
In Silico Analysis of the MitraClip in a Realistic Human Left Heart Model


Abstract
:1. Introduction
2. Materials and Methods
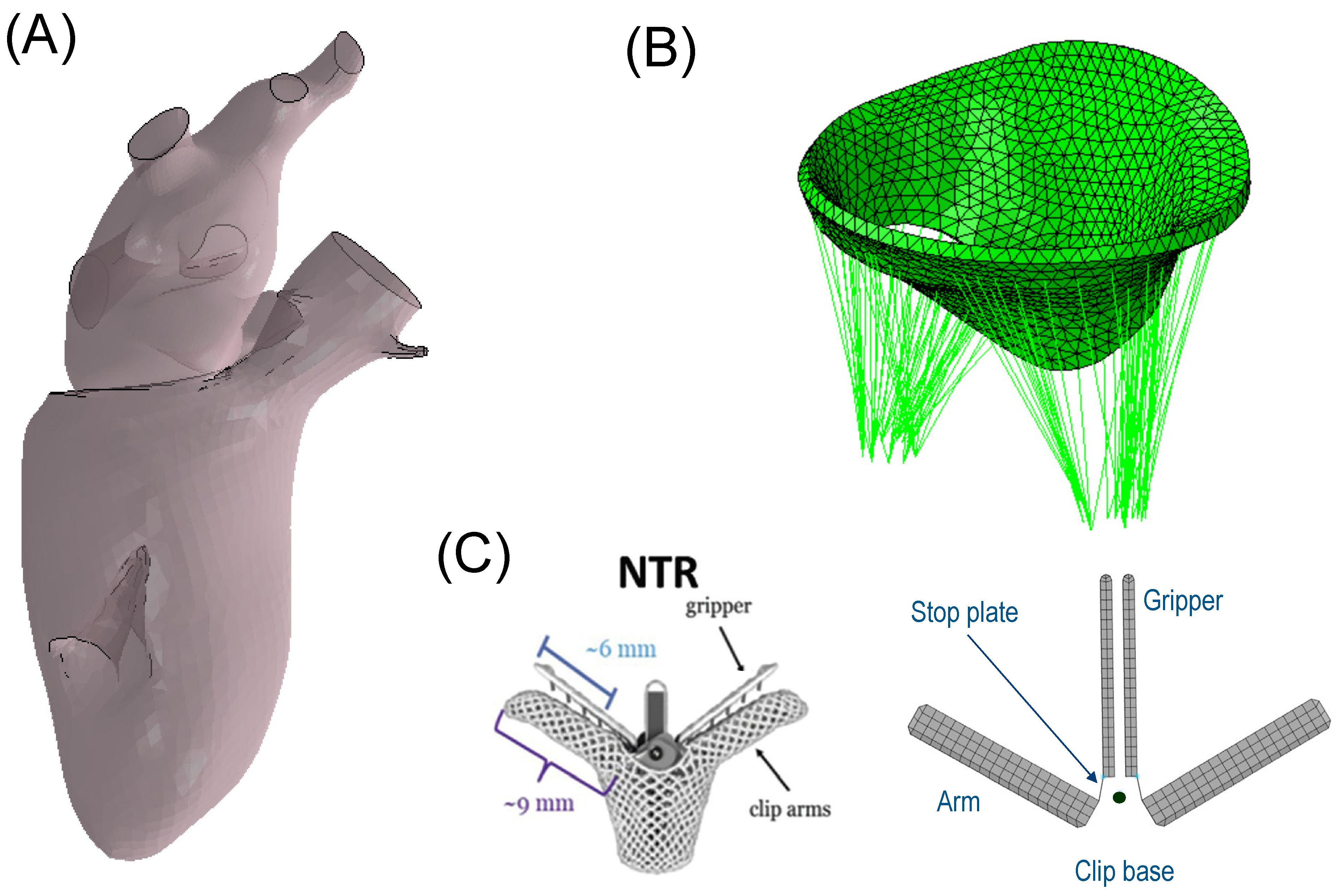
2.1. Left Heart and Mitral Valve Models
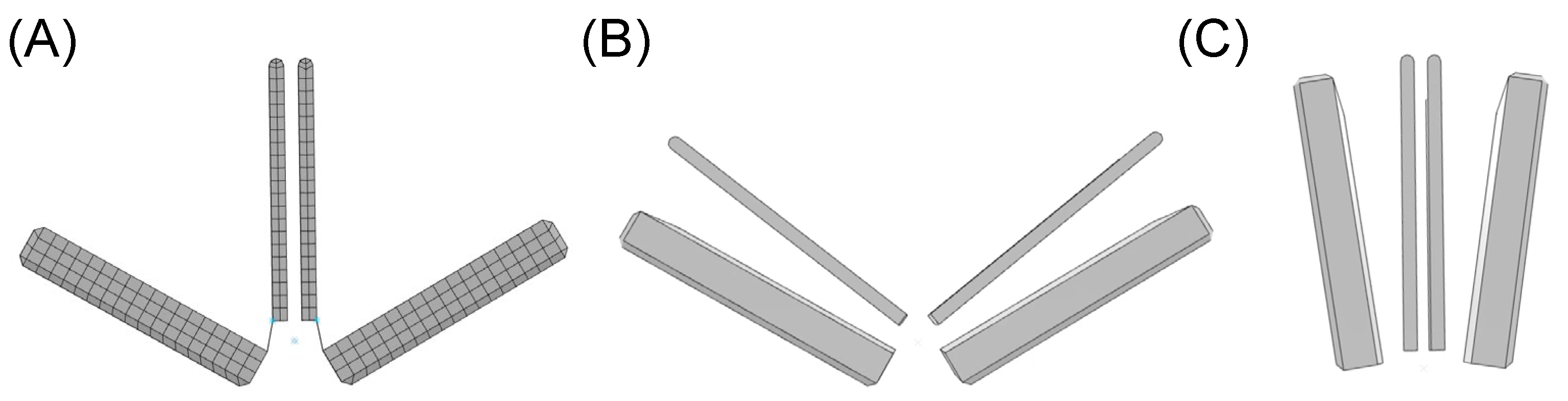
2.2. MitraClip Simulation
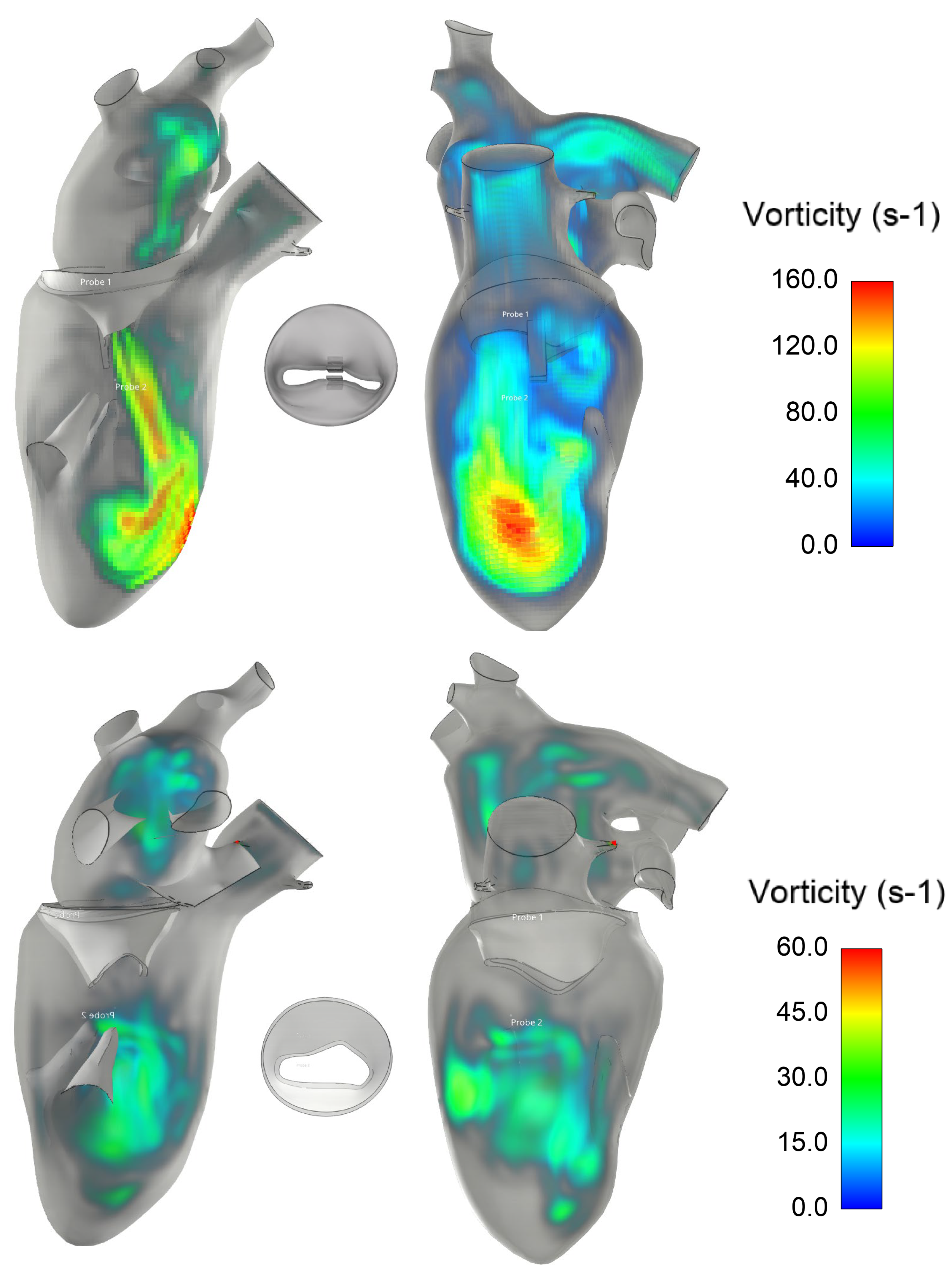
2.3. Post-MitraClip Flow Dynamic
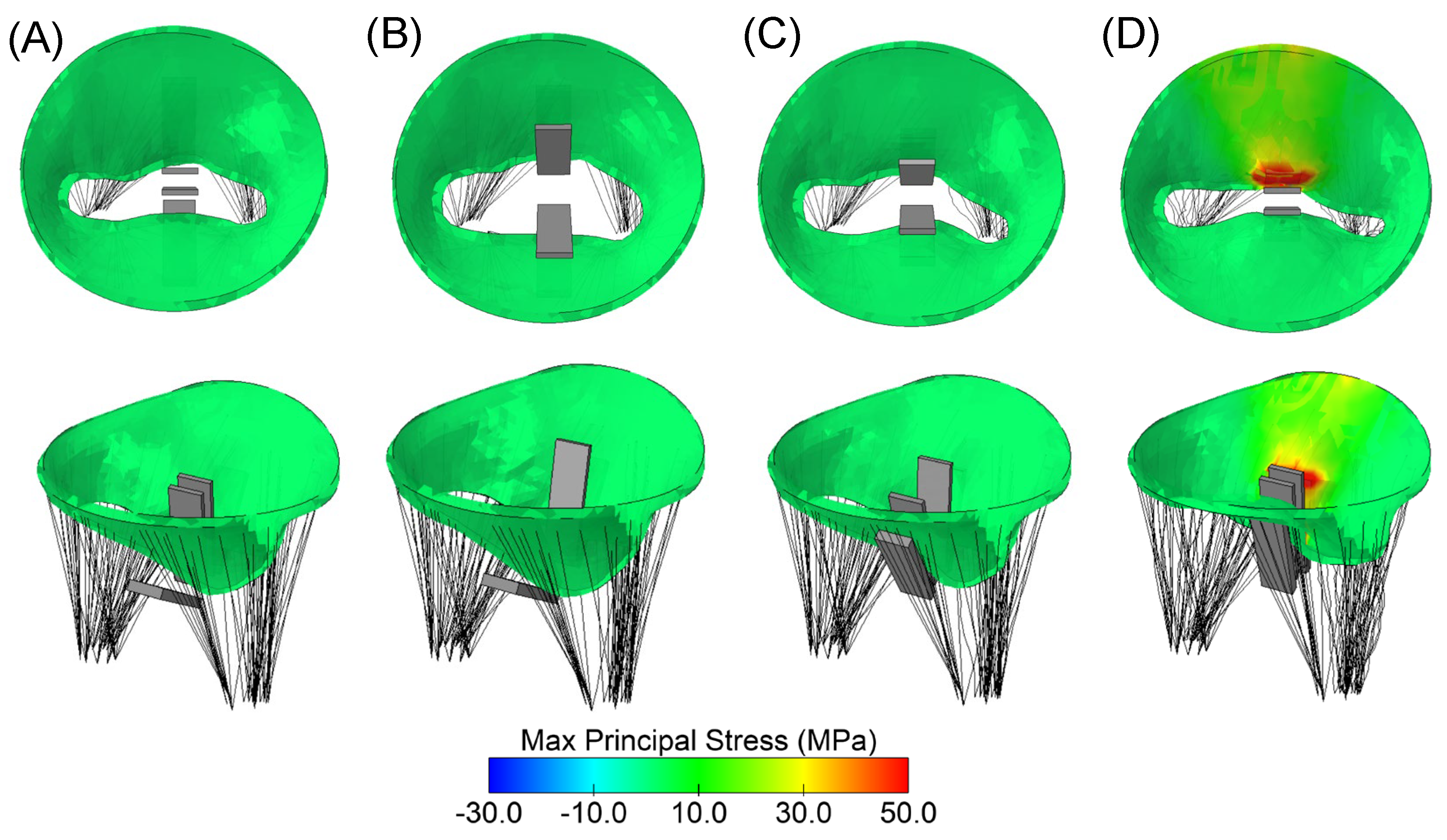
3. Results
4. Discussion
- MitraClip implantation leads to geometrical changes in the mitral valve, resulting in local maxima of principal stress in the regions of the valve leaflets that are constrained by the device.
- Hemodynamic disturbances are observed in the left ventricle after MitraClip implantation and are characterized by nested helical flow and vorticity in the superior apical region.
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Del Forno, B.; De Bonis, M.; Agricola, E.; Melillo, F.; Schiavi, D.; Castiglioni, A.; Montorfano, M.; Alfieri, O. Mitral valve regurgitation: A disease with a wide spectrum of therapeutic options. Nat. Rev. Cardiol. 2020, 17, 807–827. [Google Scholar] [CrossRef] [PubMed]
- Nkomo, V.T.; Gardin, J.M.; Skelton, T.N.; Gottdiener, J.S.; Scott, C.G.; Enriquez-Sarano, M. Burden of valvular heart diseases: A population-based study. Lancet 2006, 368, 1005–1011. [Google Scholar] [CrossRef] [PubMed]
- Mylotte, D.; Andalib, A.; Theriault-Lauzier, P.; Dorfmeister, M.; Girgis, M.; Alharbi, W.; Chetrit, M.; Galatas, C.; Mamane, S.; Sebag, I.; et al. Transcatheter heart valve failure: A systematic review. Eur. Heart J. 2015, 36, 1306–1327. [Google Scholar] [CrossRef] [PubMed]
- Feldman, T.; Kar, S.; Elmariah, S.; Smart, S.C.; Trento, A.; Siegel, R.J.; Apruzzese, P.; Fail, P.; Rinaldi, M.J.; Smalling, R.W.; et al. Randomized Comparison of Percutaneous Repair and Surgery for Mitral Regurgitation: 5-Year Results of EVEREST II. J. Am. Coll. Cardiol. 2015, 66, 2844–2854. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.W.; Lindenfeld, J.; Abraham, W.T.; Kar, S.; Lim, D.S.; Mishell, J.M.; Whisenant, B.; Grayburn, P.A.; Rinaldi, M.; Kapadia, S.R.; et al. Transcatheter Mitral-Valve Repair in Patients with Heart Failure. N. Engl. J. Med. 2018, 379, 2307–2318. [Google Scholar] [CrossRef]
- Grayburn, P.A.; Sannino, A.; Packer, M. Proportionate and Disproportionate Functional Mitral Regurgitation: A New Conceptual Framework That Reconciles the Results of the MITRA-FR and COAPT Trials. JACC. Cardiovasc. Imaging 2019, 12, 353–362. [Google Scholar] [CrossRef]
- Dowling, C.; Firoozi, S.; Brecker, S.J. First-in-Human Experience With Patient-Specific Computer Simulation of TAVR in Bicuspid Aortic Valve Morphology. JACC Cardiovasc. Interv. 2020, 13, 184–192. [Google Scholar] [CrossRef]
- Pasta, S.; Cannata, S.; Gentile, G.; Di Giuseppe, M.; Cosentino, F.; Pasta, F.; Agnese, V.; Bellavia, D.; Raffa, G.M.; Pilato, M.; et al. Simulation study of transcatheter heart valve implantation in patients with stenotic bicuspid aortic valve. Med. Biol. Eng. Comput. 2020, 58, 815–829. [Google Scholar] [CrossRef]
- Toma, M.; Einstein, D.R.; Kohli, K.; Caroll, S.L.; Bloodworth, C.H.t.; Cochran, R.P.; Kunzelman, K.S.; Yoganathan, A.P. Effect of Edge-to-Edge Mitral Valve Repair on Chordal Strain: Fluid-Structure Interaction Simulations. Biology 2020, 9, 173. [Google Scholar] [CrossRef]
- Toma, M.; Singh-Gryzbon, S.; Frankini, E.; Wei, Z.A.; Yoganathan, A.P. Clinical Impact of Computational Heart Valve Models. Materials 2022, 15, 3302. [Google Scholar] [CrossRef]
- Sacks, M.S.; Enomoto, Y.; Graybill, J.R.; Merryman, W.D.; Zeeshan, A.; Yoganathan, A.P.; Levy, R.J.; Gorman, R.C.; Gorman, J.H., 3rd. In-vivo dynamic deformation of the mitral valve anterior leaflet. Ann. Thorac. Surg. 2006, 82, 1369–1377. [Google Scholar] [CrossRef] [PubMed]
- Kamakoti, R.; Dabiri, Y.; Wang, D.D.; Guccione, J.; Kassab, G.S. Numerical Simulations of MitraClip Placement: Clinical Implications. Sci. Rep. 2019, 9, 15823. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, V.Y.; Morgan, A.E.; Kim, J.; Handschumacher, M.D.; Moskowitz, C.S.; Levine, R.A.; Ge, L.; Guccione, J.M.; Weinsaft, J.W.; et al. Mechanical effects of MitraClip on leaflet stress and myocardial strain in functional mitral regurgitation-A finite element modeling study. PLoS ONE 2019, 14, e0223472. [Google Scholar] [CrossRef]
- Hart, E.A.; De Bock, S.; De Beule, M.; Teske, A.J.; Chamuleau, S.A.J.; Voskuil, M.; Kraaijeveld, A.O. Transoesophageal echocardiography-based computational simulation of the mitral valve for MitraClip placement. Eurointerv. J. EuroPCR Collab. Work. Group Interv. Cardiol. Eur. Soc. Cardiol. 2019, 15, e239–e241. [Google Scholar] [CrossRef] [PubMed]
- Dabiri, Y.; Mahadevan, V.S.; Guccione, J.M.; Kassab, G.S. Machine learning used for simulation of MitraClip intervention: A proof-of-concept study. Front. Genet. 2023, 14, 1142446. [Google Scholar] [CrossRef]
- Cutugno, S.; Agnese, V.; Gentile, G.; Raffa, G.M.; Wisneski, A.D.; Guccione, J.M.; Pilato, M.; Pasta, S. Patient-Specific Analysis of Ascending Thoracic Aortic Aneurysm with the Living Heart Human Model. Bioengineering 2021, 8, 175. [Google Scholar] [CrossRef] [PubMed]
- Wisneski, A.D.; Wang, Y.; Deuse, T.; Hill, A.C.; Pasta, S.; Sack, K.L.; Yao, J.; Guccione, J.M. Impact of Aortic Stenosis on Myofiber Stress: Translational Application of Left Ventricle-Aortic Coupling Simulation. Front. Physiol. 2020, 11, 574211. [Google Scholar] [CrossRef] [PubMed]
- Holzapfel, G.A.; Ogden, R.W. Constitutive modelling of passive myocardium: A structurally based framework for material characterization. Philos. Trans. A. Math. Phys. Eng. Sci. 2009, 367, 3445–3475. [Google Scholar] [CrossRef]
- Walker, J.C.; Ratcliffe, M.B.; Zhang, P.; Wallace, A.W.; Hsu, E.W.; Saloner, D.A.; Guccione, J.M. Magnetic resonance imaging-based finite element stress analysis after linear repair of left ventricular aneurysm. J. Thorac. Cardiovasc. Surg. 2008, 135, 1094–1102.e2. [Google Scholar] [CrossRef]
- Wisneski, A.D.; Wang, Y.J.; Cutugno, S.; Pasta, S.; Stroh, A.; Yao, J.; Nguyen, T.C.; Mahadevan, V.S.; Guccione, J.M. Left Ventricle Biomechanics of Low-Flow, Low-Gradient Aortic Stenosis: A Patient-Specific Computational Model. Front. Physiol. 2022, 13, 848011. [Google Scholar] [CrossRef]
- Sommer, G.; Schriefl, A.J.; Andra, M.; Sacherer, M.; Viertler, C.; Wolinski, H.; Holzapfel, G.A. Biomechanical properties and microstructure of human ventricular myocardium. Acta Biomater. 2015, 24, 172–192. [Google Scholar] [CrossRef] [PubMed]
- Di Giuseppe, M.; Alotta, G.; Agnese, V.; Bellavia, D.; Raffa, G.M.; Vetri, V.; Zingales, M.; Pasta, S.; Pilato, M. Identification of circumferential regional heterogeneity of ascending thoracic aneurysmal aorta by biaxial mechanical testing. J. Mol. Cell Cardiol. 2019, 130, 205–215. [Google Scholar] [CrossRef]
- Palit, A.; Bhudia, S.K.; Arvanitis, T.N.; Turley, G.A.; Williams, M.A. In vivo estimation of passive biomechanical properties of human myocardium. Med. Biol. Eng. Comput. 2018, 56, 1615–1631. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.C.; Ratcliffe, M.B.; Zhang, P.; Wallace, A.W.; Fata, B.; Hsu, E.W.; Saloner, D.; Guccione, J.M. MRI-based finite-element analysis of left ventricular aneurysm. Am. J. Physiol. Heart Circ. Physiol. 2005, 289, H692–H700. [Google Scholar] [CrossRef]
- Genet, M.; Lee, L.C.; Nguyen, R.; Haraldsson, H.; Acevedo-Bolton, G.; Zhang, Z.H.; Ge, L.; Ordovas, K.; Kozerke, S.; Guccione, J.M. Distribution of normal human left ventricular myofiber stress at end diastole and end systole: A target for in silico design of heart failure treatments. J. Appl. Physiol. 2014, 117, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Gee, M.W.; Forster, C.; Wall, W.A. A computational strategy for prestressing patient-specific biomechanical problems under finite deformation. Int. J. Numer. Methods Biomed. Eng. 2010, 26, 52–72. [Google Scholar] [CrossRef]
- Pashakhanloo, F.; Herzka, D.A.; Ashikaga, H.; Mori, S.; Gai, N.; Bluemke, D.A.; Trayanova, N.A.; McVeigh, E.R. Myofiber Architecture of the Human Atria as Revealed by Submillimeter Diffusion Tensor Imaging. Circ. Arrhythm. Electrophysiol. 2016, 9, e004133. [Google Scholar] [CrossRef] [PubMed]
- May-Newman, K.; Yin, F.C. Biaxial mechanical behavior of excised porcine mitral valve leaflets. Am. J. Physiol. 1995, 269, H1319–H1327. [Google Scholar] [CrossRef] [PubMed]
- Zuo, K.; Pham, T.; Li, K.; Martin, C.; He, Z.; Sun, W. Characterization of biomechanical properties of aged human and ovine mitral valve chordae tendineae. J. Mech. Behav. Biomed. Mater. 2016, 62, 607–618. [Google Scholar] [CrossRef]
- Fratini, L.; Pasta, S. Residual stresses in friction stir welded parts of complex geometry. Int. J. Adv. Manuf. Tech. 2012, 59, 547–557. [Google Scholar] [CrossRef]
- Morany, A.; Lavon, K.; Bardon, R.G.; Kovarovic, B.; Hamdan, A.; Bluestein, D.; Haj-Ali, R. Fluid-structure interaction modeling of compliant aortic valves using the lattice Boltzmann CFD and FEM methods. Biomech. Model. Mechanobiol. 2023, 22, 837–850. [Google Scholar] [CrossRef] [PubMed]
- Scardulla, F.; Pasta, S.; D’Acquisto, L.; Sciacca, S.; Agnese, V.; Vergara, C.; Quarteroni, A.; Clemenza, F.; Bellavia, D.; Pilato, M. Shear stress alterations in the celiac trunk of patients with a continuous-flow left ventricular assist device as shown by in-silico and in-vitro flow analyses. J. Heart Lung. Transplant. 2017, 36, 906–913. [Google Scholar] [CrossRef]
- D’Ancona, G.; Amaducci, A.; Rinaudo, A.; Pasta, S.; Follis, F.; Pilato, M.; Baglini, R. Haemodynamic predictors of a penetrating atherosclerotic ulcer rupture using fluid-structure interaction analysis. Interact. Cardiovasc. Thorac. Surg. 2013, 17, 576–578. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, F.; Agnese, V.; Raffa, G.M.; Gentile, G.; Bellavia, D.; Zingales, M.; Pilato, M.; Pasta, S. On the role of material properties in ascending thoracic aortic aneurysms. Comput. Biol. Med. 2019, 109, 70–78. [Google Scholar] [CrossRef]
- Catalano, C.; Pasta, S. On the Modeling of Transcatheter Therapies for the Aortic and Mitral Valves: A Review. Prosthesis 2022, 4, 102–112. [Google Scholar] [CrossRef]
- Zhong, Q.; Zeng, W.; Huang, X.; Zhao, X. Finite element analysis for edge-to-edge technique to treat post-mitral valve repair systolic anterior motion. Acta Bioeng. Biomech. 2014, 16, 3–12. [Google Scholar]
- Pasta, S.; Catalano, C.; Cannata, S.; Guccione, J.M.; Gandolfo, C. Numerical simulation of transcatheter mitral valve replacement: The dynamic implication of LVOT obstruction in the valve-in-ring case. J. Biomech. 2022, 144, 111337. [Google Scholar] [CrossRef]
- Pasta, S.; Gandolfo, C. Pre-Operative Modeling of Transcatheter Mitral Valve Replacement in a Surgical Heart Valve Bioprosthesis. Prosthesis 2020, 2, 39–45. [Google Scholar] [CrossRef]
- Catalano, C.; Cannata, S.; Agnese, V.; Gentile, G.; Gandolfo, C.; Pasta, S. On the spectrum of transcatheter mitral valve replacement: In silico and in vitro assessment of neo-LVOT area in ViR, ViV and ViMAC. Bioprinting 2023, 32, e00285. [Google Scholar] [CrossRef]
- Morgan, A.E.; Wozniak, C.J.; Gulati, S.; Ge, L.; Grossi, E.A.; Weinsaft, J.W.; Ratcliffe, M.B. Association of Uneven MitraClip Application and Leaflet Stress in a Finite Element Model. JAMA Surg. 2017, 152, 111–114. [Google Scholar] [CrossRef]
- Mansi, T.; Voigt, I.; Assoumou Mengue, E.; Ionasec, R.; Georgescu, B.; Noack, T.; Seeburger, J.; Comaniciu, D. Towards patient-specific finite-element simulation of MitralClip procedure. Med. Image Comput. Comput.-Assist. Interv. MICCAI Int. Conf. Med. Image Comput. Comput. Assist. Interv. 2011, 14, 452–459. [Google Scholar] [CrossRef]
- Sturla, F.; Ronzoni, M.; Vitali, M.; Dimasi, A.; Vismara, R.; Preston-Maher, G.; Burriesci, G.; Votta, E.; Redaelli, A. Impact of different aortic valve calcification patterns on the outcome of transcatheter aortic valve implantation: A finite element study. J. Biomech. 2016, 49, 2520–2530. [Google Scholar] [CrossRef] [PubMed]
- Sack, K.L.; Dabiri, Y.; Franz, T.; Solomon, S.D.; Burkhoff, D.; Guccione, J.M. Investigating the Role of Interventricular Interdependence in Development of Right Heart Dysfunction During LVAD Support: A Patient-Specific Methods-Based Approach. Front. Physiol. 2018, 9, 520. [Google Scholar] [CrossRef]
- Sturla, F.; Vismara, R.; Jaworek, M.; Votta, E.; Romitelli, P.; Pappalardo, O.A.; Lucherini, F.; Antona, C.; Fiore, G.B.; Redaelli, A. In vitro and in silico approaches to quantify the effects of the Mitraclip((R)) system on mitral valve function. J. Biomech. 2017, 50, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Caballero, A.; Mao, W.; McKay, R.; Hahn, R.T.; Sun, W. A Comprehensive Engineering Analysis of Left Heart Dynamics After MitraClip in a Functional Mitral Regurgitation Patient. Front. Physiol. 2020, 11, 432. [Google Scholar] [CrossRef]
- Maor, E.; Raphael, C.E.; Panaich, S.S.; Reeder, G.S.; Nishimura, R.A.; Nkomo, V.T.; Rihal, C.S.; Eleid, M.F. Acute Changes in Left Atrial Pressure After MitraClip Are Associated With Improvement in 6-Minute Walk Distance. Circulation. Cardiovasc. Interv. 2017, 10, e004856. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| a (MPa) | b | af (MPa) | bf | as (MPa) | bs | afs (MPa) | bfs | Ca0 (μmol/L) | |
|---|---|---|---|---|---|---|---|---|---|
| Mitral Valve | 8.7e−4 | 2.7 | 5.0e−4 | 12.0 | 3.8e−3 | 7.6e−1 | 3.8e−3 | 7.6e−1 | |
| Left ventricle | 4.0e−1 | 12.0 | 5.0e−1 | 5.0 | 2.0e−1 | 2.0 | 1.1e−2 | 2.0 | 2.66 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pasta, S. In Silico Analysis of the MitraClip in a Realistic Human Left Heart Model. Prosthesis 2023, 5, 876-887. https://doi.org/10.3390/prosthesis5030061
Pasta S. In Silico Analysis of the MitraClip in a Realistic Human Left Heart Model. Prosthesis. 2023; 5(3):876-887. https://doi.org/10.3390/prosthesis5030061
Chicago/Turabian StylePasta, Salvatore. 2023. "In Silico Analysis of the MitraClip in a Realistic Human Left Heart Model" Prosthesis 5, no. 3: 876-887. https://doi.org/10.3390/prosthesis5030061
APA StylePasta, S. (2023). In Silico Analysis of the MitraClip in a Realistic Human Left Heart Model. Prosthesis, 5(3), 876-887. https://doi.org/10.3390/prosthesis5030061