

Diphoterine for Chemical Burns of the Skin: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources
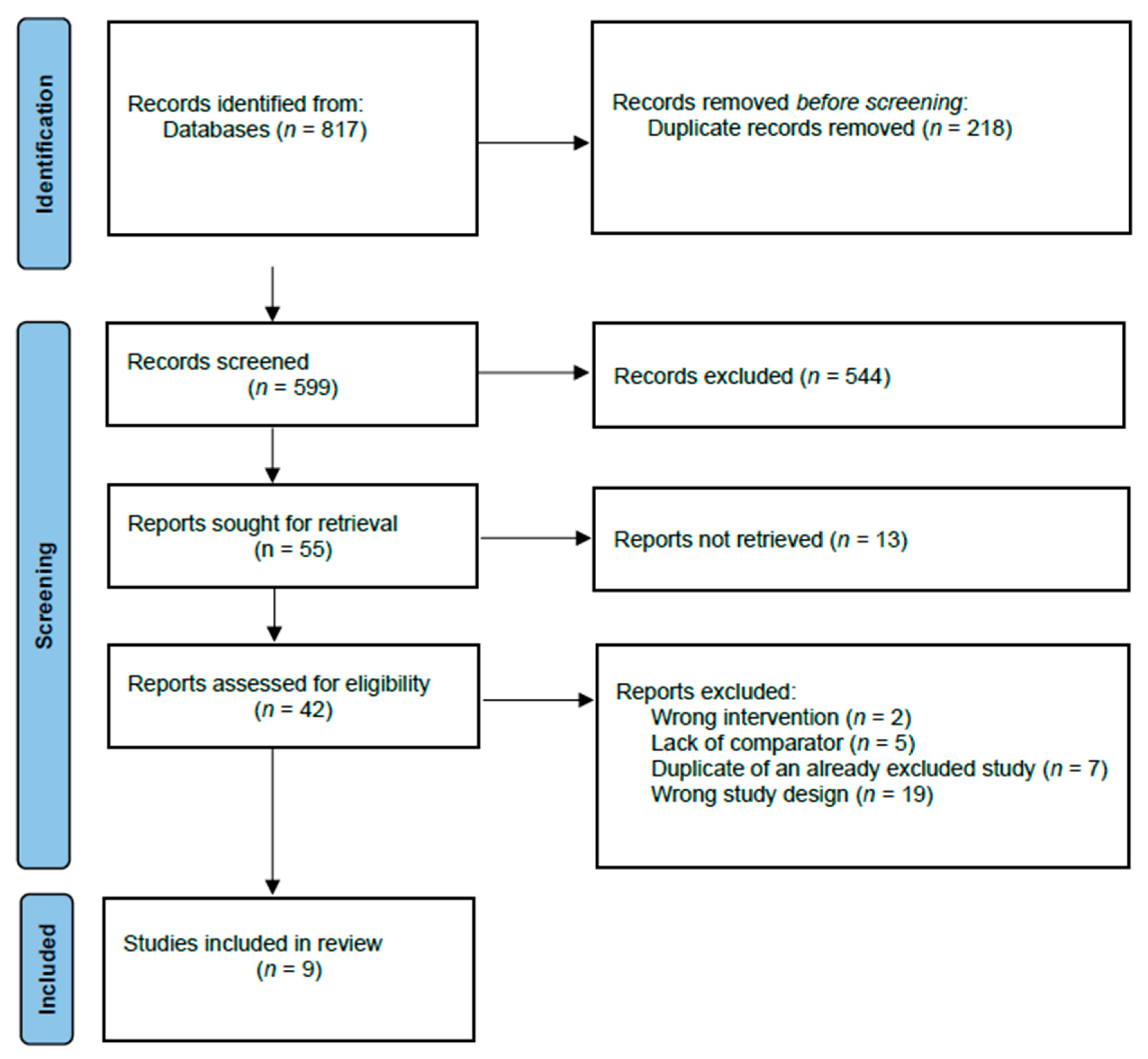
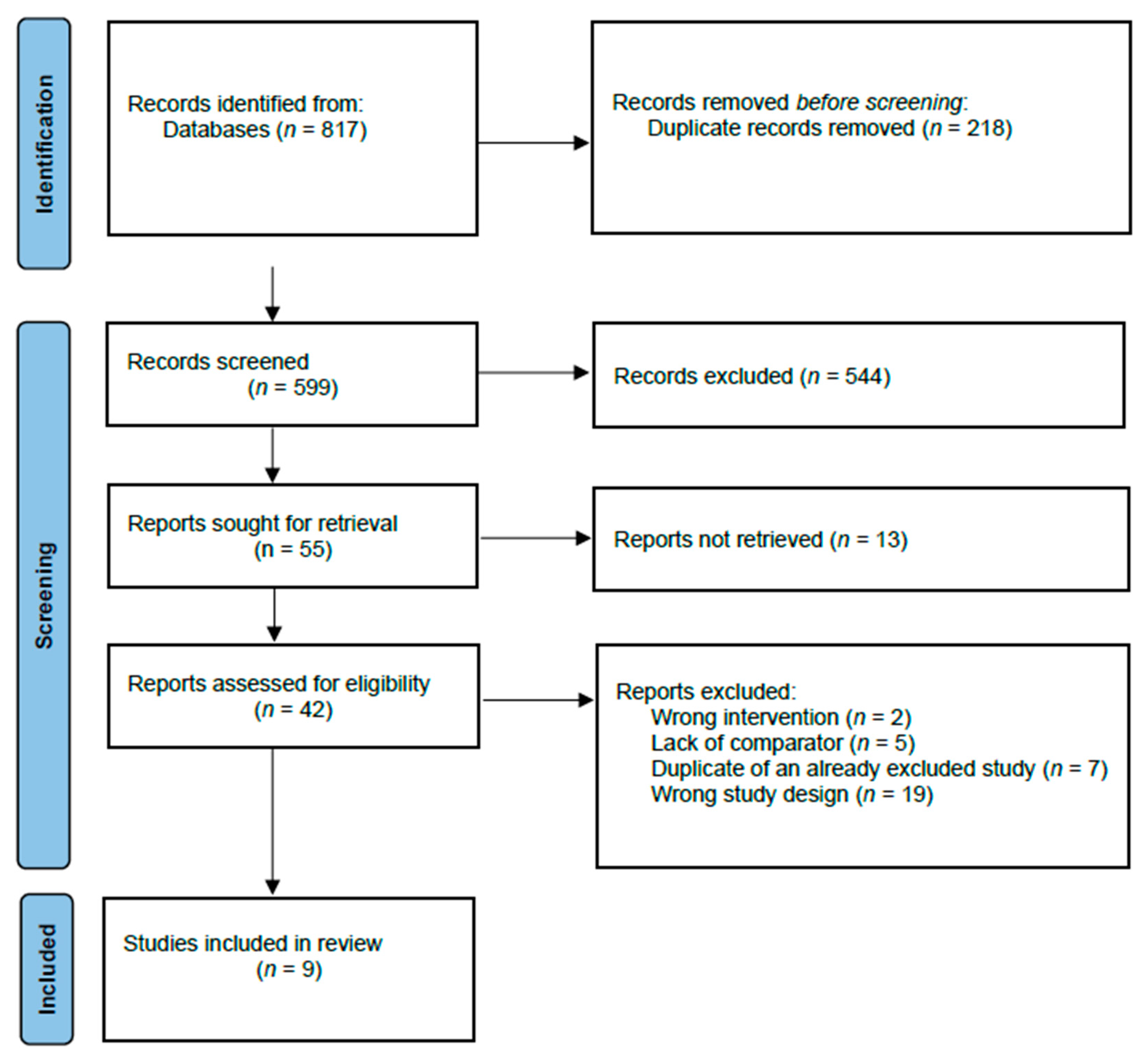
2.3. Study Selection
2.4. Data Collection Process and Data Items
2.5. Risk of Bias Assessment
2.6. Synthesis Methods
2.7. Certainty Assessment
3. Results
GRADE Assessment

{kind=link}
| Outcome | Study | Measurement Scale | Diphoterine | Control | Between Group Estimate |
|---|---|---|---|---|---|
| Depth of chemical burn | Huang, 2020 [12] | Burn degree | 25% TMAH *, 5% BSA †: - one case with first- to second-degree burn 25% TMAH, ≤1% BSA: - two cases with first-degree burn 2.38% TMAH, <1% BSA: - one case with first-degree burn 20% diluted TMAH, 1% BSA: - one case with first-degree burn | 25% TMAH, 2% BSA: - one case with second-degree burn 25%TMAH, ≤1% BSA: - two cases with first-degree burn 2.38% TMAH, ≤1% BSA: - five cases with first-degree burn, three cases with no burn 2.38% TMAH, ≤2% BSA: - one case with first-degree burn one case with no burn 2.38% TMAH, BSA N/A (forearm): - one/case with first-degree burn 0.50% TMAH, BSA “Nearly entire body”: - two cases with no burn TMAH N/A, ≤1% BSA: - five cases with first-degree burn one case with no burn 3% TMAH, BSA N/A (both forearms): - one case with no burn 1–3% TMAH, <1% BSA: - one case with first-degree burn | |
| Pain | Brvar, 2016 [13] | NRS 0–10, mean (95% CI) | Postexposure: Inside CS ¤ cloud: 9.1 (9.1–9.1) Residual pain at checkpoint 1.4 (1.3–1.4) | Inside CS cloud 9.7 (9.7–9.7) Residual pain at checkpoint 2.3 (2.3–2.3) | |
| Škarja, 2014 [15] | NRS 0–10, mean (SE) | 55 s: 11 had pain, NRS = 1.7 (±0.6) 2 min: one had pain, NRS = 1. Afterwards, no one had pain. | Water group: 55 s: 11 had pain, NRS = 2.3 (±0.9). 2 min: three had pain, NRS = 1.3 (±0.6). Afterwards, no one had pain. No treatment group: 55 s: eight had pain, NRS = 2.1 (±1.0). 2 min: seven had pain, NRS = 2.3 (±1.0). 3 min: seven had pain, NRS = 2.0 (±1.2). 15 min: six had pain, NRS = 1.8 (±0.8). 60 min: five had pain, NRS = 1.2 (±0.4). 120 min: one had pain, NRS = 1. Afterwards, no one had pain | Between water group and diphoterine group at 2 min: p = 0.32 | |
| Kulkarni, 2018 [8] | VAS 0–10, mean | Before irrigation VAS = 7.0 After irrigation VAS = 3.1 Reduction: 3.9 | Before irrigation VAS = 5.7 After irrigation VAS = 4.1 Reduction: 1.6 | p < 0.001 | |
| Nogue, 2012 [14] | Descriptive | Three cases with “Rapid improvement of local symptoms” One case with “No effect on local symptoms” | Three cases with “Local symptoms better” Two cases with “No effect on local symptoms” | ||
| Duration of hospitalization | Zack-Williams, 2015 [16] | Days, median | 1.75 days | 1.58 days | p = 0.80 |
| Time to return to work | Brvar, 2016 [13] | Min:sec (95% CI) | Preexposure: 1:26 (1:24–1:28) Postexposure: 2:30 (2:26–2:34) | CS only: 2:28 (2:26–2:30) | |
| Kulkarni, 2018 [8] | Days (mean) | 2–7 days (4.67) | 3–20.2 days (16.75) | p = 0.14 | |
| Donoghue, 2010 [17] | Days | 1 restricted workday case 0 lost workday cases | 0 restricted workday cases. 0 lost workday cases | ||
| Need for surgery | - | - | - | - | - |
| pH | Zack-Williams, 2015 [16] | pH, mean | Pre-irrigation pH = 8.07 pH change after treatment = 1.076 | Pre-irrigation pH = 7.77 pH change after treatment = 0.4 | p < 0.05/p = 0.000 |
| Cavallini, 2010 [18] | pH, mean | pH before treatment = 4.88 pH after glycolic acid = 0.7 pH after correction = 4.03 pH increase = 3.33 | pH before treatment = 4.88 pH after glycolic acid = 0.7 pH after correction = 3.4 pH increase = 2.7 | Increase, mean p < 0.001 | |
| Complications | Nogue, 2012 [14] | No ARs § | No ARs | ||
| Nehles, 2006 [19] | No adverse effects | No adverse effects |
| Risk of Bias in Randomized Trials, Using the Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomized Trials | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Randomization Process | Deviations from the Intended Interventions | Missing Outcome Data | Measurement of the Outcome | Selection of the Reported Result | Overall Risk-of-Bias Judgement | |||||
| Bvrar, 2016 [13] | High risk | Some concerns | Low risk | High risk | Some concerns | High risk of bias | ||||
| Škarja, 2014 [15] | Some concerns | Some concerns | Low risk | Low risk | Some concerns | Some concerns | ||||
| Risk of bias in non-randomized studies, using the Newcastle Ottawa Scale | ||||||||||
| Selection (maximum of four) | Comparability (maximum of two) | Outcome (maximum of three) | Total | |||||||
| Cavallini, 2010 [18] | ★★ | ★★ | ★★ | 6 | ||||||
| Donoghue, 2010 [17] | ★★ | - | ★ | 3 | ||||||
| Huang, 2020 [12] | ★★★ | ★ | ★★ | 6 | ||||||
| Kulkarni, 2018 [8] | ★★ | ★ | ★ | 4 | ||||||
| Nehles, 2006 [19] | ★ | ★ | ★ | 3 | ||||||
| Nogue, 2012 [14] | ★★★ | - | ★★ | 5 | ||||||
| Zack-Williams, 2015 [16] | ★★★ | - | ★ | 4 | ||||||
| Certainty Assessment | No. of Patients | Effect | Certainty | Importance | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | Diphoterine | Water or No Treatment | Relative (95% CI) | Absolute (95% CI) | ||
| Depth of chemical burn | ||||||||||||
| 1 | Observational study | Serious a | Serious b | Serious c | 4 | 11 | - | - |  VERY LOW | CRITICAL | ||
| Pain | ||||||||||||
| 4 | Randomized trials and observational studies | Serious d | Not serious | Serious e | 34 | 89 | - | - |  VERY LOW | CRITICAL | ||
| Duration of hospitalization | ||||||||||||
| 1 | Observational study | Serious f | Not serious | Serious g | 47 | 84 | - | - |  VERY LOW | IMPORTANT | ||
| Time to return to work | ||||||||||||
| 3 | Randomised trial and observational studies | Serious h | Not serious | Serious i | 143 | 202 | - | - |  VERY LOW | IMPORTANT | ||
| pH | ||||||||||||
| 2 | Controlled trial and observational study | Not serious f | Not serious | Serious g | 72 | 109 | - | - |  VERY LOW | IMPORTANT | ||
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Hardwicke, J.; Hunter, T.; Staruch, R.; Moiemen, N. Chemical burns—An historical comparison and review of the literature. Burns 2012, 38, 83–87. [Google Scholar] [CrossRef] [PubMed]
- American Burn Association. Burn Incidence Fact Sheet. 2016. Available online: http://ameriburn.org/who-we-are/media/burn-incidence-fact-sheet/ (accessed on 10 March 2021).
- Akelma, H.; Karahan, Z.A. Rare chemical burns: Review of the Literature. Int. Wound J. 2019, 16, 1330–1338. [Google Scholar] [CrossRef] [PubMed]
- Kozawa, S.; Kakizaki, E.; Muraoka, E.; Koketsu, H.; Setoyama, M.; Yukawa, N. An autopsy case of chemical burns by hydrochloric acid. Legal Med. 2009, 11, 535–537. [Google Scholar] [CrossRef] [PubMed]
- Cartotto, R.C.; Peters, W.J.; Neligan, P.C.; Douglas, L.G.; Beeston, J. Chemical burns. Can. J. Surg. 1996, 39, 205. [Google Scholar] [PubMed]
- Hall, A.H.; Maibach, H.I. Water decontamination of chemical skin/eye splashes: A critical review. Cutan. Ocul. Toxicol. 2006, 25, 67–83. [Google Scholar] [CrossRef] [PubMed]
- Alexander, K.S.; Wasiak, J.; Cleland, H. Chemical burns: Diphoterine untangled. Burns 2018, 44, 752–766. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, P.; Jeffery, S. The effects of the use of Diphoterine® solution on chemical burns in the Tarapur industrial complex, India. Burns Open 2018, 2, 104–107. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, 2535. [Google Scholar] [CrossRef] [PubMed]
- Center for Reviews and Dissemination, University of York. PROSPERO: International Prospective Register of Systematic Reviews. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=243156 (accessed on 9 May 2021).
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Huang, C.-K.; Hall, A.-H.; Wu, M.-L.; Yang, C.-C.; Hung, D.-Z.; Mao, Y.-C.; Deng, J.-F. Presentations of tetramethylammonium hydroxide dermal exposure and the valuable potential of diphoterine solution in decontamination: A retrospective observational study. BMC Pharmacol. Toxicol. 2020, 21, 83. [Google Scholar] [CrossRef] [PubMed]
- Brvar, M. Chlorobenzylidene malononitrile tear gas exposure: Rinsing with amphoteric, hypertonic, and chelating solution. Hum. Exp. Toxicol. 2016, 35, 213–218. [Google Scholar] [CrossRef]
- Nogué, S.; Amigo, M.; Uria, E.; Fernandez, F.; Velasco, V. Chemical decontamination in the emergency. Emergencias 2012, 24, 3–7. [Google Scholar]
- Škarja, T. Rinsing with Water and Amphoteric, Hypertonic and Chelating Solution after Sodium Hydroxide Splash [Izpiranje kože z vodo in amfoterno, hipertonično in kelatno raztopino po politju z natrijevim hidroksidom]. Master’s Thesis, Univerza v Ljubljani, Zdravstvena Fakulteta, Ljubljana, Slovenia, 2014. [Google Scholar]
- Zack-Williams, S.D.L.; Ahmad, Z.; Moiemen, N.S. The clinical efficacy of Diphoterine® in the management of cutaneous chemical burns: A 2-year evaluation study. Ann. Burn. Fire Disasters 2015, 28, 9–12. [Google Scholar]
- Donoghue, A.M. Diphoterine for alkali chemical splashes to the skin at alumina refineries. Int. J. Dermatol. 2010, 49, 894–900. [Google Scholar] [CrossRef] [PubMed]
- Cavallini, M.; Puggioni, V.; Gazzola, R. Evaluation of cutaneous pH after chemical peel and its correction with amphoteric solutions. J. Plast Dermatol. 2010, 6, 145–147. [Google Scholar]
- Nehles, J.; Hall, A.H.; Blomet, J.; Mathieu, L. Diphoterine for emergent decontamination of skin/eye chemical splashes: 24 cases. Cutan. Ocul. Toxicol. 2006, 25, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Lewis, C.J.; Al-Mousawi, A.; Jha, A.; Allison, K.P. Is it time for a change in the approach to chemical burns? The role of Diphoterine® in the management of cutaneous and ocular chemical injuries. J. Plast Reconstr. Aesthet. Surg. 2017, 70, 563–567. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.H.; Cavallini, M.; Mathieu, L.; Maibach, H.I. Safety of dermal diphoterine application: An active decontamination solution for chemical splash injuries. Cutan. Ocul. Toxicol. 2009, 28, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Lynn, D.D.; Zukin, L.M.; Dellavalle, R. The safety and efficacy of Diphoterine for ocular and cutaneous burns in humans. Cutan. Ocul. Toxicol. 2017, 36, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
| Author | Location and Study Period | Method | Study Group | Injury Type | Intervention | Control | Burn Area (TBSA †) | Assessment |
|---|---|---|---|---|---|---|---|---|
| Bvrar, 2016 [13] | Slovenia, no study year reported | Randomized controlled trial, no blinding | 22 police officers | Exposure to CS ¤ gas | Two groups. Preexposure group, who sprayed face and eyes with 200 mL diphoterine solution just before CS exposure (eight officers) Postexposure group, who sprayed face and open eyes with 200 mL diphoterine solution immediately after CS exposure (eight officers) | No treatment (six officers) | Data not available | Pain, NRS 0–10 (mean, 95% CI), time to return to work (min:sec) |
| Cavallini, 2010 [18] | Italy, no study year reported | Non-randomized controlled trial, no blinding | 25 patients | Chemical peel on both forearms using 70% glycolic acid solution for 5 min | Rinsing right forearm with diphoterine | Washing left forearm with water for 1 min and afterwards rinsing with diphoterine | Data not available | pH (mean) litmus paper |
| Donoghue, 2010 [17] | Australia, May 2005 to April 2006 and May 2007 to April 2008 (24 months) | Retrospective observational study of records from three alumina refineries | 266 workers | Alkali chemical splashes to the skin | Rinsing with diphoterine (126 workers) | Rinsing with water or no treatment (140 workers) | 0.75–38% | Time to return to work (days) |
| Huang, 2020 [12] | Taiwan, July 2010 to October 2017 | Retrospective observational study of records from the Taiwan Poison Control Center | 29 patients aged 22–48 years (male:female, 24:5) | TMAH * splashes of the skin | Rinsing with diphoterine | Rinsing with a decontaminant other than diphoterine | <1%—“Nearly entire body” | Depth of chemical burn (burn degree) |
| Kulkarni, 2018 [8] | India, September 2015 to November 2016 (14 months) | Prospective observational study of patients from The Ashirwad Clinic, Boisar | 65 patients aged 27–42 years (all male) | Both acid and alkali splashes of the skin | Rinsing with water plus diphoterine when admitted to hospital (nine patients) | Rinsing with water (56 patients) | 1–10% | Pain, VAS 0–10 (mean), time to return to work (days). |
| Nehles, 2006 [19] | Germany, 1994 to 1998 (4 years) | Retrospective observational study of records from a metallurgy | 24 workers aged 21–62 years (all male) | Both acid and alkali splashes | Rinsing with diphoterine | None | Head. Cheek. Thorax. Forearm. Face. Hand. Knee. Thorax, genitals, and thigh. | Complications |
| Nogue, 2012 [14] | Spain, 2009 to 2011 (18 months) | Prospective observational study of patients from the Área de Urgencias Hospital Clínic, Barcelona | 9 patients aged 21–71 years (male:female, 5:4) | Both acid and alkali splashes | Rinsing with diphoterine (four patients) | Rinsing with water or soap and water (five patients) | Data not available | Pain, and complications |
| Škarja, 2014 [15] | Slovenia, 2014 | Randomized controlled trial, blinded | 36 firefighters; mean age of 38 years (all male) (no collected data for 1 one firefighter) | Burn with 5 mL 15% NaOH on 25 cm2 skin for 55 s | Rinsing with diphoterine for 2 min (13 workers) | Rinsing with water for 2 min or no treatment (14 and 8 workers, respectively) | 25 cm2 skin on forearm | Pain, NRS 0–10 (mean ± SE) Measured at 55 s, and 2, 3, 15, 60, 120, 240, and 360 min. after exposure to NaOH |
| Zack-Williams, 2015 [16] | United Kingdom, January 2010 to September 2012 (32 months) | Retrospective observational study of patients from Queen Elizabeth Hospital, Birmingham, UK | 131 patients, mean age of 37.7 for the diphoterine group and mean age of 43.2 for the control group (male:female, 104:26) | Both acid and alkali splashes of the skin | Rinsing with diphoterine (47 patients) | Rinsing with water (84 patients) | Mean diphoterine group: 1.76% mean water group: 1.25% | Duration of hospitalization (days), and pH |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dinesen, F.; Pape, P.; Vestergaard, M.R.; Rasmussen, L.S. Diphoterine for Chemical Burns of the Skin: A Systematic Review. Eur. Burn J. 2023, 4, 55-68. https://doi.org/10.3390/ebj4010006
Dinesen F, Pape P, Vestergaard MR, Rasmussen LS. Diphoterine for Chemical Burns of the Skin: A Systematic Review. European Burn Journal. 2023; 4(1):55-68. https://doi.org/10.3390/ebj4010006
Chicago/Turabian StyleDinesen, Felicia, Pernille Pape, Martin Risom Vestergaard, and Lars Simon Rasmussen. 2023. "Diphoterine for Chemical Burns of the Skin: A Systematic Review" European Burn Journal 4, no. 1: 55-68. https://doi.org/10.3390/ebj4010006
APA StyleDinesen, F., Pape, P., Vestergaard, M. R., & Rasmussen, L. S. (2023). Diphoterine for Chemical Burns of the Skin: A Systematic Review. European Burn Journal, 4(1), 55-68. https://doi.org/10.3390/ebj4010006