
Listening to People with Misophonia: Exploring the Multiple Dimensions of Sound Intolerance Using a New Psychometric Tool, the S-Five, in a Large Sample of Individuals Identifying with the Condition





Abstract
1. Introduction
- To develop a tool that would be multidimensional, identifying, and measuring the complex nature of the misophonic experience.
- To make the tool brief enough to use routinely for evaluations in both research and clinical practice.
- To ensure excellent psychometric properties, including being unbiased with respect to gender and age of the respondent.
- To create a supplementary scale to quantify the burden of triggers, capturing the nature of reactions, number of triggers, intensity of the reaction, and the synergy of number and intensity. We aimed to do this with a flexible format to allow researchers and clinicians to add or remove sounds.
2. Materials and Methods
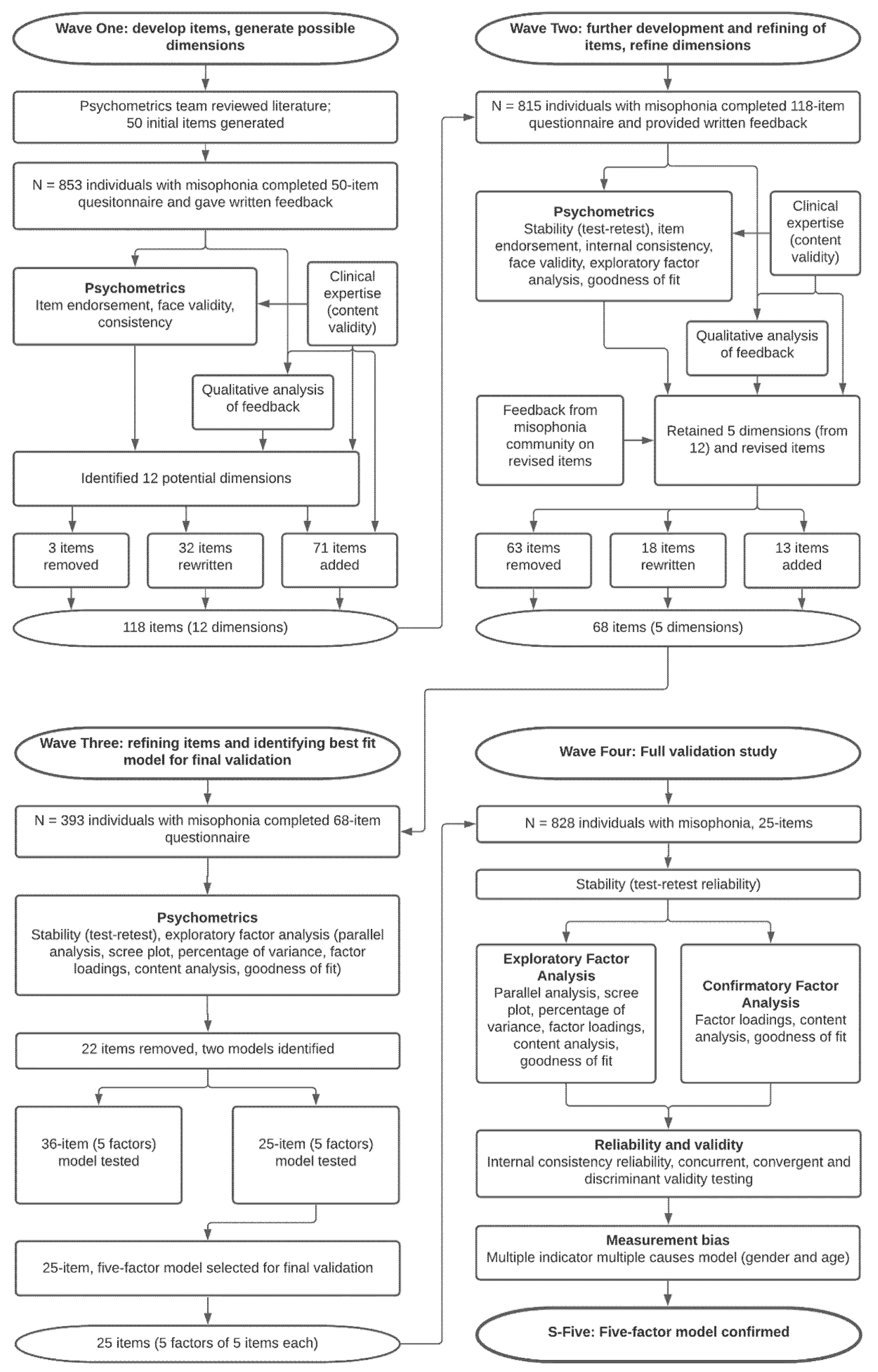
2.1. Scale Development
2.2. Sampling
2.3. Measures
2.4. Factor Analysis
2.5. Reliability and Validity
3. Results
3.1. Sample
3.1.1. Demographic and Clinical Characteristics of the Sample
3.1.2. Misophonia Statistics
3.2. Validation of the S-Five
3.2.1. Endorsement
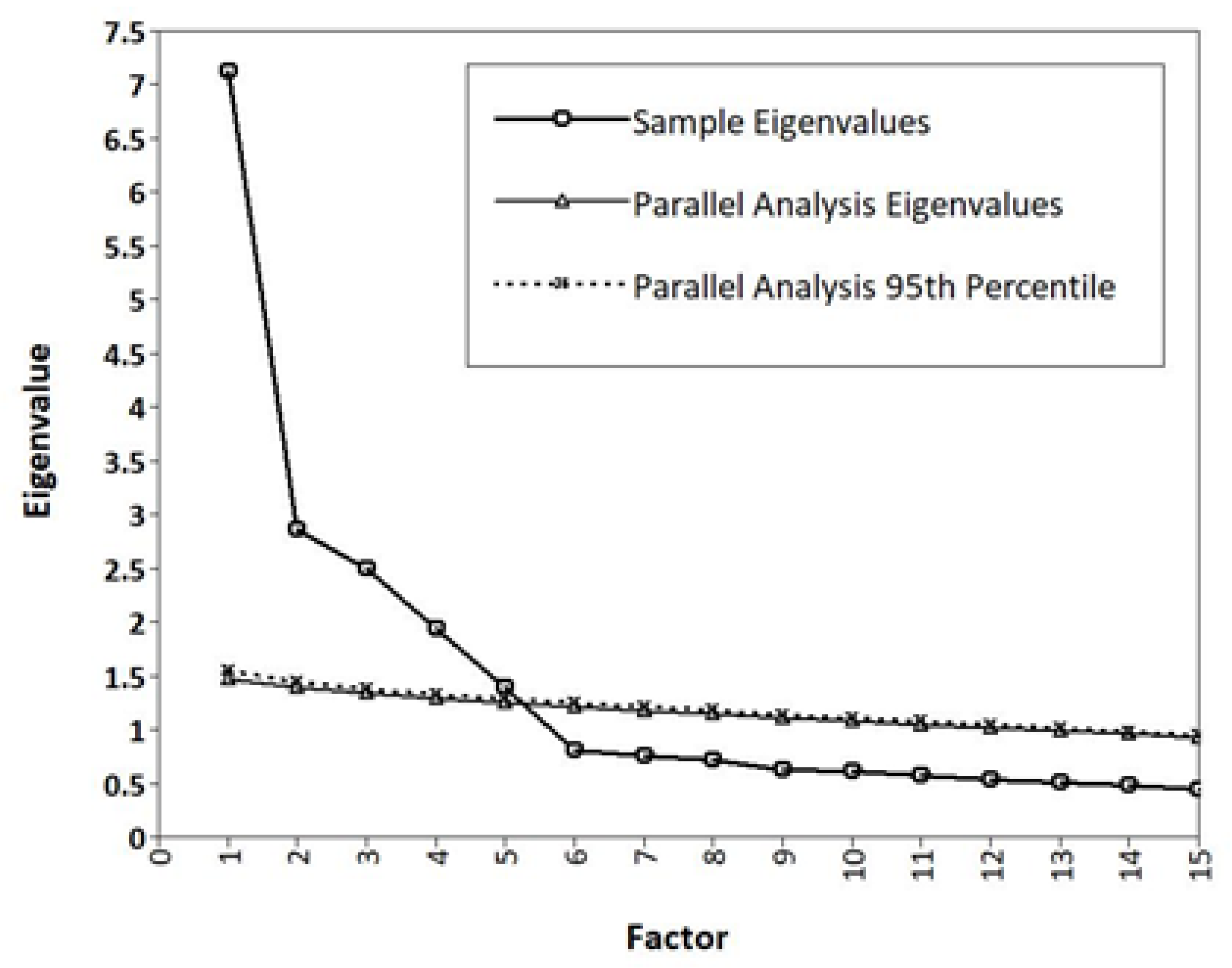
3.2.2. EFA and CFA: Dimensionality
3.2.3. MIMIC Model: Measurement Invariance
3.2.4. Scores, Reliability, and Validity
3.3. S-Five Triggers Checklist (S-Five-T)
3.3.1. Checklist Scoring Options
- Trigger Count (TC) is the total number of triggers endorsed by a participant from the list provided. So, for the present study, the participant’s TC would take values between 0–37, as we listed 37 possible triggers. For example, if an individual selected “no feeling” or “other: positive” reaction to 32 out of 37 triggers, their TC would be 5, that is, the number of triggers to which they experience a negative reaction (irrespective of intensity). This index tells us about the number of triggers that cause a negative reaction.
- Reaction count (RC) is the number of times each particular reaction type is endorsed and can be counted across triggers in a single participant, or across participants. The index is computed for each reaction type separately, resulting in a reaction count for each (for example, RC-Anger, RC-Irritability, etc.). The total possible RC for a participant is determined by the number of triggers listed (37 in the present study). For example, if a participant selected anger as their main emotional reaction to three triggers, panic as their main reaction to two triggers, and no feeling for their remaining triggers, then they would have an RC-Anger of 3, RC-Panic of 2, and RC-No feeling of 32 (irrespective of intensity). This index tells us about the nature of the emotional responses to triggers.
- Frequency/intensity of reactions score (FIRS) is the total value of the intensity items of all endorsed triggers. The intensity is rated from 0–10, and therefore, for the present study, the FIRS takes values between 0 and 370. For example, if a participant reported a negative reaction to five triggers and rated each to the highest possible intensity (that is, 10), their FIRS value would be 50. A participant who reported 10 triggers, each at a moderate intensity of 5, would also have a FIRS value of 50. This index provides combined information about the number of triggers and their intensity.
- Relative intensity of reactions score (RIRS) gives an estimate of the intensity of reactions to triggers, relative to the number of triggers reported. It is computed by dividing the FIRS index by the TC index. RIRS takes values between 0 and 100, regardless of the number of reactions available and number of triggers listed in the study. Continuing with the examples from above, the individual who had a FIRS of 50, who reported 5 triggers with an intensity of 10 each, their RIRS would equal 10 (50 divided by 5 triggers). However, the individual with the same FIRS (50) who reported 10 triggers with an intensity of 5 would have a RIRS of 5 (FIRS 50 divided by TC 10). This index provides information about the average intensity of an individual’s reaction to triggers.
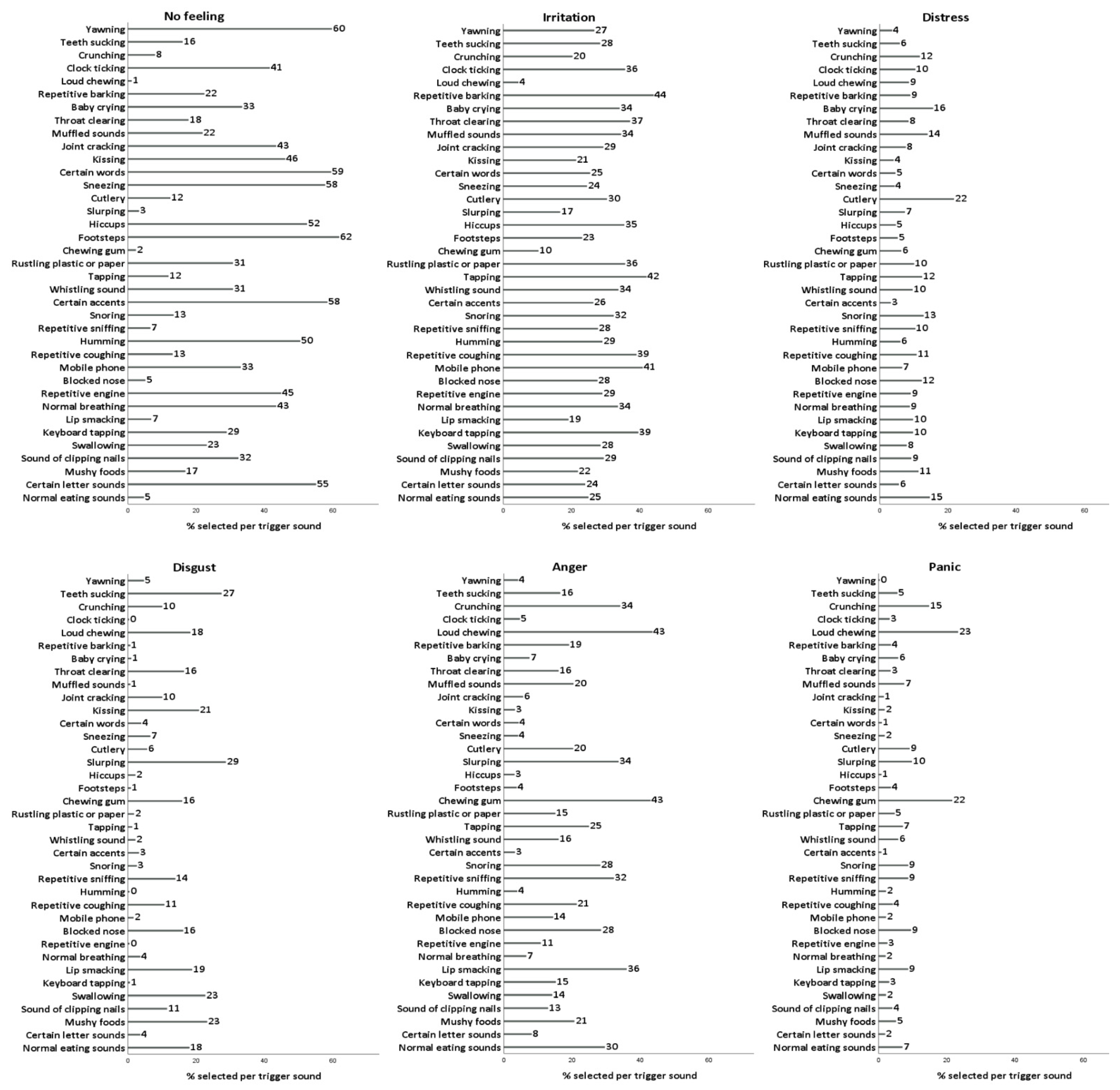
3.3.2. Reported Reactions to Triggers
4. Discussion
4.1. The Dimensions of Misophonia
4.2. Emotional Reactions to Trigger Sounds
4.3. The S-Five in the Context of the Consensus Definition of Misophonia
4.4. Limitations
4.5. Conclusions and Practical Applications
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Please read each statement * carefully and base your answer on how true they feel to you based on your current thoughts, experiences, and reactions: 0-not at all true to 10-completely true Externalising I13 People should not make certain sounds, even if they do not know about others’ sensitivities I25 I get angry at other people because of how disrespectful they are with the noises they make I06 People should do everything they can to avoid making noises that might bother others I16 I react strongly to certain sounds because I cannot stand how selfish, thoughtless, or bad-mannered people can be I21 Certain sounds are just bad manners, and it is not strange to feel intense anger about that Internalising I18 The way I react to certain sounds makes me wonder whether deep inside I am just a bad person I08 The way I react to certain noises makes me feel like I must be an unlikable person deep down I05 I respect myself less because of my responses to certain sounds I12 I feel like I must be a very angry person inside because of the way I react to certain sounds I19 I dislike myself in the moments of my reactions to sounds Impact I20 My job opportunities are limited because of my reaction to certain noises I01 I do not meet friends as often as I would like to because of the noises they make I14 There are places I would like to go but do not, because I am too worried about how the noises will impact me I15 I can see future where I cannot do everyday things because of my reactions to noises I09 The way I feel/react to certain sounds will eventually isolate me and prevent me from doing everyday things Outburst I17 I can get so angry at certain noises that I get physically aggressive towards people to make them stop I22 Sometimes I get so distressed by noises that I use violence to try and make it stop I23 Some sounds are so unbearable that I will shout at people to make them stop I04 If people make certain sounds that I cannot bear, I become verbally aggressive I24 I am afraid I will do something aggressive or violent because I cannot stand the noise someone is making Threat I11 I feel trapped if I cannot get away from certain noises I07 I feel anxious if I cannot avoid listening to certain sounds I02 If I cannot get away from certain noises, I am afraid I might panic or feel like I will explode I03 If I cannot avoid certain sounds, I feel helpless I10 I can experience distress as the result of some noises |
| * Items should be randomised before being administered and without enumeration |
| In this section each item is rated in a 0–10 ordinal scale, for example: People should not make certain sounds, even if they do not know about others’ sensitivities 0 (not at all true) 1 2 3 4 5 6 7 8 9 10 (completely true) |
| Factor scores and Total Score: Please add the responses of the corresponding items for each factor to compute the factor score and all items for the total S-Five-E score. Each factor has 5 items thus the scores are directly comparable in terms of statement endorsement. |
| Range: factor scores range between 0 and 50, total score is between 0 and 250. |
| The scoring guide and the programming codes (SPSS, R project, Stata) to obtain all factors and indices are freely available upon request made to the first author. The S-Five, © Copyright King’s College London, 2021. All Rights Reserved. |
| Trigger reaction items: Thinking about the past few weeks, what is the main feeling this sound has caused you?No feeling, irritation, distress, disgust, anger, panic, other feeling: negative, other feeling: positive, other: physiological reaction |
| Trigger intensity items: Thinking about the past few weeks, please rate the intensity of your reaction to this sound when made by another person or object (from 0: doesn’t bother me at all to 10: unbearable/causes suffering) |
| List of triggers currently included in the S-Five-t: Normal eating sounds, Certain letter sounds, Mushy foods being eaten, Sound of clipping nails, Swallowing, Keyboard tapping, Lip smacking, Normal breathing, Repetitive engine noises, Loud/unusual breathing, Mobile phone sounds, Repetitive coughing, Humming noise, Repetitive sniffing, Snoring, Certain accents, Whistling sound, Sound of tapping, Rustling, Chewing gum, Footsteps, Hiccups, Slurping, Cutlery noises, Sneezing, Certain words, Kissing, Joint cracking, Muffled sounds, Throat clearing, Baby crying, Repetitive barking, Loud chewing, Clock ticking, Crunching eating sounds, Teeth sucking, Yawning. |
| The scoring guide and the programming codes (SPSS, R project, Stata) to obtain all factors and indices are freely available upon request made to the first author. The S-Five, © Copyright King’s College London, 2021. All Rights Reserved. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
References
- Jastreboff, M.M.; Jastreboff, P.J. Decreased sound tolerance and tinnitus retraining therapy (TRT). Aust. N. Z. J. Audiol. 2002, 24, 74. [Google Scholar] [CrossRef]
- Swedo, S.; Baguley, D.M.; Denys, D.; Dixon, L.J.; Erfanian, M.; Fioretti, A.; Jastreboff, P.J.; Kumar, S.; Rosenthal, M.Z.; Rouw, R.; et al. A Consensus Definition of Misophonia: Using a Delphi Process to Reach Expert Agreement. medRxiv 2021. [Google Scholar] [CrossRef]
- Edelstein, M.; Brang, D.; Rouw, R.; Ramachandran, V.S. Misophonia: Physiological investigations and case descriptions. Front. Hum. Neurosci. 2013, 7, 296. [Google Scholar] [CrossRef] [PubMed]
- Rouw, R.; Erfanian, M. A Large-Scale Study of Misophonia. J. Clin. Psychol. 2018, 74, 453–479. [Google Scholar] [CrossRef]
- Schröder, A.E.; Vulink, N.; Denys, D. Misophonia: Diagnostic Criteria for a New Psychiatric Disorder. PLoS ONE 2013, 8, e54706. [Google Scholar] [CrossRef]
- Wu, M.S.; Lewin, A.B.; Murphy, T.K.; Storch, E.A. Misophonia: Incidence, Phenomenology, and Clinical Correlates in an Undergraduate Student Sample. J. Clin. Psychol. 2014, 70, 994–1007. [Google Scholar] [CrossRef]
- Zhou, X.; Wu, M.S.; Storch, E.A. Misophonia symptoms among Chinese university students: Incidence, associated impairment, and clinical correlates. J. Obs. Compuls. Relat. Disord. 2017, 14, 7–12. [Google Scholar] [CrossRef]
- Brout, J.J.; Edelstein, M.; Erfanian, M.; Mannino, M.; Miller, L.J.; Rouw, R.; Kumar, S.; Rosenthal, M.Z. Investigating Misophonia: A Review of the Empirical Literature, Clinical Implications, and a Research Agenda. Front. Neurosci. 2018, 12, 36. [Google Scholar] [CrossRef] [PubMed]
- Potgieter, I.; MacDonald, C.; Partridge, L.; Cima, R.; Sheldrake, J.; Hoare, D.J. Misophonia: A scoping review of research. J. Clin. Psychol. 2019, 75, 1203–1218. [Google Scholar] [CrossRef] [PubMed]
- Murphy, D.L.; Pickar, D.; Alterman, I.S. Methods for the quantitative assessment of depressive and manic behavior. In The Behaviour of Psychiatric Patients: Quantitative Techniques for Evaluation; Burdock, E.I., Sudilovsku, A., Gershon, S., Eds.; Marcel Dekker: New York, NY, USA, 1982; pp. 335–392. [Google Scholar]
- Goodman, W.K.; Price, L.H.; Rasmussen, S.A.; Mazure, C.; Fleischmann, R.L.; Hill, C.L.; Heninger, G.R.; Charney, D.S. The Yale-Brown Obsessive Compulsive Scale. I. Development, use, and reliability. Arch. Gen. Psychiatry 1989, 46, 1006–1011. [Google Scholar] [CrossRef]
- Jager, I.; de Koning, P.; Bost, T.; Denys, D.; Vulink, N. Misophonia: Phenomenology, comorbidity and demographics in a large sample. PLoS ONE 2020, 15, e0231390. [Google Scholar] [CrossRef] [PubMed]
- Fitzmaurice, G. Misophonia Activation Scale (MAS-1). Available online: http://www.misophonia-uk.org/the-misophonia-activation-scale.html (accessed on 25 October 2021).
- Johnson, M.A. Rating Misophonia Severity: The Misophonia Assessment Questionnaire. 2013; Unpublished. [Google Scholar]
- Naylor, J.; Caimino, C.; Scutt, P.; Hoare, D.J.; Baguley, D.M. The Prevalence and Severity of Misophonia in a UK Undergraduate Medical Student Population and Validation of the Amsterdam Misophonia Scale. Psychiatr. Q. 2021, 92, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Siepsiak, M.; Śliwerski, A.; Dragan, W. Development and Psychometric Properties of MisoQuest—A New Self-Report Questionnaire for Misophonia. Int. J. Environ. Res. Public Health 2020, 17, 1797. [Google Scholar] [CrossRef]
- Singer, D.A. The Mixed-Methods Case Study of "Zara": Cognitive Behavior Therapy Treatment of a College Student with Misophonia; Rutgers University: New Brunswick, NJ, USA, 2018. [Google Scholar]
- Reid, A.M.; Guzick, A.G.; Gernand, A.; Olsen, B. Intensive cognitive-behavioral therapy for comorbid misophonic and obsessive-compulsive symptoms: A systematic case study. J. Obs. Compuls. Relat. Disord. 2016, 10, 1–9. [Google Scholar] [CrossRef]
- Schneider, R.L.; Arch, J.J. Letter to the editor: Potential treatment targets for misophonia. Gen. Hosp. Psychiatry 2015, 37, 370–371. [Google Scholar] [CrossRef]
- Muller, D.; Khemlani-Patel, S.; Neziroglu, F. Cognitive-Behavioral Therapy for an Adolescent Female Presenting With Misophonia: A Case Example. Clin. Case Stud. 2018, 17, 249–258. [Google Scholar] [CrossRef]
- Alekri, J.; Al Saif, F. Suicidal misophonia: A case report. Psychiatry Clin. Psychopharmacol. 2019, 29, 232–237. [Google Scholar] [CrossRef]
- Johnson, P.; Webber, T.; Wu, M.; Lewin, A.; Murphy, T.; Storch, E. When selective audiovisual stimuli become unbearable: A case series on pediatric misophonia. Neuropsychiatry 2013, 3, 569–575. [Google Scholar] [CrossRef]
- Bernstein, R.; Angell, K.; Dehle, C. A brief course of cognitive behavioural therapy for the treatment of misophonia: A case example. Cogn. Behav. Ther. 2013, 6, E10. [Google Scholar] [CrossRef]
- Hocaoglu, C. A little known topic misophonia: Two case reports. Dusunen Adam J. Psychiatry Neurol. Sci. 2018, 31, 89–96. [Google Scholar] [CrossRef]
- Tunç, S.; Başbuğ, H.S. An extreme physical reaction in misophonia: Stop smacking your mouth! Psychiatry Clin. Psychopharmacol. 2017, 27, 416–418. [Google Scholar] [CrossRef]
- Veale, D. A Compelling Desire for Deafness. J. Deaf. Stud. Deaf. Educ. 2006, 11, 369–372. [Google Scholar] [CrossRef][Green Version]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; de Vet, H.C. The COSMIN study reached international consensus on taxonomy, terminology, and definitions of measurement properties for health-related patient-reported outcomes. J. Clin. Epidemiol. 2010, 63, 737–745. [Google Scholar] [CrossRef]
- De Vet, H.; Terwee, C.; Mokkink, L.; Knol, D. Measurement in Medicine: A Practical Guide (Practical Guides to Biostatistics and Epidemiology; Cambridge University Press: Cambridge, UK, 2011; pp. 1–6. [Google Scholar]
- Khadjesari, Z.; Boufkhed, S.; Vitoratou, S.; Schatte, L.; Ziemann, A.; Daskalopoulou, C.; Uglik-Marucha, E.; Sevdalis, N.; Hull, L. Implementation outcome instruments for use in physical healthcare settings: A systematic review. Implement. Sci. 2020, 15, 66. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Lowe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Gen. Psychiatry 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, H.F. The Application of Electronic Computers to Factor Analysis. Educ. Psychol. Meas. 1960, 20, 141–151. [Google Scholar] [CrossRef]
- Kaiser, H.F.; Rice, J. Little Jiffy, Mark I. Educ. Psychol. Meas. 1974, 34, 111–117. [Google Scholar] [CrossRef]
- Bartlett, M.S. The effect of standardization on a Chi-square approximation in factor analysis. Biometrika 1951, 38, 337–344. [Google Scholar]
- Muthen, L.K.; Muthén, B. Mplus User’s Guide; Muthén & Muthén: Los Angeles, CA, USA, 1998–2017.
- Yuan, K.-H.; Bentler, P.M. 5. Three Likelihood-Based Methods for Mean and Covariance Structure Analysis with Nonnormal Missing Data. Sociol. Methodol. 2000, 30, 165–200. [Google Scholar] [CrossRef]
- Hayton, J.C.; Allen, D.G.; Scarpello, V. Factor Retention Decisions in Exploratory Factor Analysis: A Tutorial on Parallel Analysis. Organ. Res. Methods 2004, 7, 191–205. [Google Scholar] [CrossRef]
- Guttman, L. Some necessary conditions for common factor analysis. Psychometrika 1954, 19, 149–161. [Google Scholar] [CrossRef]
- Horn, J.L. A rationale and test for the number of factors in factor analysis. Psychometrika 1965, 30, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Cattell, R.B. The Scree Test For The Number Of Factors. Multivar. Behav. Res. 1966, 1, 245–276. [Google Scholar] [CrossRef]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Clarkson, D.B.; Jennrich, R.I. Quartic rotation criteria and algorithms. Psychometrika 1988, 53, 251–259. [Google Scholar] [CrossRef]
- Muthén, B. A structural probit model with latent variables. J. Am. Stat. Assoc. 1979, 74, 807–811. [Google Scholar] [CrossRef]
- Steiger, J.H.; Lind, J.C. Statistically-based tests for the number of common factors. In Proceedings of the Annual Meeting of the Psychometric Society, Iowa City, IA, USA, 28 May 1980. [Google Scholar]
- Browne, M.W.; Cudeck, R. Alternative Ways of Assessing Model Fit. Sociol. Methods Res. 1992, 21, 230–258. [Google Scholar] [CrossRef]
- Ullman, M.T. The neural basis of lexicon and grammar in first and second language: The declarative/procedural model. Biling. Lang. Cogn. 2001, 4, 105–122. [Google Scholar] [CrossRef]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Bentler, P.M.; Bonett, D. Significance tests and goodness of fit in the analysis of covariance structures. Psychol. Bull. 1980, 88, 588–606. [Google Scholar] [CrossRef]
- Hooper, D.; Coughlan, J.; Mullen, M.R. Structural equation modelling: Guidelines for determining model fit. J. Bus. Res. Methods 2008, 6, 53–60. [Google Scholar] [CrossRef]
- Cronbach, L. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef]
- Kuiper, R.; Hoogenboezem, R. Nopaco: A Non-Parametric Concordance Coefficient, Version 1.0.5. 2019. Available online: https://CRAN.R-project.org/package=nopaco (accessed on 16 August 2021).
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Tansley-Hancock, O.; Sedley, W.; Winston, J.S.; Callaghan, M.F.; Allen, M.; Cope, T.E.; Gander, P.E.; Bamiou, D.-E.; Griffiths, T.D. The Brain Basis for Misophonia. Curr. Biol. 2017, 27, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Schröder, A.; van Wingen, G.; Eijsker, N.; San Giorgi, R.; Vulink, N.C.; Turbyne, C.; Denys, D. Misophonia is associated with altered brain activity in the auditory cortex and salience network. Sci. Rep. 2019, 9, 7542. [Google Scholar] [CrossRef]
- Clark, D.M. A cognitive approach to panic. Behav. Res. Ther. 1986, 24, 461–470. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Rosenthal, M.Z.; Anand, D.; Cassiello-Robbins, C.; Williams, Z.J.; Guetta, R.E.; Trumbull, J.; Kelley, L.D. Development and Initial Validation of the Duke Misophonia Questionnaire. Front. Psychol. 2021, 12, 709928. [Google Scholar] [CrossRef]
- McManus, S.; Bebbington, P.; Jenkins, R.; Brugha, T. Mental Health and Wellbeing in England: Adult Psychiatric Morbidity Survey 2014; NHS Digital: Leeds, UK, 2016. [Google Scholar]
- Erfanian, M.; Kartsonaki, C.; Keshavarz, A. Misophonia and comorbid psychiatric symptoms: A preliminary study of clinical findings. Nord. J. Psychiatry 2019, 73, 219–228. [Google Scholar] [CrossRef]
- Bryant, F.B.; Smith, B.D. Refining the Architecture of Aggression: A Measurement Model for the Buss–Perry Aggression Questionnaire. J. Res. Personal. 2001, 35, 138–167. [Google Scholar] [CrossRef]
- Mundt, J.C.; Marks, I.M.; Shear, M.K.; Greist, J.M. The work and social adjustment scale: A simple measure of impairment in functioning. Br. J. Psychiatry 2002, 180, 461–464. [Google Scholar] [CrossRef]
- Rimes, K.; Chalder, T. The Beliefs about Emotions Scale: Validity, reliability and sensitivity to change. J. Psychosom. Res. 2010, 68, 285–292. [Google Scholar] [CrossRef]
- Brown, K.W.; Ryan, R.M. The benefits of being present: Mindfulness and its role in psychological well-being. J. Personal. Soc. Psychol. 2003, 84, 822–848. [Google Scholar] [CrossRef]
- Roberts, N.; Beath, A.; Boag, S. Autonomous sensory meridian response: Scale development and personality correlates. Psychol. Conscious. Theory Res. Pract. 2019, 6, 22–39. [Google Scholar] [CrossRef]
- Fergus, T.A.; Valentiner, D.P. The Disgust Propensity and Sensitivity Scale-Revised: An examination of a reduced-item version. J. Anxiety Disord. 2009, 23, 703–710. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.; Zvolensky, M.J.; Cox, B.J.; Deacon, B.; Heimberg, R.G.; Ledley, D.R.; Abramowitz, J.S.; Holaway, R.M.; Sandin, B.; Stewart, S.H.; et al. Robust dimensions of anxiety sensitivity: Development and initial validation of the Anxiety Sensitivity Index-3. Psychol. Assess. 2007, 19, 176–188. [Google Scholar] [CrossRef] [PubMed]
- Peterson, R.A.; Reiss, S. Anxiety Sensitivity Index Manual; International Diagnostic Systems: Worthington, OH, USA, 1992; Volume 2. [Google Scholar]
- Hunot, C.; Fildes, A.; Croker, H.; Llewellyn, C.H.; Wardle, J.; Beeken, R.J. Appetitive traits and relationships with BMI in adults: Development of the Adult Eating Behaviour Questionnaire. Appetite 2016, 105, 356–363. [Google Scholar] [CrossRef]
- Akiskal, H.S.; Akiskal, K.K.; Haykal, R.F.; Manning, J.S.; Connor, P.D. TEMPS-A: Progress towards validation of a self-rated clinical version of the Temperament Evaluation of the Memphis, Pisa, Paris, and San Diego Autoquestionnaire. J. Affect. Disord. 2005, 85, 3–16. [Google Scholar] [CrossRef]
- John, O.P.; Srivastava, S. The Big Five trait taxonomy: History, measurement, and theoretical perspectives. In Handbook of Personality: Theory and Research, 2th ed.; Pervin, L.A., John, O.P., Eds.; Guilford Press: New York, NY, USA, 1999; pp. 102–138. [Google Scholar]
- Leahy, R.L. Leahy Emotional Schema Scale II (LESS II); American Institute for Cognitive Therapy: New York, NY, USA, 2012. [Google Scholar]
- Miller, L.C.; Murphy, R.; Buss, A.H. Consciousness of body: Private and public. J. Personal. Soc. Psychol. 1981, 41, 397–406. [Google Scholar] [CrossRef]



| Statements | Mean (SD) | Median (Q1–Q3) | Mode (min–max) | Spearman Correlation with Age | Average Gender Difference ‡ | Loadings EFA (CFA) | Psi (95% CI) | ICC |
|---|---|---|---|---|---|---|---|---|
| Externalising | ||||||||
| I06 Others avoid making noises | 6.5 (3.3) | 7 (4–10) | 10 (0–10) | 0.01 | −0.2 (0.3) | 0.75 (1a) | 0.82 (0.8,1) | 0.87 |
| I13 Others should not make sounds | 6.4 (3.5) | 7 (4–10) | 10 (0–10) | * −0.08 | 0.3 (0.3) | 0.80 (1.08) | 0.86 (0.8,1) | 0.88 |
| I16 Others selfish | 5.5 (3.6) | 6 (2–9) | 10 (0–10) | −0.02 | 0.3 (0.3) | 0.69 (1.25) | 0.83 (0.8,1) | 0.87 |
| I21 Others bad manners | 6.3 (3.2) | 7 (4–9) | 10 (0–10) | 0.02 | 0.4 (0.3) | 0.65 (0.84) | 0.84 (0.8,1) | 0.87 |
| I25 Others disrespectful | 7.0 (3.2) | 8 (5–10) | 10 (0–10) | * −0.09 | 0.1 (0.3) | 0.70 (1.15) | 0.82 (0.8,1) | 0.86 |
| Internalising | ||||||||
| I05 Respect myself less | 4.5 (3.6) | 4.5 (1–8) | 0 (0–10) | ** −0.13 | * −0.8 (0.3) | 0.67 (1a) | 0.83 (0.8,1) | 0.87 |
| I08 Unlikeable person | 5.2 (3.8) | 5 (1–9) | 10 (0–10) | ** −0.14 | * −0.8 (0.3) | 0.86 (1.18) | 0.83 (0.8,1) | 0.87 |
| I12 Angry person inside | 6.0 (3.6) | 7 (3–10) | 10 (0–10) | −0.07 | −0.5 (0.3) | 0.68 (0.85) | 0.84 (0.8,1) | 0.87 |
| I18 Bad person inside | 4.5 (3.7) | 4 (1–8) | 0 (0–10) | ** −0.20 | ** −1.5 (0.3) | 0.83 (1.14) | 0.83 (0.8,1) | 0.87 |
| I19 Dislike self | 6.8 (3.5) | 8 (4–10) | 10 (0–10) | ** −0.17 | ** −1.7 (0.3) | 0.63 (0.91) | 0.84 (0.8,1) | 0.87 |
| Impact | ||||||||
| I01 Do not meet friends | 4.6 (3.4) | 5 (1–7) | 1 (0–10) | * −0.07 | 0 (0.3) | 0.68 (1a) | 0.83 (0.8,1) | 0.87 |
| I09 Eventually isolated | 5.8 (3.5) | 6 (3–9) | 10 (0–10) | ** −0.12 | −0.4 (0.3) | 0.62 (1.27) | 0.72 (0.7,1) | 0.83 |
| I14 Avoid places | 5.8 (3.6) | 6 (2–10) | 10 (0–10) | −0.05 | −0.1 (0.3) | 0.74 (1.07) | 0.85 (0.8,1) | 0.88 |
| I15 Cannot do everyday things | 5.4 (3.5) | 6 (2–9) | 10 (0–10) | ** −0.15 | −0.5 (0.3) | 0.76 (1.31) | 0.82 (0.8,1) | 0.86 |
| I20 Limited job opportunities | 3.9 (3.6) | 3 (1–7) | 0 (0–10) | ** −0.14 | −0.3 (0.3) | 0.76 (1.05) | 0.86 (0.8,1) | 0.88 |
| Outburst | ||||||||
| I04 Verbally aggressive | 5.3 (3.3) | 5 (2–8) | 10 (0–10) | * −0.09 | −0.1 (0.3) | 0.6 (1a) | 0.82 (0.8,1) | 0.87 |
| I17 Physically aggressive | 2.7 (3.1) | 1 (0–5) | 0 (0–10) | * −0.08 | −0.3 (0.3) | 0.80 (1.01) | 0.79 (0.8,1) | 0.85 |
| I22 Violence | 2.3 (3.0) | 1 (0–3) | 0 (0–10) | ** −0.19 | −0.4 (0.3) | 0.74 (0.97) | 0.82 (0.8,1) | 0.86 |
| I23 Shout at people | 4.7 (3.7) | 4 (1–8) | 10 (0–10) | ** −0.10 | −0.4 (0.3) | 0.67 (1.16) | 0.84 (0.8,1) | 0.87 |
| I24 Afraid of outburst | 4.5 (3.7) | 4 (1–8) | 0 (0–10) | ** −0.20 | −0.2 (0.3) | 0.53 (1.11) | 0.83 (0.8,1) | 0.87 |
| Threat | ||||||||
| I02 Panic or explode | 8.9 (1.9) | 10 (8–10) | 10 (0–10) | ** −0.13 | * −0.4 (0.2) | 0.59 (1a) | 0.79 (0.8,1) | 0.85 |
| I03 Feel helpless | 8.4 (2.4) | 10 (8–10) | 10 (0–10) | ** −0.16 | −0.4 (0.2) | 0.59 (1.27) | 0.79 (0.8,1) | 0.85 |
| I07 Feel anxious | 9.2 (1.7) | 10 (9–10) | 10 (0–10) | * −0.08 | * −0.3 (0.2) | 0.69 (0.84) | 0.77 (0.7,1) | 0.84 |
| I10 Experience distress | 9.4 (1.4) | 10 (10–10) | 10 (0–10) | −0.06 | −0.3 (0.1) | 0.53 (0.62) | 0.77 (0.7,1) | 0.85 |
| I11 Feel trapped | 9.2 (1.7) | 10 (9–10) | 10 (0–10) | ** −0.10 | −0.2 (0.2) | 0.72 (0.95) | 0.81 (0.8,1) | 0.86 |
| Males (N = 141) | Females (N = 655) | Total | Comparison | Internal Consistency | Stability | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Statistic | p-Value | Alpha | IIC | ITC | Psi (95% CI) | ICC | |
| Externalising | 32.7 (13.3) | 31.6 (13.2) | 31.8 (13.2) | U = 43,707.5 | 0.318 | 0.85 | 0.40–0.67 | 0.56–0.72 | 0.87 (0.9,1) | 0.89 |
| Internalising | 22.5 (14.6) | 27.7 (14.6) | 26.8 (14.7) | U = 36,777.5 | <0.001 | 0.88 | 0.53–0.77 | 0.69–0.77 | 0.86 (0.8,1) | 0.88 |
| Impact | 23.9 (15.4) | 25.4 (14.3) | 25.1 (14.5) | U= 43,381.5 | 0.259 | 0.83 | 0.42–0.74 | 0.62–0.78 | 0.89 (0.9,1) | 0.89 |
| Outburst | 18.1 (13.5) | 19.5 (13.2) | 19.2 (13.1) | U= 43,249.5 | 0.237 | 0.84 | 0.42–0.64 | 0.61–0.67 | 0.87 (0.9,1) | 0.89 |
| Threat | 43.7 (8.3) | 45.3 (6.9) | 45.1 (7.2) | U= 39,925.5 | 0.009 | 0.83 | 0.38–0.60 | 0.55–0.71 | 0.83 (0.8,1) | 0.87 |
| S-Five total | 140.9 (46.4) | 149.5 (43.1) | 148.0 (43.8) | t = 2.11 (794) | 0.035 | 0.90 | 0.02–0.77 | 0.27–0.70 | 0.89 (0.9,1) | 0.90 |
| S-Five (N = 828) | |||||
|---|---|---|---|---|---|
| Externalising | Internalising | Impact | Outburst | Threat | |
| S-Five (N = 828) | |||||
| Internalising | 0.206 ** | ||||
| Impact | 0.288 ** | 0.495 ** | |||
| Outburst | 0.299 ** | 0.403 ** | 0.393 ** | ||
| Threat | 0.267 ** | 0.321 ** | 0.510 ** | 0.332 ** | |
| Total | 0.600 ** | 0.734 ** | 0.784 ** | 0.709 ** | 0.620 ** |
| Age (N = 828) | |||||
| Age | −0.060 | −0.123 ** | −0.192 ** | −0.167 ** | −0.192 ** |
| A-MISO-S 1 (N = 319) | |||||
| Total | 0.243 ** | 0.697 ** | 0.415 ** | 0.358 ** | 0.496 ** |
| MQ (N = 320) | |||||
| MSYS (N = 281) | 0.205 ** | 0.291 ** | 0.122 * | 0.105 | 0.273 ** |
| MEBS (N = 281) | 0.265 ** | 0.523 ** | 0.315 ** | 0.577 ** | 0.545 ** |
| MSES (N = 320) | 0.100 | 0.568 ** | 0.302 ** | 0.339 ** | 0.391 ** |
| Total (N = 281) | 0.302 ** | 0.529 ** | 0.287 ** | 0.457 ** | 0.534 ** |
| PHQ9 (N = 800) | |||||
| Total | 0.169 ** | 0.435 ** | 0.375 ** | 0.287 ** | 0.300 ** |
| GAD7 (N = 810) | |||||
| Total | 0.200 ** | 0.414 ** | 0.383 ** | 0.284 ** | 0.324 ** |
| WSAS (N = 813) | |||||
| Total | 0.230 ** | 0.764 ** | 0.484 ** | 0.383 ** | 0.404 ** |
| Trigger Sounds | Mean (SD) | Median (Q1–Q3) | Mode (Min–Max) | Average Gender Difference ‡ | Pearson r with Age | Psi (95% CI) | ICC |
|---|---|---|---|---|---|---|---|
| Normal eating sounds | 6.6 (2.5) | 7 (6–8) | 7 (0–10) | −0.1 (0.2) | ** −0.117 | 0.76 (0.7,1) | 0.84 |
| Certain letter sounds | 2.3 (3.0) | 0 (0–4) | 0 (0–10) | −0.5 (0.3) | −0.037 | 0.79 (0.8,1) | 0.85 |
| Mushy foods | 5.4 (3.3) | 6 (3–8) | 0 (0–10) | 0.0 (0.3) | ** −0.220 | 0.82 (0.8,1) | 0.87 |
| Sound of clipping nails | 3.8 (3.4) | 3 (0–7) | 0 (0–10) | ** −1.2 (0.3) | ** 0.112 | 0.85 (0.8,1) | 0.87 |
| Swallowing | 4.3 (3.3) | 4.5 (1–7) | 0 (0–10) | −0.5 (0.3) | ** −0.103 | 0.86 (0.8,1) | 0.88 |
| Keyboard tapping | 3.7 (3.3) | 3 (0–6) | 0 (0–10) | −0.3 (0.3) | *0.088 | 0.83 (0.8,1) | 0.87 |
| Lip smacking | 6.6 (3.0) | 7 (5–9) | 10 (0–10) | 0.1 (0.3) | ** −0.110 | 0.86 (0.8,1) | 0.88 |
| Normal breathing | 2.9 (3.1) | 2 (0–5) | 0 (0–10) | ** −1.2 (0.3) | ** −0.176 | 0.82 (0.8,1) | 0.86 |
| Repetitive engine | 2.5 (3.0) | 1 (0–4) | 0 (0–10) | 0.0 (0.3) | ** 0.197 | 0.82 (0.8,1) | 0.86 |
| Blocked nose | 6.3 (3.0) | 7 (4–9) | 10 (0–10) | ** −1.4 (0.3) | ** −0.104 | 0.83 (0.8,1) | 0.87 |
| Mobile phone | 3.4 (3.2) | 3 (0–6) | 0 (0–10) | −0.6 (0.3) | 0.069 | 0.84 (0.8,1) | 0.87 |
| Repetitive coughing | 5.0 (3.1) | 5 (2–8) | 0 (0–10) | ** −0.8 (0.3) | 0.016 | 0.81 (0.8,1) | 0.86 |
| Humming | 1.9 (2.7) | 0 (0–3) | 0 (0–10) | −0.4 (0.3) | ** 0.130 | 0.81 (0.8,1) | 0.86 |
| Repetitive sniffing | 6.3 (3.1) | 7 (4–9) | 10 (0–10) | ** −1.0 (0.3) | 0.039 | 0.85 (0.8,1) | 0.87 |
| Snoring | 5.8 (3.5) | 6.5 (3–9) | 10 (0–10) | ** −1.7 (0.3) | 0.045 | 0.86 (0.8,1) | 0.88 |
| Certain accents | 1.7 (2.7) | 0 (0–3) | 0 (0–10) | −0.2 (0.3) | ** 0.113 | 0.78 (0.7,1) | 0.85 |
| Whistling sound | 3.9 (3.5) | 3 (0–7) | 0 (0–10) | ** −1.0 (0.3) | ** 0.103 | 0.86 (0.8,1) | 0.88 |
| Tapping | 5.2 (3.3) | 5 (3–8) | 10 (0–10) | ** −1.2 (0.3) | * 0.088 | 0.87 (0.9,1) | 0.89 |
| Rustling plastic or paper | 3.7 (3.4) | 3 (0–7) | 0 (0–10) | −0.6 (0.3) | * 0.088 | 0.86 (0.8,1) | 0.88 |
| Chewing gum | 8.3 (2.5) | 9 (8–10) | 10 (0–10) | −0.3 (0.2) | −0.030 | 0.84 (0.8,1) | 0.87 |
| Footsteps | 1.7 (2.7) | 0 (0–3) | 0 (0–10) | −0.1 (0.3) | −0.011 | 0.77 (0.7,1) | 0.85 |
| Hiccups | 1.8 (2.5) | 0 (0–3) | 0 (0–10) | −0.4 (0.2) | −0.014 | 0.82 (0.8,1) | 0.86 |
| Slurping | 7.1 (2.9) | 8 (5–10) | 10 (0–10) | −0.4 (0.3) | 0.005 | 0.83 (0.8,1) | 0.87 |
| Cutlery | 5.7 (3.4) | 6 (3–9) | 10 (0–10) | −0.3 (0.3) | −0.030 | 0.86 (0.8,1) | 0.88 |
| Sneezing | 1.9 (2.8) | 0 (0–3) | 0 (0–10) | −0.5 (0.3) | 0.031 | 0.82 (0.8,1) | 0.86 |
| Certain words | 1.7 (2.7) | 0 (0–3) | 0 (0–10) | * −0.5 (0.3) | 0.028 | 0.75 (0.7,1) | 0.84 |
| Kissing | 2.5 (3.2) | 1 (0–5) | 0 (0–10) | ** −1.4 (0.3) | −0.050 | 0.83 (0.8,1) | 0.87 |
| Joint cracking | 2.6 (3.1) | 1 (0–5) | 0 (0–10) | ** −0.8 (0.3) | ** 0.184 | 0.83 (0.8,1) | 0.87 |
| Muffled sounds | 4.7 (3.6) | 5 (1–8) | 0 (0–10) | ** −0.7 (0.3) | 0.027 | 0.85 (0.8,1) | 0.88 |
| Throat clearing | 4.5 (3.4) | 4 (2–7) | 0 (0–10) | ** −1.1 (0.3) | 0.042 | 0.84 (0.8,1) | 0.87 |
| Baby crying | 3.2 (3.3) | 2 (0–6) | 0 (0–10) | 0.6 (0.3) | 0.011 | 0.85 (0.8,1) | 0.88 |
| Repetitive barking | 4.0 (3.3) | 3 (1–7) | 0 (0–10) | 0.3 (0.3) | ** 0.221 | 0.85 (0.8,1) | 0.88 |
| Loud chewing | 8.8 (2.0) | 10 (8–10) | 10 (0–10) | −0.2 (0.2) | ** −0.106 | 0.81 (0.8,1) | 0.86 |
| Clock ticking | 2.8 (3.4) | 1 (0–5) | 0 (0–10) | ** −0.7 (0.3) | −0.011 | 0.83 (0.8,1) | 0.87 |
| Crunching | 7.1 (3.3) | 8 (5–10) | 10 (0–10) | 0.0 (0.3) | −0.008 | 0.86 (0.8,1) | 0.88 |
| Teeth sucking | 5.3 (3.4) | 6 (3–8) | 0 (0–10) | ** −1.1 (0.3) | 0.055 | 0.87 (0.8,1) | 0.88 |
| Yawning | 1.9 (2.8) | 0 (0–4) | 0 (0–10) | −0.5 (0.3) | −0.013 | 0.81 (0.8,1) | 0.86 |
| Mean (SD) | Median (Q1–Q3) | Mode (Min–Max) | Average Gender Difference M vs. F (sd) N = 796 | Psi (95% CI) N = 104 | ICC N = 104 | |
|---|---|---|---|---|---|---|
| RC | ||||||
| No feeling | 9.8 (6.4) | 9 (5–14) | 0 (0–31) | 2.4 * (0.6) | 0.89 (0.9,1) | 0.89 |
| Irritation | 9.8 (5.2) | 10 (6.25–13) | 9 (0–31) | −0.5 (0.5) | 0.80 (0.8,1) | 0.86 |
| Distress | 3.1 (3.0) | 2 (1–5) | 0 (0–27) | −0.4 (0.3) | 0.82 (0.8,1) | 0.86 |
| Disgust | 3.0 (3.0) | 2.5 (1–5) | 0 (0–28) | −0.6 * (0.3) | 0.84 (0.8,1) | 0.87 |
| Anger | 5.8 (4.6) | 5 (2–8) | 0 (0–26) | 0.2 (0.4) | 0.82 (0.8,1) | 0.86 |
| Panic | 1.9 (2.8) | 1 (0–3) | 0 (0–18) | −0.5 (0.3) | 0.83 (0.8,1) | 0.87 |
| TC | 24.1 (8.8) | 26 (20–30) | 29 (0–37) | −1.7 (0.8) | 0.89 (0.9,1) | 0.89 |
| FIRS | 146.1 (66.4) | 150 (103–189) | 173 (0–363) | −16.5 * (6.2) | 0.89 (0.9,1) | 0.89 |
| RIRS | 6 (1.4) | 6.1 (5.1–7) | 7 (2–10) | −0.3 (0.1) | 0.84 (0.8,1) | 0.87 |
| No Feeling | Irritation | Distress | Disgust | Anger | Panic | TC | FIRS | RIRS | |
|---|---|---|---|---|---|---|---|---|---|
| S-Five-T (N = 828) | |||||||||
| Irritation | −0.025 | ||||||||
| Distress | −0.142 ** | 0.068 | |||||||
| Disgust | −0.166 ** | 0.01 | 0.101 ** | ||||||
| Anger | −0.208 ** | 0.041 | −0.105 ** | 0.074 * | |||||
| Panic | −0.070 * | −0.150 ** | 0.120 ** | 0.023 | −0.041 | ||||
| TC | −0.257 ** | 0.590 ** | 0.404 ** | 0.420 ** | 0.522 ** | 0.256 ** | |||
| FIRS | −0.344 ** | 0.325 ** | 0.344 ** | 0.354 ** | 0.594 ** | 0.287 ** | 0.862 ** | ||
| RIRS | −0.282 ** | −0.287 ** | 0.02 | 0.028 | 0.294 ** | 0.154 ** | 0.052 | 0.503 ** | 1 |
| S-Five (N = 828) | |||||||||
| Internalising | −0.194 ** | −0.064 | 0.017 | 0.047 | 0.160 ** | 0.098 ** | 0.107 ** | 0.189 ** | 0.215 ** |
| Externalising | −0.155 ** | −0.078 * | −0.072 * | 0.064 | 0.159 ** | 0.017 | 0.037 | 0.127 ** | 0.221 ** |
| Impact | −0.300 ** | −0.149 ** | 0.111 ** | 0.027 | 0.190 ** | 0.257 ** | 0.152 ** | 0.303 ** | 0.344 ** |
| Outburst | −0.145 ** | −0.102 ** | −0.011 | −0.032 | 0.213 ** | 0.032 | 0.061 | 0.143 ** | 0.221 ** |
| Threat | −0.162 ** | −0.167 ** | 0.127 ** | 0.114 ** | 0.153 ** | 0.241 ** | 0.143 ** | 0.267 ** | 0.296 ** |
| Total | −0.281 ** | −0.152 ** | 0.038 | 0.053 | 0.253 ** | 0.172 ** | 0.139 ** | 0.288 ** | 0.367 ** |
| Age (N = 828) | |||||||||
| Age | −0.016 | 0.125 ** | −0.029 | −0.130 ** | 0.003 | 0.028 | 0.022 | 0.027 | −0.009 |
| A-MISO-S (N = 341) | |||||||||
| Total | −0.206 ** | −0.221 ** | 0.049 | 0.08 | 0.146 ** | 0.291 ** | 0.105 | 0.317 ** | 0.411 ** |
| MQ (N = 320) | |||||||||
| MSYS (N = 281) | −0.626 ** | 0.054 | 0.239 ** | 0.162 ** | 0.356 ** | 0.098 | 0.421 ** | 0.514 ** | 0.370 ** |
| MEBS (N = 281) | −0.198 ** | −0.134 * | 0.022 | 0.037 | 0.224 ** | 0.167 ** | 0.116 | 0.232 ** | 0.260 ** |
| MSES (N = 320) | −0.216 ** | −0.187 ** | 0.071 | −0.028 | 0.071 | 0.304 ** | 0.066 | 0.200 ** | 0.306 ** |
| Total (N = 281) | −0.503 ** | −0.06 | 0.156 ** | 0.121 * | 0.363 ** | 0.172 ** | 0.327 ** | 0.461 ** | 0.396 ** |
| PHQ9 (N = 800) | |||||||||
| Total | −0.227 ** | −0.091 ** | 0.081 * | 0.029 | 0.159 ** | 0.137 ** | 0.119 ** | 0.187 ** | 0.171 ** |
| GAD7 (N = 810) | |||||||||
| Total | 0.207 ** | 0.207 ** | 0.207 ** | 0.207 ** | 0.207 ** | 0.207 ** | 0.207 ** | 0.207 ** | 0.207 ** |
| WSAS (N = 813) | |||||||||
| Total | −0.362 ** | −0.131 ** | 0.126 ** | 0.05 | 0.151 ** | 0.219 ** | 0.148 ** | 0.269 ** | 0.290 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vitoratou, S.; Uglik-Marucha, N.; Hayes, C.; Gregory, J. Listening to People with Misophonia: Exploring the Multiple Dimensions of Sound Intolerance Using a New Psychometric Tool, the S-Five, in a Large Sample of Individuals Identifying with the Condition. Psych 2021, 3, 639-662. https://doi.org/10.3390/psych3040041
Vitoratou S, Uglik-Marucha N, Hayes C, Gregory J. Listening to People with Misophonia: Exploring the Multiple Dimensions of Sound Intolerance Using a New Psychometric Tool, the S-Five, in a Large Sample of Individuals Identifying with the Condition. Psych. 2021; 3(4):639-662. https://doi.org/10.3390/psych3040041
Chicago/Turabian StyleVitoratou, Silia, Nora Uglik-Marucha, Chloe Hayes, and Jane Gregory. 2021. "Listening to People with Misophonia: Exploring the Multiple Dimensions of Sound Intolerance Using a New Psychometric Tool, the S-Five, in a Large Sample of Individuals Identifying with the Condition" Psych 3, no. 4: 639-662. https://doi.org/10.3390/psych3040041
APA StyleVitoratou, S., Uglik-Marucha, N., Hayes, C., & Gregory, J. (2021). Listening to People with Misophonia: Exploring the Multiple Dimensions of Sound Intolerance Using a New Psychometric Tool, the S-Five, in a Large Sample of Individuals Identifying with the Condition. Psych, 3(4), 639-662. https://doi.org/10.3390/psych3040041