
Comparison of Condylar Position Discrepancies Assessed Using an Optical Jaw Tracking System and a Conventional Condylar Position Indicator


Abstract
1. Introduction
2. Materials and Methods
2.1. Population
2.2. Diagnostic Tools and Procedures
2.3. CPI Records
2.4. Optical Jaw Tracking System (Modjaw) Records
2.5. Outcome Measures
2.6. Statistical Analysis
2.7. Sample Size Estimation
2.8. Correlation Analysis
2.9. ROC Curve Analysis
3. Results
3.1. Correlation Analysis
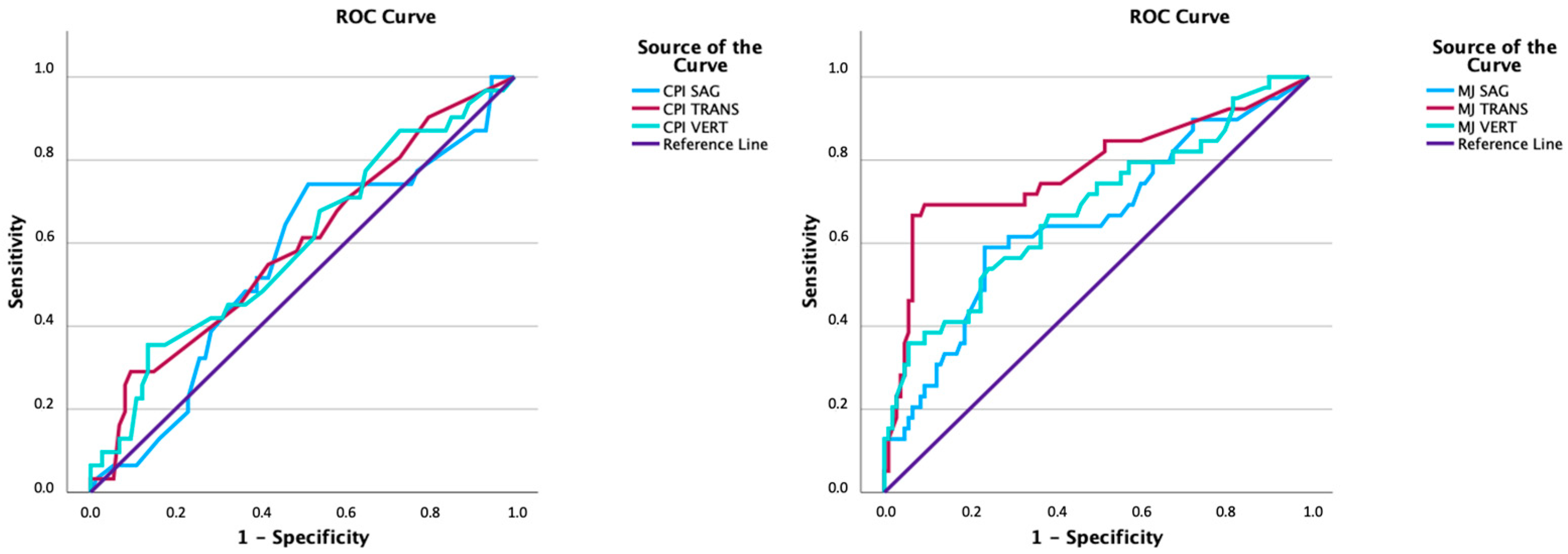
3.2. ROC Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| TMJ | temporomandibular joint |
| TMD | temporomandibular disorders |
| CR | centric relation |
| CO | centric occlusion |
| MI | maximum intercuspation |
| MJ | Modjaw |
| CPI | condylar position indicator |
| SAG | sagittal |
| VERT | vertical |
| TRANS | transverse |
| L | left |
| R | right |
| ROC | receiver operating characteristic |
| AUC | area under the curve |
| ICC | intraclass correlation coefficient |
Appendix A. Measurement Error Analysis for Repeated Measurements (n = 30)
| 1st Measurement | Repetition | p-Value | ICC | |
| Mean (SD) | Mean (SD) | |||
| CPI | ||||
| Vertical right | 2.19 (1.54) | 2.19 (1.52) | 0.846 | 0.998 |
| Sagittal right | −2.02 (1.21) | −2.02 (1.19) | 0.851 | 0.997 |
| Vertical left | 3.01 (1.45) | 3.02 (1.45) | 0.558 | 0.999 |
| Sagittal left | −2.16 (1.37) | −2.12 (1.35) | 0.130 | 0.997 |
| Transversal | −0.75 (0.95) | −0.78 (0.95) | 0.129 | 0.996 |
| Modjaw | ||||
| Vertical right | 0.08 (1.01) | 0.14 (1.22) | 0.227 | 0.967 |
| Sagittal right | −0.33 (0.79) | −0.30 (1.07) | 0.646 | 0.910 |
| Vertical left | −0.01 (0.74) | −0.05 (0.91) | 0.502 | 0.945 |
| Sagittal left | −0.39 (0.75) | −0.39 (0.90) | 0.927 | 0.971 |
| Transversal | 0.10 (0.72) | 0.13 (0.80) | 0.326 | 0.981 |
| p: paired Student’s t-test significance value; ICC: intraclass correlation coefficient. | ||||
References
- Okeson, J. Management of Temporomandibular Disorders and Occlusion, 7th ed.; Elsevier: St. Louis, MO, USA, 2008. [Google Scholar]
- Kandasamy, S.; Rinchuse, D.J.; Greene, C.S.; Johnston, L.E. Temporomandibular disorders and orthodontics: What have we learned from 1992–2022? Am. J. Orthod. Dentofac. Orthop. 2022, 161, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Crawford, S.D. Condylar axis position, as determined by the occlusion and measured by the CPI instrument, and signs and symptoms of temporomandibular dysfunction. Angle Orthod. 1999, 69, 103–115. [Google Scholar]
- Freeland, T. Articulators in Orthodontics. Semin. Orthod. 2012, 18, 51–62. [Google Scholar] [CrossRef]
- Manfredini, D.; Ercoli, C.; Poggio, C.E.; Carboncini, F.; Ferrari, M. Centric relation—A biological perspective of a technical concept. J. Oral Rehabil. 2023, 50, 1355–1361. [Google Scholar] [CrossRef]
- Academy of Denture Prosthetics. Nomenclature Committee. The Glossary of Prosthodontic Terms. J. Prosthet. Dent. 2017, 117, e1–e105. [Google Scholar] [CrossRef]
- Roth, R.H. Occlusion and condylar position. Am. J. Orthod. Dentofac. Orthop. 1995, 107, 315–318. [Google Scholar] [CrossRef]
- Roth, R.H. Functional occlusion for the orthodontist. J. Clin. Orthod. 1981, 15, 32–40, 44–51. [Google Scholar]
- Shildkraut, M.; Wood, D.P.; Hunter, W.S. The CR-CO discrepancy and its effect on cephalometric measurements. Angle Orthod. 1994, 64, 333–342. [Google Scholar]
- Cordray, F.E. Articulated dental cast analysis of asymptomatic and symptomatic populations. Int. J. Oral Sci. 2016, 8, 126–132. [Google Scholar] [CrossRef]
- Cheong, C.; Radomski, K.; Otten, J.; Lee, S. A clinical comparative analysis using an optical tracking device versus conventional tracking device in the production of occlusal appliances. J. Prosthodont. 2025, 34, 350–356. [Google Scholar] [CrossRef]
- Bapelle, M.; Dubromez, J.; Savoldelli, C.; Tillier, Y.; Ehrmann, E. Modjaw® device: Analysis of mandibular kinematics recorded for a group of asymptomatic subjects. Cranio® 2021, 42, 483–489. [Google Scholar] [CrossRef]
- Bedrossian, E.A.; Bedrossian, E.; Kois, J.C.; Revilla-Leon, M. Use of an optical jaw-tracking system to record mandibular motion for treatment planning and designing interim and definitive prostheses: A dental technique. J. Prosthet. Dent. 2022, 132, 659–674. [Google Scholar] [CrossRef]
- Revilla-Leon, M.; Agustin-Panadero, R.; Zeitler, J.M.; Barmak, A.B.; Yilmaz, B.; Kois, J.C.; Pérez-Barquero, J.A. Differences in maxillomandibular relationship recorded at centric relation when using a conventional method, four intraoral scanners, and a jaw tracking system: A clinical study. J. Prosthet. Dent. 2023, 132, 964–972. [Google Scholar] [CrossRef]
- Revilla-León, M.; Fernández-Estevan, L.; Barmak, A.B.; Kois, J.C.; Pérez-Barquero, J.A. Accuracy of the maxillomandibular relationship at centric relation position recorded by using 3 different intraoral scanners with or without an optical jaw tracking system: An in vivo pilot study. J. Dent. 2023, 132, 104478. [Google Scholar] [CrossRef]
- Revilla-Leon, M.; Zeitler, J.M.; Gomez-Polo, M.; Kois, J.C. Utilizing additively manufactured custom devices to record mandibular motion by using optical jaw tracking systems: A dental technique. J. Prosthet. Dent. 2022, 131, 560–566. [Google Scholar] [CrossRef]
- Solaberrieta, E.; Minguez, R.; Barrenetxea, L.; Otegi, J.R.; Szentpetery, A. Comparison of the accuracy of a 3-dimensional virtual method and the conventional method for transferring the maxillary cast to a virtual articulator. J. Prosthet. Dent. 2015, 113, 191–197. [Google Scholar] [CrossRef]
- da Cunha, D.V.; Degan, V.V.; Vedovello Filho, M.; Bellomo, D.P., Jr.; Silva, M.R.; Furtado, D.A.; Andrade, A.O.; Milagre, S.T.; Pereira, A.A. Real-time three-dimensional jaw tracking in temporomandibular disorders. J. Oral Rehabil. 2017, 44, 580–588. [Google Scholar] [CrossRef]
- Zhao, W.; Feng, Y.; Cao, R.; Sun, J.; Zhang, J.; Zhao, X.; Liu, W. Comparative analysis of three jaw motion tracking systems: A study on precision and trueness. J. Prosthodont. 2024, 34, 263–270. [Google Scholar] [CrossRef]
- Valesan, L.F.; Da-Cas, C.D.; Réus, J.C.; Denardin, A.C.S.; Garanhani, R.R.; Bonotto, D.; Januzzi, E.; de Souza, B.D.M. Prevalence of temporomandibular joint disorders: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 441–453. [Google Scholar] [CrossRef]
- Romani, V.; Di Giorgio, R.; Castellano, M.; Barbato, E.; Galluccio, G. Prevalence of craniomandibular disorders in orthodontic pediatric population and possible interactions with anxiety and stress. Eur. J. Paediatr. Dent. 2018, 19, 317–323. [Google Scholar]
- Manfredini, D.; Stellini, E.; Gracco, A.; Lombardo, L.; Nardini, L.; Siciliani, G. Orthodontics is temporomandibular disorder-neutral. Angle Orthod. 2016, 86, 649–654. [Google Scholar] [CrossRef]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.-P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- Al-Saleh, M.A.; Alsufyani, N.A.; Saltaji, H.; Jaremko, J.L.; Major, P.W. MRI and CBCT image registration of temporomandibular joint: A systematic review. J. Otolaryngol. Head Neck Surg. 2016, 45, 30. [Google Scholar] [CrossRef]
- Tegnander, T.; Chladek, G.A.-O.; Hovland, A.; Żmudzki, J.A.-O.; Wojtek, P. Relationship between Clinical Symptoms and Magnetic Resonance Imaging in Temporomandibular Disorder (TMD) Patients Utilizing the Piper MRI Diagnostic System. J. Clin. Med. 2021, 10, 4698. [Google Scholar] [CrossRef]
- Weffort, S.Y.; de Fantini, S.M. Condylar displacement between centric relation and maximum intercuspation in symptomatic and asymptomatic individuals. Angle Orthod. 2010, 80, 835–842. [Google Scholar] [CrossRef]
- Fantini, S.; Paiva, J.; Rino, J.; Dominguez, G.; Abrão, J.; Vigoritto, J. Increase of condylar displacement between centric relation and maximal habitual intercuspation after occlusal splint therapy. Braz. Oral Res. 2005, 19, 176–182. [Google Scholar] [CrossRef]
- Kordass, B.; Gartner, C.; Sohnel, A.; Bisler, A.; Voß, G.; Bockholt, U.; Seipel, S. The virtual articulator in dentistry: Concept and development. Dent. Clin. N. Am. 2002, 46, 493–506. [Google Scholar] [CrossRef]
- Camci, H.; Salmanpour, F. A new technique for testing accuracy and sensitivity of digital bite registration: A prospective comparative study. Int. Orthod. 2021, 19, 425–432. [Google Scholar] [CrossRef]
- Cohen, J.F.; Korevaar, D.A.; Altman, D.G.; Bruns, D.E.; Gatsonis, C.A.; Hooft, L.; Irwig, L.; Levine, D.; Reitsma, J.B.; de Vet, H.C.; et al. Stard 2015 guidelines for reporting diagnostic accuracy studies: Explanation and elaboration. BMJ Open 2016, 6, e012799. [Google Scholar] [CrossRef]
- Schmitt, M.; Kulbersh, R.; Freeland, T.; Bever, K.; Pink, F. Reproducibility of the Roth Power Centric in Determining Centric Relation. Semin. Orthod. 2003, 9, 102–108. [Google Scholar] [CrossRef]
- Fleiss, J. The Design and Analysis of Clinical Experiments; Wiley Classics Library Edition: Hoboken, NJ, USA, 1999. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Bujang, M. An elaboration on sample size determination for correlations based on effect sizes and confidence interval width: A guide for researchers. Restor. Dent. Endod. 2024, 49, e21. [Google Scholar] [CrossRef] [PubMed]
- Akobeng, A.K. Understanding diagnostic tests 1: Sensitivity, specificity and predictive values. Acta Paediatr. 2007, 96, 338–341. [Google Scholar] [CrossRef]
- Fletcher, R.H.; Fletcher, S.W.; Fletcher, G.S. Clinical Epidemiology: The Essentials, 5th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2014. [Google Scholar]
- Girardot, R.A., Jr. Comparison of condylar position in hyperdivergent and hypodivergent facial skeletal types. Angle Orthod. 2001, 71, 240–246. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Variable | CPI | Modjaw | R | 95% CI | |
|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Lower Bound | Upper Bound | ||
| Vertical left | 2.96 (2.01) | −0.07 (0.74) | −0.064 NS | −0.304 | 0.175 |
| Vertical right | 2.45 (1.81) | 0.24 (0.98) | 0.230 NS | −0.004 | 0.464 |
| Sagittal left | −2.25 (1.85) | −0.48 (0.69) | 0.286 * | 0.056 | 0.516 |
| Sagittal right | −1.90 (1.47) | −0.40 (0.71) | −0.067 NS | −0.306 | 0.173 |
| Transversal | −0.56 (1.01) | 0.04 (0.73) | 0.066 NS | −0.174 | 0.305 |
| Variables | Area | Asymptotic Significance a | Asymptotic 95% Confidence Interval | |
|---|---|---|---|---|
| Lower Bound | Upper Bound | |||
| CPI VERT | 0.595 | 0.126 | 0.473 | 0.716 |
| CPI SAG | 0.554 | 0.388 | 0.432 | 0.675 |
| CPI TRANS | 0.593 | 0.132 | 0.472 | 0.713 |
| MJ VERT | 0.683 | 0.001 | 0.580 | 0.786 |
| MJ SAG | 0.654 | 0.004 | 0.549 | 0.759 |
| MJ TRANS | 0.777 | <0.001 | 0.679 | 0.876 |
| Variable(s) | Gini Index | K-S Statistics | |
|---|---|---|---|
| Max K-S a | Cut-Off (mm) | ||
| CPI VERT | 0.189 | 0.220 | 4.30 |
| CPI SAG | 0.107 | 0.228 | 1.95 |
| CPI TRANS | 0.185 | 0.196 | 1.35 |
| MJ VERT | 0.366 | 0.302 | 1.77 |
| MJ SAG | 0.308 | 0.354 | 0.91 |
| MJ TRANS | 0.554 | 0.601 | 0.49 |
| Variable | Cut-Off (mm) | Sensitivity | Specificity | PPV | NPV | Youden’s Index |
|---|---|---|---|---|---|---|
| CPI VERT | 4.5 | 35.48 | 86.49 | 52.38 | 76.19 | 0.220 |
| CPI SAG | 2 | 74.19 | 48.65 | 37.70 | 81.82 | 0.228 |
| CPI TRANS | 1.5 | 29.03 | 90.54 | 56.25 | 75.28 | 0.196 |
| MJ VERT | 2 | 28.21 | 95.28 | 68.75 | 78.29 | 0.235 |
| MJ SAG | 1 | 48.72 | 77.36 | 44.19 | 80.39 | 0.261 |
| MJ TRANS | 0.5 | 66.67 | 93.40 | 78.79 | 88.39 | 0.601 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, J.; Martins, E.; Canabez, A.; Martin, D.; Martin, C. Comparison of Condylar Position Discrepancies Assessed Using an Optical Jaw Tracking System and a Conventional Condylar Position Indicator. Prosthesis 2025, 7, 40. https://doi.org/10.3390/prosthesis7020040
Silva J, Martins E, Canabez A, Martin D, Martin C. Comparison of Condylar Position Discrepancies Assessed Using an Optical Jaw Tracking System and a Conventional Condylar Position Indicator. Prosthesis. 2025; 7(2):40. https://doi.org/10.3390/prosthesis7020040
Chicago/Turabian StyleSilva, Joana, Eugénio Martins, Alberto Canabez, Domingo Martin, and Conchita Martin. 2025. "Comparison of Condylar Position Discrepancies Assessed Using an Optical Jaw Tracking System and a Conventional Condylar Position Indicator" Prosthesis 7, no. 2: 40. https://doi.org/10.3390/prosthesis7020040
APA StyleSilva, J., Martins, E., Canabez, A., Martin, D., & Martin, C. (2025). Comparison of Condylar Position Discrepancies Assessed Using an Optical Jaw Tracking System and a Conventional Condylar Position Indicator. Prosthesis, 7(2), 40. https://doi.org/10.3390/prosthesis7020040