
Conventional versus Digital Dental Impression Techniques: What Is the Future? An Umbrella Review

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol
- P—Population: subjects with dental implants or natural stumps on which precision impressions must be taken digitally or traditionally.
- E—Exposure: dental impressions made using an intra-oral scanner were compared to analog impressions made with high-precision impression materials in prosthetic dentistry.
- O—Outcomes: accuracy, time of digital impressions, and patient preference in comparison to those of high-precision conventional impressions in vivo.
2.2. Search Strategy
(‘digital impression’ OR ‘intraoral digital impression’ OR ‘intraoral scanner’ OR ‘intraoral digital scanner’ OR ‘conventional impression’ OR ‘accuracy’)
(‘prosthetic dentistry’ OR ‘prosthetic’ OR ‘dentistry’ OR ‘dental prosthesis’ OR ‘implant prosthesis’)
2.3. Study Selection and Eligibility Criteria
- Reviews with or without metanalysis that compare digital and conventional impressions in prosthetic dentistry that include in vivo studies.
- Systematic review with or without metanalysis
- Reviews published in the last 10 years ago
- Reviews published in the English language.
- Reviews with or without metanalysis that compare digital impressions and conventional impressions in prosthetic dentistry that include only in vitro studies.
- Clinical studies
- Reviews published more than 10 years ago.
- Reviews not published in the English language.
2.4. Data Extraction and Collection
- ○
- First, author of the journal, year of publication, kind of journal, funding, and quality of the study.
- ○
- Number and design of studies included in each systematic review, population, and sample size.
- ○
- Accuracy, preference patience, and accuracy among conventional and digital impressions.
- ○
- Main outcomes
- ○
- conclusions
2.5. Data Synthesis
2.6. Quality Assessment
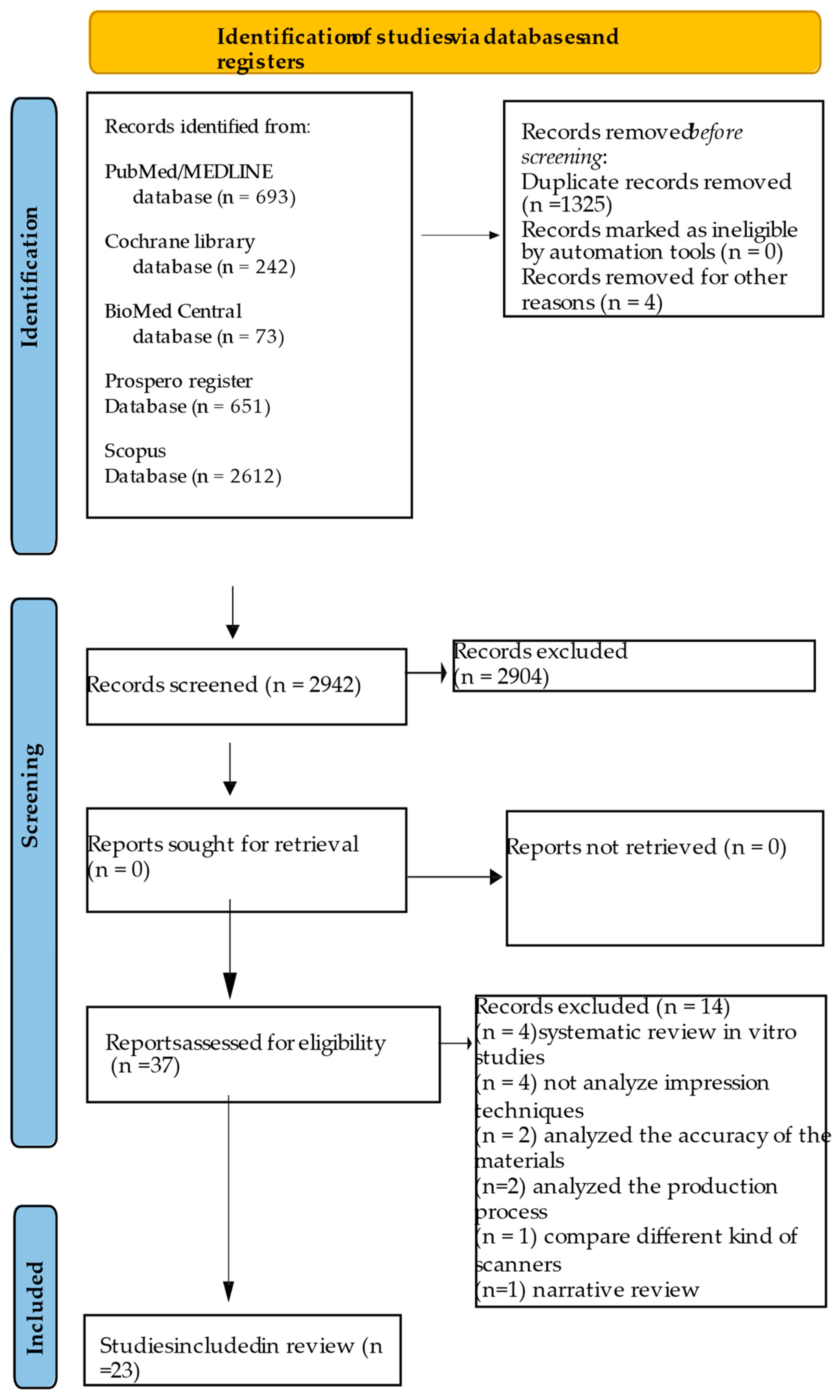
3. Results
3.1. Study Selection
3.2. Study Characteristics and Qualitative Synthesis
3.3. Digital vs. Conventional Outcome: Time
3.4. Digital vs. Conventional Outcome: Patience Preference
3.5. Digital vs. Conventional Outcome: Accuracy
3.6. Quality Assessment
4. Discussion
4.1. Accuracy
4.2. Impression Time
4.3. Patient Preferences
4.4. Clinical Considerations
4.4.1. Clinical Considerations for Dental Impressions
4.4.2. Clinical Considerations for Implant Impressions
4.5. Limitations of the Study and Distorted Quality of the Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pant, R.; Juszczyk, A.S.; Clark, R.K.; Radford, D.R. Long-term dimensional stability, and reproduction of surface detail of four polyvinyl siloxane duplicating materials. J. Dent. 2008, 36, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Donovan, T.E.; Chee, W.W. A review of contemporary impression materials and techniques. Dent. Clin. North. Am. 2004, 48, 445–470. [Google Scholar] [CrossRef] [PubMed]
- Chee, W.W.; Donovan, T.E. Polyvinyl siloxane impression materials: A review of properties and techniques. J.Prosthet. Dent. 1992, 68, 728–732. [Google Scholar] [CrossRef]
- Hacker, T.; Heydecke, G.; Reissmann, D.R. Impact of procedures during prosthodontic treatment on patients’ perceived burdens. J. Dent. 2015, 43, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Conny, D.J.; Tedesco, L.A.; Brewer, J.D.; Albino, J.E. Changes of attitude in fixed prosthodontic patients. J. Prosthet. Dent. 1985, 53, 451–454. [Google Scholar] [CrossRef]
- Schropp, L.; Wenzel, A.; Kostopoulos, L.; Karring, T. Bone healing and soft tissue contour changes following single-tooth extraction: A clinical and radiographic 12-month prospective study. Int. J. Periodontics Restor. Dent. 2003, 23, 313–323. [Google Scholar]
- Tsirogiannis, P.; Neophytou, S.; Reul, A.; Heydecke, G.; Reissmann, D.R. Can we measure patients’ perception during dental impressions? The Burdens in Dental Impression-Making Questionnaire—BiDIM-Q. J. Prosthodont. Res. 2017, 61, 34–42. [Google Scholar] [CrossRef]
- Lee, S.J.; Gallucci, G.O. Digital vs. conventional implant impressions: Efficiency outcomes. Clin. Oral Implant. Res. 2013, 24, 111–115. [Google Scholar] [CrossRef]
- Schepke, U.; Meijer, H.J.; Kerdijk, W.; Cune, M.S. Digital versus analog complete-arch impressions for single-unit premolar implant crowns: Operating time and patient preference. J. Prosthet. Dent. 2015, 114, 403–406.e1. [Google Scholar] [CrossRef] [PubMed]
- Gjelvold, B.; Chrcanovic, B.R.; Korduner, E.K.; Collin-Bagewitz, I.; Kisch, J. Intraoral digital impression technique compared to conventional impression technique. A randomized clinical trial. J. Prosthodont. 2016, 25, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Joda, T.; Bragger, U. Patient-centered outcomes comparing digital and conventional implant impression procedures: A randomized crossover trial. Clin. Oral Implant. Res. 2016, 27, e185–e189. [Google Scholar] [CrossRef]
- Haddadi, Y.; Bahrami, G.; Isidor, F. Evaluation of operating time and patient perception using conventional impression taking and intraoral scanning for crown manufacture: A split-mouth, randomized clinical study. Int. J. Prosthodont. 2018, 31, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Guo, D.N.; Liu, Y.S.; Pan, S.X.; Wang, P.F.; Wang, B.; Liu, J.Z.; Gao, W.H.; Zhou, Y.S. Clinical efficiency and patient preference of immediate digital impression after implant placement for single implant-supported crown. Chin. J. Dent. Res. 2019, 22, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Sailer, I.; Muhlemann, S.; Fehmer, V.; Hammerle, C.H.F.; Benic, G.I. Randomized controlled clinical trial of digital and conventional workflows for the fabrication of zirconia-ceramic fixed partial dentures. Part I: Time efficiency of complete-arch digital scans versus conventional impressions. J. Prosthet. Dent. 2019, 121, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Di Fiore, A.; Vigolo, P.; Graiff, L.; Stellini, E. Digital vs. Conventional workflow for screw-retained single-implant crowns: A comparison of key considerations. Int. J. Prosthodont. 2018, 31, 577–579. [Google Scholar] [CrossRef]
- Lee, S.J.; Jamjoom, F.Z.; Le, T.; Radics, A.; Gallucci, G.O. A clinical study comparing digital scanning and conventional impression making for implant-supported prostheses: A crossover clinical trial. J. Prosthet. Dent. 2021, 128, 42–48. [Google Scholar] [CrossRef]
- Marghalani, A.; Weber, H.P.; Finkelman, M.; Kudara, Y.; El Rafie, K.; Papaspyridakos, P. Digital versus conventional implant impressions for partially edentulous arches: An evaluation of accuracy. J. Prosthet. Dent. 2018, 119, 574–579. [Google Scholar] [CrossRef] [PubMed]
- Muhlemann, S.; Benic, G.I.; Fehmer, V.; Hammerle, C.H.F.; Sailer, I. Randomized controlled clinical trial of digital and conventional workflows for the fabrication of zirconia-ceramic posterior fixed partial dentures. Part II: Time efficiency of CAD-CAM versus conventional laboratory procedures. J. Prosthet. Dent. 2019, 121, 252–257. [Google Scholar] [CrossRef]
- Joda, T.; Bragger, U.; Zitzmann, N.U. CAD/CAM implant crowns in a digital workflow: Five-year follow-up of a prospective clinical trial. Clin. Implant. Dent. Relat. Res. 2019, 21, 169–174. [Google Scholar] [CrossRef]
- Joda, T.; Bragger, U. Time-efficiency analysis comparing digital and conventional workflows for implant crowns: A prospective clinical crossover trial. Int. J. Oral Maxillofac. Implant. 2015, 30, 1047–1053. [Google Scholar] [CrossRef]
- Ender, A.; Zimmermann, M.; Attin, T.; Mehl, A. In vivo precision of conventional and digital methods for obtaining quadrant dental impressions. Clin. Oral Investig. 2016, 20, 1495–1504. [Google Scholar] [CrossRef] [PubMed]
- Abduo, J.; Elseyoufi, M. Accuracy of intraoral scanners: A systematic review of influencing factors. Eur. J. Prosthodont. Restor. Dent. 2018, 26, 101–121. [Google Scholar] [CrossRef]
- Revilla-Leon, M.; Subramanian, S.G.; Ozcan, M.; Krishnamurthy, V.R. Clinical study of the influence of ambient light scanning conditions on the accuracy (trueness and precision) of an intraoral scanner. J. Prosthodont. 2020, 29, 107–113. [Google Scholar] [CrossRef]
- Kim, J.; Park, J.M.; Kim, M.; Heo, S.J.; Shin, I.H.; Kim, M. Comparison of experience curves between two 3-dimensional intraoral scanners. J. Prosthet. Dent. 2016, 116, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Lyu, P.; Wang, Y.; Sun, Y. Influence of object translucency on the scanning accuracy of a powder-free intraoral scanner: A laboratory study. J. Prosthet. Dent. 2017, 117, 93–101. [Google Scholar] [CrossRef]
- Sakornwimon, N.; Leevailoj, C. Clinical marginal fit of zirconia crowns and patients’ preferences for impression techniques using intraoral digital scanner versus polyvinyl siloxane material. J. Prosthet. Dent. 2017, 118, 386–391. [Google Scholar] [CrossRef]
- Punj, A.; Bompolaki, D.; Garaicoa, J. Dental Impression Materials and Techniques. Dent. Clin. N. Am. 2017, 61, 779–796. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, T.; Hotta, Y.; Kunii, J.; Kuriyama, S.; Tamaki, Y. A review of dental CAD/CAM: Status and future perspectives from 20 years of experience. Dent. Mater. J. 2009, 28, 44–56. [Google Scholar] [CrossRef]
- Khan, L.K.; Kunz, R.; Kleijnen, J.; Antes, G. Systematic reviews to support evidence-based medicine. How to review and apply findings of healthcare research. Kahn, K.S.; Kunz, R.; Kleijnen J, Antes, G.170 × 240 mm. Pp.136. Illustrated.2003. Royal Society of Medicine Press: London, UK. Br. J. Surg. 2004, 91, 375. [Google Scholar]
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S. The well-built clinical question: A key to evidence-based decisions. ACPJ Club 1995, 123, 12–13. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, 4008. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.; Abbasi, M.S.; Haider, S.; Ahmed, N.; Habib, S.R.; Altamash, S.; Zafar, M.S.; Alam, M.K. Fit Accuracy of Removable Partial Denture Frameworks Fabricated with CAD/CAM, Rapid Prototyping, and Conventional Techniques: A Systematic Review. Biomed. Res. Int. 2021, 2021, 3194433. [Google Scholar] [CrossRef]
- Aragón, M.L.; Pontes, L.F.; Bichara, L.M.; Flores-Mir, C.; Normando, D. Validity and reliability of intraoral scanners compared to conventional gypsum models measurements: A systematic review. Eur. J. Orthod. 2016, 38, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Albanchez-González, M.I.; Brinkmann, J.C.; Peláez-Rico, J.; López-Suárez, C.; Rodríguez-Alonso, V.; Suárez-García, M.J. Accuracy of Digital Dental Implants Impression Taking with Intraoral Scanners Compared with Conventional Impression Techniques: A Systematic Review of In Vitro Studies. Int. J. Environ. Res. Public. Health. 2022, 19, 2026. [Google Scholar] [CrossRef] [PubMed]
- Chochlidakis, K.M.; Papaspyridakos, P.; Geminiani, A.; Chen, C.J.; Feng, I.J.; Ercoli, C. Digital versus conventional impressions for fixed prosthodontics: A systematic review and meta-analysis. J. Prosthet. Dent. 2016, 116, 184–190.e12. [Google Scholar] [CrossRef] [PubMed]
- Kustrzycka, D.; Marschang, T.; Mikulewicz, M.; Grzebieluch, W. Comparison of the Accuracy of 3D Images Obtained fromDifferent Types of Scanners: A Systematic Review. J. Healthc. Eng. 2020, 2020, 8854204. [Google Scholar] [CrossRef] [PubMed]
- Mühlemann, S.; Kraus, R.D.; Hämmerle, C.H.F.; Thoma, D.S. Is the use of digital technologies for the fabrication of implant-supported reconstructions more efficient and/or more effective than conventional techniques: A systematic review. Clin. Oral Implant. Res. 2018, 29 (Suppl. S18), 184–195. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.; Gandolfi, A.; Luongo, G.; Logozzo, S. Intraoral scanners in dentistry: A review of the current literature. BMC Oral Health 2017, 17, 149. [Google Scholar] [CrossRef]
- Tabesh, M.; Nejatidanesh, F.; Savabi, G.; Davoudi, A.; Savabi, O. Marginal Accuracy of Lithium Disilicate Full-Coverage Single Crowns Made by Direct and Indirect Digital or Conventional Workflows: A Systematic Review and Meta-Analysis. J. Prosthodont. 2022, 31, 744–753. [Google Scholar] [CrossRef] [PubMed]
- Morsy, N.; El Kateb, M.; Azer, A.; Fathalla, S. Fit of zirconia fixed partial dentures fabricated from conventional impressions and digital scans: A systematic review and meta-analysis. J. Prosthet. Dent. 2021, 130, 28–34. [Google Scholar] [CrossRef]
- Valenti, C.; Isabella Federici, M.; Masciotti, F.; Marinucci, L.; Xhimitiku, I.; Cianetti, S.; Pagano, S. Mechanical properties of 3D-printed prosthetic materials compared with milled and conventional processing: A systematic review and meta-analysis of in vitro studies. J. Prosthet. Dent. 2022; in press. [Google Scholar] [CrossRef]
- Parize, H.; Dias Corpa Tardelli, J.; Bohner, L.; Sesma, N.; Muglia, V.A.; Cândido Dos Reis, A. Digital versus conventional workflow for the fabrication of physical casts for fixed prosthodontics: A systematic review of accuracy. J. Prosthet. Dent. 2022, 128, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Li, H. Accuracy of CAD-CAM milling versus conventional lost-wax casting for single metal copings: A systematic review and meta-analysis. J. Prosthet. Dent. 2022, in press. [CrossRef] [PubMed]
- Mai, H.Y.; Mai, H.N.; Kim, H.J.; Lee, J.; Lee, D.H. Accuracy of removable partial denture metal frameworks fabricated by computer-aided design/computer-aided manufacturing method: A systematic review and meta-analysis. J. Evid. Based Dent. Pract. 2022, 22, 101681. [Google Scholar] [CrossRef]
- Cicciù, M.; Fiorillo, L.; D’Amico, C.; Gambino, D.; Amantia, E.M.; Laino, L.; Crimi, S.; Campagna, P.; Bianchi, A.; Herford, A.S.; et al. 3D Digital Impression Systems Compared with Traditional Techniques in Dentistry: A Recent Data Systematic Review. Materials 2020, 13, 1982. [Google Scholar] [CrossRef]
- Sivaramakrishnan, G.; Alsobaiei, M.; Sridharan, K. Patient preference and operating time for digital versus conventional impressions: A network meta-analysis. Aust. Dent. J. 2020, 65, 58–69. [Google Scholar] [CrossRef] [PubMed]
- Flügge, T.; Van der Meer, W.J.; Gonzalez, B.G.; Vach, K.; Wismeijer, D.; Wang, P. The accuracy of different dental impression techniques for implant-supported dental prostheses: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29 (Suppl. S16), 374–392. [Google Scholar] [CrossRef]
- De Oliveira, N.R.C.; Pigozzo, M.N.; Sesma, N.; Laganá, D.C. Clinical efficiency and patient preference of digital and conventional workflow for single implant crowns using immediate and regular digital impression: A meta-analysis. Clin. Oral Implant. Res. 2020, 31, 669–686. [Google Scholar] [CrossRef] [PubMed]
- Alikhasi, M.; Alsharbaty, M.H.M.; Moharrami, M. Digital Implant Impression Technique Accuracy: A Systematic Review. Implant. Dent. 2017, 26, 929–935. [Google Scholar] [CrossRef] [PubMed]
- Giachetti, L.; Sarti, C.; Cinelli, F.; Russo, D.S. Accuracy of Digital Impressions in Fixed Prosthodontics: A Systematic Review of Clinical Studies. Int. J. Prosthodont. 2020, 33, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Hasanzade, M.; Shirani, M.; Afrashtehfar, K.I.; Naseri, P.; Alikhasi, M. In Vivo and In Vitro Comparison of Internal and Marginal Fit of Digital and Conventional Impressions for Full-Coverage Fixed Restorations: A Systematic Review and Meta-analysis. J. Evid. Based Dent. Pract. 2019, 19, 236–254. [Google Scholar] [CrossRef]
- Nagarkar, S.R.; Perdigão, J.; Seong, W.J.; Theis-Mahon, N. Digital versus conventional impressions for full-coverage restorations: A systematic review and meta-analysis. J. Am. Dent. Assoc. 2018, 149, 139–147.e1. [Google Scholar] [CrossRef]
- Gallardo, Y.R.; Bohner, L.; Tortamano, P.; Pigozzo, M.N.; Laganá, D.C.; Sesma, N. Patient outcomes and procedure working time for digital versus conventional impressions: A systematic review. J. Prosthet. Dent. 2018, 119, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Tabesh, M.; Nejatidanesh, F.; Savabi, G.; Davoudi, A.; Savabi, O.; Mirmohammadi, H. Marginal adaptation of zirconia complete-coverage fixed dental restorations made from digital scans or conventional impressions: A systematic review and meta-analysis. J. Prosthet. Dent. 2021, 125, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Hasanzade, M.; Aminikhah, M.; Afrashtehfar, K.I.; Alikhasi, M. Marginal and internal adaptation of single crowns and fixed dental prostheses by using digital and conventional workflows: A systematic review and meta-analysis. J. Prosthet. Dent. 2021, 126, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Bandiaky, O.N.; Le Bars, P.; Gaudin, A.; Hardouin, J.B.; Cheraud-Carpentier, M.; Mbodj, E.B.; Soueidan, A. Comparative assessment of complete-coverage, fixed tooth-supported prostheses fabricated from digital scans or conventional impressions: A systematic review and meta-analysis. J. Prosthet. Dent. 2022, 127, 71–79. [Google Scholar] [CrossRef] [PubMed]
- García-Gil, I.; Cortés-Bretón-Brinkmann, J.; Jiménez-García, J.; Peláez-Rico, J.; Suárez-García, M.J. Precision and practical usefulness of intraoral scanners in implant dentistry: A systematic literature review. J. Clin. Exp. Dent. 2020, 12, e784–e793. [Google Scholar] [CrossRef] [PubMed]
- Papaspyridakos, P.; Chen, C.J.; Gallucci, G.O.; Doukoudakis, A.; Weber, H.P.; Chronopoulos, V. Accuracy of implant impressions for partially and completely edentulous patients: A systematic review. Int. J. Oral Maxillofac. Implant. 2014, 29, 836–845. [Google Scholar] [CrossRef] [PubMed]
- Ahlholm, P.; Sipilä, K.; Vallittu, P.; Jakonen, M.; Kotiranta, U. Digital Versus Conventional Impressions in Fixed Prosthodontics: A Review. J. Prosthodont. 2018, 27, 35–41. [Google Scholar] [CrossRef]
- Papaspyridakos, P.; Vazouras, K.; Chen, Y.W.; Kotina, E.; Natto, Z.; Kang, K.; Chochlidakis, K. Digital vs Conventional Implant Impressions: A Systematic Review and Meta-Analysis. J. Prosthodont. 2020, 29, 660–678. [Google Scholar] [CrossRef]
- Siqueira, R.; Galli, M.; Chen, Z.; Mendonça, G.; Meirelles, L.; Wang, H.L.; Chan, H.L. Intraoral scanning reduces procedure time and improves patient comfort in fixed prosthodontics and implant dentistry: A systematic review. Clin. Ora.l Investig. 2021, 25, 6517–6531. [Google Scholar] [CrossRef]
- Joda, T.; Zarone, F.; Ferrari, M. The complete digital workflow in fixed prosthodontics: A systematic review. BMC Oral Health. 2017, 17, 124. [Google Scholar] [CrossRef]
- De Paris Matos, T.; Wambier, L.M.; Favoreto, M.W.; Rezende, C.E.E.; Reis, A.; Loguercio, A.D.; Gonzaga, C.C. Patient-related outcomes of conventional impression making versus intraoral scanning for prosthetic rehabilitation: A systematic review and meta-analysis. J. Prosthet. Dent. 2021, 130, 19–27. [Google Scholar] [CrossRef]
- Schmidt, A.; Wöstmann, B.; Schlenz, M.A. Accuracy of digital implant impressions in clinical studies: A systematic review. Clin. Oral Implant. Res. 2022, 33, 573–585. [Google Scholar] [CrossRef] [PubMed]
- Manicone, P.F.; De Angelis, P.; Rella, E.; Damis, G.; D’Addona, A. Patient preference and clinical working time between digital scanning and conventional impression making for implant-supported prostheses: A systematic review and meta-analysis. J. Prosthet. Dent. 2022, 128, 589–596. [Google Scholar] [CrossRef]
- Kong, L.; Li, Y.; Liu, Z. Digital versus conventional full-arch impressions in linear and 3D accuracy: A systematic review and meta-analysis of in vivo studies. Clin. Oral Investig. 2022, 26, 5625–5642. [Google Scholar] [CrossRef]
- Bishti, S.; Tuna, T.; Rittich, A.; Wolfart, S. Patient-reported outcome measures (PROMs) of implant-supported reconstructions using digital workflows: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2021, 32 (Suppl. S21), 318–335. [Google Scholar] [CrossRef]
- McLean, J.W.; Von Fraunhofer, J.A. The estimation of cement film thickness by an in vivo technique. Br. Dent. J. 1971, 131, 107–111. [Google Scholar] [CrossRef]
- Muddugangadhar, B.C.; Siddhi, T.; Suchismita, D. Prostho-perio-restorative interrelationship: A major junction. J. Adv. Oral Res. 2011, 2, 7–12. [Google Scholar] [CrossRef]
- Mojon, P.; Rentsch, A.; Budtz-Jørgensen, E. Relationship between prosthodontic status, caries, and periodontal disease in a geriatric population. Int. J. Prosthodont. 1995, 8, 564–571. [Google Scholar] [PubMed]
- Hsu, Y.-T.; Huang, N.; Wang, H.-L.; Kuo, Y.-w.; Chen, M.; Liu, T.-K.; Lin, H.-N.; Kuo, S.-L.; Juan, P.-K.; Liao, P.-B. Relationship between periodontics and prosthodontics: The two-way street. J. Prosthodont. Implantol. 2015, 4, 4–11. [Google Scholar] [CrossRef]
- Avetisyan, A.; Markaryan, M.; Rokaya, D.; Tovani-Palone, M.R.; Zafar, M.S.; Khurshid, Z.; Vardanyan, A.; Heboyan, A. Characteristics of Periodontal Tissues in Prosthetic Treatment with Fixed Dental Prostheses. Molecules 2021, 26, 1331. [Google Scholar] [CrossRef]
- Hao, Y.; Huang, X.; Zhou, X.; Li, M.; Ren, B.; Peng, X.; Cheng, L. Influence of Dental Prosthesis and Restorative Materials Interface on Oral Biofilms. Int. J. Mol. Sci. 2018, 19, 3157. [Google Scholar] [CrossRef]
- Yin, X.J.; Wei, B.Y.; Ke, X.P.; Zhang, T.; Jiang, M.Y.; Luo, X.Y.; Sun, H.Q. Correlation between clinical parameters of crown and gingival morphology of anterior teeth and periodontal biotypes. BMC Oral Health 2020, 20, 59. [Google Scholar] [CrossRef]
- Kossioni, A.E.; Dontas, A.S. The stomatognathic system in the elderly. Useful information for the medical practitioner. Clin. Interv. Aging 2007, 2, 591–597. [Google Scholar] [CrossRef]
- Pihlstrom, B.L.; Michalowicz, B.S.; Johnson, N.W. Periodontal diseases. Lancet 2005, 366, 1809–1820. [Google Scholar] [CrossRef] [PubMed]
- D’Ambrosio, F.; Caggiano, M.; Schiavo, L.; Savarese, G.; Carpinelli, L.; Amato, A.; Iandolo, A. Chronic Stress and Depression in Periodontitis and Peri-Implantitis: A Narrative Review on Neurobiological, Neurobehavioral and Immune–Microbiome Interplays and Clinical Management Implications. Dent. J. 2022, 10, 49. [Google Scholar] [CrossRef] [PubMed]
- Van Dyke, T.E. Inflammation, and periodontal diseases: A reappraisal. J. Periodontol. 2008, 79 (Suppl. S8), 1501–1502. [Google Scholar] [CrossRef] [PubMed]
- Pisano, M.; Amato, A.; Sammartino, P.; Iandolo, A.; Martina, S.; Caggiano, M. Laser Therapy in the Treatment of Peri-Implantitis: State-of-the-Art, Literature Review and Meta-Analysis. Appl. Sci. 2021, 11, 5290. [Google Scholar] [CrossRef]
- Di Spirito, F.; Schiavo, L.; Pilone, V.; Lanza, A.; Sbordone, L.; D’Ambrosio, F. Periodontal and Peri-Implant diseases and systemically administered statins: A systematic review. Dent. J. 2021, 9, 100. [Google Scholar] [CrossRef]
- D’Ambrosio, F.; Di Spirito, F.; Amato, A.; Caggiano, M.; Lo Giudice, R.; Martina, S. Attitudes towards Antibiotic Prescription and Antimicrobial Resistance Awareness among Italian Dentists: What Are the Milestones? Healthcare 2022, 10, 1585. [Google Scholar] [CrossRef]
- D’Ambrosio, F.; Pisano, M.; Amato, A.; Iandolo, A.; Caggiano, M.; Martina, S. Periodontal and Peri-Implant Health Status in Traditional vs. Heat-Not-Burn Tobacco and Electronic Cigarettes Smokers: A Systematic Review. Dent. J. 2022, 10, 103. [Google Scholar] [CrossRef] [PubMed]
- Di Spirito, F.; Sbordone, L.; Pilone, V.; D’Ambrosio, F. Obesity and Periodontal Disease: A Narrative Review on Current Evidence and Putative Molecular Links. Open Dent. J. 2019, 13, 526–536. [Google Scholar] [CrossRef]
- Di Spirito, F.; Lo Giudice, R.; Amato, M.; Di Palo, M.P.; D’Ambrosio, F.; Amato, A.; Martina, S. Inflammatory, reactive, and hypersensitivity lesions potentially due to metal nanoparticles from dental implants and supported restorations: An umbrella review. Appl. Sci. 2022, 12, 11208. [Google Scholar] [CrossRef]
- Boccia, G.; Di Spirito, F.; D’Ambrosio, F.; Di Palo, M.P.; Giordano, F.; Amato, M. Local and systemic antibiotics in peri-implantitis management: An umbrella review. Antibiotics 2023, 12, 114. [Google Scholar] [CrossRef] [PubMed]
- D’Ambrosio, F.; Di Spirito, F.; De Caro, F.; Lanza, A.; Passarella, D.; Sbordone, L. Adherence to antibiotic prescription of dental patients: The other side of the antimicrobial resistance. Healthcare 2022, 10, 1636. [Google Scholar] [CrossRef]
- Pisano, M.; Sammartino, P.; Di Vittorio, L.; Iandolo, A.; Caggiano, M.; Roghi, M.; Bizzoca, M.E.; Lo Muzio, L. Use of Diode Laser for Surgical Removal of Pyogenic Granuloma of the Lower Lip in a Pediatric Patient: A Case Report. Am. J. Case Rep. 2021, 22, e929690. [Google Scholar] [CrossRef]
- Caggiano, M.; Gasparro, R.; D’Ambrosio, F.; Pisano, M.; Di Palo, M.P.; Contaldo, M. Smoking Cessation on Periodontal and Peri-implant Health Status: A Systematic Review. Dent. J. 2022, 10, 162. [Google Scholar] [CrossRef]
- Di Spirito, F.; Amato, A.; Di Palo, M.P.; Cannatà, D.; Giordano, F.; D’Ambrosio, F.; Martina, S. Periodontal Management in Periodontally Healthy Orthodontic Patients with Fixed Appliances: An Umbrella Review of Self-Care Instructions and Evidence-Based Recommendations. Dent. J. 2023, 11, 35. [Google Scholar] [CrossRef]
- Ender, A.; Mehl, A. Infuence of scanning strategies on the accuracy of digital intraoral scanning systems. Int. J. Comput. Dent. 2013, 16, 11–21. [Google Scholar]
- Haddadi, Y.; Bahrami, G.; Isidor, F. Effect of software version on the accuracy of an intraoral scanning device. Int. J. Prosthodont. 2018, 31, 375–376. [Google Scholar] [CrossRef]
- Wismeijer, D.; Mans, R.; Van Genuchten, M.; Reijers, H.A. Patients’ preferences when comparing analogue implant impressions using a polyether impression material versus digital impressions (Intraoral Scan) of dental implants. Clin. Oral Implant. Res. 2014, 25, 1113–1118. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.; Mehl, A.; Mormann, W.H.; Reich, S. Intraoral scanning systems—A current overview. Int. J. Comput. Dent. 2015, 18, 101–129. [Google Scholar] [PubMed]
- Zhang, Y.J.; Shi, J.Y.; Qian, S.J.; Qiao, S.C.; Lai, H.C. Accuracy of full-arch digital implant impressions taken using intraoral scanners and related variables: A systematic review. Int. J. Oral Implantol. 2021, 14, 157–179. [Google Scholar]

{kind=link}
| Authors, Year | Reason for Exclusion | Title 1 | Title 2 |
|---|---|---|---|
| Ahmed, 2021 [32] | Analyzes the manufacturing process of removable partial dentures | entry 1 | data |
| L. C. Aragón, 2016 [33] | In Vitro Studies’ review | entry 2 | data |
| Albanchez-González, 2022 [34] | In Vitro Studies’ review | ||
| Chochlidakis, 2016 [35] | In Vitro Studies’ review | ||
| Kustrzycka, 2020 [36] | Compare different types of scanners | ||
| Mühlemann, 2018 [37] | Analyzes the manufacturing process of implant-supported reconstructions | ||
| Mangano, 2017 [38] | Is a Narrative Review | ||
| Tabesh, 2022 [39] | Analyzes the accuracy of the material | ||
| Morsy, 2021 [40] | Analyzes the accuracy of the material | ||
| ValentI, 2022 [41] | Does not analyze impression techniques | ||
| Parize, 2021 [42] | In Vitro Studies’ review | ||
| Yang, 2022 [43] | Does not analyze impression techniques | ||
| Yen Mai, 2022 [44] | Does not analyze impression techniques | ||
| Cicciu, 2020 [45] | Analyzes the accuracy of the material |
| Authors, Year Reference Journal Meta-Analysis Funding | Studies (Number and Design) Population Sample Size | Kind of Workflow | Type of Intraoral Scanner | Outcomes | Conclusions |
|---|---|---|---|---|---|
| Sivaramakrishnan, 2020 [46] Aust Dent J Network Meta-analysis | RCT or PS 14 studies included 471 patients (236 digital impressions compared to 235 conventional impressions) to evaluate patient preference; 589 patients (278 digital impressions and 311 conventional impressions) to evaluate the time | digital vs. conventional impression | TRIOS, iTERO, CEREC Omincam | Patients preferences Time | |
| Flugge, 2018 [47] Clin Oral Implants Res. A systematic review and Meta-analysis | RCT and no RCT, RS, case series, and experimental study 79 studies were included 77 experimental studies, 1 RS, and 1 RCT. 11 studies about digital impressions and 59 studies about conventional impressions. 9 studies compared the two kinds of impressions | digital vs. conventional impression | CEREC, CBCT, iTERO, LAVA, iMetric 3D, Everest | Fit of implant-supported prosthesis | Few data are available about the accuracy of digital and conventional implant impressions to give clinical advice |
| de Oliveira, 2020 [48] Clin Oral Implants Res. A systematic review and Meta-analysis | RCT, observational studies 10 studies were included Seven RCT and 3 observational studies patients: 214 Single implant crowns: 278 | digital vs. conventional impression for single implant crowns | iTero—Align Tech in, CEREC-Omnicam, Carestream dental-CS3600, 3 Shape TRIOS | impression time patient preference, time efficiency | The digital workflow has demonstrated better results than conventional workflow for patient preference, time efficiency, and impression time |
| Alikhasi, 2017 [49] Implant Dent. A systematic review | In vitro studies Pilot clinical studies 10 studies were included 8 in vitro studies and 2 clinical studies Sample size in vivo: 49 Sample size in vitro: 91 | Digital vs. conventional impression | TRIOS, iTERO, CEREC Omincam | Accuracy | No statistical differences among the techniques |
| Giachetti, 2020 [50] Int J Prosthodont. A systematic review | Clinical studies 6 studies were included Sample size: 74 | Digital vs. conventional impression with Fixed crowns | TRIOS, LAVA, iTERO, CEREC | Trueness precision | Conventional impressions with high-precision impression materials seem more accurate than digital impressions |
| Hasanzade, 2019 [51] J Evid Based Dent Pract. A systematic review and Meta-analysis | 33 studies were included 8 prospective studies; 26 in vitro studies (1 study contained both in vivo and in vitro data) Sample size in vivo: 372 Sample size in vitro: 832 | Internal and Marginal Fit for Full-fixed Prosthesis | TRIOS, LAVA; CEREC, iTERO | marginal gap internal gap | Marginal adaptation does not show differences between the digital and conventional groups for in vivo studies, but differences were found for in vitro studies, where the digital impression showed better marginal adaptation |
| Nagarkar, 2018 [52] The Journal of the American Dental Association. A systematic review and meta-analysis | Crossover RTs, no RTs Parallel-group RT 10 studies were included: 7 crossover RT There were 2 no RCTs and only 1 parallel-group randomized trial Sample size: 291 | Digital versus conventional impressions for full-coverage restorations | LAVA, BlueCam, TRIOS, TRUE def., iTERO | Survival of full coverage restorations Marginal gap, internal gap, and occlusal and interproximal contacts. | No differences were found between the two kinds to take impressions |
| Tsirogiannis, 2016 [7] J Prosthet Dent. A systematic review and Meta-analysis | 12 studies were included: 4 prospective clinical trials 8 in vitro studies | The marginal fit of single ceramic restorations made with impressions taken by the digital method and conventional method was evaluated. | N.S. | marginal fit of the ceramic single-tooth restorations | From the results obtained, no statistically significant difference was observed between the marginal gap of restorations made by digital and conventional impressions |
| Gallardo, 2018 [53] J Prosthet Dent. A systematic review and Meta-analysis | RCT and observational studies 5 studies were included: 3 RCT and 2 prospective clinical trials | Digital vs. conventional impression | iTERO, TRIOS | Patient preferences in working time | Current evidence suggests that patients prefer the digital workflow Emerging data suggest that patients prefer digital workflow to conventional analog workflow |
| Tabesh, 2021 [54] J Prosthet Dent. A systematic review and Meta-analysis | In vitro and in vivo studies 17 studies were included (8 clinical) Sample size: 1068 | The marginal fit of single-unit zirconia restorations made with impressions taken by the digital and conventional methods was evaluated. | LAVA, CEREC, iTERO, TRIOS | Survival of restorations, operator perception, marginal accuracy, and the internal fit. internal fit rather than on marginal accuracy | The results show that single-unit zirconia restorations made by using digital scanning of teeth have better marginal accuracy than those made by conventional techniques |
| Hasanzade, 2021 [55] J Prosthet Dent. A systematic review and Meta-analysis | There are 36 studies included in this systematic review of which 8 are prospective clinical studies and 29 in vitro studies (1 of these contained both in vivo and in vitro data) Sample size in vivo: 372 | Compare the marginal and internal gap of complete single crowns | LAVA, CEREC, iTERO, TRIOS | marginal gap internal gap | The data obtained showed that restorations produced with the digital workflow have a comparable if not better marginal fit than those obtained with other methods |
| Bandiaky, 2022 [56] J Prosthet Dent. A systematic review and Meta-analysis | RCT and PS Of the 16 studies included in the review, 14 are RCTs or parallel-group studies and 2 are comparative prospective studies Sample size in vivo: 599 | The purpose of the study was to compare tooth-supported fixed prosthetic restorations made by digital methods and those made by conventional impressions | LAVA, CEREC Ominicam, iTERO, TRIOS | Clinical time; Patient comfort; Marginal fit | The results showed that digital techniques are comparable to conventional ones in terms of clinical time and marginal fit. There is also evidence of greater patient comfort during the impression-taking stages with digital methods compared with conventional impression techniques |
| García-Gil, 2020 [57] J Clin Exp Dent. A systematic review | Seventy-six studies were included in this review. Of these, 19 were in vitro studies and 8 were in vivo studies. Sample size clinical studies: 85 | The purpose of the work was to evaluate the accuracy and practical utility of intraoral scanners in implant treatments. | LAVA, CEREC, iTERO, TRIOS | Accuracy of impression and efficiency | The data obtained showed that digital impressions in implantology are a viable alternative in cases of one or two contiguous implants. As for full arch rehabilitations, there is a need for new studies |
| Papaspyridakos, 2014 [58] Int J Oral Maxillofac Implants. A systematic review | In vitro and clinical studies 76 studies were included | Accuracy of Implant Impressions for Partially and Completely Edentulous Patients | N.S. | Accuracy splinted vs. nonsplinted, Open-tray vs. closed-tray impression techniques | From the data obtained, it was found that the splinted impression technique is more accurate in both partially and fully edentulous cases. it was also found that the closed spoon technique is more accurate in fully edentulous patients, with no particular differences with the open spoon technique in partially edentulous patients. Overlapping accuracy was observed among the different impression materials. The angle of implant emergence affects the accuracy of impressions while there are insufficient data to analyze the effect of implant connection type |
| Ahlholm, 2018 [59] J Prosthodont. A systematic review | In vitro and in vivo studies 11 studies were included 8 in vitro 3 in vivo size sample: 140 | Digital vs. conventional impression | LAVA, CEREC, iTERO | marginal gap internal gap trueness precision time | The data obtained showed that digital impression methods are a viable alternative to conventional impression techniques in the fabrication of short crowns. A higher speed with a shorter lead time was observed for digital impressions. Even in implant–prosthetic rehabilitations, making crowns and FDPs with digital impressions allow for a clinically acceptable fit. However, based on the data obtained, the conventional impression technique is recommended in cases of whole arch rehabilitations |
| Papaspyridakos, 2020 [60] J Prosthodont. A systematic review and meta-analysis | Eighteen studies were included in this review including 9 in vitro studies and 1 clinical study for impression analysis in fully edentulous patients and 6 in vitro studies and 2 clinical studies in partially edentulous patients. | Digital vs. Conventional Implant Impressions | 3M True Def., CEREC, iTERO, TRIOS | The accuracy and influence of implant angle on 3D accuracy were evaluated. | Data obtained mainly from in vitro studies have shown that the accuracy of 3D digital impressions is comparable to that of conventional implant impressions. However, further in vivo studies are needed to evaluate the accuracy in clinical practice |
| Siqueira, 2021 [61] Clin Oral Investig. A systematic review | RCTs and PS 17 studies were included RCTs: 9 PS: 8 Sample size: 437 | Intraoral scanning and conventional procedure in fixed prosthodontics and implant dentistry | LAVA, CEREC, iTERO, TRIOS, 3M True def., Carestream-CS3600 | working time patient comfort | IOS is faster than CI. By assessing the degree of preference and overall patient comfort, it can be said that IOS can improve the patient experience |
| Joda, 2017 [62] BMC Oral Health A systematic review | RCTs 3 studies were included sample size: 48 patients | The purpose of the study was to compare digitized methods with analog or analog-digital methods for the production of tooth- or implant-supported fixed prosthetic restorations. | iTero, Carestream | Economics esthetics patient-centered outcomes survival and success rate to assess any complications with follow-up at least 1 year under function. | It has emerged that research appears to be slower than technology in the area of digital applications, so there is a need for well-designed RCT studies |
| de Paris Matos, 2021 [63] J Prosthet Dent. A systematic review and Meta-analysis | Of the 11 included studies, 10 had a crossover design of which 2 had a split-mouth design. In total, 1 study had a parallel design. | Comparison between conventional impression and intraoral digital scan for prosthetic rehabilitation | N.S. | The patient’s degree of discomfort, presence/absence of nausea, and unpleasant taste were assessed. | From the data obtained, it was found that intraoral digital scanning is a suitable alternative to conventional impression-taking procedures in that it decreases the discomfort of patients both in terms of the absence/presence of nausea and taste and breathing difficulties |
| Schmidt, 2022 [64] Clin Oral Impl Res A systematic review | RCTs 8 studies were included Simple size: 225 | The accuracy of impressions taken by digital technique in implant cases in clinical studies was evaluated. | iTero, TRIOS, True Def. 3M | Measurement of accuracy | From the literature review, the number of clinical studies to evaluate the accuracy of impressions taken by the digital method is insufficient. However, the accuracy of IOS for digital impressions in patients rehabilitated with implants appears to be clinically acceptable |
| Manicone, 2021 [65] J Prosthet Dent. A systematic review and meta-analysis | RCTs and OS 12 studies were included 2 were randomized crossover trials 7 studies were observational studies sample size: 447 patients | The purpose of this work was to evaluate and compare the impression-taking step performed by digital scanning and conventional technique for the fabrication of implant-supported prosthetic restorations | CS3600, CEREC, iTERO, TRIOS | Patient preferences; procedure working time | The results showed that digital scanning is more efficient than conventional technical impression-taking in terms of time |
| Kong, 2022 [66] Clin Oral Investig. A systematic review and Meta-analysis | In vivo studies 13 studies were included | The purpose of the work was to compare the linear and three-dimensional accuracy of digital versus conventional impressions | LAVA, CEREC, iTERO, TRIOS, True Def. 3M | Linear dimensions of tooth width, complete and anterior Bolton ratio, intercanine distance (ICD), and intermolar distance (IMD) were evaluated. | The results showed that the accuracy and precision of impressions taken by the digital technique are superimposable to those taken by the traditional alginate technique for the full arch |
| BishtI 2021, [67] Clin Oral Implants Res. A systematic review and Meta-analysis | Clinical studies 7 studies were included | The purpose of this work was to compare implant-supported prosthetic restorations made by digital methods and those made by conventional techniques. | CS3600, CEREC, iTERO, TRIOS | The patient’s degree of anxiety, pain, shortness of breath, discomfort, and taste were assessed. | The data obtained showed that patients showed a preference for digital impressions while there were no differences between coated and monolithic restorations |
| Author | The Total Number of Involved Study Participants | Clinical Studies Included |
|---|---|---|
| Sivaramakrishnan [46] | 1060 | 14 RCT |
| Flugge [47] | NS | 1 RCT |
| de Oliveira [48] | 214 | 7 RCT |
| Alikhasi, [49] | 49 | 2 CS |
| Giachetti [50] | 74 | 6 CS |
| Hasanzade [51] | 372 | 8 PS |
| Nagarkar [52] | 291 | 8 CS |
| Tsirogiannis [7] | 145 | 4 CS |
| Gallardo [53] | 155 | 3 RCT 2 PS |
| Tabesh [54] | 1068 | 8 CS |
| Hasanzade [55] | 372 | 8 CS |
| Bandiaky [56] | 599 | 14 RCT |
| García-Gil [57] | 85 | 8 CS |
| Papaspyridakos [58] | 32 | 4 CS |
| Ahlholm [59] | 140 | 3 CS |
| Papaspyridakos [60] | 19 | 3 CS |
| Siqueira [61] | 437 | 17 RCT |
| Joda [62] | 48 | 3 CS |
| de Paris Matos [63] | NS | 11 CS |
| Schmidt [64] | 225 | 8 CS |
| Manicone [65] | 447 | 12 CS |
| Kong [66] | 496 | 13 CS |
| BishtI [67] | 367 | 7 CS |
| TOT = 6.695 | TOT = 174 |
| Authors | Main Results | Statistical Analysis | p Value |
|---|---|---|---|
| Sivaramakrishnan, 2020 [46] | The time is greater for digital impressions | Time: 2.72 [0.08, 5.32] | Time: p < 0.005 |
| Cunha de Oliveira, 2020 [48] | The results showed better efficiency in terms of time for digital impression-taking. | MD: 8.22 [95%CI: 5.48, 10.96] | p < 0.01 |
| Gallardo, 2018 [53] | The results showed a faster procedure for the conventional technique in 2 studies while a faster procedure for the digital technique in 3 studies. | NS | NS |
| Bandiaky, 2022 [56] | The data obtained showed that digital scanning techniques are superimposable to conventional ones in terms of operative time. | digital scans: 784 ± 252 s; conventional impressions: 1125 ± 159 s | p > 0.5 |
| Siqueira, 2021 [61] | In the following review, it appears that the technique with IOS is faster than the conventional technique in both single quadrant and full arch scan cases. | NS | NS |
| Manicone, 2021 [65] | Digital scanning was found to be more time-efficient | SMD: −1.96 [−3.09, −0.83] | p < 0.001 |
| Ahlholm, 2018 [59] | The time taken to taking the impression is less if it is made by digital technique. | Digital impression: 248.48 ± 23.48 s. Conventional impression: 605.38 ± 23.66 s. | NS |
| Bishti, 2021 [67] | Patients showed a high preference for optical impressions | MD: −10.91 [−21.90, 0.08] | p = 0.05 |
| Author | Main results | Statistical Analysis | p Value |
|---|---|---|---|
| Sivaramakrishnan, 2020 [46] | The data showed a general preference for impressions taken by digital technique. | Overall: 31.23 [5.95, 163.87] | p < 0.001 |
| De Oliveira, 2020 [48] | The data obtained showed better clinical efficiency in terms of operative time and patient preference for the digital workflow than the conventional one. | NS | NS |
| Gallardo, 2018 [53] | A preference for digital workflow over conventional workflow has emerged on the part of patients. | NS | NS |
| Bandiaky, 2022 [56] | Patients report greater comfort in impression-taking procedures using digital techniques than those taken using conventional analog techniques. | The mean VAS score:
| p < 0.05 |
| Siqueira, 2021 [61] | Based on the results obtained in terms of general patient preference and comfort, and in terms of the reliability of prosthetic outcomes, the intraoral scanner can be a means to improve procedures. | NS | NS |
| Joda, 2017 [62] | It was found that the too low number of quality RCT studies does not allow us to establish a patient preference for one or the other technique. | NS | NS |
| De Paris Matos, 2021 [63] | The data obtained showed that the discomfort reported by patients during the impression-taking phase is lower in cases using intraoral scanning. | SMD: 15.02 [8.33–21.73] | p < 0.001 |
| Manicone, 2021 [65] | Patients consider the impression-taking stage made by intraoral scanning more comfortable. | SMD: 1.86 [0.26, 3.45] | p = 0.02 |
| Bishti, 2021 [67] | Patients showed a high preference for optical impressions. | MD: 22.83 [12.29, 33.36] | p = 0.002 |
| Author | Discussion | Statistical Analisys | p Value |
|---|---|---|---|
| Flugge, 2018 [47] | Due to the limited amount of available data on the accuracy of digital impressions and conventional impressions in vivo, it is not possible to derive adequate clinical recommendations. | NS | NS |
| Marzieh Alikhasi, 2017 [49] | Due to the heterogeneity of the included studies, it is not possible to conclude whether the use of an intraoral scanner is better clinically than conventional techniques. More in vivo and in vitro studies need to be conducted to evaluate the accuracy of scanners. | NS | NS |
| Giachetti, 2020 [50] | The data obtained from the following review showed that impressions taken by conventional technique with high-precision materials were more accurate than those taken by digital technique. | The selected studies reported different values of accuracy:
| NS |
| Hasanzade, 2019 [51] | The data obtained in vitro showed that fingerprints result in better marginal adaptation while in vivo no significant differences were found. | In vitro
| p = 0.002 |
| Nagarkar, 2018 [52] | The data obtained are insufficient to determine the difference in accuracy between fingerprinting and conventional techniques. | Marginal gap
| p = 0.003 |
| Tsirogiannis, 2016 [7] | The data obtained showed no significant difference in the marginal gap of single-unit ceramic restorations made after digital or conventional impressions. | NS | NS |
| Tabesh, 2021 [54] | The data obtained showed that in teeth prepared for zirconia single-unit crown dentures, digital intraoral scanning exhibited greater marginal accuracy than those prepared with impressions taken using conventional techniques. | −0.89 mm (95% CI: −1.24, −0.54) | p < 0.001 |
| Hasanzade, 2021 [55] | Digital methods are more efficient at producing restorations with comparable if not better marginal fit than other methods. | 0.25 (−0.09, 0.59) | p = 0.006 |
| Bandiaky, 2022 [56] | The data obtained showed that the marginal fit of restorations made with impressions taken with digital techniques is superimposable to those made with conventional impressions. | Marginal fit
| p > 0.005 |
| García-Gil, 2020 [57] | Further studies are needed to evaluate the accuracy of digital techniques. | NS | NS |
| Papaspyridakos, 2014 [58] | From the data obtained, it was found that the splinted impression technique is more accurate in both partially and fully edentulous cases. it was also found that the closed spoon technique is more accurate in fully edentulous patients, with no particular differences with the open spoon technique in partially edentulous patients. Overlapping accuracy was observed among the different impression materials. The angle of implant emergence affects the accuracy of impressions while there are insufficient data to analyze the effect of implant connection type. | NS | NS |
| Ahlholm, 2018 [59] | It has been shown that for the fabrication of implant-supported crowns and FDPs, digital impression systems provide a clinically acceptable fit. | Accuracy marginal fit
| NS |
| Papaspyridakos, 2020 [60] | Data obtained mainly from in vitro studies have shown that the accuracy of 3D digital impressions is comparable to that of conventional implant impressions. | In vitro: 8.20 μm (95% CI: −53.56, 37.15) In vivo: 52.31 μm (95% CI: 6.30, 98.33) | In vitro: p = 0.72 In vivo: p= 0.03 |
| Schmidt, 2022 [64] | From the literature review, the number of clinical studies to evaluate the accuracy of impressions taken by the digital method is insufficient. However, the accuracy of IOS for digital impressions in patients rehabilitated with implants appears to be clinically acceptable. | Linear distance:
digital 40 ± 29 μm; lower jaw conventional 46 ± 27 μm, digital 79 ± 50 μm | NS |
| Kong, 2022 [66] | The results showed that the accuracy and precision of impressions taken by the digital technique are superimposable to those taken by the traditional alginate technique for the full arch. | ICD: −0.11 [−0.47,0.26] IMD: 0.04 [−0.49, 0.58] | p = 0.88 |
| Level | Description | Sivaramakrishnan [46] | Flugge [47] | de Oliveira [48] | Alikhasi, [49] | Giachetti [50] | Hasanzade [51] | Nagarkar [52] | Tsirogiannis [7] | Gallardo [53] | Tabesh [54] | Hasanzade [55] | Bandiaky [56] | García-Gil [57] | Papaspyridakos [58] | Ahlholm [59] | Papaspyridakos [60] | Siqueira [61] | Joda [62] | de Paris Matos [63] | Schmidt [64] | Kong [66] | BishtI [67] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| High | No or one non-critical weakness: the systematic review provides an accurate and comprehensive summary of the results of the available studies that address the question of interest | ✓ | ✓ | ✓ | |||||||||||||||||||
| Moderate | More than one non-critical weakness: the systematic review has more than one weakness but no critical flaws. It may provide an accurate summary of the results of the available studies that were included in the review | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||
| Low | One critical flaw with or without non-critical weaknesses: the review has a critical flaw and may not provide an accurate and comprehensive summary of the available studies that address the question of interest | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||||
| Critically low | More than one critical flaw with or without non-critical weaknesses: the review has more than one critical flaw and should not be relied on to provide an accurate and comprehensive summary of the available studies |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Ambrosio, F.; Giordano, F.; Sangiovanni, G.; Di Palo, M.P.; Amato, M. Conventional versus Digital Dental Impression Techniques: What Is the Future? An Umbrella Review. Prosthesis 2023, 5, 851-875. https://doi.org/10.3390/prosthesis5030060
D’Ambrosio F, Giordano F, Sangiovanni G, Di Palo MP, Amato M. Conventional versus Digital Dental Impression Techniques: What Is the Future? An Umbrella Review. Prosthesis. 2023; 5(3):851-875. https://doi.org/10.3390/prosthesis5030060
Chicago/Turabian StyleD’Ambrosio, Francesco, Francesco Giordano, Giuseppe Sangiovanni, Maria Pia Di Palo, and Massimo Amato. 2023. "Conventional versus Digital Dental Impression Techniques: What Is the Future? An Umbrella Review" Prosthesis 5, no. 3: 851-875. https://doi.org/10.3390/prosthesis5030060
APA StyleD’Ambrosio, F., Giordano, F., Sangiovanni, G., Di Palo, M. P., & Amato, M. (2023). Conventional versus Digital Dental Impression Techniques: What Is the Future? An Umbrella Review. Prosthesis, 5(3), 851-875. https://doi.org/10.3390/prosthesis5030060