
Complications during Pregnancy after Abdominal Burn Scars: A Review

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Search Strategy
2.3. Selection Process and Criteria
2.4. Data Extraction
2.5. Risk of Bias Assessment
2.6. Strategy for Data Synthesis
3. Results
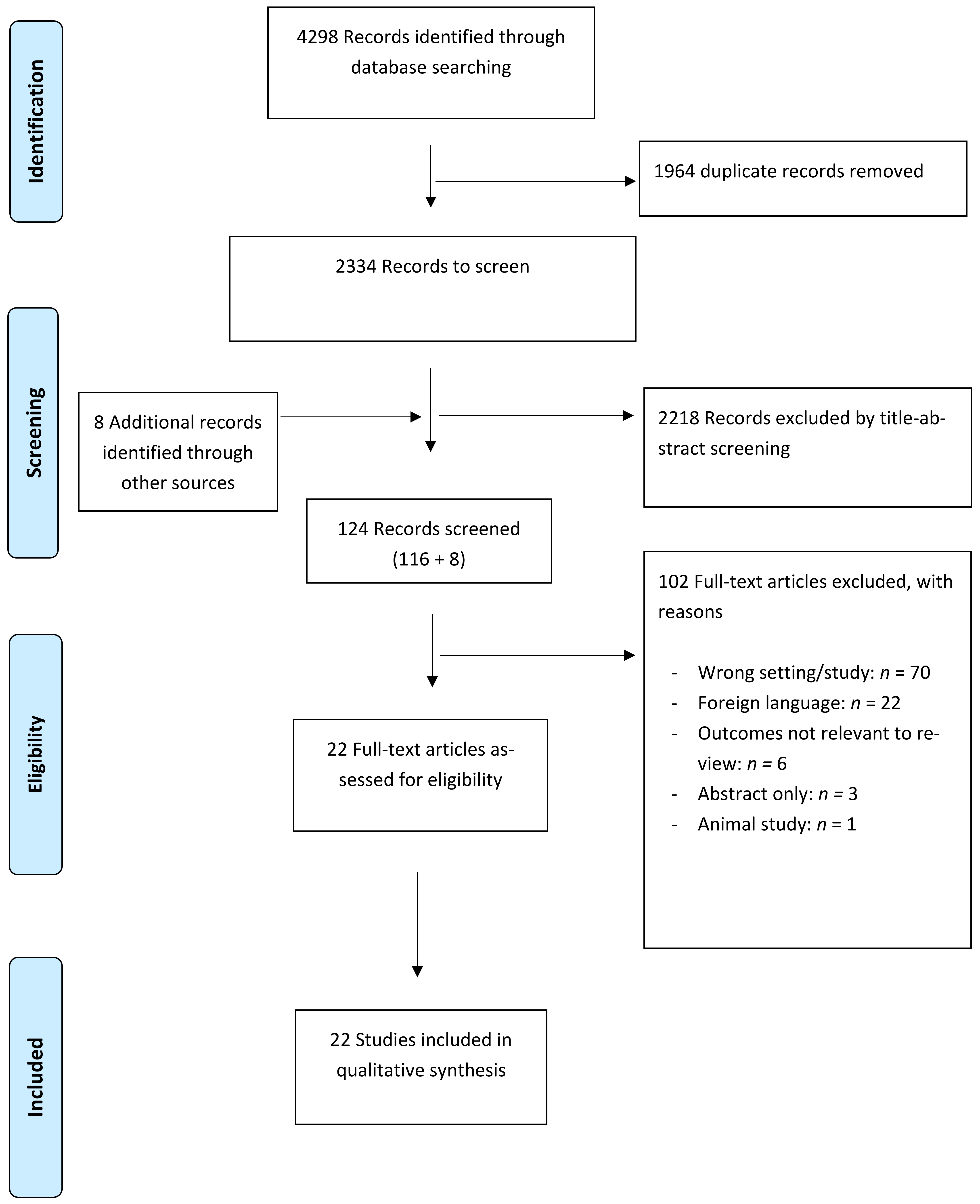
3.1. Literature Search
3.2. Study and Patient Characteristics
3.3. Patient and Burn Characteristics
3.4. Abdominal Burn Scar Complications
Other Symptoms
3.5. Foetal Complications
3.6. Other Complications
3.6.1. Delivery Mode
3.6.2. Effects on Breastfeeding
3.7. Positive Effects
3.7.1. Scar Improvement
3.7.2. Pregnancy as a Natural Tissue Expander
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Search | Query | Items Found |
|---|---|---|
| #8 | #4 OR #7 | 1388 |
| #7 | #5 AND #6 | 248 |
| #6 | “pregnan*“[ti] OR “pregnan*”[ot] OR “vaginal”[ti] OR “vaginal”[ot] OR “abdominal”[ti] OR “abdominal”[ot] OR “truncal”[ti] OR “truncal”[ot] | 402,641 |
| #5 | “burn”[ti] OR “burns”[ti] OR “scald*”[ti] OR “postburn *”[ti] OR (“thermal”[ti] AND “injur*”[ti]) OR (“chemical”[ti] AND “injur *”[ti]) OR “burn”[ot] OR “burns”[ot] OR “scald*”[ot] OR “postburn *”[ot] OR (“thermal”[ot] AND “injur*”[ot]) OR (“chemical”[ot] AND “injur*”[ot]) | 44,069 |
| #4 | #1 AND #2 AND #3 | 1153 |
| #3 | “abdom*”[tw] OR “truncal”[tiab] | 428,002 |
| #2 | “Pregnancy Complications”[Mesh] OR “Gestational Age”[Mesh] OR “Pregnancy”[Mesh] OR “Pregnancy Trimesters”[Mesh] OR “Pregnant Women”[Mesh] OR “Preconception Care”[Mesh] OR “Maternal Mortality”[Mesh] OR “Maternal Health”[Mesh] OR “Fetal Mortality”[Mesh] OR “Delivery, Obstetric”[Mesh] OR “maternal”[tiab] OR “mother*”[tiab] OR “fetal”[tiab] OR “foetal”[tiab] OR “fetus”[tiab] OR “foetus”[tiab] OR “maternity”[tiab] OR “pregnan*”[tiab] OR “pseudopregnan*”[tiab] OR “gravidit*”[tiab] OR “nulligravid*”[tiab] OR “primigravid*”[tiab] OR “multigravid*”[tiab] OR “gravidation”[tiab] OR “gravidarum”[tiab] OR “gravida”[tiab] OR “parturition*”[tiab] OR “parity”[tiab] OR “childbirth*”[tiab] OR “birthing”[tiab] OR “birth”[tiab] OR “stillbirth”[tiab] OR “childbed”[tiab] OR (“abdominal”[tiab] AND “deliver*”[tiab]) OR “gestation*”[tiab] OR “parturien*”[tiab] OR “child-bear*”[tiab] OR “childbear*”[tiab] OR “placentat*”[tiab] OR “prepregnan*”[tiab] OR “conception*”[tiab] OR “preconception*”[tiab] OR “obstetric*”[tiab] OR “prenatal”[tiab] OR “perinatal”[tiab] OR “intranatal”[tiab] OR “antenatal”[tiab] OR “prepartum”[tiab] OR “peripartum”[tiab] OR “intrapartum”[tiab] OR “antepartum”[tiab] OR “pre-natal”[tiab] OR “peri-natal”[tiab] OR “intra-natal”[tiab] OR “ante-natal”[tiab] OR “pre-partum”[tiab] OR “peri-partum”[tiab] OR “intra-partum”[tiab] OR “ante-partum”[tiab] | 1,625,975 |
| #1 | “Cicatrix”[Mesh] OR “cicatr*”[tiab] OR “keloid*”[tiab] OR “scar”[tiab] OR “scars”[tiab] OR “scarring”[tiab] OR “contractur*”[tiab] | 123,866 |
| Search | Query | Items Found |
|---|---|---|
| #9 | #8 NOT (‘conference abstract’/it OR ‘conference review’/it) | 1778 |
| #8 | #4 OR #7 | 2433 |
| #7 | #5 AND #6 | 274 |
| #6 | ‘pregnan*’:ti OR ‘pregnan*’:kw OR ‘vaginal’:ti OR ‘vaginal’:kw OR ‘abdominal’:ti OR ‘abdominal’:kw OR ‘truncal’:ti OR ‘truncal’:kw | 511,336 |
| #5 | ‘burn’:ti OR ‘burns’:ti OR ‘scald*’:ti OR ‘postburn*’:ti OR (‘thermal’:ti AND ‘injur*’:ti) OR (‘chemical’:ti AND ‘injur*’:ti) OR ‘burn’:kw OR ‘burns’:kw OR ‘scald*’:kw OR ‘postburn*’:kw OR (‘thermal’:kw AND ‘injur*’:kw) OR (‘chemical’:kw AND ‘injur*’:kw) | 53,170 |
| #4 | #1 AND #2 AND #3 | 2171 |
| #3 | ‘abdom*’:ab,ti,kw,de OR ‘truncal’:ab,ti,kw | 769,423 |
| #2 | ‘pregnancy complication’/exp OR ‘gestational age’/exp OR ‘pregnancy’/exp OR ‘named groups by pregnancy’/exp OR ‘prepregnancy care’/exp OR ‘maternal mortality’/exp OR ‘maternal welfare’/exp OR ‘fetus mortality’/exp OR ‘fetal health’/exp OR ‘obstetric delivery’/exp OR ‘maternal’:ab,ti,kw OR ‘mother*’:ab,ti,kw OR ‘fetal’:ab,ti,kw OR ‘foetal’:ab,ti,kw OR ‘fetus’:ab,ti,kw OR ‘foetus’:ab,ti,kw OR ‘maternity’:ab,ti,kw OR ‘pregnan*’:ab,ti,kw OR ‘pseudopregnan*’:ab,ti,kw OR ‘gravidit*’:ab,ti,kw OR ‘nulligravid*’:ab,ti,kw OR ‘primigravid*’:ab,ti,kw OR ‘multigravid*’:ab,ti,kw OR ‘gravidation’:ab,ti,kw OR ‘gravidarum’:ab,ti,kw OR ‘gravida’:ab,ti,kw OR ‘parturition*’:ab,ti,kw OR ‘parity’:ab,ti,kw OR ‘childbirth*’:ab,ti,kw OR ‘birthing’:ab,ti,kw OR ‘birth’:ab,ti,kw OR ‘stillbirth’:ab,ti,kw OR ‘childbed’:ab,ti,kw OR (‘abdominal’:ab,ti,kw AND ‘deliver*’:ab,ti,kw) OR ‘gestation*’:ab,ti,kw OR ‘parturien*’:ab,ti,kw OR ‘child-bear*’:ab,ti,kw OR ‘childbear*’:ab,ti,kw OR ‘placentat*’:ab,ti,kw OR ‘prepregnan*’:ab,ti,kw OR ‘conception*’:ab,ti,kw OR ‘preconception*’:ab,ti,kw OR ‘obstetric*’:ab,ti,kw OR ‘prenatal’:ab,ti,kw OR ‘perinatal’:ab,ti,kw OR ‘intranatal’:ab,ti,kw OR ‘antenatal’:ab,ti,kw OR ‘prepartum’:ab,ti,kw OR ‘peripartum’:ab,ti,kw OR ‘intrapartum’:ab,ti,kw OR ‘antepartum’:ab,ti,kw OR ‘pre-natal’:ab,ti,kw OR ‘peri-natal’:ab,ti,kw OR ‘intra-natal’:ab,ti,kw OR ‘ante-natal’:ab,ti,kw OR ‘pre-partum’:ab,ti,kw OR ‘peri-partum’:ab,ti,kw OR ‘intra-partum’:ab,ti,kw OR ‘ante-partum’:ab,ti,kw | 1,958,693 |
| #1 | ‘scar’/exp OR ‘cicatr*’:ab,ti,kw OR ‘keloid*’:ab,ti,kw OR ‘scar’:ab,ti,kw OR ‘scars’:ab,ti,kw OR ‘scarring’:ab,ti,kw OR ‘contractur*’:ab,ti,kw | 167,645 |
| Search | Query | Items Found |
|---|---|---|
| #8 | #4 OR #7 | 1132 |
| #7 | #5 AND #6 | 278 |
| #6 | TITLE (“pregnan*” OR “vaginal” OR “abdominal” OR “truncal”) OR AUTHKEY (“pregnan*” OR “vaginal” OR “abdominal” OR “truncal”) | 498,977 |
| #5 | TITLE (“burn” OR “burns” OR “scald*” OR “postburn*” OR (“thermal” AND “injur*”) OR (“chemical” AND “injur*”)) OR AUTHKEY (“burn” OR “burns” OR “scald*” OR “postburn*” OR (“thermal” AND “injur*”) OR (“chemical” AND “injur*”)) | 64,253 |
| #4 | #1 AND #2 AND #3 | 865 |
| #3 | TITLE-ABS (“abdom*” OR “truncal”) OR AUTHKEY (“abdom*” OR “truncal”) | 463,391 |
| #2 | TITLE-ABS (“maternal” OR “mother*” OR “fetal” OR “foetal” OR “fetus” OR “foetus” OR “maternity” OR “pregnan*” OR “pseudopregnan*” OR “gravidit*” OR “nulligravid*” OR “primigravid*” OR “multigravid*” OR “gravidation” OR “gravidarum” OR “gravida” OR “parturition*” OR “parity” OR “childbirth*” OR “birthing” OR “birth” OR “stillbirth” OR “childbed” OR (“abdominal” AND “deliver*”) OR “gestation*” OR “parturien*” OR “child-bear*” OR “childbear*” OR “placentat*” OR “prepregnan*” OR “conception*” OR “preconception*” OR “obstetric*” OR “prenatal” OR “perinatal” OR “intranatal” OR “antenatal” OR “prepartum” OR “peripartum” OR “intrapartum” OR “antepartum” OR “pre-natal” OR “peri-natal” OR “intra-natal” OR “ante-natal” OR “pre-partum” OR “peri-partum” OR “intra-partum” OR “ante-partum”) OR AUTHKEY (“maternal” OR “mother*” OR “fetal” OR “foetal” OR “fetus” OR “foetus” OR “maternity” OR “pregnan*” OR “pseudopregnan*” OR “gravidit*” OR “nulligravid*” OR “primigravid*” OR “multigravid*” OR “gravidation” OR “gravidarum” OR “gravida” OR “parturition*” OR “parity” OR “childbirth*” OR “birthing” OR “birth” OR “stillbirth” OR “childbed” OR (“abdominal” AND “deliver*”) OR “gestation*” OR “parturien*” OR “child-bear*” OR “childbear*” OR “placentat*” OR “prepregnan*” OR “conception*” OR “preconception*” OR “obstetric*” OR “prenatal” OR “perinatal” OR “intranatal” OR “antenatal” OR “prepartum” OR “peripartum” OR “intrapartum” OR “antepartum” OR “pre-natal” OR “peri-natal” OR “intra-natal” OR “ante-natal” OR “pre-partum” OR “peri-partum” OR “intra-partum” OR “ante-partum”) | 1,957,453 |
| #1 | TITLE-ABS (“cicatr*” OR “keloid*” OR “scar” OR “scars” OR “scarring” OR “contractur*”) OR AUTHKEY (“cicatr*” OR “keloid*” OR “scar” OR “scars” OR “scarring” OR “contractur*”) | 141,659 |


References
- Pereira, C.; Murphy, K.; Herndon, D. Outcome measures in burn care. Is mortality dead? Burns 2004, 30, 761–771. [Google Scholar] [CrossRef]
- Tompkins, R.G. Survival from burns in the new millennium: 70 years’ experience from a single institution. Ann. Surg. 2015, 261, 263–268. [Google Scholar] [CrossRef]
- Strassle, P.D.; Williams, F.N.; Napravnik, S.; van Duin, D.; Weber, D.J.; Charles, A.; Cairns, B.A.; Jones, S.W. Improved Survival of Patients with Extensive Burns: Trends in Patient Characteristics and Mortality among Burn Patients in a Tertiary Care Burn Facility, 2004–2013. J. Burn. Care Res. 2017, 38, 187–193. [Google Scholar] [CrossRef]
- Tsoutsos, D.; Rodopoulou, S.; Keramidas, E.; Lagios, M.; Stamatopoulos, K.; Ioannovich, J. Early escharotomy as a measure to reduce intraabdominal hypertension in full-thickness burns of the thoraciand abdominal area. World J. Surg. 2003, 27, 1323–1328. [Google Scholar] [CrossRef] [PubMed]
- Panicker, V.V.; Riyaz, N.; Balachandran, P.K. A clinical study of cutaneous changes in pregnancy. J. Epidemiol. Glob. Health 2017, 7, 63–70. [Google Scholar] [CrossRef]
- Kitzmiller, W.J.; Neale, H.W.; Warden, G.D.; Smith, D. The effect of full-thickness abdominal wall burns sustained during childhood on subsequent childbearing ability. Ann. Plast. Surg. 1998, 40, 111–113. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-D.; Hwang, S.-M.; Lim, K.-R.; Jung, Y.-H.; Ahn, S.-M.; Song, J.K. Recurrent auricular keloids during pregnancy. Arch. Plast. Surg. 2013, 40, 70–72. [Google Scholar] [CrossRef] [PubMed]
- Moustafa, M.F.; Abdel-Fattah, M.A.; Abdel-Fattah, D.C. Presumptive evidence of the effect of pregnancy estrogens on keloid growth: Case report. Plast. Reconstr. Surg. 1975, 56, 450–453. [Google Scholar] [CrossRef]
- Bayat, A.; Arscott, G.; Ollier, W.; Mc Grouther, D.; Ferguson, M. Keloid disease: Clinical relevance of single versus multiple site scars. Br. J. Plast. Surg. 2005, 58, 28–37. [Google Scholar] [CrossRef]
- Ibrahim, N.E.; Shaharan, S.; Dheansa, B. Adverse Effects of Pregnancy on Keloids and Hypertrophic Scars. Cureus 2020, 12, e12154. [Google Scholar] [CrossRef] [PubMed]
- NIHR. International prospective register of systematic reviews. Available online: https://www.crd.york.ac.uk/prospero/ (accessed on 22 May 2020).
- PRISMA. Transparent reporting of systematic reviews and meta-analysis. Available online: www.prisma-statement.org (accessed on 20 May 2020).
- Dijkerman, M.L.; Breederveld-Walters, M.L.; Pijpe, A.; Breederveld, R.S. Management and outcome of burn injuries during pregnancy: A systematic review and presentation of a comprehensive guideline. Burns 2022, 48, 1544–1560. [Google Scholar] [CrossRef]
- Chambers, D.; Rodgers, M.; Woolacott, N. Methods of systematic reviews and meta–analysis not only randomized controlled trials, but also case series should be considered in systematic reviews of rapidly developing technologies. J. Clin. Epidemiol. 2009, 62, 1253–1260.e4. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 17 August 2020).
- Rai, Y.; Jackson, D.M. Child-bearing in relation to the scarred abdominal wall from burns. Burns 1975, 1, 167–171. [Google Scholar] [CrossRef]
- Daw, E.; Mohandas, I. Pregnancy in patients after severe abdominal burns. Br. J. Obstet. Gynaecol. 1983, 90, 69–72. [Google Scholar] [CrossRef] [PubMed]
- Widgerow, A.; Ford, T.D.; Botha, M. Burn contracture preventing uterine expansion. Ann. Plast. Surg. 1991, 27, 269–271. [Google Scholar] [CrossRef] [PubMed]
- Haeseker, B.; Green, M.F. A complication in pregnancy due to severe burns in childhood. Br. J. Plast. Surg. 1981, 34, 102–104. [Google Scholar] [CrossRef]
- Matthews, R.N. Old burns and pregnancy. Br. J. Obstet. Gynaecol. 1982, 89, 610–611. [Google Scholar] [CrossRef] [PubMed]
- Webb, J.C.; Baack, B.R.; Osler, T.M.; Davis, V.H.; Izquierdo, L.A.; Binur, N. A pregnancy complicated by mature abdominal burn scarring and its surgical solution: A case report. J. Burn. Care Rehabil. 1995, 16 Pt 1, 276–279. [Google Scholar] [CrossRef]
- Takeda, K.; Sowa, Y.; Numajiri, T.; Nishino, K. Expansion abdominoplasty for a pregnant woman with severe abdominal wall contracture due to a major burn during childhood: A case report. Ann. Plast. Surg. 2013, 70, 643–646. [Google Scholar] [CrossRef]
- Mitsukawa, N.; Saiga, A.; Satoh, K. Protocol of surgical indications for scar contracture release before childbirth: Women with severe abdominal scars after burn injuries. J. Plast. Surg. Hand Surg. 2015, 49, 32–35. [Google Scholar] [CrossRef]
- Kakagia, D.; Kyriopoulos, E.; Zapandioti, P.; Tsoutsos, D. Natural expansion of artificial dermal template by successful full-term pregnancy. J. Burn. Care Res. 2012, 33, e166-8. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.A.; Dainer, M.; Shumaker, P.R. Ablative fractional laser resurfacing for abdominal scar contractures in pregnancy. Obstet. Gynecol. 2015, 125, 924–926. [Google Scholar] [CrossRef] [PubMed]
- McCauley, R.L.; Stenberg, B.A.; Phillips, L.G.; Blackwell, S.J.; Robson, M.C. Long-term assessment of the effects of circumferential truncal burns in pediatric patients on subsequent pregnancies. J. Burn. Care Rehabil. 1991, 12, 51–53. [Google Scholar] [CrossRef]
- Fioretti, P.; Weiss, C.; Cilotti, A.; Strigini, F.; Melis, G.B. Old abdominal burns and caesarean section. Case report. Br. J. Obstet. Gynaecol. 1987, 94, 596–597. [Google Scholar] [CrossRef] [PubMed]
- Aykan, A.; Ozturk, S.; Dede, M.; Keskin, U. Constricting wide abdominal burn scar and pregnancy. Eur. J. Plast. Surg. 2013, 36, 463–466. [Google Scholar] [CrossRef]
- Ozog, S.A. COURSE OF PREGNANCY IN WOMEN WITH MARKED SCARRING OF ENTIRE TORSO. J. Am. Osteopath. Assoc. 1963, 63, 235–237. [Google Scholar]
- Pant, R.; Manandhar, V.; Wittgenstein, F.; Fortney, J.; Fukushima, C. Genital burns and vaginal delivery. Int. J. Gynaecol. Obstet. 1995, 50, 61–63. [Google Scholar] [CrossRef]
- Vathulya, M.; Joshi, M. A pregnant patient with fetal distress with severe post burn contracture of anterior trunk and perineum: A surgeon’s nightmare! Indian J. Plast. Surg. 2014, 47, 456–459. [Google Scholar] [CrossRef]
- Rajagopalan, S.; Ortiz, J.; Chandrasekhar, S. Anesthetic management of a pregnant patient with significant post-burn scars and contractures. Glob. Anesth. Perioper. Med. 2015, 1, 17–18. [Google Scholar]
- Duke, J.; Wood, F.; Semmens, J.; Edgar, D.W.; Rea, S. Long-term follow-up of the impacts on obstetric complications of trunk burn injuries sustained during childhood. J. Burn. Care Res. 2012, 33, 654–659. [Google Scholar] [CrossRef]
- Arabi, Z.; Monoto, E.M.; Bojeng, A. Impact of childhood burn injuries on breastfeeding: A case report. Int. Breastfeed. J. 2019, 14, 17. [Google Scholar] [CrossRef]
- Duke, J.; Wood, F.; Semmens, J.; Edgar, D.W.; Rea, S. Pregnancy as a tissue expander in the correction of a scar deformity. Am. J. Obstet. Gynecol. 2004, 190, 579–580. [Google Scholar]
- Digregorio, V.R. Two Unusual Postburn Reconstructions Using Tissue Expansion: One Exogenous and One Endogenous. Ann. Plast. Surg. 1993, 30, 549–551. [Google Scholar] [CrossRef]
- Pingel, J.; Langberg, H.; Skovgård, D.; Koskinen, S.; Flyvbjerg, A.; Frystyk, J.; Kjær, M.; Hansen, M.; Kjaer, M. Effects of transdermal estrogen on collagen turnover at rest and in response to exercise in postmenopausal women. Am. Physiol. Soc. 2012, 113, 1040–1047. [Google Scholar] [CrossRef] [PubMed]
- Elwood, E.T.; Ingram, W.L.; Carlson, G.W. Pregnancy as a Tissue Expander in the Repair of a Massive Ventral Hernia. Ann. Plast. Surg. 2000, 45, 431–433. [Google Scholar] [CrossRef] [PubMed]
| Study | Study Design | Country | Study Time Period | Patients (n) | Pregnancies n | Outcome Measures ¥ | Data Source | Risk of Bias |
|---|---|---|---|---|---|---|---|---|
| Duke (2012) | Cohort (retrospective) | Australia | 1983–2008 | 134 | 213 | Abdominal, other | MNS * database | Good |
| Rai (1975) | Case series (retrospective) | UK | 1948–1967 | 21 | 42 | Abdominal, other | Burns Unit | Poor |
| Kitzmiller (1998) | Case series (retrospective) | USA | 1975–1989 | 19 | 31 | Abdominal, other | Burns Unit | Poor |
| Mitsukawa (2015) | Case series (prospective) | Japan | 2000–2015 | 12 | - | Abdominal, other | Department of PS ^ | Poor |
| McCauley (1990) | Case series (retrospective) | USA | 1967–1985 | 7 | 14 | Abdominal, other | Burns Institute | Poor |
| Daw (1983) | Case series (retrospective) | UK | 1976–1981 | 6 | 11 | Abdominal, other | Department of Gynaecology | Poor |
| Matthews (1982) | Review based on personal communication | UK | Unknown | 2 | 2 | Abdominal | Centre for Burns and PS | Poor |
| Widgerow (1991) | Case report | South Africa | 1990 | 2 | 2 | Abdominal | Department of PS | Poor |
| Arabi (2019) | Case report | Malaysia | 2015 | 1 | 1 | Other | Health Clinic | Poor |
| Aykan (2012) | Case report | Turkey | 2012 | 1 | 1 | Abdominal, other | Department of PS | Poor |
| Cox (2015) | Case report | USA | 2015 | 1 | 1 | Abdominal, other | Department of dermatology | Poor |
| Del Frari (2004) | Case report | Austria | Unknown | 1 | 1 | Natural tissue expansion | Department of PS | Poor |
| Digregorio (1993) | Case report | USA | Unknown | 1 | 1 | Natural expansion | Department of PS | Poor |
| Fioretti (1987) | Case report | Italy | Unknown | 1 | 1 | Abdominal, other | Department of Gynaecology | Poor |
| Haeseker (1981) | Case report | Wales | Unknown | 1 | 1 | Abdominal, foetal | Centre of PS | Poor |
| Kakagia (2012) | Case report | Greece | Unknown | 1 | 1 | Abdominal | Department of PS | Poor |
| Ozog (1963) | Case report | USA | 1962 | 1 | 2 | Abdominal, foetal | Hospital | Poor |
| Pant (1995) | Case report | Nepal | Unknown | 1 | 1 | Foetal, other | Hospital | Poor |
| Rajagopalan (2015) | Case report | USA | Unknown | 1 | 1 | Foetal, other | Department of Anaesthesiology | Poor |
| Takeda (2013) | Case report | Japan | Unknown | 1 | 1 | Abdominal, other | Department of PS | Poor |
| Vathulya (2014) | Case report | India | Unknown | 1 | 1 | Foetal, other | Department of PS | Poor |
| Webb (1995) | Case report | Mexico | Unknown | 1 | 1 | Abdominal, other | Regional Burn Centre | Poor |
| Study | Age at Burn, Yr | Age at First Pregnancy, Yr | Burn Characteristics | Duration of Pregnancy * |
|---|---|---|---|---|
| Duke (2012) | Mean 5.7 | Mean 20.9 | 131 patients <10% BSA 3 patients = 10–19% BSA | All: full term |
| Rai (1975) | Childhood | >15 yr or <45 yr | Full thickness: >4% of the abdomen | 35: full term; 2: premature labour; 3: abortion; (2: during pregnancy) |
| Kitzmiller (1998) | Mean 7.6 | ^ | Mean 55% BSA Full thickness: mean 42% | All: full term |
| Mitsukawa (2015) | ^ | ^ | Mean 64% BSA of the abdomen | ^ |
| McCauley (1990) | Mean 7.66 | Mean 19.83 | Mean 63.21% BSA Full thickness: mean 44.2% | All: full term |
| Daw (1983) | Mean 6.25 | Mean 20.5 | Around abdomen | 3: full term; 6: induction labour around full term; 2: premature labour |
| Matthews (1982) | ^ | ^ | Circumferential lower abdomen | ^ |
| Widgerow (1991) | Case 1: 9 Case 2: childhood | Case 1: 19 Case 2: 21 | Circumferential abdomen | Both: full term |
| Arabi (2019) | 5 | 20 | Chest, abdomen, upper limb, and part of her trunk | Full term |
| Aykan (2012) | 4 | 29 | Full thickness of genital region, bilateral lumber areas, lower two thirds of the abdominal wall | Full term |
| Cox (2015) | 2 | 31 | 2nd and 3rd degree burns on breasts, abdomen, thighs, lower back | Full term |
| Del Frari (2004) | 14 | 24 | Right lower abdomen, groin area, and thigh | ^ (after 8 months) |
| Digregorio (1993) | 27 | 34 | 50% BSA third degree burns on face, hands, chest, and abdomen | Full term |
| Fioretti (1987) | 4 | 24 | From lower abdomen to thigh | Full term |
| Haeseker (1981) | 4 | 21 | Full thickness: 60% | Premature labour 3 days after operation |
| Kakagia (2012) | 3 | 30 | Postburn scars torso (anterior + lateral abdominal + chest wall, gluteal areas, breasts) | ^ |
| Ozog (1963) | Childhood | 19 | From chest to midthigh | 1st pregnancy: 5 months; 2nd pregnancy: premature |
| Pant (1995) | 5 | 17 | Most of the perineum | ^ |
| Rajagopalan (2015) | 6 | 38 | >90% BSA on chest, neck, face, abdomen, elbows, knees | 27 weeks |
| Takeda (2013) | 6 | 23 | BSA: 80% Full thickness: 65% | 36 weeks |
| Vathulya (2014) | 6 | 22 | Chest region to abdomen + perineal region with supra-clitoral hooding deformity; left breast nipple-areolar complex | Third trimester |
| Webb (1995) | 3 | 23 | Full thickness: mean 40% | Full term |
| Study | Complication | Follow Up | Outcome | Notes |
|---|---|---|---|---|
| Duke (2012) | No admissions during pregnancy for scar complications, revisions of scars or contractures; 2 times hypertrophic/ keloid scar was recorded | - | No long-term detrimental effects of burns on pregnancy, delivery or to the foetus | The majority of trunk burns were burns of partial thickness or unspecified depth |
| Rai (1975) | 2 itch, 7 tightness, 6 both | Unknown | Unknown | Three patients said the scars improved after pregnancy and in subsequent pregnancies |
| Kitzmiller (1998) | Minor scar breakdown in third trimester 25% instance of subjective sensation of abdominal tightness | Local care No narcotics necessary | Healed rapidly after delivery | |
| McCauley (1990) | Breakdown of abdominal scar tissue in 3rd trimester | Unknown | Unknown | |
| Daw (1983) | Tautness with a hot burning sensation to constant indescribable pain | Admitted to hospital, bed rest, inactivity, analgesics, surgical decompression (36 weeks) | Induction of labour in 6 of 11 pregnancies, premature labour | |
| Matthews (1982) | Maternal pain | Surgical intervention during 3rd trimester | Immediate pain relief | |
| Widgerow (1991) | Tightness, contracture limited progress of pregnancy | Surgical release (16 weeks/4 months) | Normal expansion of the uterus | |
| Aykan (2012) | Scar related hot burning sensation in 3rd trimester | Unknown | Unknown | Shortly after the operation, abdominal scar tissue tension-related symptoms and hot burning sensation decreased. |
| Cox (2015) | Intermittent ich and mild restriction with inactivity | Ablative functional laser (30 and 38 weeks) | Immediate postprocedure relief of tension, increased mobility, and improved respiration | Comfort and functionality were improved compared with prepregnancy; scar contour and pliability had improved |
| Fioretti (1987) | Mild dyspnoea | Had to reduce housework | Unknown | |
| Haeseker (1981) | Tightness and pain; potential obstruction for growing uterus | Surgical scar release (24 weeks) | Decompression→ premature labour→ foetus died | |
| Ozog (1963) | backache, nausea, anorexia, vomiting, dyspepsia, and severe constipation due to direct pressure | Re-examined each month and drug treatment | Refractory to drug treatment | |
| Takeda (2013) | Abdominal pain | Expansion abdominoplasty (20 weeks) | Abdominal wall expansion and foetal growth were found to be favourable | |
| Webb (1995 | Pain and a localised area of skin breakdown | Close monitoring | 38 weeks: pre-eclampsia→ CS | Taking advantage of the natural skin expansion of pregnancy |
| Study | Complication | Cause | Direct/Indirect Cause on Complication | Outcome | Likelihood of Relation to Burns |
|---|---|---|---|---|---|
| Haeseker (1981) | Premature labour | Surgical release→ decompression effect | Indirect | Dead due to prematurity | Likely/certain |
| Ozog (1963) | Pressure deformity of the skull→ right side of the face flat appearance + bilateral clubfoot deformity | Little room for rotation and movement | Direct | Temporary deformities | Likely |
| Pant (1995) | Non progressive labour (22hours in labour) | Scar tissue on perineum→ oedematous vulva with the foetal scalp visible | Direct | Dead | Likely/certain |
| Rajagopalan (2015) | Repeated foetal decelerations and non-reactive tracings | Unknown (preeclampsia, elevated aminotransferase, hyperglycaemia?) (placental insufficiency?) | Unknown | Emergency caesarean | Possible |
| Vathulya (2014) | Absent foetal heart sounds, meconium stained liquor, nonprogressive labour | Unknown | Unknown | Emergency caesarean | Possible |
| Study | Mode of Delivery | Potential Explanation | Notes |
|---|---|---|---|
| Duke (2012) | 142: NVD *; 26: instrument; 45: CS ^ | Unknown | No statistically significant differences between subjects who had sustained a burn to the trunk and those with burns to other sites of the body or erythema burns to trunk |
| Rai (1975) | 31: NVD; 4: forceps; 2: CS | Scarred abdominal wall was not responsible/Any lack of expulsive force not total excluded: an objective study by measurements of intraabdominal pressure changes and abdominal wall extensibility in relation to cervical dilatation is made | One of the forceps deliveries contained twins. Three abortions |
| Kitzmiller (1998) | 28: NVD; 3: CS | Failure of labour due to cephalopelvic disproportion | Abdominal wall healing after CS was not complicated |
| Mitsukawa (2015) | 2: NVD; 9: CS; 1: Not pregnant yet | If patients have scars covering 75% or more of the total abdominal area, scar release surgery is always performed. In addition, an open leg position is necessary. | |
| McCauley (1990) | 13: NVD; 1: CS | Unknown | 1 elective caesarean section |
| Daw (1983) | All: NVD | Abdominal pain from tightness | In 6 of 11 pregnancies necessitated |
| Aykan (2012) | CS | perineal scar tissue was dense and preventing vaginal delivery | classical Pfannenstiel incision was preferred |
| Cox (2015) | CS | Non progressive labour | 6 months after delivery she reported negligible tension and itch in the scarred areas |
| Fioretti (1987) | CS | the uterus could only expand transversely, foetal lie was transverse at term | Elective caesarean section |
| Ozog (1963) | 1st: stillborn, twins; 2nd: forceps | Unknown | 1 month premature |
| Pant (1995) | Incision anterior to the anus up to symphysis in the midline | Scar tissue covered most of the perineum | An incision was made anterior to the anus up to the symphysis pubis in the midline to separate the vulva obstruction. |
| Rajagopalan (2015) | CS | Foetal distress | Emergency caesarean section |
| Takeda (2013) | CS | Perineal scar contractures resulted in rigidity of the soft birth canal and limited hip joint flexion | Elective caesarean section |
| Vathulya (2014) | CS | Foetal distress and supra-clitoral hooding deformity: the clitoris, and the labia anterior 2/3 were almost invisible | Emergency caesarean section |
| Webb (1995) | CS | Preeclampsia and transverse lie | Caesarean section |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Gelder, Z.J.; Snoeks, A.; van Zuijlen, P.P.M.; de Vries, R.; Pijpe, A. Complications during Pregnancy after Abdominal Burn Scars: A Review. Eur. Burn J. 2023, 4, 35-54. https://doi.org/10.3390/ebj4010005
van Gelder ZJ, Snoeks A, van Zuijlen PPM, de Vries R, Pijpe A. Complications during Pregnancy after Abdominal Burn Scars: A Review. European Burn Journal. 2023; 4(1):35-54. https://doi.org/10.3390/ebj4010005
Chicago/Turabian Stylevan Gelder, Zosha J., Annabel Snoeks, Paul P.M. van Zuijlen, Ralph de Vries, and Anouk Pijpe. 2023. "Complications during Pregnancy after Abdominal Burn Scars: A Review" European Burn Journal 4, no. 1: 35-54. https://doi.org/10.3390/ebj4010005
APA Stylevan Gelder, Z. J., Snoeks, A., van Zuijlen, P. P. M., de Vries, R., & Pijpe, A. (2023). Complications during Pregnancy after Abdominal Burn Scars: A Review. European Burn Journal, 4(1), 35-54. https://doi.org/10.3390/ebj4010005