
Investigation of the “Surgical Cuts CO2 Laser Therapy Technique” to Treat Minor Burn Scar Contractures in Children


Abstract
1. Introduction
2. Materials and Methods
- Identify the discrete, linear band causing the minor scar contracture.
- Visually examine and manually palpate the contracture to determine the perceived thickness and adjust laser energy settings accordingly (typical settings for “fusion mode” include core energy = 70 mJ, ring energy = 48–55.2 mJ, and fractional coverage = 20–25%).
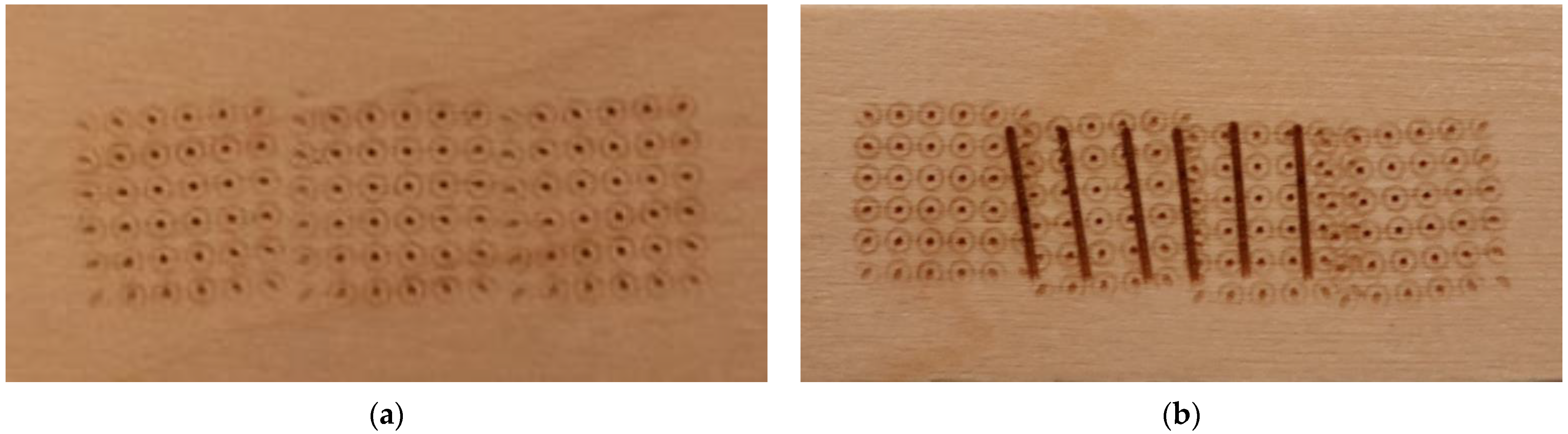
- Use the traditional, fractional CO2 laser setting to create a grid-like pattern of holes along the length of the contracture and apply the same technique to any adjacent scarring surrounding the contracture.
- Adjust the CO2 laser settings to the “surgical mode” to create a series of linear cuts that are perpendicular to the contracture.
- Determine the appropriate width of the laser beam by measuring the visible width of the contracture and extending it by 2 mm to ensure appropriate coverage. When using the surgical cuts technique, initial laser energy settings should not exceed 25 mJ to ensure patient safety. The treating clinician may try a test pulse and then gradually increase the energy settings until the desired effect is achieved.
- Space surgical cuts as close together as is feasible without overlapping.
- Apply topical triamcinolone (40 mg/mL) and topical xylocaine to the laser-treated area. Place digits and hand in a stretched position and place in a plaster splint (not circumferential) for one week. Following removal, commence stretching exercises and/or rehabilitation therapy and/or night splinting and return to daily activities.

3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tredget, E.E.; Nedelec, B.; Scott, P.G.; Ghahary, A. Hypertrophic scars, keloids, and contractures. The cellular and molecular basis for therapy. Surg. Clin. N. Am. 1997, 77, 701–730. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, D.G. Wound Healing. In Burn Care for General Surgeons and General Practitioners; Greenhalgh, D.G., Ed.; Springer International Publishing: Cham, Switzerland, 2016; pp. 95–116. [Google Scholar]
- Li, B.; Wang, J.H. Fibroblasts and myofibroblasts in wound healing: Force generation and measurement. J. Tissue Viability 2011, 20, 108–120. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.; Minn, K.W. The effect of myofibroblast on contracture of hypertrophic scar. Plast. Reconstr. Surg. 2004, 113, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, T.L.; Nelson-Mooney, K.; Kagan, R.J.; Stubbs, T.K.; Meyer, W.J., 3rd; Herndon, D.N.; Hinson, M.I.; Lee, A.F.; Li, N.C.; Kazis, L.E.; et al. Impact of hand burns on health-related quality of life in children younger than 5 years. J. Trauma. Acute Care Surg. 2012, 73 (Suppl. 2), S197–S204. [Google Scholar] [CrossRef] [PubMed]
- Hendriks, T.C.C.; Botman, M.; Binnerts, J.J.; Mtui, G.S.; Nuwass, E.Q.; Niemeijer, A.S.; Mullender, M.G.; Winters, H.A.H.; Nieuwenhuis, M.K.; van Zuijlen, P.P.M. The development of burn scar contractures and impact on joint function, disability and quality of life in low- and middle-income countries: A prospective cohort study with one-year follow-up. Burns 2021, 48, 215–227. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.R.; Donelan, M.B.; Hivnor, C.; Greeson, E.; Ross, E.V.; Shumaker, P.R.; Uebelhoer, N.S.; Waibel, J.S. Laser treatment of traumatic scars with an emphasis on ablative fractional laser resurfacing consensus report. JAMA Dermatol. 2014, 150, 187–193. [Google Scholar] [CrossRef]
- Khandelwal, A.; Yelvington, M.; Tang, X.; Brown, S. Ablative fractional photothermolysis for the treatment of hypertrophic burn scars in adult and pediatric patients: A single surgeon’s experience. J. Burn. Care Res. 2014, 35, 455–463. [Google Scholar] [CrossRef]
- Ozog, D.M.; Liu, A.; Chaffins, M.L.; Ormsby, A.H.; Fincher, E.F.; Chipps, L.K.; Mi, Q.S.; Grossman, P.H.; Pui, J.C.; Moy, R.L. Evaluation of clinical results, histological architecture, and collagen expression following treatment of mature burn scars with a fractional carbon dioxide laser. JAMA Dermatol. 2013, 149, 50–57. [Google Scholar] [CrossRef]
- Manstein, D.; Herron, G.S.; Sink, R.K.; Tanner, H.; Anderson, R.R. Fractional photothermolysis: A new concept for cutaneous remodeling using microscopic patterns of thermal injury. Lasers Surg. Med. 2004, 34, 426–438. [Google Scholar] [CrossRef]
- Krakowski, A.C.; Goldenberg, A.; Eichenfield, L.F.; Murray, J.P.; Shumaker, P.R. Ablative fractional laser resurfacing helps treat restrictive pediatric scar contractures. Pediatrics 2014, 134, e1700–e1705. [Google Scholar] [CrossRef]
- Shumaker, P.R.; Kwan, J.M.; Landers, J.T.; Uebelhoer, N.S. Functional improvements in traumatic scars and scar contractures using an ablative fractional laser protocol. J. Trauma. Acute Care Surg. 2012, 73 (Suppl. 1), S116–S121. [Google Scholar] [CrossRef]
- Xi, W.; Xie, Y.; Zhang, Z.; Li, K.; Wang, J.; Li, J.; Feng, S.; Hultman, C.S.; Liu, Y.; Zhang, Y. 3D Mesh Releasing Method: A Retrospective Analysis of Fractional CO2 Treatment on Contracture Scars. Lasers Surg. Med. 2021, 53, 227–235. [Google Scholar] [CrossRef]
- Zuccaro, J.; Kelly, C.; Perez, M.M.; Doria, A.; Fish, J.S. The Effectiveness of Laser Therapy for Hypertrophic Burn Scars in Pediatric Patients: A Prospective Investigation. J. Burn. Care Res. 2021, 42, 847–856. [Google Scholar] [CrossRef]
- Blome-Eberwein, S.; Gogal, C.; Weiss, M.J.; Boorse, D.; Pagella, P. Prospective Evaluation of Fractional CO2 Laser Treatment of Mature Burn Scars. J. Burn. Care Res. 2016, 37, 379–387. [Google Scholar] [CrossRef]
- Issler-Fisher, A.C.; Fisher, O.M.; Smialkowski, A.O.; Li, F.; van Schalkwyk, C.P.; Haertsch, P.; Maitz, P.K.M. Ablative fractional CO2 laser for burn scar reconstruction: An extensive subjective and objective short-term outcome analysis of a prospective treatment cohort. Burns 2017, 43, 573–582. [Google Scholar] [CrossRef]
- Miletta, N.; Siwy, K.; Hivnor, C.; Clark, J.; Shofner, J.; Zurakowski, D.; Anderson, R.R.; Lee, K.; Donelan, M. Fractional Ablative Laser Therapy is an Effective Treatment for Hypertrophic Burn Scars: A Prospective Study of Objective and Subjective Outcomes. Ann. Surg. 2021, 274, e574–e580. [Google Scholar] [CrossRef]
- Seago, M.; Shumaker, P.R.; Spring, L.K.; Alam, M.; Al-Niaimi, F.; Rox Anderson, R.; Artzi, O.; Bayat, A.; Cassuto, D.; Chan, H.H.; et al. Laser Treatment of Traumatic Scars and Contractures: 2020 International Consensus Recommendations. Lasers Surg. Med. 2020, 52, 96–116. [Google Scholar] [CrossRef]
- Azzam, O.A.; Bassiouny, D.A.; El-Hawary, M.S.; El Maadawi, Z.M.; Sobhi, R.M.; El-Mesidy, M.S. Treatment of hypertrophic scars and keloids by fractional carbon dioxide laser: A clinical, histological, and immunohistochemical study. Lasers Med. Sci. 2016, 31, 9–18. [Google Scholar] [CrossRef]
- El-Zawahry, B.M.; Sobhi, R.M.; Bassiouny, D.A.; Tabak, S.A. Ablative CO2 fractional resurfacing in treatment of thermal burn scars: An open-label controlled clinical and histopathological study. J. Cosmet. Dermatol. 2015, 14, 324–331. [Google Scholar] [CrossRef]
- Qu, L.; Liu, A.; Zhou, L.; He, C.D.; Grossman, P.H.; Moy, R.L.; Mi, Q.S.; Ozog, D. Clinical and molecular effects on mature burn scars after treatment with a fractional CO2 laser. Lasers Surg. Med. 2012, 44, 517–524. [Google Scholar] [CrossRef]
- Issler-Fisher, A.C.; Waibel, J.S.; Donelan, M.B. Laser Modulation of Hypertrophic Scars: Technique and Practice. Clin. Plast. Surg. 2017, 44, 757–766. [Google Scholar] [CrossRef] [PubMed]
- Mowbrey, K.; Ferland-Caron, G.; Tredget, E.E. Important Developments in the Management of Fibroproliferative Scars and Contractures after Burn Injury. In Burn Care for General Surgeons and General Practitioners; Greenhalgh, D.G., Ed.; Springer International Publishing: Cham, Switzerland, 2016; pp. 239–259. [Google Scholar]
- Hultman, C.S.; Friedstat, J.S.; Edkins, R.E.; Cairns, B.A.; Meyer, A.A. Laser Resurfacing and Remodeling of Hypertrophic Burn Scars the Results of a Large, Prospective, before-after Cohort Study, with Long-term Follow-up. Ann. Surg. 2014, 260, 519–532. [Google Scholar] [CrossRef] [PubMed]
- Donelan, M.B.; Parrett, B.M.; Sheridan, R.L. Pulsed dye laser therapy and z-plasty for facial burn scars—The alternative to excision. Ann. Plast. Surg. 2008, 60, 480–486. [Google Scholar] [CrossRef] [PubMed]
- Issler-Fisher, A.C.; Fisher, O.M.; Clayton, N.A.; Aggarwala, S.; Haertsch, P.A.; Li, Z.; Maitz, P.K.M. Ablative fractional resurfacing for burn scar management affects the number and type of elective surgical reconstructive procedures, hospital admission patterns as well as length of stay. Burns 2020, 46, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Nedelec, B.; Correa, J.A.; Rachelska, G.; Armour, A.; LaSalle, L. Quantitative measurement of hypertrophic scar: Interrater reliability and concurrent validity. J. Burn. Care Res. 2008, 29, 501–511. [Google Scholar] [CrossRef]
- Nedelec, B.; Correa, J.A.; Rachelska, G.; Armour, A.; LaSalle, L. Quantitative measurement of hypertrophic scar: Intrarater reliability, sensitivity, and specificity. J. Burn. Care Res. 2008, 29, 489–500. [Google Scholar] [CrossRef]
- Waibel, J.S.; Rudnick, A.C.; Wulkan, A.J.; Holmes, J.D. The Diagnostic Role of Optical Coherence Tomography (OCT) in Measuring the Depth of Burn and Traumatic Scars for More Accurate Laser Dosimetry: Pilot Study. J. Drugs Dermatol. 2016, 15, 1375–1380. [Google Scholar]


{kind=link}
{kind=link}
| Gender | n (%) |
|---|---|
| Male | 5 (41.7) |
| Female | 7 (58.3) |
| Participant Age at Laser Treatment | n (SD) |
| Mean (SD) | 5.5 years (3.9) |
| Range | 1–15 years |
| Fitzpatrick Skin Type | n (%) |
| I | 4 (33.3) |
| II | 5 (41.7) |
| III | 1 (8.3) |
| IV | 2 (16.7) |
| Burn Etiology | (n, %) |
| Contact | 12 (100) |
| Burn Depth | (n, %) |
| Partial thickness | 2 (16.7) |
| Full thickness | 5 (41.7) |
| Undocumented due to acute treatment at different institution | 5 (41.7) |
| Acute Burn Treatment | (n, %) |
| Conservative therapy | 3 (25.0) |
| Skin grafting | 4 (33.3) |
| Undocumented due to acute treatment at different institution | 5 (41.7) |
| Age of Scar at Laser Treatment | (n, SD) |
| Mean (SD) | 39.7 months (52.0) |
| Range | 2–174 months |
| ID | Location of Affected Joint(s) | Pre-Laser Range of Motion | Post-Laser Range of Motion | Pre-Laser Digit Length | Post-Laser Digit Length | Pre-Laser Hand- Span | Post-Laser Hand- Span |
|---|---|---|---|---|---|---|---|
| 1 | Right D † 5 PIP § Right D5 DIP ‡ | Passive −55° extension Passive −50° extension | Passive 0° (full extension) Passive −10° extension | ||||
| 2 | Right D5 PIP | Passive −15° extension | Passive −10° extension | 12 cm | 13 cm | ||
| 3 | Left D2 PIP | Active −30° extension | Active 0° (full extension) | 7.9 cm | 8.6 cm | ||
| 4 | Left D3 Left D4 | 5.2 cm 5.0 cm | 5.3 cm 5.7 cm | 15.5 cm | 15.5 cm | ||
| 5 | Right D3 Right D4 | 3.5 cm 4.0 cm | 4.5 cm 4.0 cm | ||||
| 6 | Right D2 DIP | Active −25° extension | Active −15° extension | ||||
| 7 | Right D4 DIP | Active −15° extension | Active 0° (full extension) | 6.5 cm | 6.9 cm | ||
| 8 | Left D1 IP * | Active −60° Extension | Active 0° (full extension) | ||||
| 9 | Right D2 DIP | Active −30° extension | Active 0° (full extension) | 5.5 cm | 6.0 cm | ||
| 10 | Right D4 DIP | Passive −15° extension | Passive 0° (full extension) | ||||
| 11 | Left D5 PIP | Passive −5° extension | Passive 0° (full extension) | 8.5 cm | 8.5 cm | ||
| 12 | Left D5 DIP | Passive −15° extension | Passive 0° (full extension) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zuccaro, J.; Lazzarotto, L.; Lati, J.; Kelly, C.; Fish, J. Investigation of the “Surgical Cuts CO2 Laser Therapy Technique” to Treat Minor Burn Scar Contractures in Children. Eur. Burn J. 2023, 4, 293-302. https://doi.org/10.3390/ebj4030027
Zuccaro J, Lazzarotto L, Lati J, Kelly C, Fish J. Investigation of the “Surgical Cuts CO2 Laser Therapy Technique” to Treat Minor Burn Scar Contractures in Children. European Burn Journal. 2023; 4(3):293-302. https://doi.org/10.3390/ebj4030027
Chicago/Turabian StyleZuccaro, Jennifer, Lisa Lazzarotto, Jamil Lati, Charis Kelly, and Joel Fish. 2023. "Investigation of the “Surgical Cuts CO2 Laser Therapy Technique” to Treat Minor Burn Scar Contractures in Children" European Burn Journal 4, no. 3: 293-302. https://doi.org/10.3390/ebj4030027
APA StyleZuccaro, J., Lazzarotto, L., Lati, J., Kelly, C., & Fish, J. (2023). Investigation of the “Surgical Cuts CO2 Laser Therapy Technique” to Treat Minor Burn Scar Contractures in Children. European Burn Journal, 4(3), 293-302. https://doi.org/10.3390/ebj4030027