A Relational Model for Stress: A Systematic Review of the Risk and Protective Factors for Stress-Related Diseases in Firefighters



{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility
2.2. Information Source and Search
3. Results
3.1. The Perception of Stress
3.2. Social and Organizational Support
3.3. Professionals and Volunteers
3.4. Coping
4. Discussion
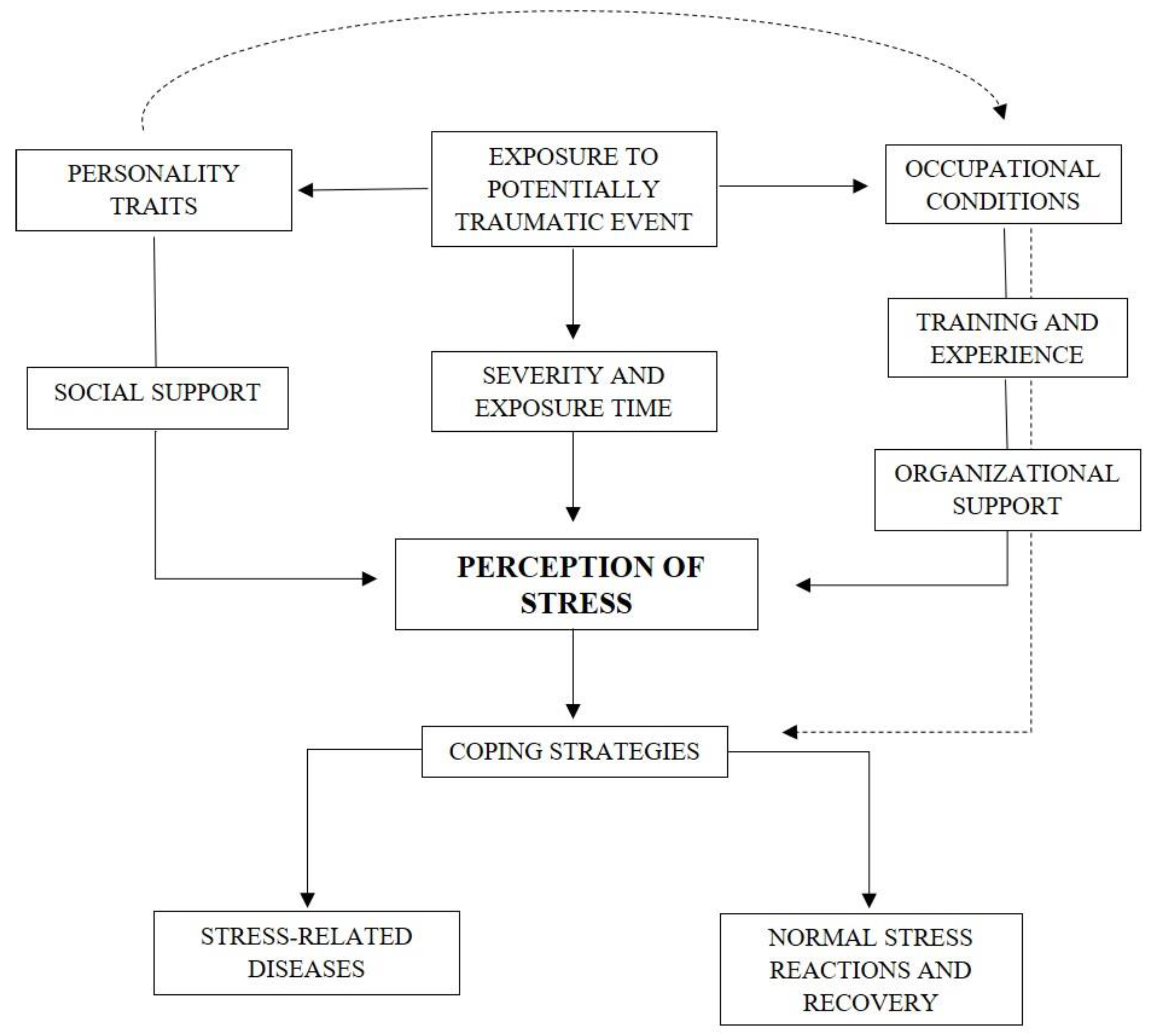
A Relational Model for Stress in Firefighters
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Psarros, C.; Theleritis, C.; Kokras, N.; Lyrakos, D.; Koborozos, A.; Kakabakou, O.; Tzanoulinos, G.; Katsiki, P.; Bergiannaki, J.D. Personality characteristics and individual factors associated with PTSD in firefighters one month after extended wildfires. Nord. J. Psychiatry 2018, 72, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Dunn, R.; Amlôt, R.; Greenberg, N.; Rubin, J. Social and occupational factors associated with psychological distress and disorder among disaster responders: A systematic review. BMC Psychol. 2016, 4, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Fraess-Phillips, A.; Wagner, S.; Harris, R. Firefighters and traumatic stress: A review. Int. J. Emerg. Serv. 2017, 6, 67–80. [Google Scholar] [CrossRef]
- Stanley, I.H.; Hom, M.A.; Joiner, T.E. A systematic review of suicidal thoughts and behaviors among police officers, firefighters, EMTs, and paramedics. Clin. Psychol. Rev. 2016, 44, 24–44. [Google Scholar] [CrossRef]
- Lowe, S.R.; Blachman-Forshay, J.; Koenen, K.C. Trauma as a Public Health Issue: Epidemiology of Trauma and Trauma-Related Disorders. In Evidence Based Treatments for Trauma-Related Psychological Disorders: A Practical Guide for Clinicians; Schnyder, U., Cloitre, M., Eds.; Springer: Zurich, Switzerland, 2015; pp. 11–40. [Google Scholar]
- Association, A.P. Diagnostic and Statistical Manual of Mental Disorders: Fifth edition DSM-5™; American Psychiatric Association Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Brewin, C.R.; Andrews, B.; Valentine, J.D. Meta-Analysis of Risk Factors for Posttraumatic Stress Disorder in Trauma-Exposed Adults. J. Consult. Clin. Psychol. 2000, 68, 748–766. [Google Scholar] [CrossRef]
- Institute of Medicine. Posttraumatic Stress Disorder: Diagnosis and Assessment; The National Academies Press: Washington, DC, USA, 2006. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Bartlett, B.A.; Jardin, C.; Martin, C.; Tran, J.K.; Buser, S.; Anestis, M.D.; Vujanovic, A.A. Posttraumatic stress and suicidality among firefighters: The moderating role of distress tolerance. Cogn. Ther. Res. 2018, 42, 483–496. [Google Scholar] [CrossRef]
- Boffa, J.W.; Stanley, I.H.; Hom, M.A.; Norr, A.M.; Joiner, T.E.; Schmidt, N.B. PTSD symptoms and suicidal thoughts and behaviors among firefighters. J. Psychiatr. Res. 2017, 84, 277–283. [Google Scholar] [CrossRef]
- Katsavouni, F.; Bebetsos, E.; Malliou, P.; Beneka, A. The relationship between burnout, PTSD symptoms and injuries in firefighters. Occup. Med. 2016, 66, 32–37. [Google Scholar] [CrossRef]
- Jo, I.; Lee, S.; Sung, G.; Kim, M.; Lee, S.; Park, J.; Lee, K. Relationship between burnout and PTSD symptoms in firefighters: The moderating effects of a sense of calling to firefighting. Int. Arch. Occup. Environ. Health 2018, 91, 117–123. [Google Scholar] [CrossRef]
- Brazil, A. Exploring Critical Incidents and Postexposure Management in a Volunteer Fire Service. J. Aggress. Maltreatment Trauma 2017, 26, 244–257. [Google Scholar] [CrossRef]
- Kim, J.E.; Dager, S.R.; Jeong, H.S.; Ma, J.; Park, S.; Kim, J.; Choi, Y.; Lee, S.L.; Kang, I.; Ha, E.; et al. Firefighters, posttraumatic stress disorder, and barriers to treatment: Results from a nationwide total population survey. PLoS ONE 2018, 13, e0190630. [Google Scholar] [CrossRef] [PubMed]
- Boffa, J.W.; Stanley, I.H.; Smith, L.J.; Mathes, B.M.; Tran, J.K.; Buser, S.J.; Schmidt, N.B.; Vujanovic, A.A. Posttraumatic Stress Disorder Symptoms and Suicide Risk in Male Firefighters: The mediating role of anxiety sensitivity. J. Nerv. Ment. Dis. 2018, 206, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Stanley, I.H.; Boffa, J.W.; Hom, M.A.; Kimbrel, N.A.; Joiner, T.E. Differences in psychiatric symptoms and barriers to mental health care between volunteer and career firefighters. Psychiatry Res. 2017, 247, 236–242. [Google Scholar] [CrossRef]
- Carpenter, T.P.; Pennington, M.L.; Seebeck, J.; Gomez, D.R.; Denman, T.C.; Kimbrel, N.A.; Cammarata, C.M.; Leto, F.; Ostiguy, W.J.; Gulliver, S.B. Dispositional self-forgiveness in firefighters predicts less help-seeking stigma and fewer mental health challenges. Stigma Health 2020, 5, 29–37. [Google Scholar] [CrossRef]
- Gulliver, S.B.; Pennington, M.L.; Torres, V.A.; Steffen, L.E.; Mardikar, A.; Leto, F.; Ostiguy, W.; Zimering, R.T.; Kimbrel, N.A. Behavioral health programs in fire service: Surveying access and preferences. Psychol. Serv. 2019, 16, 340–345. [Google Scholar] [CrossRef]
- Armstrong, D.; Schakespeare-Finch, J.; Shochet, I. Predicting post-traumatic growth and post-traumatic stress in firefighters. Aust. J. Psychol. 2014, 66, 38–46. [Google Scholar] [CrossRef]
- Bartlett, B.A.; Smith, L.J.; Lebaut, A.; Tran, J.K.; Vujanovic, A. PTSD symptom severity and impulsivity among firefighters: Associations with alcohol use. Psychiatry Res. 2019, 278, 315–323. [Google Scholar] [CrossRef]
- Bastug, G.; Ergul-Topcu, A.; Ozel-Kizil, E.T.; Ergun, O.F. Secondary Traumatization and Related Psychological Outcomes in Firefighters. J. Loss Trauma 2019, 24, 143–158. [Google Scholar] [CrossRef]
- Haraldsdóttir, H.A.; Gudmundsdóttir, D.; Romano, E.; Póroardóttir, E.B.; Guomundsdóttir, B.; Elklit, A. Volunteers and professional rescue workers: Traumatization and adaptation after an avalanche disaster. J. Emerg. Manag. 2014, 12, 457–466. [Google Scholar] [CrossRef]
- Kim, J.I.; Park, H.; Kim, J.H. The mediation effect of PTSD, perceived job stress and resilience on the relationship between trauma exposure and the development of depression and alcohol use problems in 7151 Korean firefighters: A cross-sectional study. J. Affec. Disord. 2018, 229, 450–455. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Lee, D.; Kim, J.; Jeon, K.; Sim, M. Duty-Related Trauma Exposure and Posttraumatic Stress Symptoms in Professional Firefighters. J. Trauma Stress 2017, 30, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Paulus, D.J.; Vujanovic, A.A.; Schuhmann, B.B.; Smith, L.J.; Tran, J. Main and interactive effects of depression and posttraumatic stress in relation to alcohol dependence among urban male firefighters. Psychiatry Res. 2017, 251, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Jahnke, S.A.; Poston, W.S.; Haddock, C.K.; Murphy, B. Firefighting and mental health: Experiences of repeated exposure to trauma. Work 2016, 53, 737–744. [Google Scholar] [CrossRef]
- Yip, J.; Zeig-Owens, R.; Hall, C.B.; Webber, M.P.; Olivieri, B.; Schwartz, T.; Kelly, K.J.; Prezant, D.J. Health Conditions as Mediators of the Association Between World Trade Center Exposure and Health-Related Quality of Life in Firefighters and EMS Workers. J. Occup. Environ. Med. 2016, 58, 200–206. [Google Scholar] [CrossRef]
- Kehl, D.; Knuth, D.; Hulse, L.; Schmidt, S. Posttraumatic Reactions among Firefighters after Critical Incidents: Cross-National Data. J. Aggress. Maltreatment Trauma 2014, 23, 842–853. [Google Scholar] [CrossRef]
- Lee, J.S. Perceived social support functions as a resilience in buffering the impact of trauma exposure on PTSD symptoms via intrusive rumination and entrapment in firefighters. PLoS ONE 2019, 14, e0220454. [Google Scholar] [CrossRef]
- Pinto, R.J.; Henriques, S.P.; Jongenelen, I.; Carvalho, C.; Maia, Â.C. The Strongest Correlates of PTSD for Firefighters: Number, Recency, Frequency, or Perceived Threat of Traumatic Events? J. Trauma Stress 2015, 28, 434–440. [Google Scholar] [CrossRef]
- Smith, L.J.; Paulus, D.J.; Gallagher, M.W.; Norman, S.B.; Tran, J.; Vujanovic, A. Perceived stress and probable alcohol misuse in firefighters: The role of posttraumatic stress. J. Stress Manag. 2019, 26, 367–377. [Google Scholar] [CrossRef]
- Lee, J.S.; Ahn, Y.S.; Jeong, K.S.; Chae, J.H.; Choi, K.S. Resilience buffers the impact of traumatic events on the development of PTSD symptoms in firefighters. J. Affec. Disord. 2014, 162, 128–133. [Google Scholar] [CrossRef]
- Makara-Studzinska, M.; Golonka, K.; Izydorczyk, B. Self-Efficacy as a Moderator between Stress and Professional Burnout in Firefighters. Int. J. Environ. Res. Public Health 2018, 16, 183. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.E.; Tran, J.K.; Buser, S.J. Correlates of suicidality in firefighters/EMS personnel. J. Affec. Disord. 2017, 208, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Sattler, D.N.; Boyd, B.; Kirsch, J. Trauma-exposed Firefighters: Relationships among Posttraumatic Growth, Posttraumatic Stress, Resource Availability, Coping and Critical Incident Stress Debriefing Experience. Stress Health 2014, 30, 356–365. [Google Scholar] [CrossRef] [PubMed]
- Yun, J.A.; Ahn, Y.S.; Jeong, K.S.; Joo, E.J.; Choi, K.S. The Relationship between Chronotype and Sleep Quality in Korean Firefighters. Clin. Psychopharmacol. Neurosci. 2015, 13, 201–208. [Google Scholar] [CrossRef]
- Oginska-Bulik, N.; Kobylarczyk, M. Association between resiliency and posttraumatic growth in firefighters: The role of stress appraisal. Int. J. Occup. Saf. Erg. 2016, 22, 40–48. [Google Scholar] [CrossRef]
- Shrira, A.; Shmotkin, D.; Palgi, Y.; Soffer, Y.; Hamama, Y.R.; Tal-Katz, P.; Ben-Ezra, M.; Benight, C.C. How Do Meaning in Life and Positive Affect Relate to Adaptation to Stress? The Case of Firefighters Following the Mount Carmel Forest Fire. Isr. J. Psychiatry Relat. Sci. 2015, 52, 68–70. [Google Scholar]
- Yang, S.K.; Ha, Y. Predicting Posttraumatic Growth among Firefighters: The Role of Deliberate Rumination and Problem-Focused Coping. Int. J. Environ. Res. Public Health 2019, 16, 3879. [Google Scholar] [CrossRef]
- Armstrong, D.; Shakespeare-Finch, J.; Shochet, I. Organizational Belongingness Mediates the Relationship between Sources of Stress and Posttrauma Outcomes in Firefighters. Psychol. Trauma 2016, 8, 343–347. [Google Scholar] [CrossRef]
- Huang, J.; Wang, X.; Li, W.; An, Y. The relationship between conscientiousness and posttraumatic stress disorder among young Chinese firefighters: The mediating effect of perceived social support. Psychiatry Res. 2019, 273, 450–455. [Google Scholar] [CrossRef]
- Wagner, S.; Pasca, R.; Crosina, J. Hostility in firefighters: Personality and mental health. Int. J. Emerg. Serv. 2016, 5, 6–17. [Google Scholar] [CrossRef]
- Stanley, I.H.; Hom, M.A.; Chu, C.; Dougherty, S.P.; Gallyer, A.J.; Spencer-Thomas, S.; Shelef, L.; Fruchter, E.; Comtois, K.A.; Gutierrez, P.M.; et al. Perceptions of belongingness and social support attenuate PTSD symptom severity among firefighters: A multistudy investigation. Psychol Serv. 2019, 16, 543–555. [Google Scholar] [CrossRef]
- Skeffington, P.M.; Rees, C.S.; Mazzucchelli, T. Trauma exposure and post-traumatic stress disorder within fire and emergency services in Western Australia. Aust. J. Psychol. 2016, 69, 20–28. [Google Scholar] [CrossRef]
- Levy-Gigi, E.; Bonanno, G.A.; Shapiro, A.R.; Richter-Levin, G.; Kéri, S.; Sheppes, G. Emotion Regulatory Flexibility Sheds Light on the Relationship Between Repeated Traumatic Exposure and Posttraumatic Stress Disorder Symptoms. Clin. Psychol. Sci. 2015, 4, 28–39. [Google Scholar] [CrossRef]
- Park, H.; Kim, J.I.; Oh, S.; Kim, J.H. The impact of emotional labor on the severity of PTSD symptoms in firefighters. Compr. Psychiatry 2018, 83, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Kim, J.I.; Min, B.; Oh, S.; Kim, J.H. Prevalence and correlates of suicidal ideation in Korean firefighters: A nationwide study. BMC Psychiatry 2019, 19, 428. [Google Scholar] [CrossRef]
- Tomaka, J.; Magoc, D.; Morales-Monks, S.M.; Reyes, A.C. Posttraumatic Stress Symptoms and Alcohol-Related Outcomes among Municipal Firefighters. J. Trauma Stress 2017, 30, 416–424. [Google Scholar] [CrossRef]
- Zegel, M.; Tran, J.; Vujanovic, A. Posttraumatic stress, alcohol use, and alcohol use motives among firefighters: The role of distress tolerance. Psychiatry Res. 2019, 282, 112633. [Google Scholar] [CrossRef]
- Lee, J.H.; Park, S.; Sim, M. Relationship between ways of coping and posttraumatic stress symptoms in firefighters compared to the general population in South Korea. Psychiatry Res. 2018, 270, 649–655. [Google Scholar] [CrossRef]
- Bing-Canar, H.; Ranney, R.M.; McNett, S.; Tran, J.; Berenz, E.C.; Vujanovic, A. Alcohol Use Problems, Posttraumatic Stress Disorder, and Suicide Risk Among Trauma-Exposed Firefighters. J. Nerv. Ment. Dis 2019, 207, 192–198. [Google Scholar] [CrossRef]
- Kim, J.I.; Park, H.; Kim, J.H. Alcohol use disorders and insomnia mediate the association between PTSD symptoms and suicidal ideation in Korean firefighters. Depress. Anxiety 2018, 35, 1095–1103. [Google Scholar] [CrossRef]
- Milligan-Saville, J.S.; Paterson, H.M.; Harkness, E.L.; Marsh, A.M.; Dobson, M.; Kemp, R.I.; Bryant, R.A.; Harvey, S.B. The Amplification of Common Somatic Symptoms by Posttraumatic Stress Disorder in Firefighters. J. Trauma Stress 2017, 30, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Straud, C.; Henderson, S.N.; Vega, L.; Black, R.; Van Hasselt, V. Resiliency and Posttraumatic Stress Symptoms in Firefighters Paramedics: The Mediating Role of Depression, Anxiety, and Sleep. Traumatology 2018, 24, 140–147. [Google Scholar] [CrossRef]
- Paltell, K.C.; Bing-Canar, H.; Ranney, R.M.; Tran, J.; Berenz, E.C.; Vujanovic, A. Anxiety Sensitivity Moderates the Effect of Posttraumatic Stress Disorder Symptoms on Emotion Dysregulation among Trauma-Exposed Firefighters. J. Psychopathol. Behav. Asess. 2019, 41, 524–535. [Google Scholar] [CrossRef]
- Khumtong, C.; Taneepanichskul, N. Posttraumatic stress disorder and sleep quality among urban firefighters in Thailand. Nat. Sci. Sleep 2019, 11, 123–130. [Google Scholar] [CrossRef]
- Kim, W.; Bae, M.; Chang, S.J.; Yoon, J.H.; Jeong, D.Y.; Hyun, D.S.; Ryu, H.Y.; Park, K.S.; Kim, M.J.; Kim, C. Effect of Burnout on Post-traumatic Stress Disorder Symptoms Among Firefighters in Korea: Data From the Firefighter Research on Enhancement of Safety & Health (FRESH). J. Prev. Med. Public Health 2019, 52, 345–354. [Google Scholar] [CrossRef]
- Kim, M.J.; Jeong, Y.; Choi, Y.S.; Seo, A.R.; Ha, Y.; Seo, M.; Park, K.S. The Association of the Exposure to Work-Related Traumatic Events and Work Limitations among Firefighters: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2019, 16, 756. [Google Scholar] [CrossRef]
- Noor, N.; Pao, C.; Dragomir-Davis, M.; Tran, J.; Arbona, C. PTSD symptoms and suicidal ideation in US female firefighters. Occup. Med. 2019, 69, 577–585. [Google Scholar] [CrossRef]

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Becker, J.P.; Paixão, R.; Quartilho, M.J. A Relational Model for Stress: A Systematic Review of the Risk and Protective Factors for Stress-Related Diseases in Firefighters. Psych 2020, 2, 74-84. https://doi.org/10.3390/psych2010008
Becker JP, Paixão R, Quartilho MJ. A Relational Model for Stress: A Systematic Review of the Risk and Protective Factors for Stress-Related Diseases in Firefighters. Psych. 2020; 2(1):74-84. https://doi.org/10.3390/psych2010008
Chicago/Turabian StyleBecker, Joana Proença, Rui Paixão, and Manuel João Quartilho. 2020. "A Relational Model for Stress: A Systematic Review of the Risk and Protective Factors for Stress-Related Diseases in Firefighters" Psych 2, no. 1: 74-84. https://doi.org/10.3390/psych2010008
APA StyleBecker, J. P., Paixão, R., & Quartilho, M. J. (2020). A Relational Model for Stress: A Systematic Review of the Risk and Protective Factors for Stress-Related Diseases in Firefighters. Psych, 2(1), 74-84. https://doi.org/10.3390/psych2010008