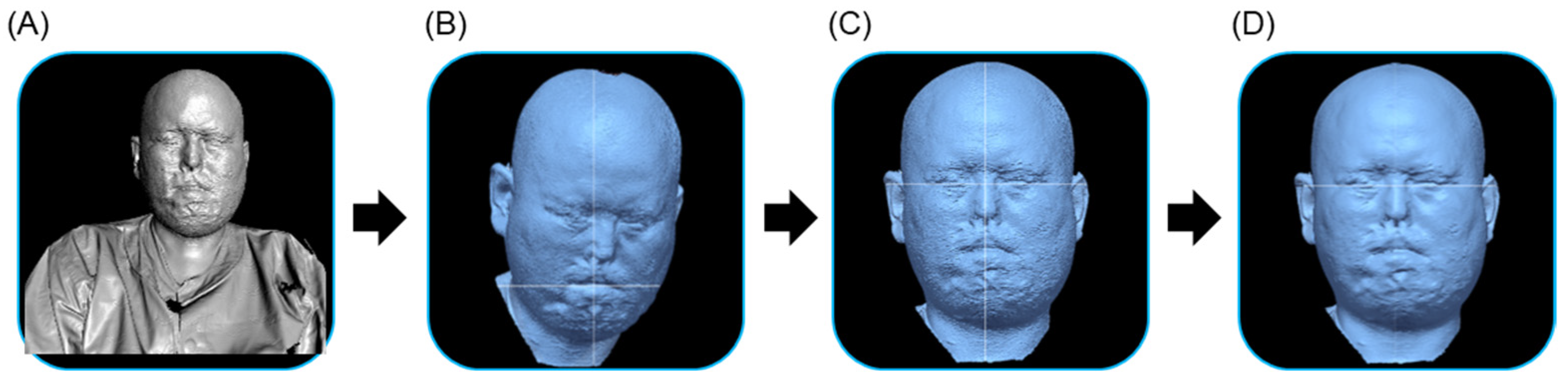
2.1.1. 3D Scanning of Patient’s Face
2.1.2. Generation of Facial Mask Model
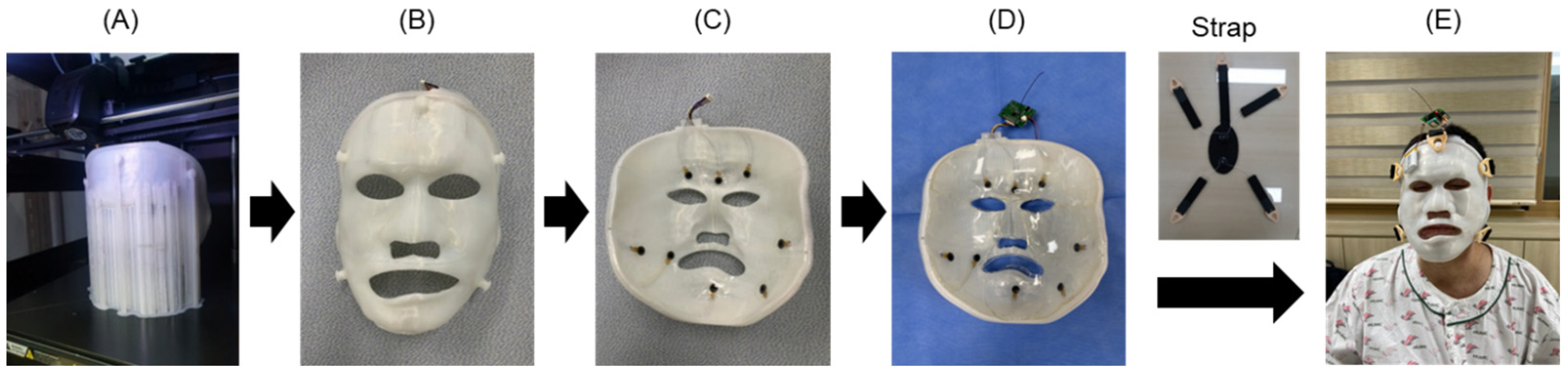
2.1.3. 3D Printing Production and Assembly of the Burn Facial Mask
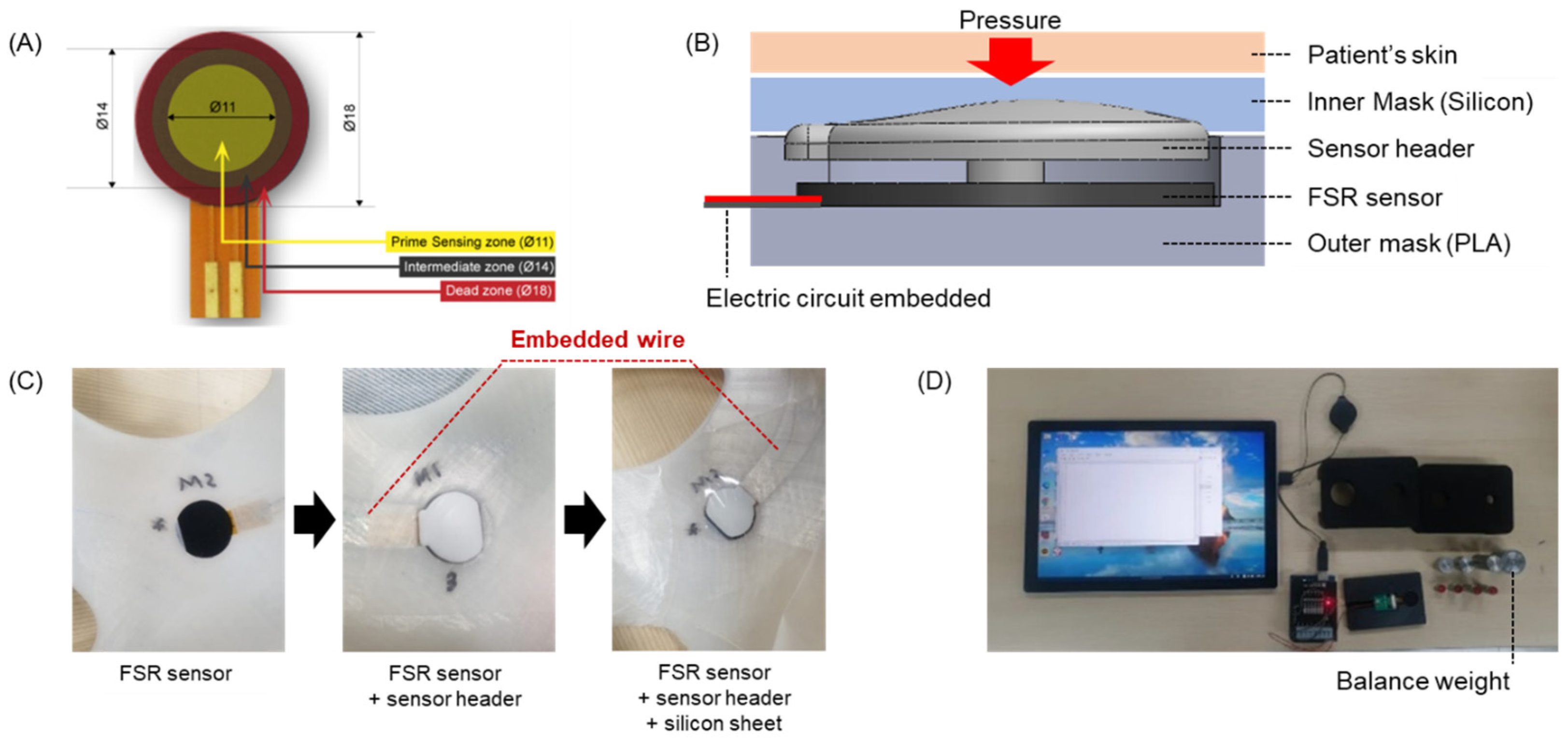
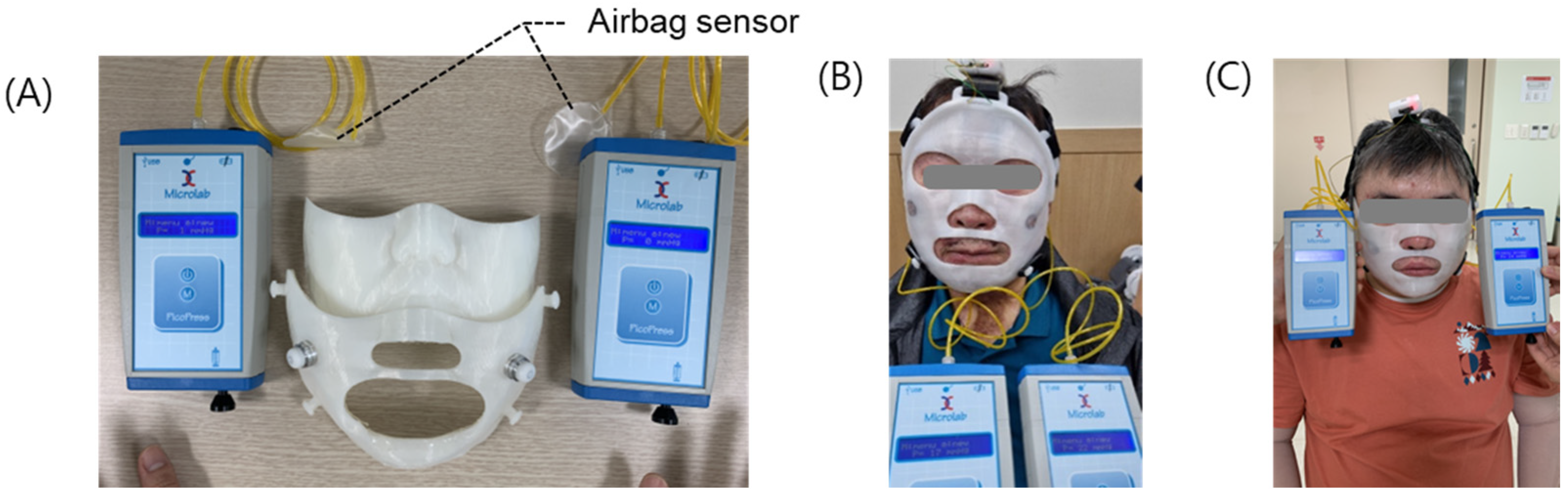
2.2. Development of the Pressure-Sensing Module for Real-Time Measurements
2.3. Development of the Strap System
2.4. Clinical Test Method
3. Results
3.1. Sensor Calibration and Monitoring
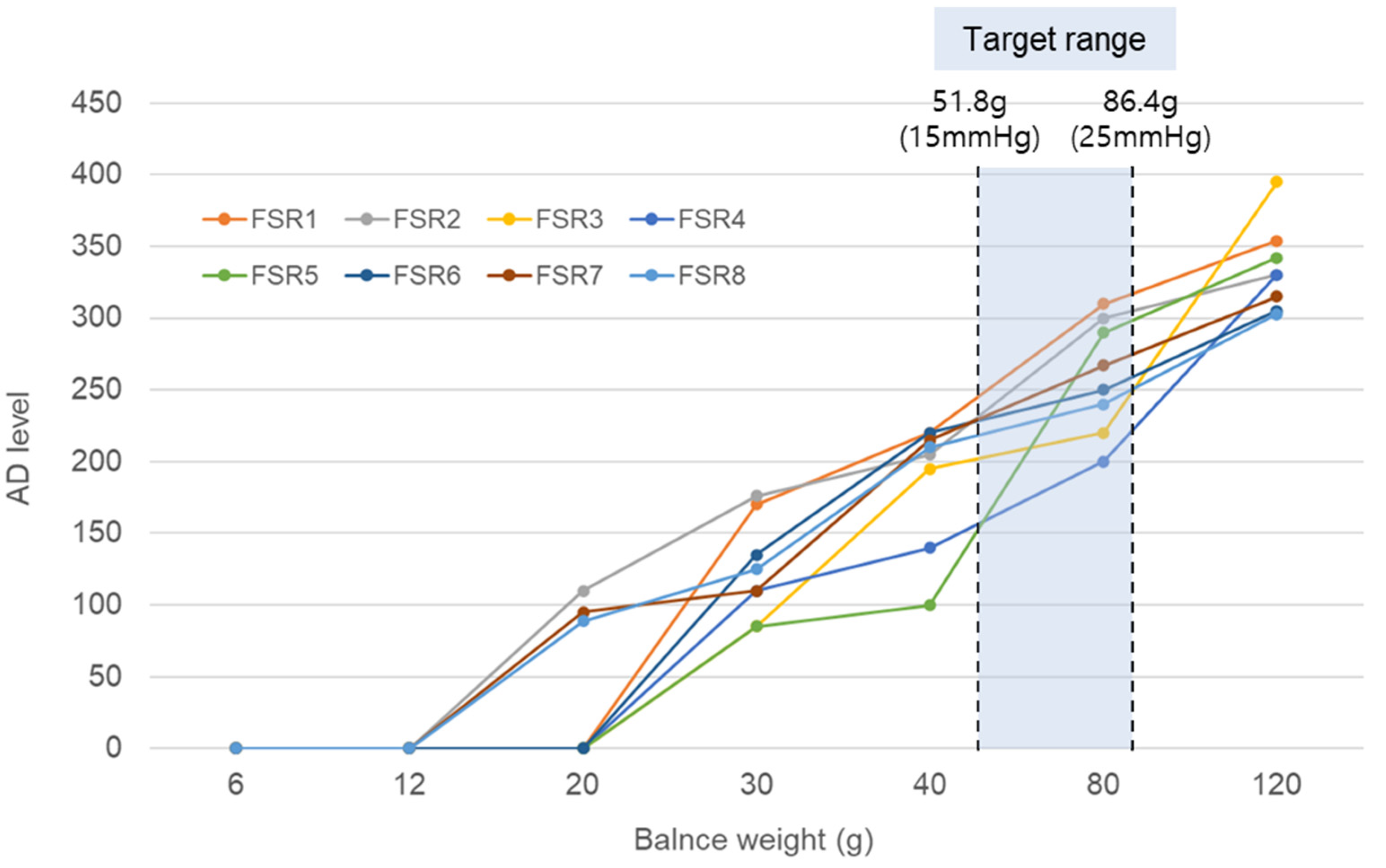
3.1.1. Sensor Grouping
3.1.2. Simultaneous Pressure Measurement Results
3.1.3. Pressure Sensor Calibration with Air Cell Measurement System Before Clinical Test
3.2. Clinical Tests
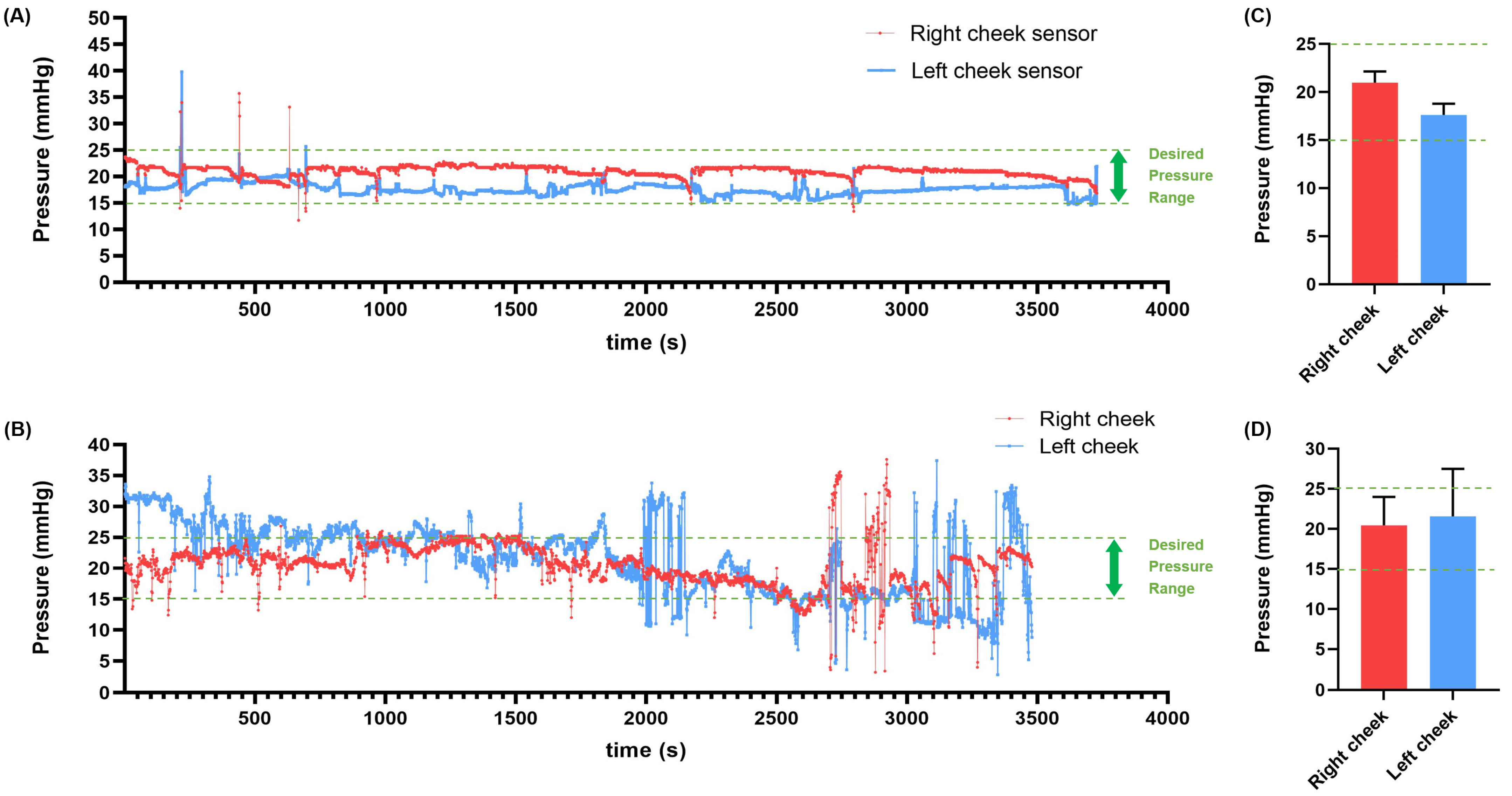
3.2.1. Daily Pressure Measurements
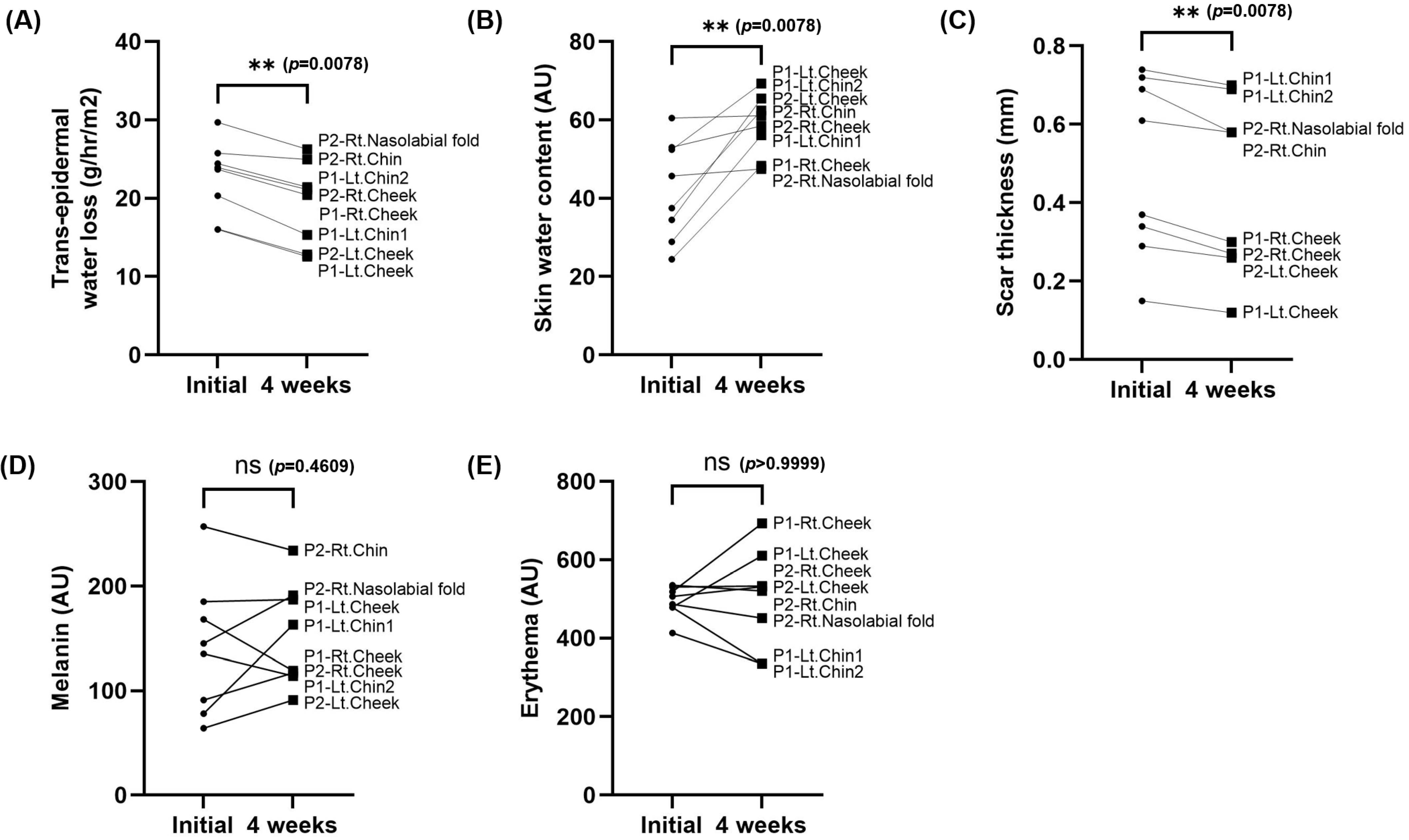
3.2.2. Clinical Test Results
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hwang, S.-H.; Park, S.-Y. Hospital-Based Social Welfare Service Needs among Caregivers of Adult Burn Survivors. Health Soc. Welf. Rev. 2024, 44, 30–49. [Google Scholar] [CrossRef]
- American Burn Association. National Burn Repository: Report of Data from 2006–2015; American Burn Association: Chicago, IL, USA, 2016. [Google Scholar]
- Kim, D.C.; Lee, R.; Kim, J.H.; Lee, H.Y.; Jung, D.J.; Kim, T.Y.; Tark, K.C.; LEE, C.J. Epidemiology of Burns in Korea from 2010 to 2014. J. Korean Burn Soc. 2015, 18, 1–6. [Google Scholar]
- Lawrence, J.W.; Mason, S.T.; Schomer, K.; Klein, M.B. Epidemiology and Impact of Scarring After Burn Injury: A Systematic Review of the Literature. J. Burn Care Res. 2012, 33, 136–146. [Google Scholar] [CrossRef]
- Bloemen, M.C.T.; van der Veer, W.M.; Ulrich, M.M.W.; van Zuijlen, P.P.M.; Niessen, F.B.; Middelkoop, E. Prevention and curative management of hypertrophic scar formation. Burns 2009, 35, 463–475. [Google Scholar] [CrossRef]
- Wolfram, D.; Tzankov, A.; Pulzl, P.; Piza-Katzer, H. Hypertrophic scars and keloids—A review of their pathophysiology, risk factors, and therapeutic management. Dermatol. Surg. 2009, 35, 171–181. [Google Scholar] [CrossRef]
- Dobson, G.P.; Morris, J.L.; Letson, H.L. Pathophysiology of Severe Burn Injuries: New Therapeutic Opportunities from a Systems Perspective. J. Burn Care Res. 2024, 45, 1041–1050. [Google Scholar] [CrossRef]
- Thomas, D.W.; Hopkinson, I.; Harding, K.G.; Shepherd, J.P. The pathogenesis of hypertrophic/ keloid scarring. Int. J. Oral Maxillofac. Surg. 1994, 23, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Borchers, A.; Pieler, T. Programming pluripotent precursor cells derived from Xenopus embryos to generate specific tissues and organs. Genes 2010, 1, 413–426. [Google Scholar] [CrossRef]
- Bock, O.; Schmid-Ott, G.; Malewski, P.; Mrowietz, U. Quality of life of patients with keloid and hypertrophic scarring. Arch. Dermatol. Res. 2006, 297, 433–438. [Google Scholar] [CrossRef]
- Ye, E.M. Psychological morbidity in patients with facial and neck burns. Burns 1998, 24, 646–648. [Google Scholar] [CrossRef]
- Reid, W.H.; Evans, J.H.; Naismith, R.S.; Tully, A.E.; Sherwin, S. Hypertrophic scarring and pressure therapy. Burn. Incl. Therm. Inj. 1987, 13, S29–S32. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Li-Tsang, C.W.P.; Deng, X.; Wang, X.; Wang, H.; Zhang, Y.; Tan, Z.; He, C. The recovery of post-burn hypertrophic scar in a monitored pressure therapy intervention programme and the timing of intervention. Burns 2018, 44, 1451–1467. [Google Scholar] [CrossRef]
- Li-Tsang, C.W.; Feng, B.; Huang, L.; Liu, X.; Shu, B.; Chan, Y.T.; Cheung, K.K. A histological study on the effect of pressure therapy on the activities of myofibroblasts and keratinocytes in hypertrophic scar tissues after burn. Burns 2015, 41, 1008–1016. [Google Scholar] [CrossRef] [PubMed]
- Ai, J.W.; Liu, J.T.; Pei, S.D.; Liu, Y.; Li, D.S.; Lin, H.M.; Pei, B. The effectiveness of pressure therapy (15–25 mmHg) for hypertrophic burn scars: A systematic review and meta-analysis. Sci. Rep. 2017, 7, 40185. [Google Scholar] [CrossRef]
- Candy, L.H.; Cecilia, L.T.; Ping, Z.Y. Effect of different pressure magnitudes on hypertrophic scar in a Chinese population. Burns 2010, 36, 1234–1241. [Google Scholar] [CrossRef] [PubMed]
- Van den Kerckhove, E.; Stappaerts, K.; Fieuws, S.; Laperre, J.; Massage, P.; Flour, M.; Boeckx, W. The assessment of erythema and thickness on burn related scars during pressure garment therapy as a preventive measure for hypertrophic scarring. Burns 2005, 31, 696–702. [Google Scholar] [CrossRef]
- Williams, F.; Knapp, D.; Wallen, M. Comparison of the characteristics and features of pressure garments used in the management of burn scars. Burns 1998, 24, 329–335. [Google Scholar] [CrossRef]
- Wiseman, J.; Simons, M.; Kimble, R.; Tyack, Z. Variability of pressure at the pressure garment-scar interface in children after burn: A pilot longitudinal cohort study. Burns 2019, 45, 103–113. [Google Scholar] [CrossRef]
- Brown, C.A. A comparison of the outcomes of two clinical audits of burn pressure garment satisfaction and compliance in Saudi Arabia. Burns 2001, 27, 342–348. [Google Scholar] [CrossRef]
- Atiyeh, B.S.; El Khatib, A.M.; Dibo, S.A. Pressure garment therapy (PGT) of burn scars: Evidence-based efficacy. Ann. Burn. Fire Disasters 2013, 26, 205–212. [Google Scholar]
- Macintyre, L.; Baird, M. Pressure garments for use in the treatment of hypertrophic scars—A review of the problems associated with their use. Burns 2006, 32, 10–15. [Google Scholar] [CrossRef]
- Lin, J.T.; Nagler, W. Use of surface scanning for creation of transparent facial orthoses. A report of two cases. Burns 2003, 29, 599–602. [Google Scholar] [CrossRef] [PubMed]
- Shons, A.R.; Rivers, E.A.; Solem, L.D. A rigid transparent face mask for control of scar hypertrophy. Ann. Plast. Surg. 1981, 6, 245–248. [Google Scholar] [CrossRef]
- Wei, Y.; Wang, Y.; Zhang, M.; Yan, G.; Wu, S.; Liu, W.; Ji, G.; Li-Tsang, C.W.P. The application of 3D-printed transparent facemask for facial scar management and its biomechanical rationale. Burns 2018, 44, 453–461. [Google Scholar] [CrossRef]
- Wei, Y.; Li-Tsang, C.W.P.; Liu, J.; Xie, L.; Yue, S. 3D-printed transparent facemasks in the treatment of facial hypertrophic scars of young children with burns. Burns 2017, 43, e19–e26. [Google Scholar] [CrossRef] [PubMed]
- Rivers, E.A.; Strate, R.G.; Solem, L.D. The transparent face mask. Am. J. Occup. Ther. Off. Publ. Am. Occup. Ther. Assoc. 1979, 33, 108–113. [Google Scholar]
- Kant, S.B.; Colla, C.; van den Kerckhove, E.; Piatkowski de Grzymala, A. Clinical effects of transparent facial pressure masks: A literature review. Prosthet. Orthot. Int. 2019, 43, 349–355. [Google Scholar] [CrossRef]
- Parry, I.; Hanley, C.; Niszczak, J.; Sen, S.; Palmieri, T.; Greenhalgh, D. Harnessing the Transparent Face Orthosis for facial scar management: A comparison of methods. Burns 2013, 39, 950–956. [Google Scholar] [CrossRef]
- Hwang, S.J.; Seo, J.; Cha, J.Y.; Shin, H.; Kim, G.S.; Cho, Y.M.; Hua, Z.; Youn, H.S.; Seo, C.H.; Joo, S.Y.; et al. Utility of customized 3D compression mask with pressure sensors on facial burn scars: A single-blinded, randomized controlled trial. Burns 2024, 50, 1885–1897. [Google Scholar] [CrossRef]
- Yu, A.; Yick, K.L.; Ng, S.P.; Yip, J.; Chan, Y.F. Numerical simulation of pressure therapy glove by using Finite Element Method. Burns 2016, 42, 141–151. [Google Scholar] [CrossRef]
- Wei, Y.; Li-Tsang, C.W.P.; Wu, J.; Zhang, W.; Zhang, Y.; Deng, H.; Zhang, M.; Wang, Y. A finite element model of the 3D-printed transparent facemask for applying pressure therapy. Clin. Biomech. 2021, 87, 105414. [Google Scholar] [CrossRef] [PubMed]
- Alkhalil, A.; Tejiram, S.; Travis, T.E.; Prindeze, N.J.; Carney, B.C.; Moffatt, L.T.; Johnson, L.S.; Ramella-Roman, J.; Shupp, J.W. A Translational Animal Model for Scar Compression Therapy Using an Automated Pressure Delivery System. Eplasty 2015, 15, e29. [Google Scholar] [PubMed]
- Tejiram, S.; Zhang, J.; Travis, T.E.; Carney, B.C.; Alkhalil, A.; Moffatt, L.T.; Johnson, L.S.; Shupp, J.W. Compression therapy affects collagen type balance in hypertrophic scar. J. Surg. Res. 2016, 201, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Leung, K.S.; Cheng, J.C.Y.; Ma, G.F.Y.; Clark, J.A.; Leung, P.C. Complications of pressure therapy for post-burn hypertrophic scars: Biomechanical analysis based on 5 patients. Burns 1984, 10, 434–438. [Google Scholar] [CrossRef]
- Hubbard, M.; Masters Ib Fau-Williams, G.R.; Williams Gr Fau-Chang, A.B.; Chang, A.B. Severe obstructive sleep apnoea secondary to pressure garments used in the treatment of hypertrophic burn scars. Eur. Respir. J. 2000, 16, 1205–1207. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject 1 | Subject 2 | |
|---|---|---|
| Gender | Male | Male |
| Age (years) | 62 | 41 |
| Burn type | Flame burn (FB) | Flame burn (FB) |
| Burn lesions without and with mask |  |  |
| Number of sensors | 2 | 2 |
| Test period | 4 weeks | 4 weeks |
| Wearing time | 12 h per day on average | 12 h per day on average |
| Evaluation | (Quantitative evaluation) skin water content, transepidermal water loss, melanin, erythema, and scar thickness. Qualitative evaluation: Vancouver Scar Scale (VSS) (five parameters) and Patient and Observer Scar Assessment Scale (POSAS) (observer scale: six parameters; patient scale: seven parameters). | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the European Burns Association. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, H.; Jeon, G.-J.; Hwang, S.-J.; Cho, H.; Cho, Y.-M.; Youn, H.-S.; Seo, J.; Park, S.; Cho, Y.-S.; Kim, G.-S. Preliminary Study on the Development of a Real-Time Pressure-Monitoring Facial Mask for Burn Rehabilitation. Eur. Burn J. 2025, 6, 12. https://doi.org/10.3390/ebj6010012
Shin H, Jeon G-J, Hwang S-J, Cho H, Cho Y-M, Youn H-S, Seo J, Park S, Cho Y-S, Kim G-S. Preliminary Study on the Development of a Real-Time Pressure-Monitoring Facial Mask for Burn Rehabilitation. European Burn Journal. 2025; 6(1):12. https://doi.org/10.3390/ebj6010012
Chicago/Turabian StyleShin, Hyunjun, Gyung-Jin Jeon, Seok-Jin Hwang, Hyeonseok Cho, Young-Min Cho, Hyoung-Soon Youn, Jisu Seo, Sehoon Park, Yoon-Soo Cho, and Gyu-Seok Kim. 2025. "Preliminary Study on the Development of a Real-Time Pressure-Monitoring Facial Mask for Burn Rehabilitation" European Burn Journal 6, no. 1: 12. https://doi.org/10.3390/ebj6010012
APA StyleShin, H., Jeon, G.-J., Hwang, S.-J., Cho, H., Cho, Y.-M., Youn, H.-S., Seo, J., Park, S., Cho, Y.-S., & Kim, G.-S. (2025). Preliminary Study on the Development of a Real-Time Pressure-Monitoring Facial Mask for Burn Rehabilitation. European Burn Journal, 6(1), 12. https://doi.org/10.3390/ebj6010012