
Laser, Intense Pulsed Light, and Radiofrequency for the Treatment of Burn Scarring: A Systematic Review and Meta-Analysis



Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Inclusion
2.3. Data Extraction
2.4. Methodological Quality Assessment of Included Studies
2.5. Statistical Analysis
3. Results
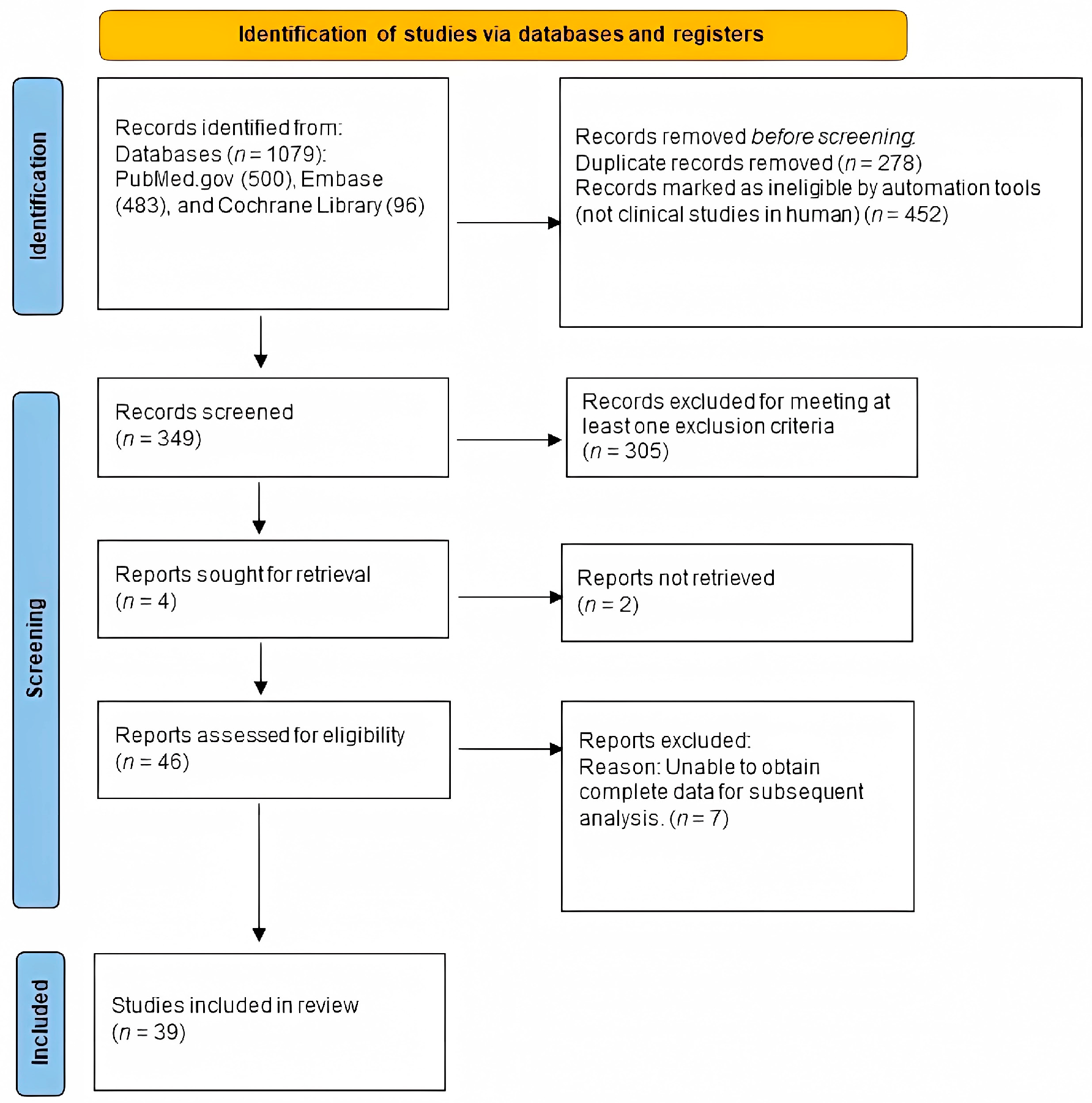
3.1. Identification of Eligible Studies
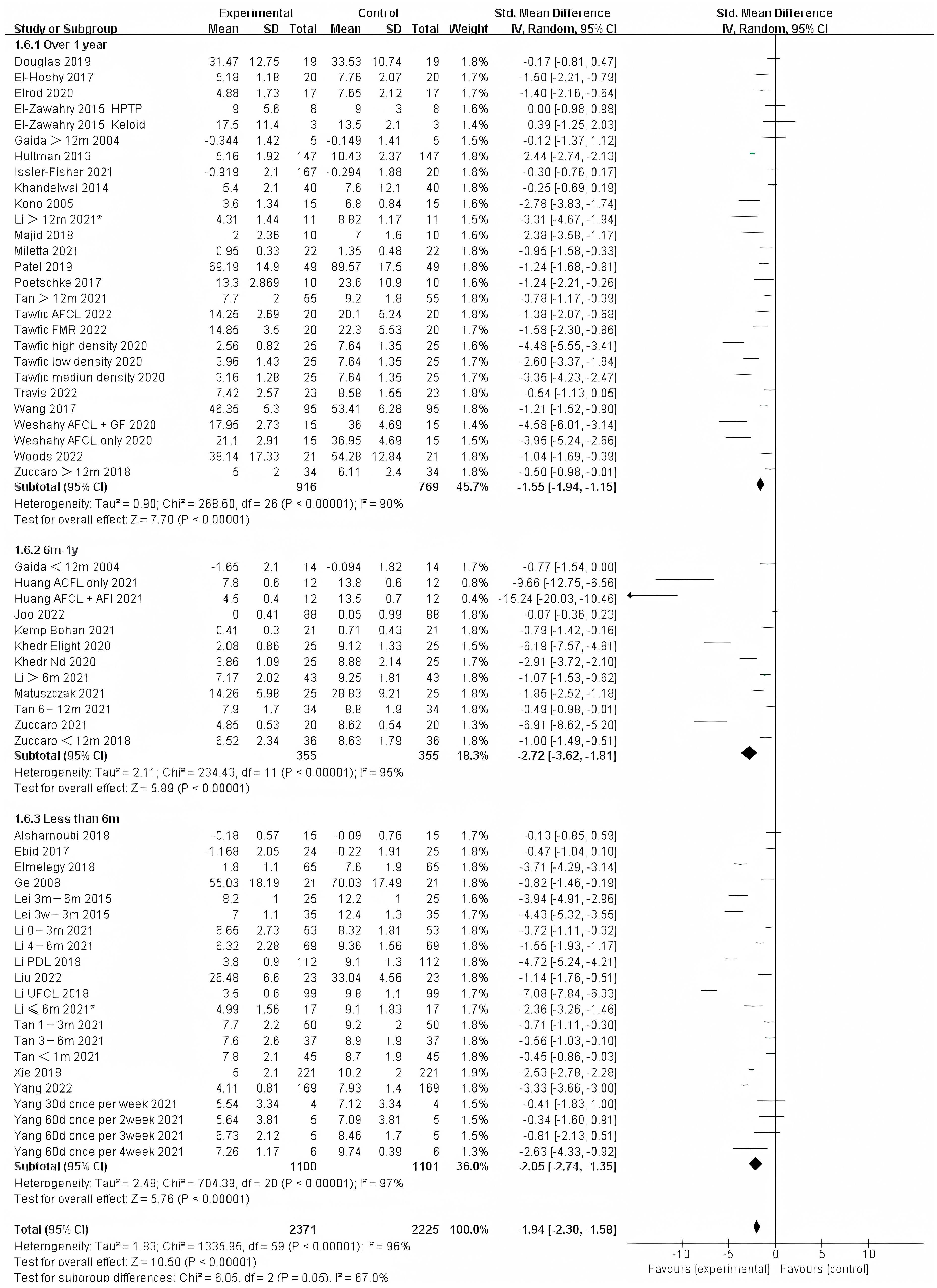
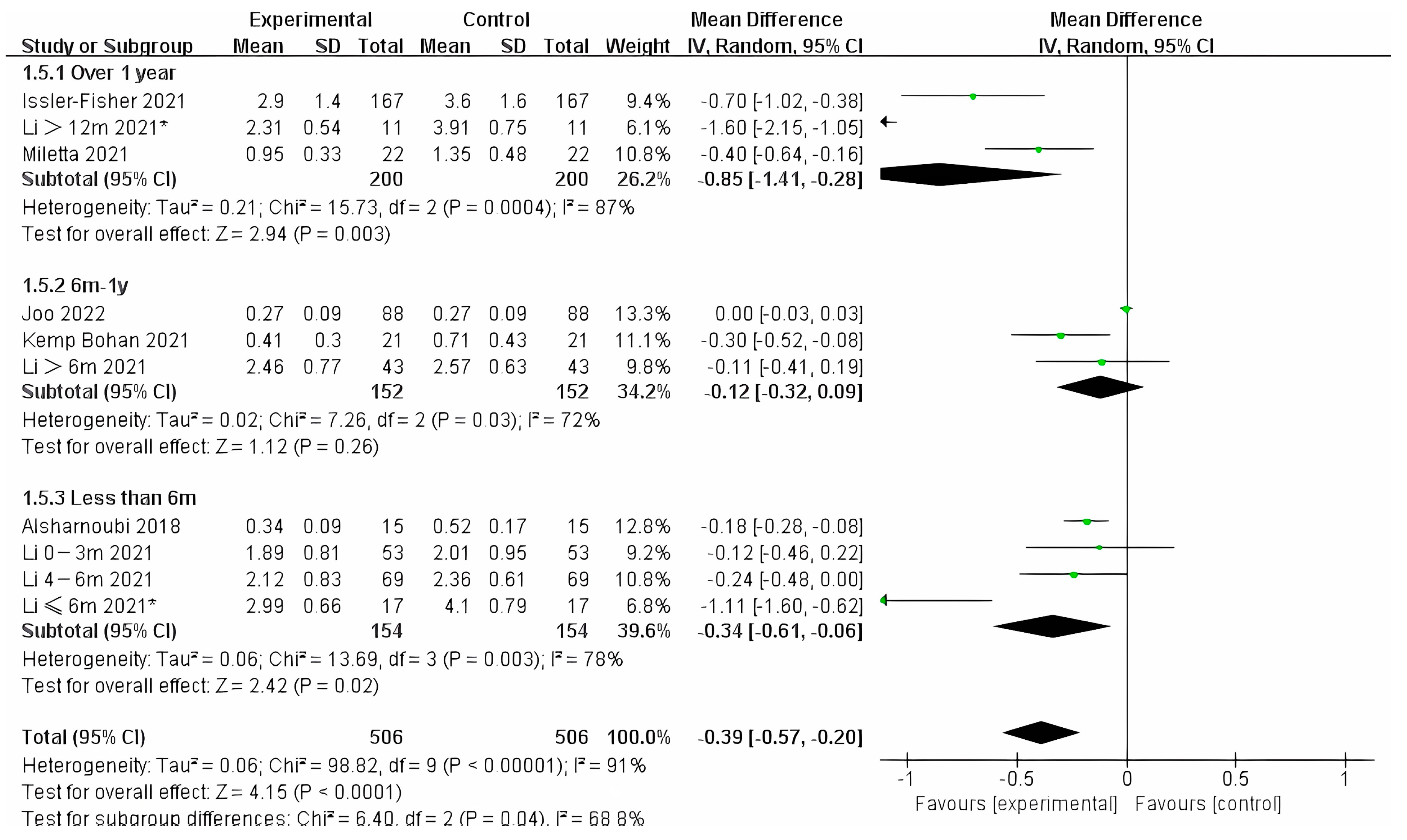
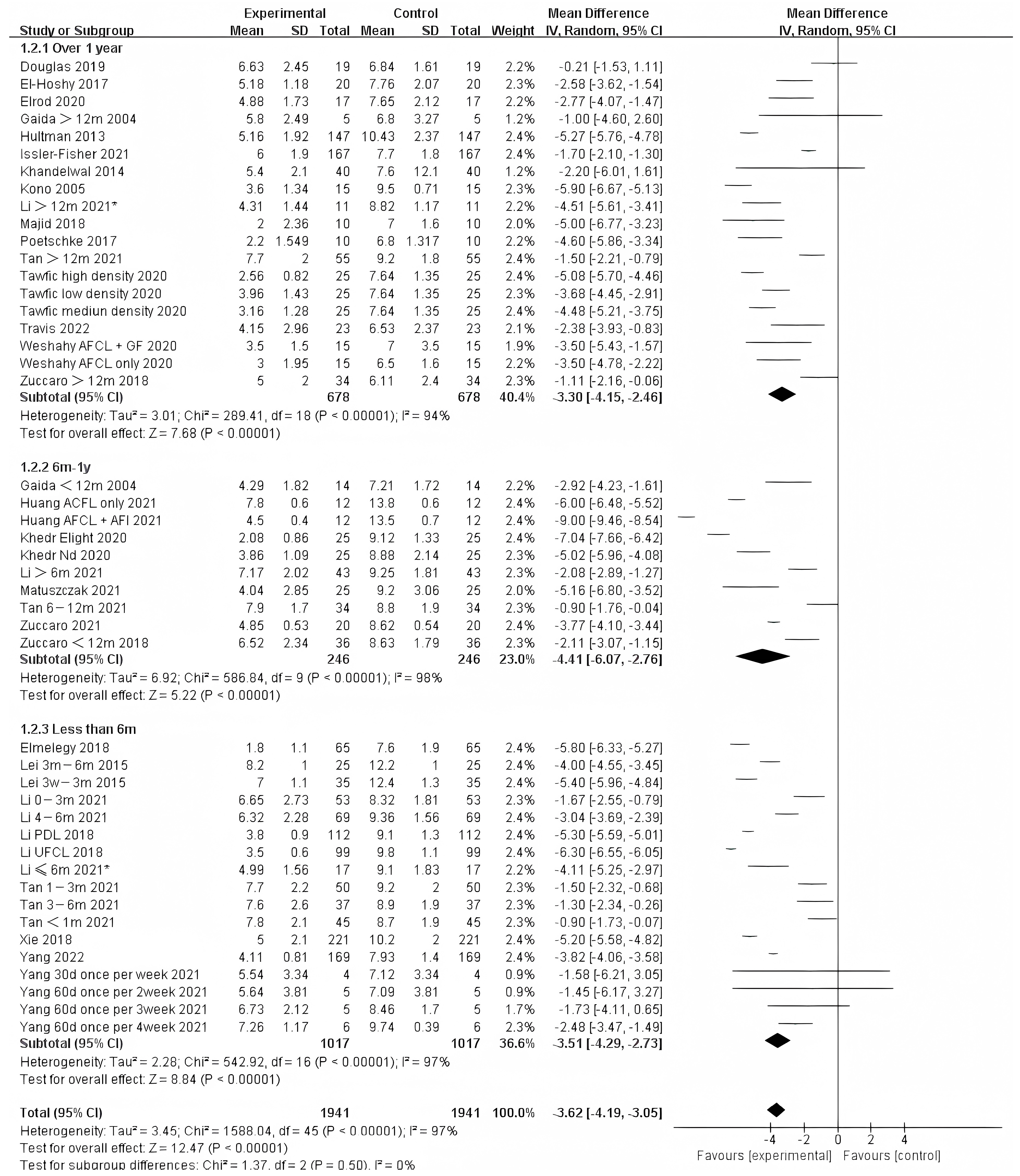
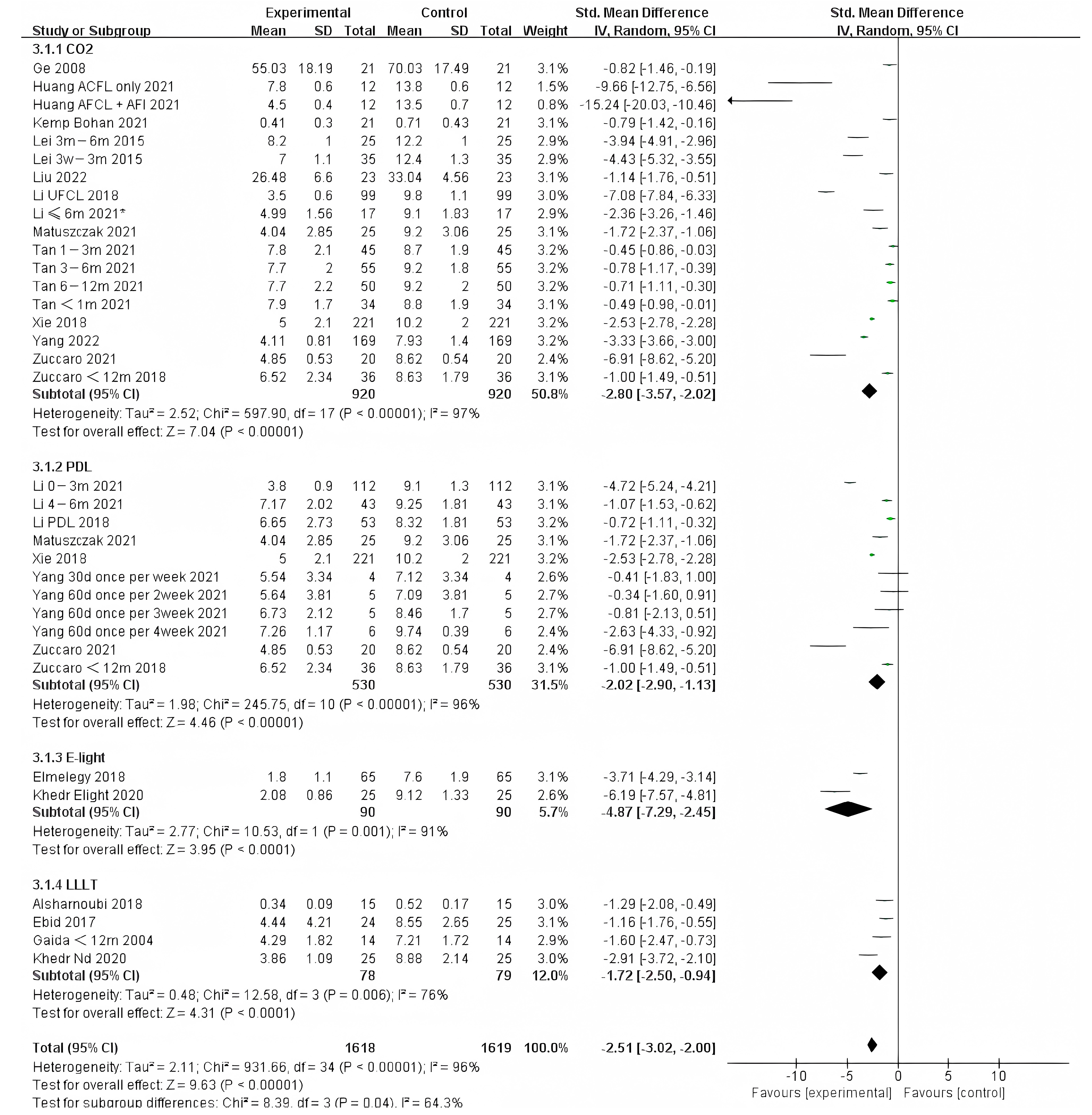
3.2. Time of Intervention
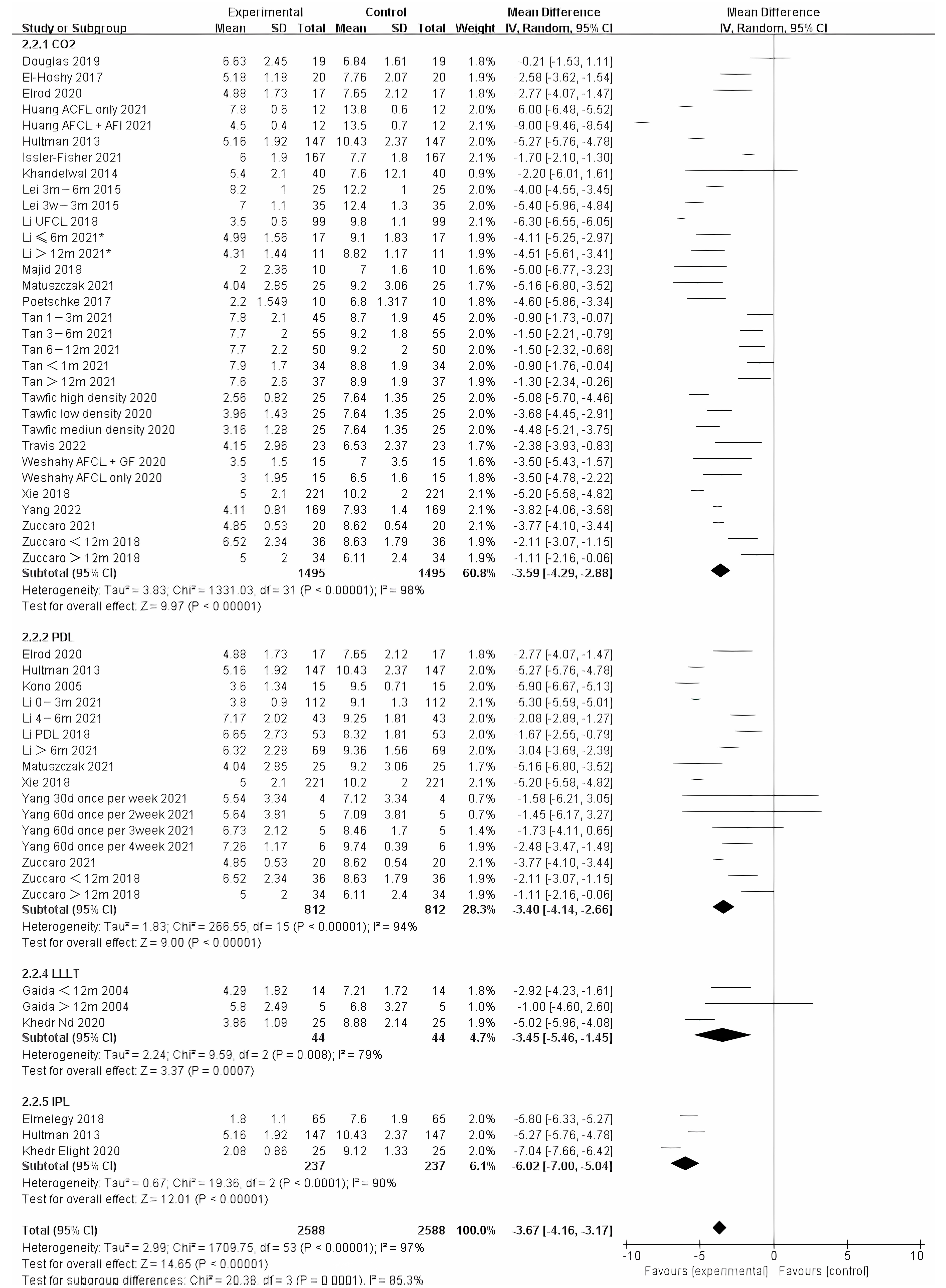
3.3. Method for Burn Scarring
3.4. Publication Bias
4. Discussion
5. Conclusions
6. Limitations
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Peck, M.D.; Kruger, G.E.; Van Der Merwe, A.E.; Godakumbura, W.; Ahuja, R.B. Burns and fires from non-electric domestic appliances in low and middle income countries Part I. The scope of the problem. Burns 2008, 34, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Forjuoh, S.N. Burns in low- and middle-income countries: A review of available literature on descriptive epidemiology, risk factors, treatment, and prevention. Burns 2006, 32, 529–537. [Google Scholar] [CrossRef] [PubMed]
- Arno, A.I.; Gauglitz, G.G.; Barret, J.P.; Jeschke, M.G. Up-to-date approach to manage keloids and hypertrophic scars: A useful guide. Burns 2014, 40, 1255–1266. [Google Scholar] [CrossRef] [PubMed]
- Bloemen, M.C.; van der Veer, W.M.; Ulrich, M.M.; van Zuijlen, P.P.; Niessen, F.B.; Middelkoop, E. Prevention and curative management of hypertrophic scar formation. Burns 2009, 35, 463–475. [Google Scholar] [CrossRef]
- Oosterwijk, A.M.; Mouton, L.J.; Schouten, H.; Disseldorp, L.M.; van der Schans, C.P.; Nieuwenhuis, M.K. Prevalence of scar contractures after burn: A systematic review. Burns 2017, 43, 41–49. [Google Scholar] [CrossRef]
- Zuber, T.J.; DeWitt, D.E. Earlobe keloids. Am. Fam. Physician 1994, 49, 1835–1841. [Google Scholar]
- Hatamipour, E.; Mehrabi, S.; Hatamipour, M.; Ghafarian Shirazi, H.R. Effects of combined intralesional 5-Fluorouracil and topical silicone in prevention of keloids: A double blind randomized clinical trial study. Acta Med. Iran. 2011, 49, 127–130. [Google Scholar]
- Hassel, J.C.; Loser, C.; Koenen, W.; Kreuter, A.; Hassel, A.J. Promising results from a pilot study on compression treatment of ear keloids. J. Cutan. Med. Surg. 2011, 15, 130–136. [Google Scholar] [CrossRef]
- Nast, A.; Eming, S.; Fluhr, J.; Fritz, K.; Gauglitz, G.; Hohenleutner, S.; Panizzon, R.G.; Sebastian, G.; Sporbeck, B.; Koller, J.; et al. German S2k guidelines for the therapy of pathological scars (hypertrophic scars and keloids). J. Dtsch. Dermatol. Ges. 2012, 10, 747–762. [Google Scholar] [CrossRef]
- Robles, D.T.; Berg, D. Abnormal wound healing: Keloids. Clin. Dermatol. 2007, 25, 26–32. [Google Scholar] [CrossRef]
- Poochareon, V.N.; Berman, B. New therapies for the management of keloids. J. Craniofac. Surg. 2003, 14, 654–657. [Google Scholar] [CrossRef]
- Gold, M.H.; Berman, B.; Clementoni, M.T.; Gauglitz, G.G.; Nahai, F.; Murcia, C. Updated international clinical recommendations on scar management: Part 1—Evaluating the evidence. Dermatol. Surg. 2014, 40, 817–824. [Google Scholar]
- Gold, M.H.; McGuire, M.; Mustoe, T.A.; Pusic, A.; Sachdev, M.; Waibel, J.; Murcia, C.; International Advisory Panel on Scar, M. Updated international clinical recommendations on scar management: Part 2—Algorithms for scar prevention and treatment. Dermatol. Surg. 2014, 40, 825–831. [Google Scholar] [CrossRef]
- Ahuja, R.B.; Chatterjee, P. Comparative efficacy of intralesional verapamil hydrochloride and triamcinolone acetonide in hypertrophic scars and keloids. Burns 2014, 40, 583–588. [Google Scholar] [CrossRef]
- Grisolia, G.A.; Danti, D.A.; Santoro, S.; Panozzo, G.; Bonini, G.; Pampaloni, A. Injection therapy with triamcinolone hexacetonide in the treatment of burn scars in infancy: Results of 44 cases. Burns 1983, 10, 131–134. [Google Scholar] [CrossRef]
- Wang, X.Q.; Liu, Y.K.; Qing, C.; Lu, S.L. A review of the effectiveness of antimitotic drug injections for hypertrophic scars and keloids. Ann. Plast. Surg. 2009, 63, 688–692. [Google Scholar]
- Trisliana Perdanasari, A.; Torresetti, M.; Grassetti, L.; Nicoli, F.; Zhang, Y.X.; Dashti, T.; Di Benedetto, G.; Lazzeri, D. Intralesional injection treatment of hypertrophic scars and keloids: A systematic review regarding outcomes. Burn. Trauma 2015, 3, 14. [Google Scholar] [CrossRef]
- Fredman, R.; Tenenhaus, M. Cushing’s syndrome after intralesional triamcinolone acetonide: A systematic review of the literature and multinational survey. Burns 2013, 39, 549–557. [Google Scholar] [CrossRef]
- Ragoowansi, R.; Cornes, P.G.; Moss, A.L.; Glees, J.P. Treatment of keloids by surgical excision and immediate postoperative single-fraction radiotherapy. Plast. Reconstr. Surg. 2003, 111, 1853–1859. [Google Scholar] [CrossRef]
- Cho, Y.S.; Jeon, J.H.; Hong, A.; Yang, H.T.; Yim, H.; Cho, Y.S.; Kim, D.H.; Hur, J.; Kim, J.H.; Chun, W.; et al. The effect of burn rehabilitation massage therapy on hypertrophic scar after burn: A randomized controlled trial. Burns 2014, 40, 1513–1520. [Google Scholar] [CrossRef]
- Willows, B.M.; Ilyas, M.; Sharma, A. Laser in the management of burn scars. Burns 2017, 43, 1379–1389. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.J.; Williams, E.A.; Pham, C.H.; Collier, Z.J.; Dang, J.; Yenikomshian, H.A.; Gillenwater, T.J. Fractional CO2 laser treatment for burn scar improvement: A systematic review and meta-analysis. Burns 2021, 47, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Mahar, P.D.; Spinks, A.B.; Cleland, H.; Bekhor, P.; Waibel, J.S.; Lo, C.; Goodman, G. Improvement of Burn Scars Treated with Fractional Ablative CO2 Lasers-A Systematic Review and Meta-analysis Using the Vancouver Scar Scale. J. Burn Care Res. 2021, 42, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Zuccaro, J.; Ziolkowski, N.; Fish, J. A Systematic Review of the Effectiveness of Laser Therapy for Hypertrophic Burn Scars. Clin. Plast. Surg. 2017, 44, 767–779. [Google Scholar] [CrossRef] [PubMed]
- Kent, R.A.; Shupp, J.; Fernandez, S.; Prindeze, N.; DeKlotz, C.M.C. Effectiveness of Early Laser Treatment in Surgical Scar Minimization: A Systematic Review and Meta-analysis. Dermatol. Surg. 2020, 46, 402–410. [Google Scholar] [CrossRef]
- Behrouz-Pirnia, A.; Liu, H.; Peternel, S.; Dervishi, G.; Labeit, A.; Peinemann, F. Early laser intervention to reduce scar formation in wound healing by primary intention: A systematic review. J. Plast. Reconstr. Aesthet. Surg. 2020, 73, 528–536. [Google Scholar] [CrossRef]
- Brewin, M.P.; Lister, T.S. Prevention or treatment of hypertrophic burn scarring: A review of when and how to treat with the pulsed dye laser. Burns 2014, 40, 797–804. [Google Scholar] [CrossRef]
- Poetschke, J.; Gauglitz, G.G. Treatment of Immature Scars: Evidence-Based Techniques and Treatments. In Textbook on Scar Management: State of the Art Management and Emerging Technologies; Springer: Cham, Switzerland, 2020. [Google Scholar]
- Santer, M.; Kloppenburg, M.; Gottfried, T.A.-O.; Runge, A.; Schmutzhard, J.; Vorbach, S.M.; Mangesius, J.A.-O.; Riedl, D.A.-O.; Mangesius, S.A.-O.; Widmann, G.; et al. Current Applications of Artificial Intelligence to Classify Cervical Lymph Nodes in Patients with Head and Neck Squamous Cell Carcinoma—A Systematic Review. Cancers 2022, 14, 5397. [Google Scholar] [CrossRef]
- Chinese Association of Plastics; Aesthetics Scar Medicine Branch. National expert consensus on early management of scars (2020 version). Zhonghua Shao Shang Za Zhi 2021, 37, 113–125. [Google Scholar]
- Elrod, J.; Schiestl, C.; Neuhaus, D.; Mohr, C.; Neuhaus, K. Patient- and Physician-Reported Outcome of Combined Fractional CO2 and Pulse Dye Laser Treatment for Hypertrophic Scars in Children. Ann. Plast. Surg. 2020, 85, 237–244. [Google Scholar] [CrossRef]
- Ge, X.; Sun, Y.; Lin, J.; Zhou, F.; Yao, G.; Su, X. Effects of multiple modes of UltraPulse fractional CO2 laser treatment on extensive scarring: A retrospective study. Lasers Med. Sci. 2022, 37, 1575–1582. [Google Scholar] [CrossRef]
- Hultman, C.S.; Edkins, R.E.; Wu, C.; Calvert, C.T.; Cairns, B.A. Prospective, before-after cohort study to assess the efficacy of laser therapy on hypertrophic burn scars. Ann. Plast. Surg. 2013, 70, 521–526. [Google Scholar] [CrossRef]
- Khandelwal, A.; Yelvington, M.; Tang, X.; Brown, S. Ablative fractional photothermolysis for the treatment of hypertrophic burn scars in adult and pediatric patients: A single surgeon’s experience. J. Burn Care Res. 2014, 35, 455–463. [Google Scholar] [CrossRef]
- Li, N.; Yang, L.; Cheng, J.; Han, J.; Yang, X.; Zheng, Z.; Guan, H.; Hu, D. A retrospective study to identify the optimal parameters for pulsed dye laser in the treatment of hypertrophic burn scars in Chinese children with Fitzpatrick skin types III and IV. Lasers Med. Sci. 2021, 36, 1671–1679. [Google Scholar] [CrossRef]
- Li, N.; Yang, L.; Cheng, J.; Han, J.T.; Hu, D.H. Clinical comparative study of pulsed dye laser and ultra-pulsed fractional carbon dioxide laser in the treatment of hypertrophic scars after burns. Zhonghua Shao Shang Za Zhi 2018, 34, 603–607. [Google Scholar] [CrossRef]
- Patel, S.P.; Nguyen, H.V.; Mannschreck, D.; Redett, R.J.; Puttgen, K.B.; Stewart, F.D. Fractional CO2 Laser Treatment Outcomes for Pediatric Hypertrophic Burn Scars. J. Burn Care Res. 2019, 40, 386–391. [Google Scholar] [CrossRef]
- Tan, J.; Zhou, J.; Huang, L.; Fu, Q.; Ao, M.; Yuan, L.; Luo, G. Hypertrophic Scar Improvement by Early Intervention with Ablative Fractional Carbon Dioxide Laser Treatment. Lasers Surg. Med. 2021, 53, 450–457. [Google Scholar] [CrossRef]
- Travis, T.E.; Allely, R.A.; Johnson, L.S.; Shupp, J.W. A Single-Institution Experience with Standardized Objective and Subjective Scar Evaluation While Undergoing Fractional Ablative Carbon Dioxide Laser Treatment. J. Burn Care Res. 2022, 43, 61–69. [Google Scholar] [CrossRef]
- Woods, J.F.C.; Kirkham, J.; Shelley, O.P. Treatment of Postburn Scar Erythema and Dyschromia with Pulsed Dye and Q-Switched KTP Laser. Dermatol. Surg. 2022, 48, 700–702. [Google Scholar] [CrossRef]
- Xie, W.G.; Lei, F.; Wang, J.; Xu, J.; Ruan, J.J.; Li, Z. Clinical effects of sequential laser treatments on early stage hypertrophic burn scars. Zhonghua Shao Shang Za Zhi 2018, 34, 615–623. [Google Scholar] [CrossRef]
- Zuccaro, J.; Kelly, C.; Perez, M.; Doria, A.; Fish, J.S. The Effectiveness of Laser Therapy for Hypertrophic Burn Scars in Pediatric Patients: A Prospective Investigation. J. Burn Care Res. 2021, 42, 847–856. [Google Scholar] [CrossRef]
- Li, N.; Yang, L.; Cheng, J.; Han, J.; Hu, D. Early intervention by Z-plasty combined with fractional CO2 laser therapy as a potential treatment for hypertrophic burn scars. J. Plast. Reconstr. Aesthet. Surg. 2021, 74, 3087–3093. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Shu, F.; Xu, H.; Ji, C.; Wang, Y.; Lou, X.; Luo, P.; Xiao, S.; Xia, Z.; Lv, K. Ablative fractional carbon dioxide laser improves quality of life in patients with extensive burn scars: A nested case-control study. Lasers Surg. Med. 2022, 54, 1207–1216. [Google Scholar] [CrossRef] [PubMed]
- Issler-Fisher, A.C.; Fisher, O.M.; Haertsch, P.A.; Li, Z.; Maitz, P.K.M. Effectiveness and safety of ablative fractional CO2 laser for the treatment of burn scars: A case-control study. Burns 2021, 47, 785–795. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Li, N.; Cheng, J.; Han, J.T.; Hu, D.H. A prospective randomized controlled clinical study on the optimal treatment interval of pulsed dye laser in treating hypertrophic scar after burn. Zhonghua Shao Shang Za Zhi 2021, 37, 57–63. [Google Scholar] [CrossRef]
- Tawfic, S.O.; Hassan, A.S.; El-Zahraa Sh Aly, F.; Elbendary, A.; Shaker, O.G.; AlOrbani, A.M. Fractional microneedle radiofrequency versus fractional carbon dioxide laser in the treatment of postburn hypertrophic scars. Lasers Surg. Med. 2022, 54, 1089–1098. [Google Scholar] [CrossRef]
- Alsharnoubi, J.; Shoukry, K.E.; Fawzy, M.W.; Mohamed, O. Evaluation of scars in children after treatment with low-level laser. Lasers Med. Sci. 2018, 33, 1991–1995. [Google Scholar] [CrossRef]
- Ebid, A.A.; Ibrahim, A.R.; Omar, M.T.; El Baky, A.M.A. Long-term effects of pulsed high-intensity laser therapy in the treatment of post-burn pruritus: A double-blind, placebo-controlled, randomized study. Lasers Med. Sci. 2017, 32, 693–701. [Google Scholar] [CrossRef]
- Douglas, H.; Lynch, J.; Harms, K.A.; Krop, T.; Kunath, L.; van Vreeswijk, C.; McGarry, S.; Fear, M.W.; Wood, F.M.; Murray, A.; et al. Carbon dioxide laser treatment in burn-related scarring: A prospective randomised controlled trial. J. Plast. Reconstr. Aesthet. Surg. 2019, 72, 863–870. [Google Scholar] [CrossRef]
- El-Zawahry, B.M.; Sobhi, R.M.; Bassiouny, D.A.; Tabak, S.A. Ablative CO2 fractional resurfacing in treatment of thermal burn scars: An open-label controlled clinical and histopathological study. J. Cosmet. Dermatol. 2015, 14, 324–331. [Google Scholar] [CrossRef]
- Gaida, K.; Koller, R.; Isler, C.; Aytekin, O.; Al-Awami, M.; Meissl, G.; Frey, M. Low Level Laser Therapy—A conservative approach to the burn scar? Burns 2004, 30, 362–367. [Google Scholar] [CrossRef]
- Joo, S.Y.; Cho, Y.S.; Lee, S.Y.; Seo, C.H. Regenerative effect of combined laser and human stem cell-conditioned medium therapy on hypertrophic burn scar. Burns 2022. [Google Scholar] [CrossRef]
- Kono, T.; Ercocen, A.R.; Nakazawa, H.; Nozaki, M. Treatment of hypertrophic scars using a long-pulsed dye laser with cryogen-spray cooling. Ann. Plast. Surg. 2005, 54, 487–493. [Google Scholar] [CrossRef]
- El-Hoshy, K.; Abdel-Halim, M.R.E.; Dorgham, D.; El-Din Sayed, S.S.; El-Kalioby, M. Efficacy of Fractional Carbon Dioxide Laser in the Treatment of Mature Burn Scars: A Clinical, Histopathological, and Histochemical Study. J. Clin. Aesthet. Dermatol. 2017, 10, 36–43. [Google Scholar]
- Elmelegy, N.G.; Hegazy, A.M.; Sadaka, M.S.; Abdeldaim, D.E. Electrophotobiomodulation in the treatment of facial post-burn hypertrophic scars in pediatric patients. Ann. Burn. Fire Disasters 2018, 31, 127–132. [Google Scholar]
- Huang, Z.; Chen, Y.; Wang, P.; Zheng, D.W.; Zong, Y.L.; Lyu, G.Z. A prospective randomized controlled clinical study on the treatment of hypertrophic scar after burn by fractional carbon dioxide laser combined with autologous fat injection. Zhonghua Shao Shang Za Zhi 2021, 37, 49–56. [Google Scholar] [CrossRef]
- Kemp Bohan, P.M.; Cooper, L.E.; Lu, K.N.; Raper, D.M.; Batchinsky, M.; Carlsson, A.H.; Cancio, L.C.; Chan, R.K. Fractionated Ablative Carbon Dioxide Laser Therapy Decreases Ultrasound Thickness of Hypertrophic Burn Scar: A Prospective Process Improvement Initiative. Ann. Plast. Surg. 2021, 86, 273–278. [Google Scholar] [CrossRef]
- Khedr, M.M.; Mahmoud, W.H.; Sallam, F.A.; Elmelegy, N. Comparison of Nd: YAG Laser and Combined Intense Pulsed Light and Radiofrequency in the Treatment of Hypertrophic Scars: A Prospective Clinico-Histopathological Study. Ann. Plast. Surg. 2020, 84, 518–524. [Google Scholar] [CrossRef]
- Lei, J.; Hao, Z.; Yu, L.; Duan, P.; Meng, Y. Clinical observation of the effects of lattice ultra pulse carbon dioxide laser combined with traditional Chinese medicine on the treatment of hyperplastic scar. Chin. J. Burn. 2015, 31, 164–167. [Google Scholar] [CrossRef]
- Majid, I.; Imran, S. Fractional Carbon Dioxide Laser Resurfacing in Combination with Potent Topical Corticosteroids for Hypertrophic Burn Scars in the Pediatric Age Group: An Open Label Study. Derm. Surg. 2018, 44, 1102–1108. [Google Scholar] [CrossRef]
- Matuszczak, E.; Weremijewicz, A.; Koper-Lenkiewicz, O.M.; Kaminska, J.; Hermanowicz, A.; Debek, W.; Komarowska, M.; Tylicka, M. Effects of combined Pulsed Dye Laser and Fractional CO2 Laser treatment of burn scars and correlation with plasma levels of collagen type I, MMP-2 and TIMP-1. Burns 2021, 47, 1342–1351. [Google Scholar] [CrossRef] [PubMed]
- Miletta, N.; Siwy, K.; Hivnor, C.; Clark, J.; Shofner, J.; Zurakowski, D.; Anderson, R.R.; Lee, K.; Donelan, M. Fractional Ablative Laser Therapy is an Effective Treatment for Hypertrophic Burn Scars: A Prospective Study of Objective and Subjective Outcomes. Ann. Surg. 2021, 274, e574–e580. [Google Scholar] [CrossRef] [PubMed]
- Poetschke, J.; Dornseifer, U.; Clementoni, M.T.; Reinholz, M.; Schwaiger, H.; Steckmeier, S.; Ruzicka, T.; Gauglitz, G.G. Ultrapulsed fractional ablative carbon dioxide laser treatment of hypertrophic burn scars: Evaluation of an in-patient controlled, standardized treatment approach. Lasers Med. Sci. 2017, 32, 1031–1040. [Google Scholar] [CrossRef] [PubMed]
- Tawfic, S.; Sayed, S.; Nada, A.; Manaa, D.; Shalaby, S. High-Versus Low-Density Fractional Laser in the Treatment of Hypertrophic Postburn Scars: A Randomized Clinical Trial. Dermatol. Surg. 2020, 46, e38–e44. [Google Scholar] [CrossRef]
- Wang, S.; Mi, J.; Li, Q.; Jin, R.; Dong, J. Fractional microplasma radiofrequency technology for non-hypertrophic post-burn scars in Asians: A prospective study of 95 patients. Lasers Surg. Med. 2017, 49, 563–569. [Google Scholar] [CrossRef]
- Weshahy, R.H.; Aly, D.G.; Shalaby, S.; Mohammed, F.N.; Sayed, K.S. Clinical and Histological Assessment of Combined Fractional CO2 Laser and Growth Factors Versus Fractional CO2 Laser Alone in the Treatment of Facial Mature Burn Scars: A Pilot Split-Face Study. Lasers Surg. Med. 2020, 52, 952–958. [Google Scholar] [CrossRef]
- Yang, J.; Shi, S.; Wang, L.; Li, N.; Han, J.T.; Hu, D.H. A prospective randomized controlled study on the effects of compound analgesia in ultra-pulsed fractional carbon dioxide laser treatment of post-burn hypertrophic scars in children. Zhonghua Shao Shang Za Zhi 2022, 38, 683–690. [Google Scholar] [CrossRef]
- Zuccaro, J.; Muser, I.; Singh, M.; Yu, J.; Kelly, C.; Fish, J. Laser Therapy for Pediatric Burn Scars: Focusing on a Combined Treatment Approach. J. Burn Care Res. 2018, 39, 457–462. [Google Scholar] [CrossRef]
- Schäfer, M.; Werner, S. Cancer as an overhealing wound: An old hypothesis revisited. Nat. Rev. Mol. Cell Biol. 2008, 9, 628–638. [Google Scholar] [CrossRef]
- Yang, Y.; Liu, L.; Yang, R.; Ding, X.; Li, Y.; Liu, H.; Yan, H. Blood perfusion in hypertrophic scars and keloids studied by laser speckle contrast imaging. Skin Res. Technol. 2021, 27, 789–796. [Google Scholar] [CrossRef]
- Chen, Y.; Liu, J.; Li, X. Research progress of DPL in early prevention and treatment of hypertrophic scar after burn in children. J. Tissue Eng. Reconstr. Surg. 2021, 17, 497–502. [Google Scholar] [CrossRef]
- Fajardo, L.F.; Kwan, H.H.; Kowalski, J.; Prionas, S.D.; Allison, A.C. Dual role of tumor necrosis factor-alpha in angiogenesis. Am. J. Pathol. 1992, 140, 539–544. [Google Scholar]
- Jaspers, M.E.H.; Stekelenburg, C.M.; Simons, J.M.; Brouwer, K.M.; Vlig, M.; van den Kerckhove, E.; Middelkoop, E.; van Zuijlen, P.P.M. Assessing blood flow, microvasculature, erythema and redness in hypertrophic scars: A cross sectional study showing different features that require precise definitions. Burns 2017, 43, 1044–1050. [Google Scholar] [CrossRef]
- Li, N.; Han, J.; Hu, D.; Cheng, J.; Wang, H.; Wang, Y.; Yang, X.; Liu, J.; Li, T.; Zhao, W. Intense pulsed light is effective in treating postburn hyperpigmentation and telangiectasia in Chinese patients. J. Cosmet. Laser Ther. 2018, 20, 436–441. [Google Scholar] [CrossRef]
- Vrijman, C.; van Drooge, A.M.; Limpens, J.; Bos, J.D.; van der Veen, J.P.; Spuls, P.I.; Wolkerstorfer, A. Laser and intense pulsed light therapy for the treatment of hypertrophic scars: A systematic review. Br. J. Dermatol. 2011, 165, 934–942. [Google Scholar] [CrossRef]
- Cao, Y.; Huo, R.; Feng, Y.; Li, Q.; Wang, F. Effects of intense pulsed light on the biological properties and ultrastructure of skin dermal fibroblasts: Potential roles in photoaging. Photomed. Laser Surg. 2011, 29, 327–332. [Google Scholar] [CrossRef]
- Feng, Y.; Zhao, J.; Gold, M.H. Skin rejuvenation in Asian skin: The analysis of clinical effects and basic mechanisms of intense pulsed light. J. Drugs Dermatol. 2008, 7, 273–279. [Google Scholar]
- Zhang, Y.; Dong, J.; Wang, C.; Yan, M.; Yao, M. Clinical effects of a combination treatment with narrow-spectrum intense pulsed light and fractional carbon dioxide laser on hypertrophic scar pruritus. Chin. J. Burns 2018, 34, 608–614. [Google Scholar] [CrossRef]
- Allison, K.P.; Kiernan, M.N.; Waters, R.A.; Clement, R.M. Pulsed dye laser treatment of burn scars. Alleviation or irritation? Burns 2003, 29, 207–213. [Google Scholar] [CrossRef]
- Makboul, M.; Makboul, R.; Abdelhafez, A.H.; Hassan, S.S.; Youssif, S.M. Evaluation of the effect of fractional CO2 laser on histopathological picture and TGF-beta1 expression in hypertrophic scar. J. Cosmet. Dermatol. 2014, 13, 169–179. [Google Scholar] [CrossRef]
- Baroni, A.; Verolino, P. Plasma Radiofrequency Ablation for Scar Treatment. J. Clin. Med. 2021, 11, 140. [Google Scholar] [CrossRef] [PubMed]
- Jin, R.; Huang, X.; Li, H.; Yuan, Y.; Li, B.; Cheng, C.; Li, Q. Laser therapy for prevention and treatment of pathologic excessive scars. Plast. Reconstr. Surg. 2013, 132, 1747–1758. [Google Scholar] [CrossRef] [PubMed]
- Jinping, D.; Bo, C.; Yilin, C. Research progress of laser treatment for pathological scar. J. Tissue Eng. Reconstr. Surg. 2016, 12, 141–143. [Google Scholar]
- Pan, L.; Qin, H.; Li, C.; Zhang, G.; Yang, L.; Zhang, L. Efficacy of the Neodymium-Doped Yttrium Aluminum Garnet Laser in the Treatment of Keloid and Hypertrophic Scars: A Systematic Review and Meta-analysis. Aesthet. Plast. Surg. 2022, 46, 1997–2005. [Google Scholar] [CrossRef] [PubMed]
- Rikihisa, N.; Shimanouchi, K.; Saito, Y.; Sakai, H.; Mitsukawa, N. Carbon monoxide combined with artificial blood cells acts as an antioxidant for tissues thermally-damaged by dye laser irradiation. Burns 2023, 49, 388–400. [Google Scholar] [CrossRef]
- Shu, B.; Ni, G.X.; Zhang, L.Y.; Li, X.P.; Jiang, W.L.; Zhang, L.Q. High-power helium-neon laser irradiation inhibits the growth of traumatic scars in vitro and in vivo. Lasers Med. Sci. 2013, 28, 693–700. [Google Scholar] [CrossRef]
- Lev-Tov, H.; Brody, N.; Siegel, D.; Jagdeo, J. Inhibition of fibroblast proliferation in vitro using low-level infrared light-emitting diodes. Dermatol. Surg. 2013, 39, 422–425. [Google Scholar] [CrossRef]
- Khan, I.; Rahman, S.U.; Tang, E.; Engel, K.; Hall, B.; Kulkarni, A.B.; Arany, P.R. Author Correction: Accelerated burn wound healing with photobiomodulation therapy involves activation of endogenous latent TGF-beta1. Sci. Rep. 2021, 11, 17706. [Google Scholar] [CrossRef]
- Hantash, B.M.; Ubeid, A.A.; Chang, H.; Kafi, R.; Renton, B. Bipolar fractional radiofrequency treatment induces neoelastogenesis and neocollagenesis. Lasers Surg. Med. 2009, 41, 1–9. [Google Scholar] [CrossRef]
- Li, J.; Wang, D.; Wang, Y.; Du, Y.; Yu, S. Effectiveness and safety of fractional micro-plasma radio-frequency treatment combined with ablative fractional carbon dioxide laser treatment for hypertrophic scar: A retrospective study. Ann. Palliat. Med. 2021, 10, 9800–9809. [Google Scholar] [CrossRef]
- Vestita, M.; Filoni, A.; Elia, R.; Bonamonte, D.; Giudice, G. 595 nm Pulsed Dye Laser for Hypetrophic and Keloid Scars Treatment. A Randomized-Controlled Study. Plast. Reconstr. Surg. Glob. Open 2017, 5, 86–87. [Google Scholar] [CrossRef]
- Pinheiro, N.M.; Melo, P.R.; Crema, V.O.; Mendonça, A.C. Effects of radiofrequency procedure on hypertrophic scar due to burns. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 187–189. [Google Scholar] [CrossRef]
- Swanson, E. A Systematic Review of Subsurface Radiofrequency Treatments in Plastic Surgery. Ann. Plast. Surg. 2022, 89, 274–285. [Google Scholar] [CrossRef]
- Mulholland, R.S. The Science and Art of Radiofrequency Assisted Lipocoagulation (RFAL) in Body Contouring Surgery. In The Art of Body Contouring; Books on Demand: Paris, France, 2019. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- OCEBM Levels of Evidence Work Group. The Oxford Levels of Evidence 2. Oxford Center of Evidence Based Medicine. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence (accessed on 20 January 2023).
- Cooper, L.E.; Nuutila, K.; Kemp Bohan, P.M.; Diaz, V.; Batchinsky, M.; Carlsson, A.H.; Cancio, L.C.; Chan, R.K. Analysis of the Utility of CO2 and Pulse-Dye Lasers Together and Separately in the Treatment of Hypertrophic Burn Scars. Ann. Plast. Surg. 2022, 89, 166–172. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants | Intervention | Study | |
|---|---|---|---|
| Mesh word | burn* AND Cicatrix | (laser* OR light OR radiofrequency) AND therap* | Clinical Study in Humans |
| Free word | (postburn OR ‘post burn’) AND (Scar OR Scars OR Cicatrization OR Scarring OR ‘hypertrophic scar*’ OR keloid) | (‘fractional carbon dioxide’ OR ‘fractional CO2′ OR ‘pulsed dye laser’ OR PDL OR Biostimulation OR Photobiomodulation OR ‘low level laser’ OR LLLT OR ‘Neodymium Doped Yttrium Aluminum Garnet’ OR er yag OR ‘erbium‘ OR ‘nd yag’ OR photothermol* OR ‘intense pulsed light’ OR IPL OR radio-frequency) AND (treatment* OR therapeutic*) |
| Author | Year | Study | Control | Follow-Up (Month) after Final Treatment | Sample Size | Gender | Age | Treatment | Other Treatments Combined | Parameter | Device | Outcomes Measure | NIH |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Design | (M/F) | (Years) | |||||||||||
| Alsharnoubi [48] | 2018 | RCT | UAC | 3 | 15 | 5/10 | 4.73 ± 1.79 | LLLT | NA | Λ = 632.8 ED = 16 | Bbravo terza serie HENE laser (ASA s.r.i) | VSS, ST | GOOD |
| Douglas [50] | 2019 | RCT | UAC | 1.5 | 19 | 15/4 | 29 | UFCL | NA | 5% density, 300 Hz, 50 mJ | Ultrapulse, Lumenis | VSS, P-POSAS | GOOD |
| Ebid [49] | 2017 | RCT | Placebo control | 3 | 49 | 30/19 | 31.53 ± 10.14 | Pulsed Nd:YAG laser | NA | Λ = 1064, ED = 0.510–1.78, 10–40 Hz, PD = 0.12–0.15, S = 4.47 | HIRO3 machine, ASA Laser company, Italy | VAS | GOOD |
| El-Hoshy [55] | 2017 | IPCS | PC | 2 | 20 | 4/16 | 26.35 ± 9.85 | AFCL | NA | stacking, 3; PD = 0.6; spacing, 200 µm | SmartXide DOT®; DEKA, Florence, Italy | VSS, POSAS | GOOD |
| Elrod [31] | 2020 | cohort (retrospective) | PC | After the final laser session | 17 | 8/9 | 11.37 ± 4.82 | Combined AFCL + PDL (94%), with AFCL only (6%). | NA | PDL firstly: λ = 595, PD = 6–8, PD = 0.45, S = 10, no more than 30% overlap; | PDL: V-beam2; Candela, Wayland, MA, USA; AFCL: DeepFX hand-piece (Ultrapulse, Lumenis) | VSS, POSAS | GOOD |
| Secondly AFCL: 2–3% density, 250 Hz, 70–20 mJ per micropulse | |||||||||||||
| El-Zawahry [51] | 2015 | NRCT | UAC | 3 | 15 | 2/13 | 30.8 ± 11.3 | AFCL | NA | 30 W, 800 μm spacing, 800 us dwelling time (the first session followed by 30 W, 300 μm spacing, 800 us dwelling time) | NA | VSS, P-POSAS, O-POSAS | FAIR |
| Elmelegy [56] | 2018 | IPCS | PC | 1 | 65 | 49/16 | 49/16 | E-light | NA | IPL: λ = 530/560/580/630/755 (differs from patients’ skin color). ED = 6.25–6.47; S = 8–32. PD = 2–7, pulse delays 15–30 ms. RF: fluence = 10–12 J | Beijing Oriental Wison Mechanical & Electronic Co., Ltd. | VSS | GOOD |
| Gaida [52] | 2004 | NRCT | UAC | 2 | 19 | 14/5 | 38 ± 13.97 (18–77) | LLLT | NA | λ = 670, ED = 4 | Helbo®; Gallspach, Austria | VSS | FAIR |
| Ge [32] | 2022 | Cohort (retrospective) | PC | 3 | 21 | 8/13 | 31.4 (15–47) | UFCL | NA | 3–5% density, 30–300 Hz, 20–175 mJ, 1–60 W | Lumenis Ltd., Yokneam, Israel | Total POSAS | GOOD |
| Huang [57] | 2021 | IPCS | PC | 6 | 12 | 7/5 | 32 ± 11 | AFCL | Autologous fat injection in AFI group | 8% density, 40~50 mJ/cm2, 10–50 W | KL type fractional CO2 laser | mVSS | GOOD |
| Hultman [33] | 2013 | Cohort | PC | 4.65 | 147 | NA | 26.9 | PDL, UFCL, IPL, Alexandrite laser | NA | PDL: λ = 595, ED = 8.3 ± 1.1 (5.0–10.0), PD = 1.5, S = 7; end point: ecchymosis; AFCL: 15% density, 600 Hz, 15 mJ/micropulse for deep penetration; 150 Hz and 70–90 mJ/micropulse for more superficial ablation; | PDL:Candela V-beam, Wayland, MA, USA AFCL: Lumenis UltraPulse, ActiveFX, DeepFX handpieces, Santa Clara, CA, USA IPL/Nd: YAG/lightsheer diode Workstation, Santa Clara, CA, USA AL: Cynosure, Westford, MA, USA | VSS | GOOD |
| IPL: λ = 515–590, ED = 18–24; AL: λ = 755 with an aiming beam of λ = 543, S = 12, ED = 12.5 | |||||||||||||
| Issler-Fisher [45] | 2021 | Case–control | Conventional management | 5.1 | 187 | 75/112 | 39 (IQR 27–49) | UFCL | NA | ActiveFxTM (3–45% Density, 250–300 Hz, 80–125 mJ), DeepFxTM (5–15% Density, 300 Hz, 15–50 mJ) SCAAR FxTM mode (1–5% Density, 250 Hz, 60–150 mJ) | Ultrapulse, Lumenis | VSS, O-POSAS, P-POSAS, ST | GOOD |
| Joo [53] | 2022 | NRCT | UAC | 7 days after the 3rd laser treatment | 14 | 14/0 | 45.01 ± 15.03 | Er:YAG (non-ablative fractional laser) | NA | λ = 1550, 70 mJ (at level 7, with eight passes) | Fraxel Restore; Solta Medical, Pleasanton, CA, USA | ST | FAIR |
| Kemp Bohan [58] | 2021 | IPCS | PC | 2 | 21 | 17/4 | 30.0 (24.5–40.5) | UFCL | NA | 15% density, 300 Hz, 15 or 17.5 mJ | Lumenis UltraPulse Ltd., Yokneam, Israel | ST | GOOD |
| Khandelwa [34] | 2014 | Cohort (retrospective) | PC | 7 | 40 | 22/18 | 18 (1–70) | UFCL | NA | DeepFX™: 12.5–27.5 mJ, density of 15%. ActiveFX™: 90–125 mJ, density 3–5%. | Lumenis UltraPulse®, Santa Clara, CA | VSS | GOOD |
| Khedr [59] | 2020 | IPCS | PC | 3 | 50 | 27/23 | 16.76 ± 7.72 | Nd:YAG laser (n = 25) or E-light (IPL + radiofrequency) (n = 25) | NA | Nd: YAG: λ = 1064, ED = 45–75, PD = 25–45, S = 6. E-light:IPL: λ = 530–755, ED = 30–40, PD = 2–7 with 15–30 ms pulse delay, 8 mm × 32 mm hand piece. RF: 6–10 J/cm3 | Nd: YAG laser (Cynergy; Cynosure Inc, Westford, MA), E-light (two-handle beauty machine; Beijing Oriental Wison Mechanical & Electronic Co., Ltd.) | VSS | GOOD |
| Kono [54] | 2005 | NRCT | UAC | 1 | 15 | 8/7 | 13.7 (1–42) | Long-pulsed PDL | NA | Λ = 595, S = 7, ED = 9–10, PD = 1.5–10 | model V-beam; Candela Laser Corporation, Wayland, MA | mVGH | FAIR |
| Lei [60] | 2015 | IPCS | PC | 3.75 | 63 | 25/38 | 16–45 | UFCL | Traditional Chinese medicine | P = 25~32 W, PD = 4~6, spacing 0.6~1.0 mm (for early stage of scar growth, 1.0 mm, decreasing with the number of treatments) | LJL35-CS Ultra Pulse CO2 Fractional Laser | VSS | GOOD |
| Li [35] | 2021 | Cohort (retrospective) | PC | 1 | 165 | 79/86 | 3.5 ± 3.02 | UCFL | NA | 5% density, 30–50 mJ/microbeam exposure | Lumenis Ltd., Yokneam, Israel | VSS, ST | GOOD |
| Li * [43] | 2021 | Case–control (retrospective) | PC | 12 | 105 | 46/59 | 39.5 ± 6.02 | 595 nm PDL | NA | PD = 0.45, ED = 5–9 (low ED: 5–7 and high ED = 7–9), S = 7 | Vbeam Perfecta, Candela, USA | VSS, ST | GOOD |
| Li [36] | 2018 | Cohort (retrospective) | PC | 1–2 | 221 | 81/140 | 3–48 (29 ± 8) | 595-PDL or UFCL | NA | PDL: λ = 595, S = 7, PD = 0.45~1.50, ED = 5.0~7.0. CO2: For scar height <2 mm, choose Deep FX mode (5~10% density, 25~50 mJ); for scar height ≥2 mm, choose Scaar FX mode (3~5% density, 60~120 mJ) | PDL: Vbeam Perfecta, Candela, USA; CO2: Ultra Pulse CO2 Fractional Laser (Cornmedical Medical Laser, Inc., USA) | VSS, VAS | GOOD |
| Liu [44] | 2022 | Case–control (retrospective) | Conventional surgery | 1–1.5 | 46 | 28/18 | 38.22 ± 10.28 | UFCL | NA | 3–5% density, 20–150 MJ, depth: 0.4–4 mm | UltraPulse® Encore; Lumenis™ | P-POSAS | GOOD |
| Majid [61] | 2018 | IPCS (open-label study) | PC | 3 | 10 | 3/7 | 9.7 (5–12) | AFCL | Topical corticosteroids | 8.4% density, 90–150 mJ at 30 W | eCO2 Laser; Lutronics Corp., Seoul, South Korea | VSS | GOOD |
| Matuszczak [62] | 2021 | IPCS | PC | 1.25–1.5 | 25 | 16/9 | 6.40 ± 1.72 | PDL followed by AFCL | NA | PDL: λ = 595, ED = 6.86 (5–10); AFCL: 75.12 mJ (54–80 mJ). | PDL: Syneron Candela VBeam Perfecta, Wayland, MA; AFCL: Smaxe | VSS, P-POSAS | GOOD |
| Miletta [63] | 2021 | IPCS | PC | 6 | 22 | 15/7 | 28 ± 16.8 | UFCL | NA | 5–10% density, 30–50 mJ, depth 1.2–2.2 mm | Lumenis Ltd., Yokneam, Israel | P-POSAS, O-POSAS, ST | GOOD |
| Patel [37] | 2019 | Cohort | PC | After all laser treatment | 49 | 26/23 | 4.86 ± 4.5 | UFCL | NA | First pass: SCAAR FX (majority): for scar depth: 1–3 mm: 1.7% density, 250 Hz, 101.6 mJ. Second pass: DeepFX for scar depth less than 1 mm: 5.3% density, 266.2 Hz, 13.7 mJ and ActiveFX (minority) | Ultrapulse, Lumenis | O-POSAS, P-POSAS, total POSAS | GOOD |
| Poetschke [64] | 2017 | IPCS | PC | 6 | 10 | 3/7 | 39.3 ± 15.3 | UFCL | NA | First: ScaarFX, shape 2, size 10, pulse 1, density 1%, repeat delay 0.3 s, 250 Hz, 70–120 mJ; Second: ActiveFX: 9% density, 40 mJ, 350 Hz, pattern 1, size 2, repeat delay 0.1 s. Finally: ActiveFX: 2% density, 100 mJ, 125 Hz, pattern 1, size 6, repeat delay 0.1 s | Ultrapulse, Lumenis | VSS, O-POSAS, P-POSAS | GOOD |
| Tan [38] | 2021 | Cohort (retrospective) | PC | 1 | 221 | 118/103 | 33.6 ± 11.8 | AFCL | NA | Deep mode: 5–10% density, 15–30 MJ, depth of 550–800 μm. Superficial mode: 40% density, 70–150 MJ, depth of 50–150 μm | AcuPulse; Lumenis Ltd., Yokneam, Israel | VSS | GOOD |
| Tawfic [65] | 2020 | IPCS | PC | 3 | 25 | 2/23 | 22.04 ± 9.92 | AFCL OR FMR (fractional microneedle radiofrequency) | NA | FMR: power level of eight to nine (max 70 w), an exposure time of 800 ms, a depth of 2 mm (using non-insulated needles, 2 Hz frequency, and 2 passes and diameters of 0.3 mm per needle). AFCL: 18–20 W, 800–1000 µs dwell time, 500–600 μm spacing (13% density), microspot size 120 μm, two to three stacks | FMR:VIVACE™ combine microneedling with bipolar RF; AFCL: DEKA Smartxide DOT, Italy | VSS, POSAS | GOOD |
| Tawfic [47] | 2022 | RCT | PC | 1 | 20 | 2/18 | 24.80 ± 9.87 (16–48) | AFCL | NA | 20 W, 800–1000 ms dwell time, and 2–3 stacks for scar thickness (low-density, 900 mm, medium-density, 600 mm, spacing (12.6% density), high-density, 300 mm spacing (25.6% density)) | The DEKA; Smart Xide DOT, Calenzano, Italy | O-POSAS, P-POSAS | GOOD |
| Travis [39] | 2022 | Cohort | PC | 1–2 weeks | 23 | 16/13 | 49.1 (IQR: 36.7–58.6) | AFCL | NA | Firstly, SCAARFx modality 1% density, 70 mJ | Ultrapulse, Lumenis, Yokneam, Israel | VSS, O-POSAS, P-POSAS, total POSAS | GOOD |
| Wang [66] | 2017 | IPCS | PC | 6 | 95 | 40/55 | 22.9 (12–55) | FMR (fractional microplasma radiofrequency) | NA | Roller tip at 50–80 watts; 3–4 passes in different directions over each area with a high rolling speed of 5 cm/s and a delay of 5–10 s between passes | Pixel RF, Accent XL; Alma Lasers, Caesarea, Israel | O-POSAS, P-POSAS, total POSAS | GOOD |
| Weshahy [67] | 2020 | IPCS | PC | 2 | 15 | 8/7 | 38.95 ± 8.85 | AFCL | Combined with growth factors in group AFCL + GF | Smart stack, dot mode, power: 30 W, dwell time: 800 ms, spacing: 400 μm and smart stacking: 2, depth 200 µm, S = 15, 17% density. Readymade GFs after sessions for at least 6 h | SmartXide DOT®; DEKA, Florence, Italy | VSS, O-POSAS, P-POSAS, total POSAS | GOOD |
| Woods [40] | 2022 | Cohort | PC | 18 months after injury | 21 | NA | NA | PDL (13) or Nd:YAG Q-switched KTP laser (8) or combined | NA | PDL: λ = 595, S = 7–10, PD = 0.5–10, ED = 7–12, KTP: λ = 532, S = 2–6, ED = 1–6 | V-Beam 595 pulsed dye laser (Candela), Nd: YAG Q-switched KTP laser (Cynosure) | Total POSAS | GOOD |
| Xie [41] | 2018 | Cohort | PC | 11 | 221 | 118/103 | 8 (IQR: 4, 31) | PDL + AFCL | NA | PDL:λ = 595, S = 7–12, PD = 1.5–3.0, ED = 8.0~9.5. AFCL: For scar height < 1 mm, choose Deep FX mode: 5~10% density, 25~50 mJ; for scar height ≥1 mm, choose Scaar FX mode: 3~5% density, 80~150 mJ | PDL, Vbeam Platinum, Candela, USA | Self-made scar rating score (refer to the VSS), ST | GOOD |
| AFCL: UltraPulse Encor, Lumenis, USA | |||||||||||||
| Yang [68] | 2022 | IPCS | PC | 1 | 169 | 92/77 | 3.28 (1–6) | UFCL | NA | 1. Scar height ≤2 mm, ActiveFX: 125 mJ, 50 Hz; Deepn FX: 25–50 mJ, 5–10% density | UltraPulse Encor, Lumenis, Santa Clara, CA, USA | VSS | GOOD |
| 2. Scar height ≥2 mm, ActiveFX: 150 mJ, 150 Hz; Deepn FX: 60–120 mJ, 3–5% density | |||||||||||||
| Yang [46] | 2021 | RCT | PC | 3 | 20 | 13/7 | 26 (3–67) | PDL | NA | λ = 595, S = 7, ED = 5–7 PD = 0.45–1.50 | America, Candela Company | VSS | GOOD |
| Zuccaro [42] | 2021 | Cohort | PC | 12 | 32 | 13/7 | 5.89 | AFCL or AFCL + PDL | NA | PDL: λ = 595, ED = 5.50 (5.00–7.00); PD = 0.45 (0.45–1.50) | PDL (Vbeam Perfecta, Candela Corporation, Wayland, MA, USA) | VSS, P–POSAS, O–POSAS | GOOD |
| AFCL: deep: 5% density; 70.00 mJ | AFCL (CO2RE, Candela Corporation, Wayland, MA, USA) | ||||||||||||
| Fusion: core energy: 70.00 mJ, ring energy: 48.00–55.20 mJ, 20–25% density | |||||||||||||
| Zuccaro [69] | 2018 | IPCS | PC | Differed for each patient | 71 | NA | 6.62 | PDL or AFCL or AFCL + PDL | NA | PDL:ED = 6.45 (5–9). | PDL: Syneron Candela Vbeam Perfecta, Wayland, MA, USA AFCL:Syneron Candela CO2RE, Wayland, MA, USA | VSS | GOOD |
| AFCL: core energy 70.86 mJ (53–78 mJ); settings: fusion and deep modes (most-used) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bai, Y.; Zhang, Y.; Ni, W.; Yao, M. Laser, Intense Pulsed Light, and Radiofrequency for the Treatment of Burn Scarring: A Systematic Review and Meta-Analysis. Eur. Burn J. 2023, 4, 142-162. https://doi.org/10.3390/ebj4020013
Bai Y, Zhang Y, Ni W, Yao M. Laser, Intense Pulsed Light, and Radiofrequency for the Treatment of Burn Scarring: A Systematic Review and Meta-Analysis. European Burn Journal. 2023; 4(2):142-162. https://doi.org/10.3390/ebj4020013
Chicago/Turabian StyleBai, Yubing, Yiqiu Zhang, Wei Ni, and Min Yao. 2023. "Laser, Intense Pulsed Light, and Radiofrequency for the Treatment of Burn Scarring: A Systematic Review and Meta-Analysis" European Burn Journal 4, no. 2: 142-162. https://doi.org/10.3390/ebj4020013
APA StyleBai, Y., Zhang, Y., Ni, W., & Yao, M. (2023). Laser, Intense Pulsed Light, and Radiofrequency for the Treatment of Burn Scarring: A Systematic Review and Meta-Analysis. European Burn Journal, 4(2), 142-162. https://doi.org/10.3390/ebj4020013