

Digital Analysis of Occlusion in Fixed Partial Implant Prostheses: How to Overcome Age-Related Changes in the Stomatognathic System

 , ,
, ,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Methodology of the Project
- Patients with partially implant-supported prostheses.
- Patients with Angle Class I occlusion.
- Patients without dental absences, excluding third molars.
- Adult patients.
- Patients over 80 years of age.
- Patients with disabilities that hindered proper understanding and execution of the study.
- Patients with temporomandibular joint pathologies.
- Patients without occlusal stability, preventing reliable and repetitive attainment of MI.
- Patients unwilling to participate or desiring to withdraw from the study.
- Group 1: 60 patients with partially implant-supported prostheses, where occlusal adjustment and the necessary procedures to establish IPO were performed using conventional methods with articulating paper, along with simultaneous EMG.
- Group 2: 60 patients with partially implant-supported prostheses, where IPO was established using T-Scan III software, along with simultaneous EMG.
2.1.1. Common Methodology for Both Groups
2.1.2. Specific Methodology of Group 1
2.1.3. Specific Methodology of Group 2
2.2. Variables
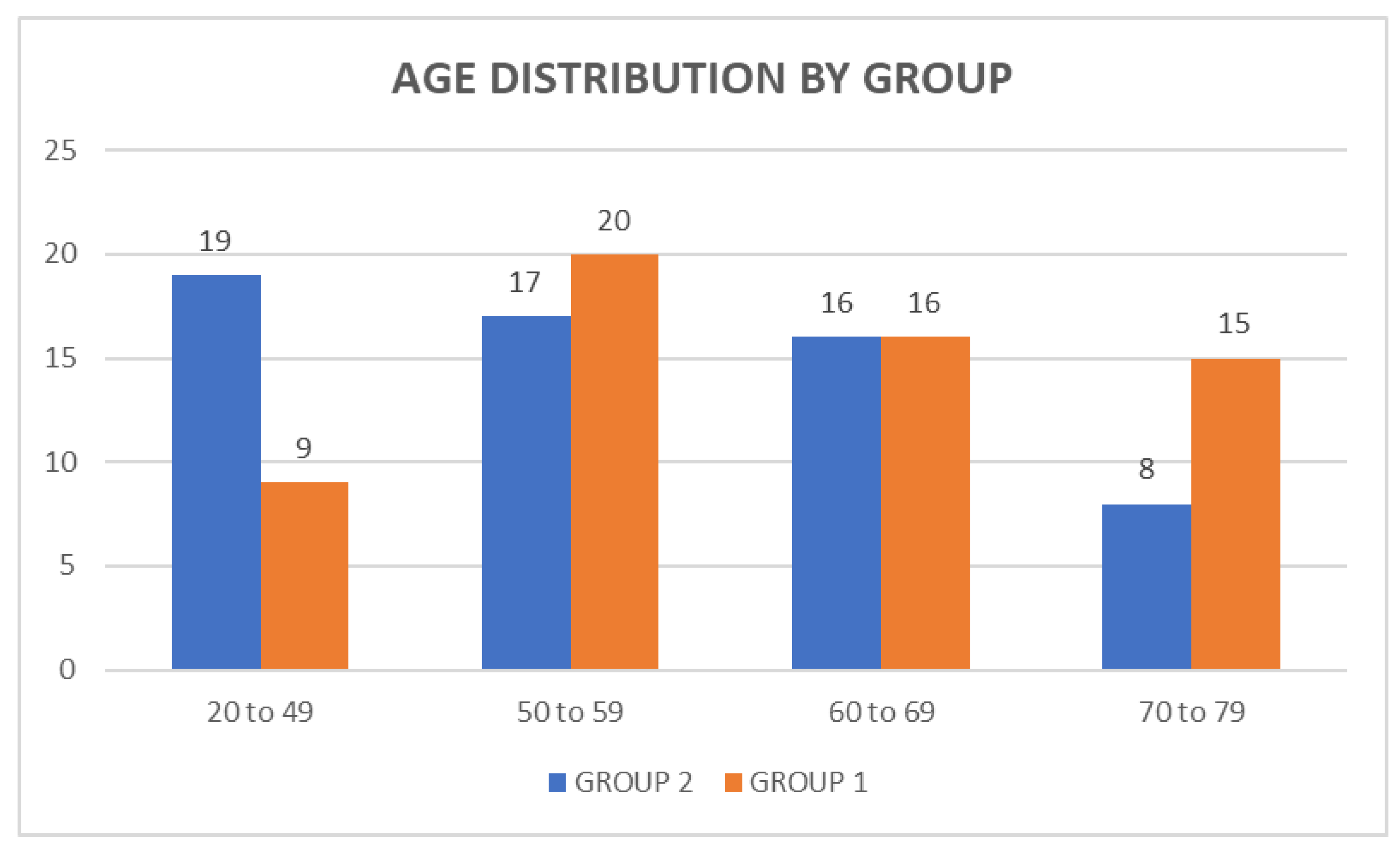
- Age. Patients were divided intro subgroups based on age intervals: 20 to 49; 50 to 59; 60 to 69; and 70 to 79 years. The aim was to observe if other variables and IPO differed with age.
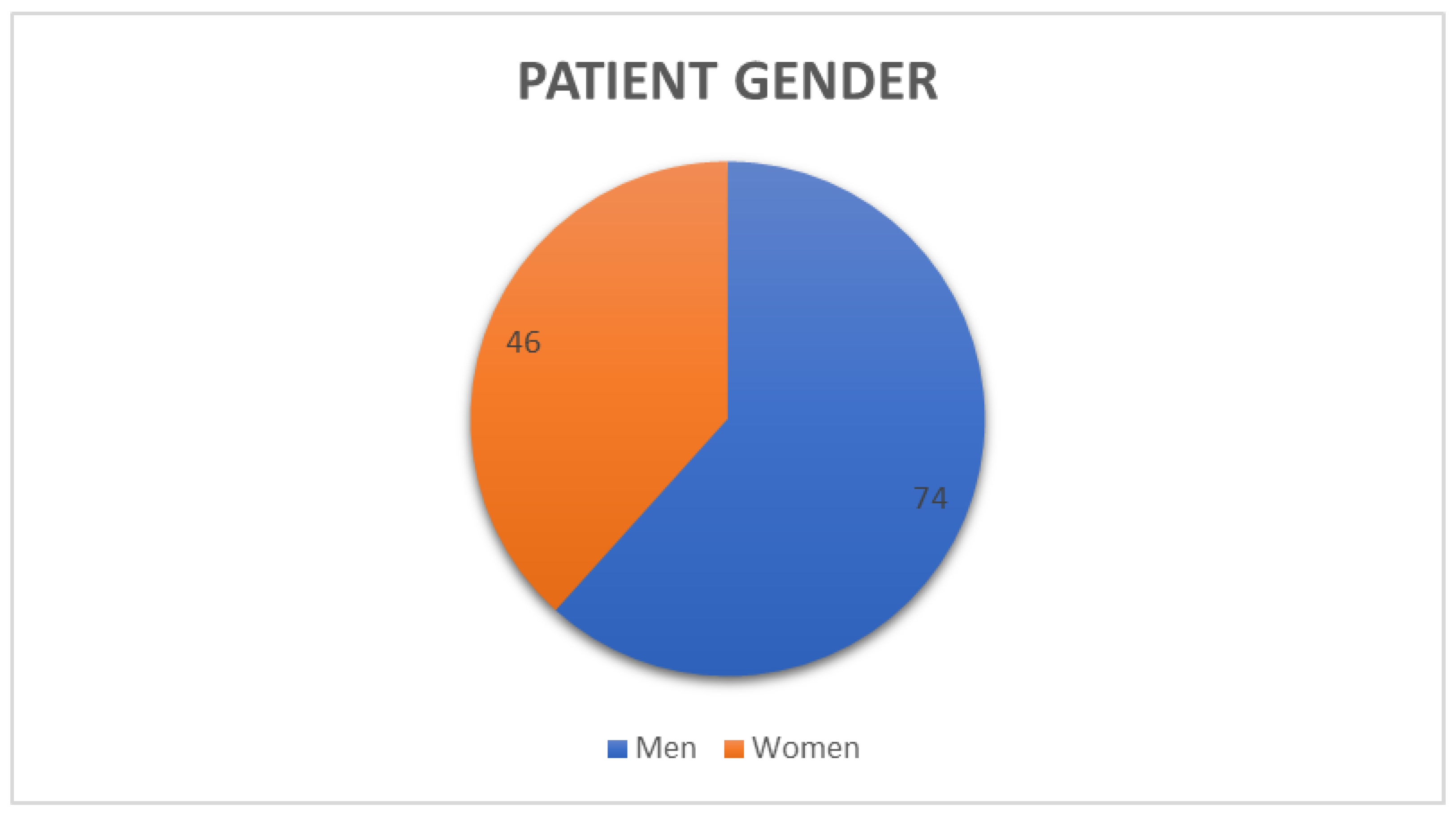
- Sex. This study aimed to determine if sex influenced other variables and the body’s response to the implementation of IPO.
- Pre-IPO prosthesis contact. The presence of contact between the implant-supported prosthesis and the opposing tooth when the patient was asked to bite without applying conscious force (without exerting force) before the occlusal adjustment for IPO. This variable aimed to determine if the patient had an existing IPO and if this situation could be improved after implementing IPO.
- Post-IPO prosthesis contact. The presence of contact between the prosthesis and the opposing tooth when the patient was asked to perform an MI position without conscious force after the IPO was installed. These data were extracted from T-Scan analysis. This variable aimed to assess the effectiveness of the methodology implemented in establishing IPO and to compare conventional methods with digital systems.
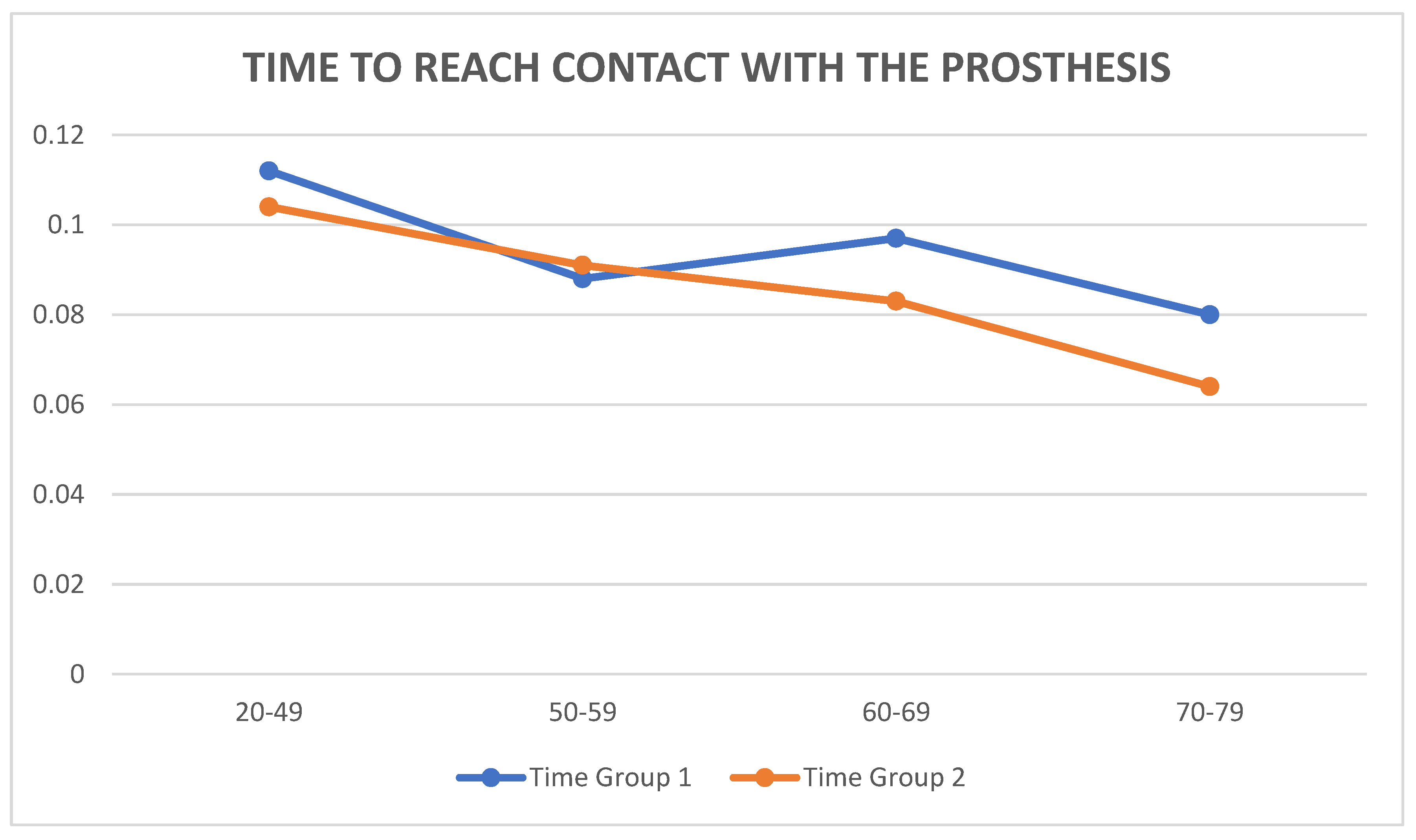
- Time to first contact. The time in seconds (s) it took for the prosthesis to make its first contact with the opposing tooth when the patient performed a forceful MI. These data were extracted from T-Scan analysis and helped to verify theories about the PL space around the teeth, serving as evidence to assess the correct implementation of IPO.
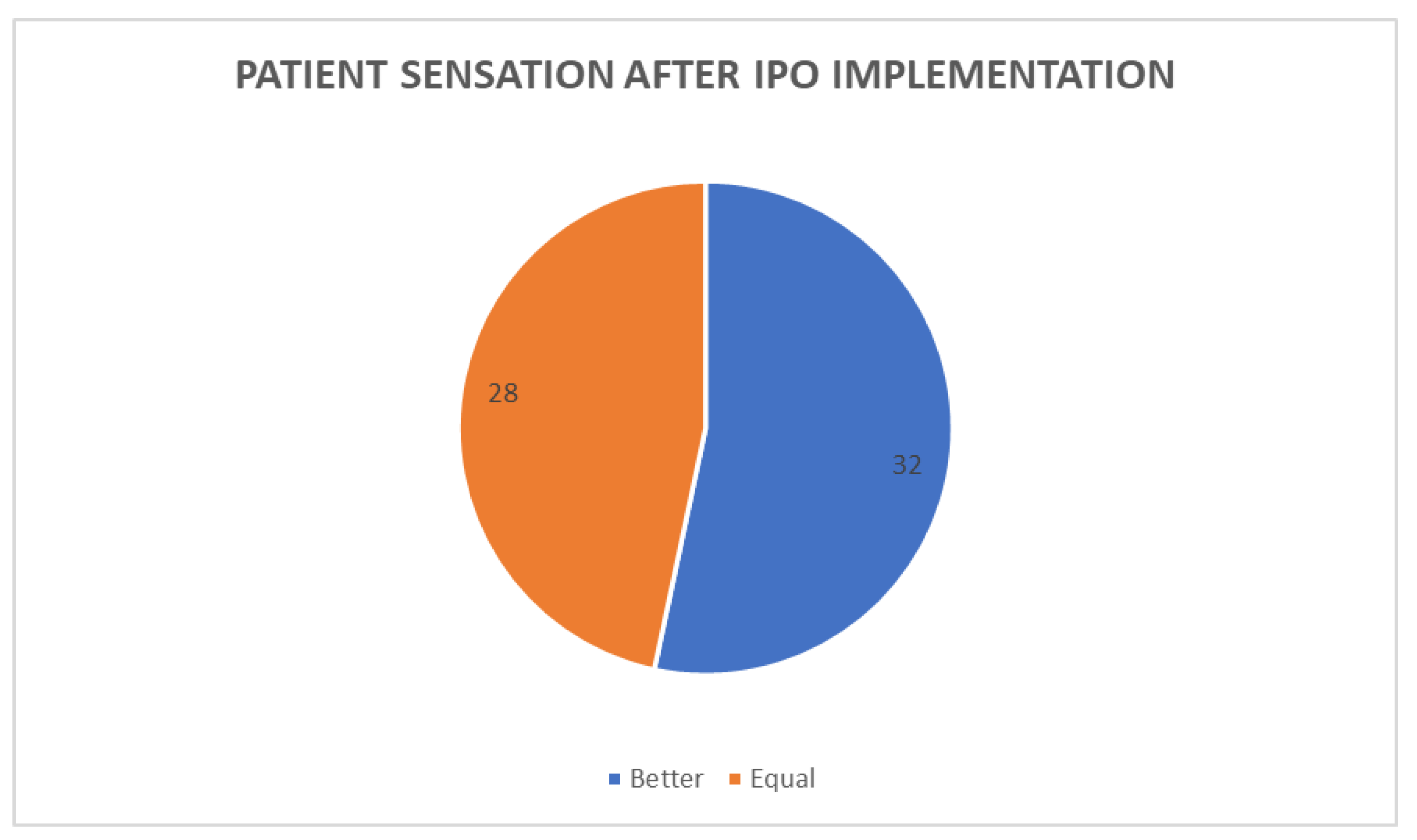
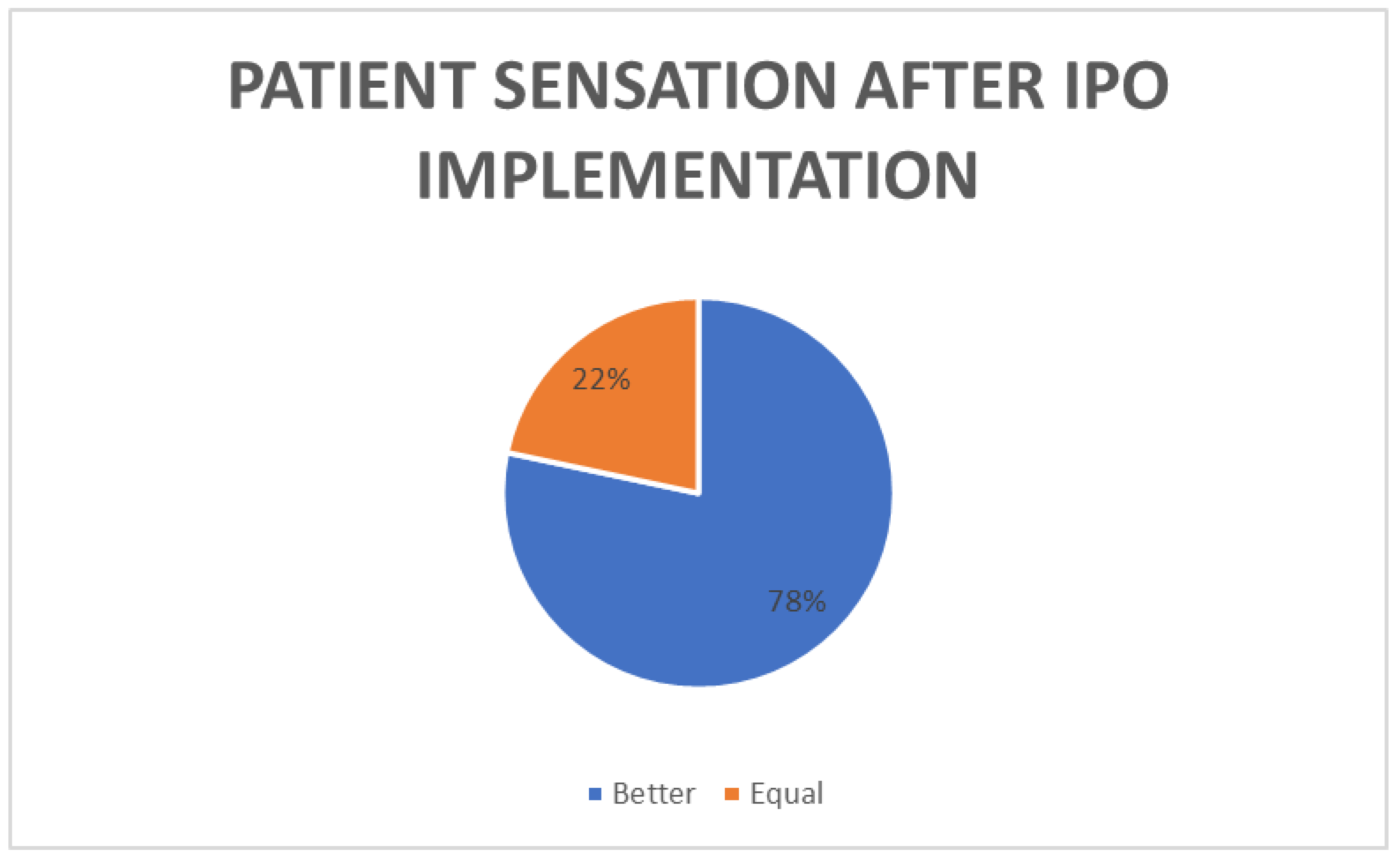
- Post-IPO patient sensation. The patient’s perception of comfort and conformity after the completion of the study, compared to their previous state. This variable aimed to involve the patient and gather their opinion on comfort after the implementation of IPO.
- Electromyographic data. Measured in microvolts (μv), these data represent the muscular activity of the masseter muscles. Values were extracted before and after the implementation of IPO for comparison. These data are useful to assess the reactivity of the stomatognathic system to changes in the dental arch. The goal was to achieve an occlusal balance that also allowed for a balance in muscular electrical activity.
2.3. Statistical Analysis
- One-way analysis of variance (ANOVA) with the following statistical tests, depending on the type of distribution and variances:
- a.
- For normally distributed variables with equal variances, the Scheffe test and Tukey–Kramer test were used.
- b.
- For normally distributed variables with unequal variances, stabilizing transformations were applied, followed by the Scheffe test.
- c.
- For variables with any other distribution, either equal or unequal variances, non-parametric methods were used: Kruskal–Wallis Z-value multiple comparison (Dunn’s Test) with Regular Test or Bonferroni Test.
- Two-sample T-test, in which, depending on the type of distribution and variances, the following tests were applied:
- d.
- For normally distributed variables with equal variances, Student’s T-test was used.
- e.
- For normally distributed variables with unequal variances, the Aspin–Welch test was applied.
- f.
- For variables with any other distribution, either equal or unequal variances, the Kolmogorov–Smirnov test was used.
- g.
- For differences between medians, the Mann–Whitney U or Wilcoxon Rank-Sum test was applied.
- Correlation of matrices was determined using the following tests:
- h.
- Pearson correlation
- i.
- Spearman correlation
3. Results
3.1. Descriptive Statistics
3.2. Analysis of Data by Groups
3.2.1. Group 1
3.2.2. Group 2
3.3. Analysis of Data between Groups 1 and 2
3.4. Analysis of Data via Age Intervals
4. Discussion
5. Conclusions
- It has been shown that there are many differences between dental implants and teeth.
- The use of digital software improves the results of occlusal adjustment.
- Age affects the sensitivity of patients and the results of the adjustment.
- LPO is influenced by age: the older the person is, the more time is needed to compress the LPO.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Swaminathan, Y.; Rao, G. Implant Protected Occlusion. J. Dent. Med. Sci. 2013, 11, 20–25. [Google Scholar] [CrossRef]
- Graves, C.V.; Harrel, S.K.; Rossmann, J.A.; Kerns, D.; Gonzalez, J.A.; Kontogiorgos, E.D.; Al-Hashimi, I.; Abraham, C. The Role of Occlusion in the Dental Implant and Peri-implant Condition: A Review. Open Dent. J. 2016, 10, 594–601. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.C.C.; Sukotjo, C. Occlusion for implant-supported fixed dental prostheses in partially edentulous patients: A literature review and current concepts. J. Periodontal. Implant Sci. 2013, 43, 51–57. [Google Scholar] [CrossRef]
- Michalakis, K.X.; Calvani, P.; Hirayama, H. Biomechanical considerations on tooth-implant supported fixed partial dentures. J. Dent. Biomech. 2012, 3, 1758736012462025. [Google Scholar] [CrossRef]
- Haggard, P.; de Boer, L. Oral somatosensory awareness. Neurosci. Biobehav. Rev. 2014, 47, 469–484. [Google Scholar] [CrossRef]
- Lim, W.H.; Liu, B.; Mah, S.J.; Chen, S.; Helms, J.A. The molecular and cellular effects of ageing on the periodontal ligament. J. Clin. Periodontol. 2014, 41, 935–942. [Google Scholar] [CrossRef]
- Yilmaz, G.; Laine, C.M.; Tinastepe, N.; Özyurt, M.G.; Türker, K.S. Periodontal mechanoreceptors and bruxism at low bite forces. Arch. Oral. Biol. 2019, 98, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kweon, H.H.I.; Choi, S.H.; Kim, Y.T. Association between dental implants in the posterior region and traumatic occlusion in the adjacent premolars: A long-term follow-up clinical and radiographic analysis. J. Periodontal. Implant Sci. 2016, 46, 396–404. [Google Scholar] [CrossRef]
- Sheridan, R.A.; Decker, A.M.; Plonka, A.B.; Wang, H.L. The Role of Occlusion in Implant Therapy: A Comprehensive Updated Review. Implant Dent. 2016, 25, 829–838. [Google Scholar] [CrossRef]
- Zhou, T.; Wongpairojpanich, J.; Sareethammanuwat, M.; Lilakhunakon, C.; Buranawat, B. Digital occlusal analysis of pre and post single posterior implant restoration delivery: A pilot study. PLoS ONE 2021, 16, e0252191. [Google Scholar] [CrossRef]
- Oliveira, A.; Bessa, A.; Dias, F.; Oliveira, A. Clinical applications of occlusion principles in implantology—Narrative review. J. Surg. Peridontology Implant Res. 2019, 1, 40–45. [Google Scholar]
- Wiens, J.P.; Priebe, J.W. Occlusal stability. Dent. Clin. N. Am. 2014, 58, 19–43. [Google Scholar] [CrossRef] [PubMed]
- Abichandani, S.; Bhojaraju, N.; Guttal, S.; Srilakshmi, J. Implant protected occlusion: A comprehensive review. Eur. J. Prosthodont. 2013, 1, 29. [Google Scholar] [CrossRef]
- Madani, A.S.; Nakhaei, M.; Alami, M.; Haghi, H.R.; Moazzami, S.M. Post-insertion posterior single-implant occlusion changes at different intervals: A T-scan computerized occlusal analysis. J. Contemp. Dent. Pract. 2017, 18, 927–932. [Google Scholar] [CrossRef] [PubMed]
- Afrashtehfar, K.I.; Qadeer, S. Computerized occlusal analysis as an alternative occlusal indicator. Cranio-J. Craniomandib. Pract. 2016, 34, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Chaithanya, R.; Sajjan, S.; Raju, A.R. A study of change in occlusal contacts and force dynamics after fixed prosthetic treatment and after equilibration—Using Tekscan III. J. Indian Prosthodont. Soc. 2019, 19, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Röhrle, O.; Saini, H.; Lee, P.V.S.; Ackland, D.C. A novel computational method to determine subject-specific bite force and occlusal loading during mastication. Comput. Methods Biomech. Biomed. Eng. 2018, 21, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Roque, M.A.; Gallucci, G.O.; Lee, S.J. Occlusal Pressure Redistribution with Single Implant Restorations. J. Prosthodont. 2017, 26, 275–279. [Google Scholar] [CrossRef]
- Qadeer, S.; Kerstein, R.; Kim, R.J.Y.; Huh, J.B.; Shin, S.W. Relationship between articulation paper mark size and percentage of force measured with computerized occlusal analysis. J. Adv. Prosthodont. 2012, 4, 7–12. [Google Scholar] [CrossRef]
- Dib-Zakkour, J.; Flores-Fraile, J.; Montero-Martin, J.; Dib-Zakkour, S.; Dib-Zaitun, I. Evaluation of the Effectiveness of Dry Needling in the Treatment of Myogenous Temporomandibular Joint Disorders. Medicina 2022, 58, 256. [Google Scholar] [CrossRef]
- Dib, A.; Montero, J.; Sanchez, J.M.; López-Valverde, A. Electromyographic and patient-reported outcomes of a computer-guided occlusal adjustment performed on patients suffering from chronic myofascial pain. Med. Oral Patol. Oral Cir. Bucal. 2015, 20, e135–e143. Available online: http://www.ncbi.nlm.nih.gov/pubmed/25475783 (accessed on 12 November 2017). [CrossRef] [PubMed]
- Lewis, M.B.; Klineberg, I. Prosthodontic considerations designed to optimize outcomes for single-tooth implants. A review of the literature. Aust. Dent. J. 2011, 56, 181–192. [Google Scholar] [CrossRef] [PubMed]
- Nuzzolese, E.; Lepore, M.M.; Cukovic-Bagic, I.; Montagna, F.; Di Vella, G. Forensic sciences and forensic odontology. Int. Dent. J. 2008, 58, 342–348. [Google Scholar] [CrossRef]
- Duyck, J.; Vandamme, K. The effect of loading on peri-implant bone: A critical review of the literature. J. Oral Rehabil. 2014, 41, 783–794. [Google Scholar] [CrossRef]
- Luo, Q.; Ding, Q.; Zhang, L.; Xie, Q. Analyzing the occlusion variation of single posterior implant–supported fixed prostheses by using the T-scan system: A prospective 3-year follow-up study. J. Prosthet. Dent. 2020, 123, 79–84. [Google Scholar] [CrossRef]
- Koos, B.; Godt, A.; Schille, C.; Göz, G. Präzision eines instrumentellen Analyseverfahrens der Okklusion und ihrer resultierenden Kraftverteilung im Zahnbogen. J. Orofac. Orthop. 2010, 71, 403–410. [Google Scholar] [CrossRef]
- Sadowsky, S.J. Occlusal overload with dental implants: A review. Int. J. Implant Dent. 2019, 5, 29. [Google Scholar] [CrossRef] [PubMed]
- Cordaro, L.; Torsello, F.; Rocuzzo, M. Implant loading protocols for the partially edentulous posterior mandible. Int. J. Oral Maxillofac. Implants 2009, 24, 169–179. Available online: http://www.ncbi.nlm.nih.gov/pubmed/19885444 (accessed on 15 March 2022).
- Ding, X.; Liao, S.H.; Zhu, X.H.; Zhang, X.H.; Zhang, L. Effect of diameter and length on stress distribution of the alveolar crest around immediate loading implants. Clin. Implant Dent. Relat. Res. 2009, 11, 279–287. [Google Scholar] [CrossRef]
- Al-Omiri, M.K.; Sghaireen, M.G.; Alhijawi, M.M.; Alzoubi, I.A.; Lynch, C.D.; Lynch, E. Maximum bite force following unilateral implant-supported prosthetic treatment: Within-subject comparison to opposite dentate side. J. Oral Rehabil. 2014, 41, 624–629. [Google Scholar] [CrossRef]
- Kazemi, M.; Geramipanah, F.; Negahdari, R.; Rakhshan, V. Active tactile sensibility of single-tooth implants versus natural dentition: A split-mouth double-blind randomized clinical trial. Clin. Implant Dent. Relat. Res. 2014, 16, 947–955. [Google Scholar] [CrossRef] [PubMed]
- Lossdörfer, S.; Kraus, D.; Jäger, A. Aging affects the phenotypic characteristics of human periodontal ligament cells and the cellular response to hormonal stimulation in vitro. J. Periodontal. Res. 2010, 45, 764–771. [Google Scholar] [CrossRef] [PubMed]
- Benatti, B.B.; Silverio, K.G.; Casati, M.Z.; Sallum, E.A.; Nociti, F.H. Influence of aging on biological properties of periodontal ligament cells. Connect. Tissue Res. 2008, 49, 401–408. [Google Scholar] [CrossRef]
- Denes, B.J.; Mavropoulos, A.; Bresin, A.; Kiliaridis, S. Influence of masticatory hypofunction on the alveolar bone and the molar periodontal ligament space in the rat maxilla. Eur. J. Oral Sci. 2013, 121, 532–537. [Google Scholar] [CrossRef]
- Grigoriadis, A.; Trulsson, M. Excitatory drive of masseter muscle during mastication with dental implants. Sci. Rep. 2018, 8, 8597. [Google Scholar] [CrossRef]
- Grigoriadis, A.; Johansson, R.S.; Trulsson, M. Adaptability of mastication in people with implant-supported bridges. J. Clin. Periodontol. 2011, 38, 395–404. [Google Scholar] [CrossRef]
- Mishellany-Dutour, A.; Renaud, J.; Peyron, M.A.; Rimek, F.; Woda, A. Is the goal of mastication reached in young dentates, aged dentates and aged denture wearers? Br. J. Nutr. 2008, 99, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Kerstein, R.B.; Radke, J. Clinician accuracy when subjectively interpreting articulating paper markings. Cranio-J. Craniomandib. Sleep Pract. 2014, 32, 13–23. [Google Scholar] [CrossRef]
- Carey, J.P.; Craig, M.; Kerstein, R.B.; Radke, J. Determining a Relationship Between Applied Occlusal Load and Articulating Paper Mark Area. Open Dent. J. 2007, 1, 1–7. [Google Scholar] [CrossRef]
- Lee, S.M.; Lee, J.W. Computerized occlusal analysis: Correlation with occlusal indexes to assess the outcome of orthodontic treatment or the severity of malocculusion. Korean J. Orthod. 2016, 46, 27–35. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group 1 | Group 2 |
|---|---|
| 60 patients | 60 patients |
| Partial implant-supported prosthesis wearers | Partial implant-supported prosthesis wearers |
| EMG recording | EMG recording |
| NO recording with T-Scan III | Occlusal recording with T-Scan III |
| Articulating paper used to observe existing occlusion and subsequently study and interpret occlusion | Articulating paper used solely to identify occlusal points that need to be modified/eliminated after T-Scan III |
| Occlusal adjustment | Occlusal adjustment |
| T-Scan measurement to verify the outcome of occlusal adjustment | T-Scan measurement to verify the outcome of occlusal adjustment |
| EMG recording | EMG recording |
| Satisfaction survey | Satisfaction survey |
| Group | Equal | Better | Total |
|---|---|---|---|
| 1 | 28 | 32 | 60 |
| 2 | 13 | 47 | 60 |
| Total | 41 | 79 | 120 |
| Mean | Standard Error | |
|---|---|---|
| Group 1 | 0.09 | 0.095 |
| Group 2 | 0.08 | 0.08 |
| 20–49 Years | 50–59 Years | 60–69 Years | 70–79 Years | |
|---|---|---|---|---|
| Better | 16 | 10 | 8 | 8 |
| Equal | 3 | 10 | 8 | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dib Zakkour, J.; Dib Zakkour, S.; Montero, J.; García-Cenador, B.; Flores-Fraile, J.; Dib Zaitun, A. Digital Analysis of Occlusion in Fixed Partial Implant Prostheses: How to Overcome Age-Related Changes in the Stomatognathic System. Prosthesis 2024, 6, 119-134. https://doi.org/10.3390/prosthesis6010010
Dib Zakkour J, Dib Zakkour S, Montero J, García-Cenador B, Flores-Fraile J, Dib Zaitun A. Digital Analysis of Occlusion in Fixed Partial Implant Prostheses: How to Overcome Age-Related Changes in the Stomatognathic System. Prosthesis. 2024; 6(1):119-134. https://doi.org/10.3390/prosthesis6010010
Chicago/Turabian StyleDib Zakkour, Juan, Sara Dib Zakkour, Javier Montero, Begoña García-Cenador, Javier Flores-Fraile, and Abraham Dib Zaitun. 2024. "Digital Analysis of Occlusion in Fixed Partial Implant Prostheses: How to Overcome Age-Related Changes in the Stomatognathic System" Prosthesis 6, no. 1: 119-134. https://doi.org/10.3390/prosthesis6010010
APA StyleDib Zakkour, J., Dib Zakkour, S., Montero, J., García-Cenador, B., Flores-Fraile, J., & Dib Zaitun, A. (2024). Digital Analysis of Occlusion in Fixed Partial Implant Prostheses: How to Overcome Age-Related Changes in the Stomatognathic System. Prosthesis, 6(1), 119-134. https://doi.org/10.3390/prosthesis6010010