

Scanning Electron Microscopy Analyses of Dental Implant Abutments Debonded from Monolithic Zirconia Restorations Using Heat Treatment: An In Vitro Study

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
Outcomes
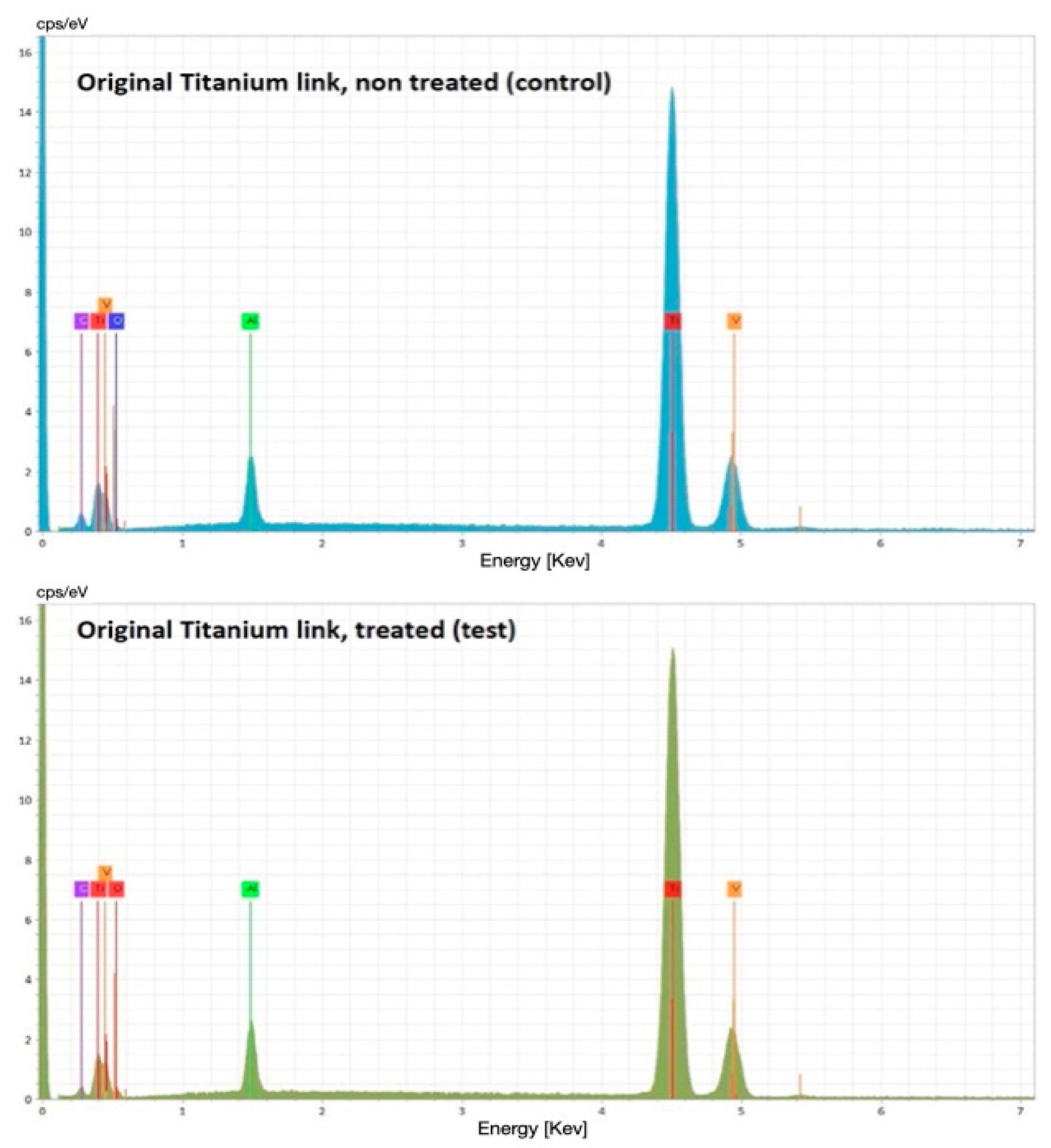
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tallarico, M.; Canullo, L.; Caneva, M.; Ozcan, M. Microbial colonization at the implant-abutment interface and its possible influence on periimplantitis: A systematic review and meta-analysis. J. Prosthodont. Res. 2017, 61, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Hermann, J.S.; Buser, D.; Schenk, R.K.; Schoolfield, J.D.; Cochran, D.L. Biologic Width around one- and two-piece titanium implants. Clin. Oral Implants Res. 2001, 12, 559–571. [Google Scholar] [CrossRef] [PubMed]
- Tallarico, M.; Caneva, M.; Meloni, S.M.; Xhanari, E.; Covani, U.; Canullo, L. Definitive Abutments Placed at Implant Insertion and Never Removed: Is It an Effective Approach? A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Oral Maxillofac. Surg. 2018, 76, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Tallarico, M.; Caneva, M.; Baldini, N.; Gatti, F.; Duvina, M.; Billi, M.; Iannello, G.; Piacentini, G.; Meloni, S.M.; Cicciù, M. Patient-centered rehabilitation of single, partial, and complete edentulism with cemented- or screw-retained fixed dental prosthesis: The First Osstem Advanced Dental Implant Research and Education Center Consensus Conference 2017. Eur. J. Dent. 2018, 12, 617–626. [Google Scholar] [CrossRef]
- Tallarico, M.; Czajkowska, M.; Cicciù, M.; Giardina, F.; Minciarelli, A.; Zadrożny, Ł.; Park, C.J.; Meloni, S.M. Accuracy of surgical templates with and without metallic sleeves in case of partial arch restorations: A systematic review. J. Dent. 2021, 115, 103852. [Google Scholar] [CrossRef]
- Zadrożny, Ł.; Czajkowska, M.; Mijiritsky, E.; Wagner, L. Repeatability of Freehand Implantations Supported with Universal Plastic Sleeves—In Vitro Study. Int. J. Environ. Res. Public Health 2020, 17, 4453. [Google Scholar] [CrossRef]
- Judgar, R.; Giro, G.; Zenobio, E.; Coelho, P.G.; Feres, M.; Rodrigues, J.A.; Mangano, C.; Iezzi, G.; Piattelli, A.; Shibli, J.A. Biological width around one- and two-piece implants retrieved from human jaws. BioMed Res. Int. 2014, 2014, 850120. [Google Scholar] [CrossRef]
- Spinato, S.; Galindo-Moreno, P.; Bernardello, F.; Zaffe, D. Minimum Abutment Height to Eliminate Bone Loss: Influence of Implant Neck Design and Platform Switching. Int. J. Oral Maxillofac. Implants 2018, 33, 405–411. [Google Scholar] [CrossRef]
- Guo, T.; Gulati, K.; Arora, H.; Han, P.; Fournier, B.; Ivanovski, S. Race to invade: Understanding soft tissue integration at the transmucosal region of titanium dental implants. Dent. Mater. 2021, 37, 816–831. [Google Scholar] [CrossRef]
- Ivanovski, S.; Lee, R. Comparison of peri-implant and periodontal marginal soft tissues in health and disease. Periodontol. 2000 2018, 76, 116–130. [Google Scholar] [CrossRef]
- Esposito, M.; Salina, S.; Rigotti, F.; Mazzarini, C.; Longhin, D.; Grigoletto, M.; Buti, J.; Sbricoli, L.; Gualini, F. Multicentre withinperson randomised controlled trial of 0.5 mm versus 1.5 subcrestal placement of dental implants with internal conical connection: Five-year post-loading results. Clin. Trials Dent. 2020, 2, 77–89. [Google Scholar] [CrossRef]
- Novaes, A.B., Jr.; Barros, R.R.; Muglia, V.A.; Borges, G.J. Influence of interimplant distances and placement depth on papilla formation and crestal resorption: A clinical and radiographic study in dogs. J. Oral Implantol. 2009, 35, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Lops, D.; Stocchero, M.; Motta Jones, J.; Freni, A.; Palazzolo, A.; Romeo, E. Five Degree Internal Conical Connection and Marginal Bone Stability around Subcrestal Implants: A Retrospective Analysis. Materials 2020, 13, 3123. [Google Scholar] [CrossRef] [PubMed]
- Rabel, K.; Spies, B.C.; Pieralli, S.; Vach, K.; Kohal, R.J. The clinical performance of all-ceramic implant-supported single crowns: A systematic review and meta-analysis. Clin. Oral Implants Res. 2018, 29, s196–s223. [Google Scholar] [CrossRef] [PubMed]
- Pjetursson, B.E.; Valente, N.A.; Strasding, M.; Zwahlen, M.; Liu, S.; Sailer, I. A systematic review of the survival and complication rates of zirconia-ceramic and metal-ceramic single crowns. Clin. Oral Implants Res. 2018, 29, s199–s214. [Google Scholar] [CrossRef]
- Larsson, C.; Wennerberg, A. The clinical success of zirconia-based crowns: A systematic review. Int. J. Prosthodont. 2014, 27, 33–43. [Google Scholar] [CrossRef]
- Al-Thobity, A.M. Titanium Base Abutments in Implant Prosthodontics: A Literature Review. Eur. J. Dent. 2022, 16, 49–55. [Google Scholar] [CrossRef]
- Tallarico, M.; Fiorellini, J.; Nakajima, Y.; Omori, Y.; Takahisa, I.; Canullo, L. Mechanical Outcomes, Microleakage, and Marginal Accuracy at the Implant-Abutment Interface of Original versus Nonoriginal Implant Abutments: A Systematic Review of In Vitro Studies. BioMed Res. Int. 2018, 2018, 2958982. [Google Scholar] [CrossRef]
- Joda, T.; Zarone, F.; Ferrari, M. The complete digital workflow in fixed prosthodontics: A systematic review. BMC Oral Health 2017, 17, 124. [Google Scholar] [CrossRef]
- Mühlemann, S.; Kraus, R.D.; Hämmerle, C.H.F.; Thoma, D.S. Is the use of digital technologies for the fabrication of implant-supported reconstructions more efficient and/or more effective than conventional techniques: A systematic review. Clin. Oral Implants Res. 2018, 29, s184–s195. [Google Scholar] [CrossRef]
- Czajkowska, M.; Walejewska, E.; Zadrożny, Ł.; Wieczorek, M.; Święszkowski, W.; Wagner, L.; Mijiritsky, E.; Markowski, J. Comparison of Dental Stone Models and Their 3D Printed Acrylic Replicas for the Accuracy and Mechanical Properties. Materials 2020, 13, 4066. [Google Scholar] [CrossRef] [PubMed]
- Zadrożny, Ł.; Roguś, P.; Pyzlak, M.; Tallarico, M. Full versus semi-digital workflow in case of surgical management of mandibular cyst. J. Dent. 2022, 121, 104013. [Google Scholar] [CrossRef]
- Zahoui, A.; Bergamo, E.T.; Marun, M.M.; Silva, K.P.; Coelho, P.G.; Bonfante, E.A. Cementation Protocol for Bonding Zirconia Crowns to Titanium Base CAD/CAM Abutments. Int. J. Prosthodont. 2020, 33, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Burkhardt, F.; Pitta, J.; Fehmer, V.; Mojon, P.; Sailer, I. Retention Forces of Monolithic CAD/CAM Crowns Adhesively Cemented to Titanium Base Abutments-Effect of Saliva Contamination Followed by Cleaning of the Titanium Bond Surface. Materials 2021, 14, 3375. [Google Scholar] [CrossRef] [PubMed]
- Pitta, J.; Burkhardt, F.; Mekki, M.; Fehmer, V.; Mojon, P.; Sailer, I. Effect of airborne-particle abrasion of a titanium base abutment on the stability of the bonded interface and retention forces of crowns after artificial aging. J. Prosthet. Dent. 2021, 126, 214–221. [Google Scholar] [CrossRef]
- Pozzi, A.; Tallarico, M.; Barlattani, A. Monolithic lithium disilicate full-contour crowns bonded on CAD/CAM zirconia complete-arch implant bridges with 3 to 5 years of follow-up. J. Oral Implantol. 2013, 41, 450–458. [Google Scholar] [CrossRef]
- Pozzi, A.; Holst, S.; Fabbri, G.; Tallarico, M. Clinical Reliability of CAD/CAM Cross-Arch Zirconia Bridges on Immediately Loaded Implants Placed with Computer-Assisted/Template-Guided Surgery: A Retrospective Study with a Follow-up between 3 and 5 Years. Clin. Implant Dent. Relat. Res. 2015, 17, e86–e96. [Google Scholar] [CrossRef]
- Amorfini, L.; Storelli, S.; Mosca, D.; Scanferla, M.; Romeo, E. Comparison of cemented vs screw-retained, customized computer-aided design/computer-assisted manufacture zirconia abutments for esthetically located single-tooth implants: A 10-year randomized prospective study. Int. J. Prosthodont. 2018, 31, 359–366. [Google Scholar] [CrossRef]
- Gasser, T.J.W.; Papageorgiou, S.N.; Eliades, T.; Hämmerle, C.H.F.; Thoma, D.S. Interproximal contact loss at implant sites: A retrospective clinical study with a 10-year follow-up. Clin. Oral Implants Res. 2022, 33, 482–491. [Google Scholar] [CrossRef]
- Stimmelmayr, M.; Edelhoff, D.; Güth, J.F.; Erdelt, K.; Happe, A.; Beuer, F. Wear at the titanium-titanium and the titanium-zirconia implant-abutment interface: A comparative in vitro study. Dent. Mater. 2012, 28, 1215–1220. [Google Scholar] [CrossRef]
- Solá-Ruíz, M.F.; Selva-Otaolaurruchi, E.; Senent-Vicente, G.; González-de-Cossio, I.; Amigó-Borrás, V. Accuracy combining different brands of implants and abutments. Med. Oral Patol. Oral Cir. Bucal 2013, 18, e332–e336. [Google Scholar] [CrossRef] [PubMed]
- Bakri, A.S.; Sahdan, M.Z.; Adriyanto, F.; Raship, N.A.; Said, N.D.M.; Abdullah, A.A.; Rahim, M.S. Effect of annealing temperature of titanium dioxide thin films on structural and electrical properties. AIP Conf. Proc. 2017, 1788, 030030. [Google Scholar] [CrossRef]
- Peng, W.; Zeng, W.; Zhang, Y.; Shi, C.; Quan, B.; WU, J. The Effect of Colored Titanium Oxides on the Color Change on the Surface of Ti-5Al-5Mo-5V-1Cr-1Fe Alloy. J. Mater. Eng. Perform. 2013, 22, 2588–2593. [Google Scholar] [CrossRef]
- Alcisto, J.; Enriquez, A.; Garcia, H.; Hinkson, S.; Hahn, M.; Foyos, J.; Ogren, J.; Lee, E.W.; Es-Said, O.S. The effect of thermal history on the color of oxide layers in titanium 6242 alloy. Eng. Fail. Anal. 2004, 6, 811–816. [Google Scholar] [CrossRef]
- Gaddam, R.; Sefer, B.; Pederson, R.; Antti, M.-L. Oxidation and alpha-case formation in Ti–6Al–2Sn–4Zr–2Mo alloy. Mater. Charact. 2015, 99, 166–174. [Google Scholar] [CrossRef]
- Minervini, G.; Fiorillo, L.; Russo, D.; Lanza, A.; D’Amico, C.; Cervino, G.; Meto, A.; Di Francesco, F. Prosthodontic Treatment in Patients with Temporomandibular Disorders and Orofacial Pain and/or Bruxism: A Review of the Literature. Prosthesis 2022, 4, 253–262. [Google Scholar] [CrossRef]
- Minervini, G.; Romano, A.; Petruzzi, M.; Maio, C.; Serpico, R.; Lucchese, A.; Candotto, V.; Di Stasio, D. Telescopic overdenture on natural teeth: Prosthetic rehabilitation on (OFD) syndromic patient and a review on available literature. J. Biol. Regul. Homeost. Agents 2018, 32 (Suppl. 1), 131–134. [Google Scholar]
- Antonelli, A.; Bennardo, F.; Brancaccio, Y.; Barone, S.; Femiano, F.; Nucci, L.; Minervini, G.; Fortunato, L.; Attanasio, F.; Giudice, A. Can Bone Compaction Improve Primary Implant Stability? An In Vitro Comparative Study with Osseodensification Technique. Appl. Sci. 2020, 10, 8623. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
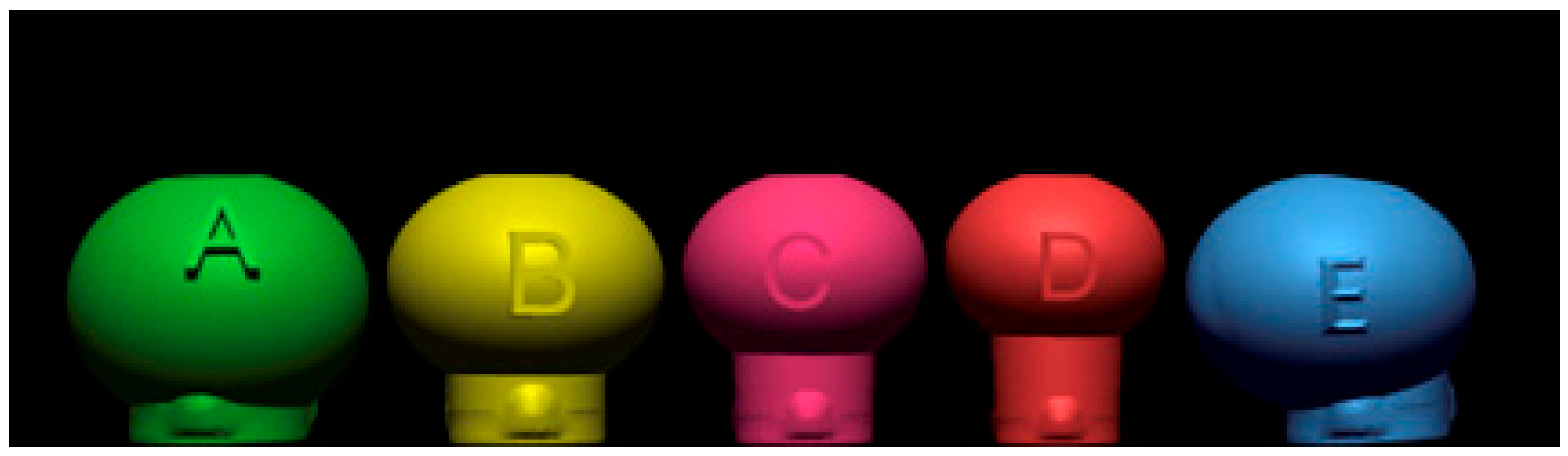
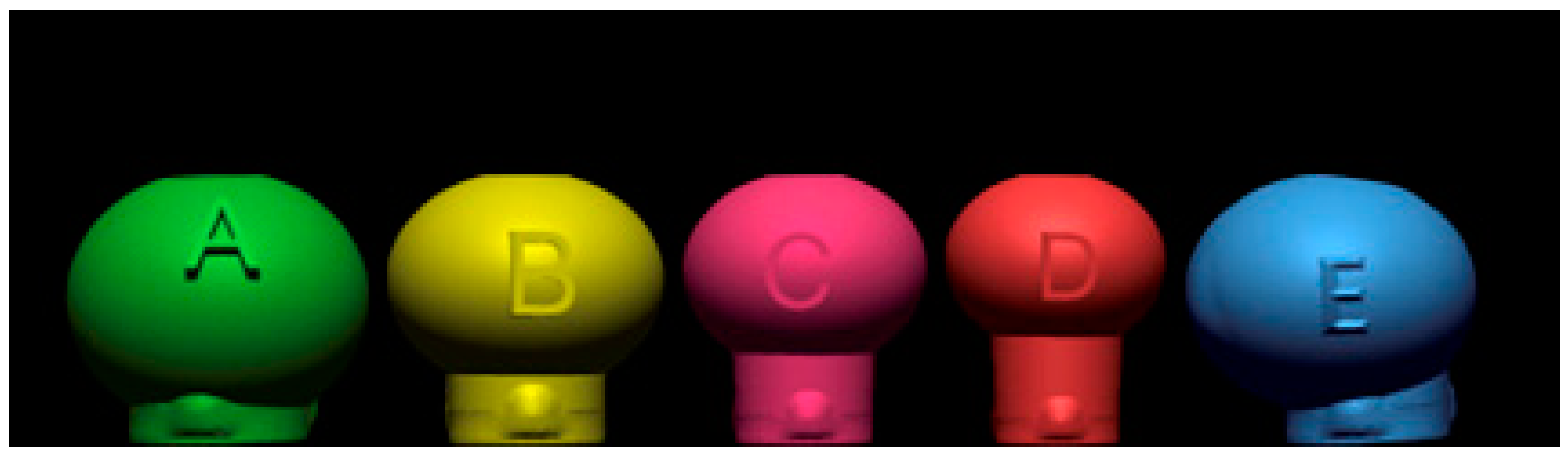
| Test Sample | Characteristics |
|---|---|
| A green | Standard anatomical center mass with 1 mm of gingival height |
| B yellow | Standard anatomical center mass with 2 mm of gingival height |
| C fucsia | Slightly shifted anatomical center mass with 3 mm of gingival height |
| D red | Standard anatomical center mass with 5 mm of gingival height |
| E blu | Shifted anatomical center mass with 2.5 mm of gingival height |
| Physical Property | Data |
|---|---|
| Thermal expansion coefficients (CTE) | 10.5 ± 1.0 × 10−6 K−1 (25–500 °C) |
| Density after sintering | 6.08 ± 0.01 g/cm3 |
| Bending strength (three-point bending test) | >1200 Mpa |
| Sintering temperature (recommended temperature) | 1450–1580 °C (1530 °C) |
| Translucency | 43% |
| MZR | TBA |
|---|---|
| Sandblasting with aluminum dioxide 50 μm | Steam cleaning |
| Ultrasonic bath at low frequency for 10 min with distilled water | Drying with air |
| Drying with air | Primer * |
| Primer * |
| Settings and Procedures |
|---|
| After disinfection, remove the screw and place the restoration into the ceramic tray. |
| Pre-heating (initial temperature) to 300 °C. |
| Closing the oven for 2 min. |
| Stabilization for 5 min at 300 °C with the chamber closed. |
| Temperature increasing 30 °C per minute up to 370 °C. |
| Stabilization for 5 min at 370 °C. |
| Cooling for 2 min at 300 °C. |
| Opening the ceramic oven for 2 min. |
| Stabilization before handling for 10 min. |
| MZR | TBA |
|---|---|
| Ultrasonic bath at low frequency for 1 min (distilled water). | Ultrasonic bath at low frequency for 15 min (distilled water). |
| Sandblasting with aluminum dioxide at 50 microns. | Ultrasonic bath at low frequency for 10 min with a liquid detergent (Pi-Ku-Plast Clear, Bredent). |
| Manual cleaning. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tallarico, M.; Zadrożny, Ł.; Squadrito, N.; Colella, L.; Gualandri, M.; Montanari, D.; Zibetti, G.; Santini, S.; Chromiński, W.; Baldoni, E.; et al. Scanning Electron Microscopy Analyses of Dental Implant Abutments Debonded from Monolithic Zirconia Restorations Using Heat Treatment: An In Vitro Study. Prosthesis 2022, 4, 500-510. https://doi.org/10.3390/prosthesis4030041
Tallarico M, Zadrożny Ł, Squadrito N, Colella L, Gualandri M, Montanari D, Zibetti G, Santini S, Chromiński W, Baldoni E, et al. Scanning Electron Microscopy Analyses of Dental Implant Abutments Debonded from Monolithic Zirconia Restorations Using Heat Treatment: An In Vitro Study. Prosthesis. 2022; 4(3):500-510. https://doi.org/10.3390/prosthesis4030041
Chicago/Turabian StyleTallarico, Marco, Łukasz Zadrożny, Nino Squadrito, Leonardo Colella, Maurizio Gualandri, Daniele Montanari, Gianantonio Zibetti, Simone Santini, Witold Chromiński, Edoardo Baldoni, and et al. 2022. "Scanning Electron Microscopy Analyses of Dental Implant Abutments Debonded from Monolithic Zirconia Restorations Using Heat Treatment: An In Vitro Study" Prosthesis 4, no. 3: 500-510. https://doi.org/10.3390/prosthesis4030041
APA StyleTallarico, M., Zadrożny, Ł., Squadrito, N., Colella, L., Gualandri, M., Montanari, D., Zibetti, G., Santini, S., Chromiński, W., Baldoni, E., Meloni, S. M., Lumbau, A. I., & Pisano, M. (2022). Scanning Electron Microscopy Analyses of Dental Implant Abutments Debonded from Monolithic Zirconia Restorations Using Heat Treatment: An In Vitro Study. Prosthesis, 4(3), 500-510. https://doi.org/10.3390/prosthesis4030041