

Review of Indications for Endotracheal Intubation in Burn Patients with Suspected Inhalational Injury

 ,
,
Abstract
1. Introduction
Aims
2. Materials and Methods
3. Results
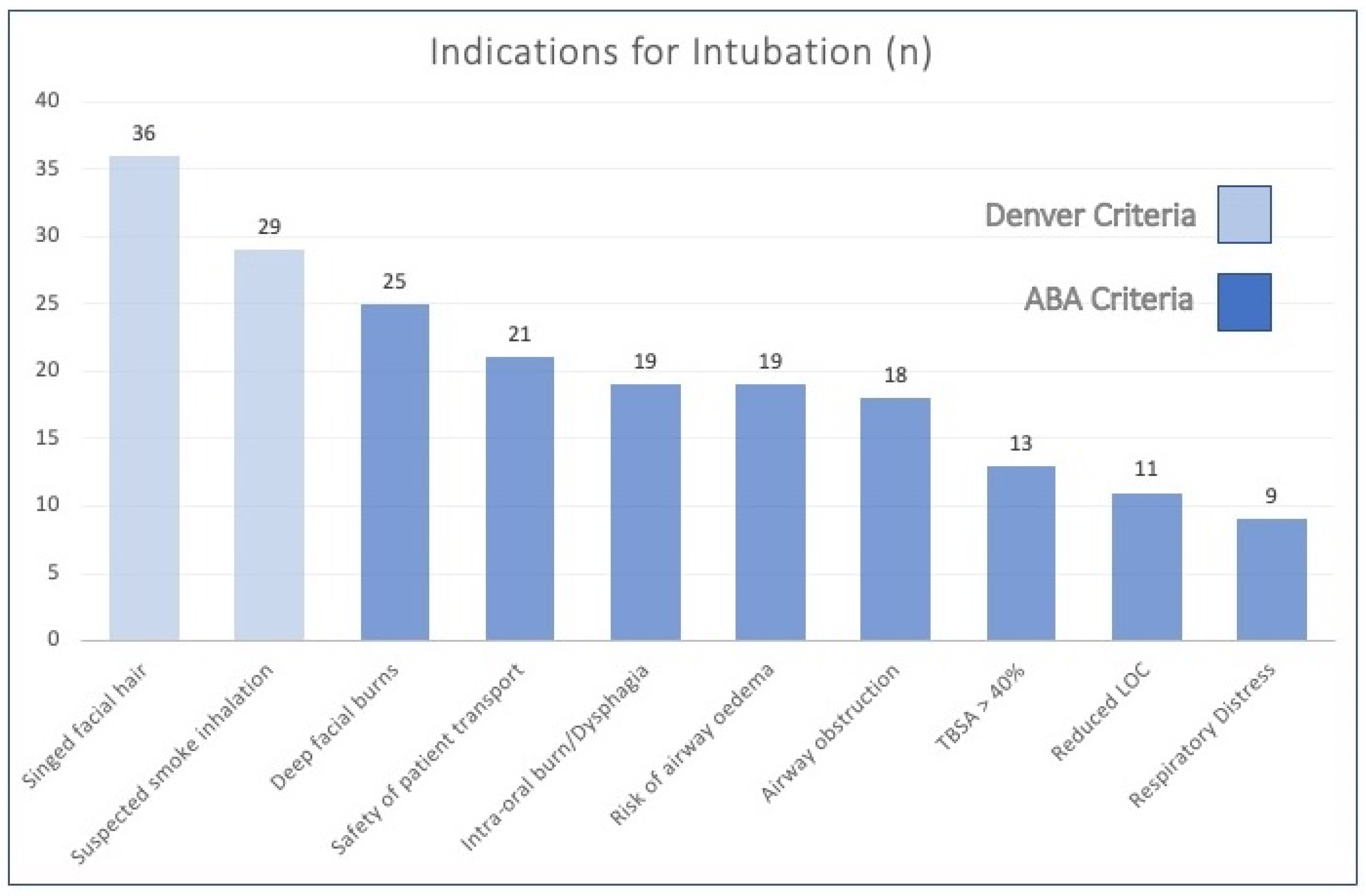
3.1. Concordance with ABA and Denver Indications for Intubation
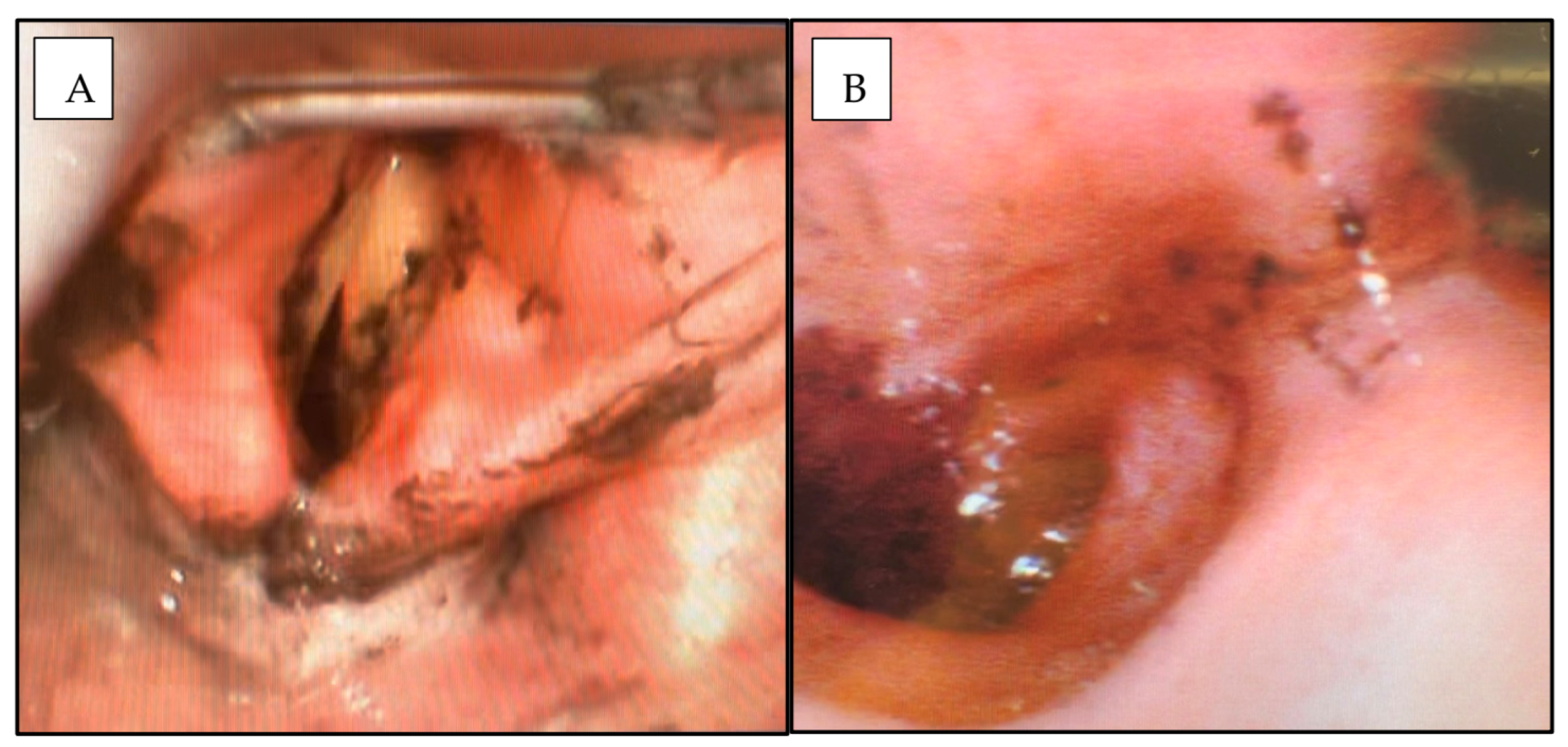
3.2. Bronchoscopic Findings
3.3. Policy of Early Extubation and Prediction of Extubation Failure
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization. Media Centre, Fact Sheet, Burns. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/burns (accessed on 9 February 2023).
- Australian Institute of Health and Welfare. Thermal Causes. 2021. Available online: https://www.aihw.gov.au/reports/injury/burns-and-other-thermal-causes (accessed on 9 February 2023).
- Colohan, S.M. Predicting Prognosis in Thermal Burns with Associated Inhalational Injury: A Systematic Review of Prognostic Factors in Adult Burn Victims. J. Burn. Care Res. 2010, 31, 529–539. [Google Scholar] [CrossRef] [PubMed]
- Foster, K.N.; Holmes, J.H., IV. Inhalation Injury: State of the Science 2016. J. Burn. Care Res. 2017, 38, 137–141. [Google Scholar] [PubMed]
- Tracy, L.M.; Dyson, K.; Le Mercier, L.; Cleland, H.; McInnes, J.A.; Cameron, P.A.; Singer, Y.; Edgar, D.W.; Darton, A.; Gabbe, B.J. Variation in documented inhalation injury rates following burn injury in Australia and New Zealand. Injury 2020, 51, 1152–1157. [Google Scholar]
- Toppi, J.; Cleland, H.; Gabbe, B. Severe burns in Australian and New Zealand adults: Epidemiology and burn centre care. Burns 2019, 45, 1456–1461. [Google Scholar] [PubMed]
- Eastman, A.L.; Arnoldo, B.A.; Hunt, J.L.; Purdue, G.F. Pre-burn center management of the burned airway: Do we know enough? J. Burn. Care Res. 2010, 31, 701–705. [Google Scholar] [PubMed]
- Moshrefi, S.; Sheckter, C.C.; Shepard, K.; Pereira, C.; Davis, D.J.; Karanas, Y.; Rochlin, D.H. Preventing Unnecessary Intubations: A 5-Year Regional Burn Center Experience Using Flexible Fiberoptic Laryngoscopy for Airway Evaluation in Patients With Suspected Inhalation or Airway Injury. J. Burn. Care Res. 2019, 40, 341–346. [Google Scholar]
- American Burn Association. Advanced burn life support provider manual 2018 update. J. Burn. Care Res. 2018. [Google Scholar]
- ISBI Practice Guidelines Committee; Advisory Subcommittee; Steering Subcommittee. ISBI practice guidelines for burn care, part 2. Burns 2018, 44, 1617–1706. [Google Scholar] [CrossRef]
- Dingle, L.A.; Wain, R.A.J.; Bishop, S.; Soueid, A.; Sheikh, Z. Intubation in burns patients: A 5-year review of the Manchester regional burns centre experience. Burns 2020, 47, 576–586. [Google Scholar]
- Kim, Y.; Kym, D.; Hur, J.; Yoon, J.; Yim, H.; Cho, Y.S.; Chun, W. Does inhalation injury predict mortality in burns patients or require redefinition? PLoS ONE 2017, 12, e0185195. [Google Scholar]
- Walker, P.F.; Buehner, M.F.; Wood, L.A.; Boyer, N.L.; Driscoll, I.R.; Lundy, J.B.; Cancio, L.C.; Chung, K.K. Diagnosis and management of inhalation injury: An updated review. Crit. Care 2015, 19, 351. [Google Scholar] [PubMed]
- Aung, M.T.; Garner, D.; Pacquola, M.; Rosenblum, S.; McClure, J.; Cleland, H.; Pilcher, D.V. The use of a simple three-level bronchoscopic assessment of inhalation injury to predict in-hospital mortality and duration of mechanical ventilation in patients with burns. Anaesth. Intensive Care 2018, 46, 67–73. [Google Scholar] [CrossRef]
- Yang, K.L.; Tobin, M.J. A Prospective Study of Indexes Predicting the Outcome of Trials of Weaning from Mechanical Ventilation. N. Engl. J. Med. 1991, 324, 1445–1450. [Google Scholar] [CrossRef] [PubMed]
- Meade, M.; Guyatt, G.; Cook, D.; Griffith, L.; Sinuff, T.; Kergl, C.; Mancebo, J.; Esteban, A.; Epstein, S. Predicting success in weaning from mechanical ventilation. Chest 2001, 120, 400S–424S. [Google Scholar] [PubMed]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar]
- Moore, E.C.; Pilcher, D.V.; Bailey, M.J.; Cleland, H.; McNamee, J. A simple tool for mortality prediction in burns patients: APACHE III score and FTSA. Burns 2010, 36, 1086–1091. [Google Scholar] [PubMed]
- Cook, D.A.; Joyce, C.J.; Barnett, R.J.; Birgan, S.P.; Playford, H.; Cockings, J.G.L.; Hurford, R.W. Prospective independent validation of APACHE III models in an Australian tertiary adult intensive care unit. Anaesth. Intensive Care 2002, 30, 308–315. [Google Scholar] [PubMed]
- Tanaka, Y.; Shimizu, M.; Hirabayashi, H. Acute physiology, age, and chronic health evaluation (APACHE) III score is an alternative efficient predictor of mortality in burn patients. Burns 2007, 33, 316–320. [Google Scholar] [CrossRef]
- Miller, A.; Elamin, E.; Suffredini, A. Inhaled Anticoagulation Regimens for the Treatment of Smoke Inhalation-Associated Acute Lung Injury: A Systematic Review. Crit. Care Med. 2014, 42, 413–419. [Google Scholar] [PubMed]
- Lan, X.; Huang, Z.; Tan, Z.; Huang, Z.; Wang, D.; Huang, Y. Nebulized heparin for inhalation injury in burn patients: A systematic review and meta-analysis. Burn. Trauma 2020, 8, tkaa015. [Google Scholar]
- Badulak, J.; Schurr Sauaia, A.; Ivanschenko, A.; Peltz, E. Defining the criteria for intubation of the patient with thermal burns. Burns 2018, 44, 531–538. [Google Scholar]
- Danne, P.D. Trauma management in Australia and the tyranny of distance. World J. Surg. 2003, 27, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Ching, J.A.; Ching, Y.H.; Shivers, S.C.; Karlnoski, R.A.; Payne, W.G.; Smith, D.J., Jr. An Analysis of Inhalation Injury Diagnostic Methods and Patient Outcomes. J. Burn. Care Res. 2016, 37, e27–e32. [Google Scholar] [CrossRef]
- Ching, J.A.; Shah, J.L.; Doran, C.J.; Chen, H.; Payne, W.G.; Smith, D.J., Jr. The evaluation of physical exam findings in patients assessed for suspected burn inhalation injury. J. Burn. Care Res 2015, 36, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Madnani, D.D.; Steele, N.P.; de Vries, E. Factors that predict the need for intubation in patients with smoke inhalation injury. Ear Nose Throat J. 2006, 85, 278–280. [Google Scholar] [CrossRef] [PubMed]
- Holley, A.; Reade, M.; Lipman, J.; Cohen, J. There is no fire without smoke! Pathophysiology and treatment of inhalational injury in burns: A narrative review. Anaesth. Intensive Care 2020, 48, 114–122. [Google Scholar]
- Woodson, L.C.; Talon, M.; Medieros, F.; Knox, S.L.; McQuitty, A. Risk of intubations before transport to burn center. J. Burn. Care Res. 2017, 38, e994. [Google Scholar] [CrossRef]
- Toon, M.; Maybauer, M.; Greenwood, J.; Maybauer, D.; Fraser, J. Management of acute smoke inhalation injury. Crit. Care Resusc. 2010, 12, 53–61. [Google Scholar]
- Greenwood, J.E. Advantages of immediate excision of burn eschar. Anaesth. Intensive Care 2020, 48, 89–92. [Google Scholar]



{kind=link}
{kind=link}
| ABA Criteria [9] (2018) | Denver Criteria [10] (2018) |
|---|---|
| Signs of airway obstruction—hoarseness, stridor, accessory muscle use, and sternal retraction | Any of the ABA criteria listed with two additional indications below |
| Extent of burn > 40% TBSA | Singed facial or nasal hair |
| Extensive facial burns—deep dermal or full thickness depth | Suspected smoke inhalation |
| Dysphagia | |
| Intra-oral burns | |
| Signs of respiratory compromise—respiratory fatigue, hypoxia, and poor ventilation | |
| Reduced level of consciousness (LOC) with loss of protective reflexes | |
| Anticipated transfer of patient with major burn to burn centre without qualified medical professional to intubate en route | |
| Significant risk of oedema which may compromise airway |
| Demographic/Characteristic | Value | |
|---|---|---|
| Total Patients, n | 55 | |
| Mean Patient Age, years | 48.2 (16–84) | |
| Male:Female | 3:1 (n = 44 Male, n = 14 Female) | |
| Mortality, n (% of total cohort) | 5 (9%) | |
| Location of Intubation, n | Pre-RAH—32 | Pre-Hospital—21 |
| Other Hospital—11 | ||
| RAH—23 | ||
| Median Total Length of Acute Hospital stay | 40 days (range 1–258) | |
| Median Length of ICU stay | 4 days (range 1–50) | |
| Mean Ventilated days | 5 days (range 0–39) | |
| Median TBSA % | 20% (range 1–80) | |
| Mean APACHE II Score | 15 (range 2–30) | |
| Mean APACHE III-j Score | 53 (range 13–122) | |
| All Patients | Extubated within 48 h | Extubated from 48 h to 7 Days | Extubation > 7 Days | |
|---|---|---|---|---|
| Single indication | 7 | 4 | 2 | 1 |
| Multiple indications | 48 | 27 | 10 | 11 |
| Total | 55 | 31 | 12 | 12 |
| AIS Grade | 0 | 1 | 2 | 3 | 4 | Total |
|---|---|---|---|---|---|---|
| Grade Description | No injury | Mild injury | Moderate injury | Severe injury | Massive injury | |
| Patient numbers | 16 | 4 | 3 | 1 | 0 | 24 |
| Patient | TBSA and AIS Grade | Cause of Extubation Failure | VAP | Day Post-Burn at Failed Extubation | Day Post-Burn at Successful Extubation | RSBI |
|---|---|---|---|---|---|---|
| 1. | 60% TBSA with Grade 1 injury | Immediate oxygen desaturation | N | Day 3 | Day 7 | 44 |
| 2. | 7% TBSA with Grade 2 injury | Respiratory distress and tachypnea | N | Day 3 | Day 12 | 28 |
| 3. | 60% TBSA with Grade 1 injury | Respiratory distress and tachypnea | N | Day 5 | Day 6 | 40 |
| 4. | 7% TBSA with Grade 2 injury | Agitation and excessive respiratory secretions | Y | Day 4 and Day 9 | Tracheostomy decannulated Day 14 | 63 |
| 5. | 3% TBSA with Grade 0 injury and reduced GCS (Diffuse axonal injury) | Oxygen desaturation and excessive respiratory secretions | Y | Day 5 | Tracheostomy decannulated Day 38 | 37 |
| 6. | 20% TBSA with Grade 1 injury | Facial swelling and respiratory secretions | Y | Day 1 | Day 4 | 31 |
| 7. | 36% TBSA with Grade 0 injury and reduced GCS (Alcoholic Encephalopathy) | Poor spontaneous respiratory effort on attempted weaning | N | Day 1 | Day 4 | 37 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Concannon, E.; Damkat Thomas, L.; Kerr, L.; Damkat, I.; Reddi, B.; Greenwood, J.E.; Solanki, N.S.; Wagstaff, M.J.D. Review of Indications for Endotracheal Intubation in Burn Patients with Suspected Inhalational Injury. Eur. Burn J. 2023, 4, 163-172. https://doi.org/10.3390/ebj4020014
Concannon E, Damkat Thomas L, Kerr L, Damkat I, Reddi B, Greenwood JE, Solanki NS, Wagstaff MJD. Review of Indications for Endotracheal Intubation in Burn Patients with Suspected Inhalational Injury. European Burn Journal. 2023; 4(2):163-172. https://doi.org/10.3390/ebj4020014
Chicago/Turabian StyleConcannon, Elizabeth, Lindsay Damkat Thomas, Lachlan Kerr, Ivo Damkat, Benjamin Reddi, John E. Greenwood, Nicholas S. Solanki, and Marcus J. D. Wagstaff. 2023. "Review of Indications for Endotracheal Intubation in Burn Patients with Suspected Inhalational Injury" European Burn Journal 4, no. 2: 163-172. https://doi.org/10.3390/ebj4020014
APA StyleConcannon, E., Damkat Thomas, L., Kerr, L., Damkat, I., Reddi, B., Greenwood, J. E., Solanki, N. S., & Wagstaff, M. J. D. (2023). Review of Indications for Endotracheal Intubation in Burn Patients with Suspected Inhalational Injury. European Burn Journal, 4(2), 163-172. https://doi.org/10.3390/ebj4020014